
Abstract
Previous research suggests that victims of partner physical violence (PPV) often face multiple distinct problems, but comparative population-based studies focusing on the prevalence of multiple problems are lacking. Aim of the present study is to gain insight in the prevalence of multiple problems among individuals victimized by PPV in the past 12 months, compared with matched nonvictims and victims of non-partner physical violence (non-PPV). For this purpose, data were extracted from two population-based surveys conducted in 2018 and 2019 on potentially traumatic events in the Netherlands. We focused on problems identified in previous studies on PPV and non-PPV and related problems, varying from physical health, mental health, financial and legal problems, to lack of social support and being exposed to other potentially traumatic and stressful life events (LFEs). In total, 49 respondents were victimized by PPV and 89 by non-PPV in the past 12 months. They were compared with pairwise matched groups not affected by any traumatic or stressful LFEs in this period (nPPV victims comparison group = 245, nnon-PPV comparison group = 445). Results showed that PPV victims significantly more often faced all 12 distinct problems than matched nonvictims (2.31 ≤ odds ratio [OR] ≤ 15.48) and non-PPV victims (2.12 ≤ OR ≤ 4.52). PPV victims more often had any problem than non-PPV victims (OR = 8.19), but no significant differences were found between PPV and non-PPV victims with regard to mental health problems. Findings stress the necessity of a multidisciplinary coordinated community response to help PPV victims.
Introduction
Partner physical violence (PPV) is a serious problem across countries, age categories, sexes, and religions (Azam Ali & Naylor, 2013). The World Health Organization’s (WHO) World Mental Health Surveys conducted in 24 countries found a lifetime prevalence of physical abuse by a romantic partner of 14% across countries (Kessler et al., 2017). However, differences between countries and estimates exist, partly depending on sampling methods and definitions of partner violence. For example, the 2010 U.S. National Intimate Partner and Sexual Violence Survey (NIPSVS; Black et al., 2011) showed a lifetime prevalence of physical violence by an intimate partner of 32.9% among women and 28.2% among men (cf. Garcia-Moreno, Jansen, Ellsberg, Heise, & Watts, 2006). PPV is associated with an increased risk of various serious mental health problems besides post-traumatic stress disorder (PTSD; Kessler et al., 2017). PPV is also correlated with depression (Beydoun, Beydoun, Kaufman, Lo, & Zonderman, 2012), disordered eating (Bartlett, Iverson, & Mitchell, 2018), suicidality (McLaughlin, O’Carroll, & O’Connor, 2012), alcohol problems (Devries et al., 2014), borderline traits (Kuijpers, van der Knaap, Winkel, Pemberton, & Baldry, 2011), low spiritual well-being (Arnette, Mascaro, Santana, Davis, & Kaslow, 2007), bodily pain (Loxton, Dolja-Gore, Anderson, & Townsend, 2017), and cardiovascular diseases (Stene, Jacobsen, Dyb, Tverdal, & Schel, 2018). However, associations between PPV and problems are not restricted to the associations between PPV with various mental and physical health problems. PPV is also related with financial problems or stressors (Schwab-Reese, Peek-Asa, & Parker, 2016); legal problems or problems with the justice system (Jordan, 2004); a lack of social support (Dias et al., 2018); work problems, such as job instability and job loss (Showalter, 2016); and challenges related to faith and religion (Tarrezz Nash, Faulkner, & Abell, 2013) that may have a negative impact on mental health and well-being. In addition, victims of PPV may be more often confronted with other potentially traumatic stressful life events (LFEs; Kennedy, Bybee, Palma-Ramirez, & Jacobs, 2017).
The list of associations between PPV and problems clearly suggest that victims of PPV are often more confronted with an accumulation of various problems than nonvictims. However, to the best of our knowledge, population-based studies assessing the prevalence of multiple problems among victims compared with matched nonvictims are absent; for example studies assessing the prevalence of having, for example, physical problems and psychological problems and financial problems and a lack of emotional social support and legal problems and experiencing other potentially traumatic events (PTEs). Similarly, to the best of our knowledge, to date, no population-based study examined problems and multiple problems among PPV victims compared with victims of non-partner physical violence (non-PPV), although this comparison may help to provide insight in the unique effects of partner-related violence above the effects of violence.
Nevertheless, insight in the nature and prevalence of multiple problems among victims is of relevance for policy makers and involved professionals, such as social workers, law enforcers, family practitioners, medical specialists, lawyers, therapist, and employees of (non)governmental agencies devoted to victims of PPV. It may, if confirmed by empirical data, enhance awareness of the multiple problems victims are faced with and, therefore, enhance effective multidisciplinary interventions without ignoring the relevance and efficacy of interventions for PPV victims aimed at distinct problems, such as the treatment of PPV victims with PTSD (cf. Arroyo, Lundahl, Butters, Vanderloo, & Wood, 2017). For instance, if financial problems are very prominent among PPV victims with mental health problems, interventions should focus on both, given the stress accompanied by financial problem (Kiely, Leach, Olesen, & Butterworth, 2015).
The aim of the present study is to examine the nature and prevalence of multiple problems among individuals victimized by PPV in the past 12 months, by comparing the prevalence of 12 different problems and multiple problems with the prevalence among matched nonvictims and among matched non-PPV victims (also victimized in the past 12 months). For this purpose, we also compared the prevalence of problems and multiple problems among victims of non-partner violence with matched nonvictims. We hypothesized that victims of non-partner violence more often suffer from problems and multiple problems than nonvictims, and victims of PPV more often suffered from problems and multiple problems than nonvictims and victims of non-partner violence.
Based on previous research on the effects of partner violence (see above), we focused on the following problems: physical problems; mental health problems; problems with religion; problems at work; problems in the family/with partner; financial problems; legal problems; lack of emotional, appreciation support, and listening ear; and being exposed to other potentially traumatic and/or LFEs in the past year. We also assessed administrative problems because, although we could not find studies among victims of PPV aimed at these problems, aforementioned problems may be accompanied by various letters and emails from, for instance, banks, insurance companies, work, health institutions, social welfare, and housing corporations creating a problem in itself.
Method
Procedures and Participants
Data were collected in the Longitudinal Internet Studies for the Social Sciences (LISS) panel, administered by CentERdata (Tilburg, The Netherlands; Scherpenzeel & Das, 2011) and granted by the Netherlands Organization for Scientific Research (NWO). The LISS panel is based on a large representative random sample drawn from the Dutch population register by Statistics Netherlands. Panel members receive an incentive of €15 per hour for their participation and those who do not have a computer and/or Internet access are provided with the necessary equipment at home (Scherpenzeel & Das, 2011). Further information about the panel and free access to the data archive can be found on https://www.lissdata.nl/ (in English).
We extracted data from two surveys of the longitudinal research project titled Victims in Modern Society (VICTIMS) project. In March 2018 (with reminders in April), participants were administered the first survey (N = 7,292, responsecompleters = 82.1%) and the second survey was conducted in March 2019 (with reminders in April; N = 6,298, responsecompleters = 83.2%). The questionnaire was approved by a panel of internal and external reviewers of CentERdata. Previous research using the LISS panel revealed that the possible burden of participating in research on trauma was related to perceived burden of other nontrauma studies (such as on political values), and not PTSD symptoms and other PTE-related variables (van der Velden, Bosmans, & Scherpenzeel, 2013). All participants gave their informed consent.
Measures
At both surveys, respondents were asked whether they were exposed to PPV and to non-PPV in the past 12 months, besides 19 other PTEs varying from serious threat, accidents, burglary, medical errors, to (un)expected loss of a significant other to disaster (1 = not exposed, 2 = exposed). As said, in the list, we also included events such as (un)expected death of a significant other (Criterion A1 events in Diagnostic and Statistical Manual of Mental Disorders [4th ed.; DSM-IV; American Psychiatric Association, 1994]) regardless if the death involved some type of accident or violence (Criterion A1 in Diagnostic and Statistical Manual of Mental Disorders [5th ed., DSM-5; American Psychiatric Association, 2013]). The 21-item PTE questionnaire is based on previous research on (lifetime) PTEs (Bronner et al., 2009; de Vries & Olff, 2009; Hentschel, Eid, & Kutscher, 2016; van der Velden et al., 2013) and the criteria of DSM-IV and DSM-5. Because we focused on adults and events in the past 12 months, PTEs such as child abuse and World War II (WW II) experiences were excluded (see the appendix). Participants were offered the opportunity to describe PTEs in the past 12 months that were not listed. They were recoded in present or new categories of PTE, or LFEs. For example, described events that were recoded as LFEs were becoming unemployed, divorce of adult child, or diagnosis dementia of parent.
To assess current problems, the brief screening Problems and Help Inventarisation-List (PHIL; van der Velden & Kleber, 1999) was administered at both surveys because it captures the various problems victims of PPV may face according to previous research (except administrative problems). Respondents were asked whether they have physical problems, mental health problems, problems with religion, problems at work, problems in the family/with partner, financial problems, administrative problems, and/or legal problems (1 = yes, 2 = no). For each reported problem, respondents were asked whether they needed, used, postponed, searched for, or could not afford professional help, but for the present study, we focused on reported problems only.
Anxiety and depression symptoms were examined twice using the brief Mental Health Inventory (MHI-5, five-item subscale of the Medical Outcomes Study [MOS] 36-item short-form health survey; Ware & Sherbourne, 1992). The MHI-5 has 6-point Likert-type scales (5 = never to 0 = continuously). After recoding the positive formulated third and fifth items, the total scores were computed and multiplied by four (Cronbach’s α > .85) according to the instructions. Lower scores reflect more symptoms. A cutoff of ≤44 (Driessen, 2011) was used to identify respondents with moderate to severe anxiety and depression symptoms.
To examine lack of social support, two scales of the Social Support List–Discrepancy (SSL-D; Bridges, Sanderman, & van Sonderen, 2002) were administered at both surveys. They examined lack of emotional support in response to problems (eight items) and lack of appreciation support (six items). The SSL-D invites respondents to rate their opinions or perceptions about people with whom they interact, that is, rating statements such as “they comfort you” on 4-point Likert-type scales (1 = I miss it, I would like it to happen more often to 4 = it happens too often; Cronbach’s αs ≥ .78). For the present study, scores on both scales of the SSL-D were dichotomized in relative high and low scores (cutoff scores of about lower 20% or lowest two deciles among the total study sample of 5,879 respondents: SSL-Dhigh lack of emotional support scores ≤ 19, SSL-Dhigh lack of appreciation support scores ≤ 14). In addition, one separate item was devoted to having a “listening ear” with the same 4-point Likert-type scale. For the present study, the answers were recoded (1 and 2 = no, 3 and 4 = yes).
Data Analysis
Using the data of the two surveys, in total, 49 respondents appeared to be exposed to PPV and 89 respondents to non-PPV violence in the previous 12 months. Some respondents were exposed to both types of violence and this subgroup (n = 7) was too small for the statistical analyses. We, therefore, included these respondents in the PPV group and excluded them from the non-PPV group, to obtain exclusive PPV and non-PPV groups enabling comparisons between the two subgroups. A small number of respondents was exposed to violence in the year before the first survey and in the year before the second survey. For the present study, they were included in the sample of victims identified in the first survey.
To obtain optimal estimates of the relative prevalence of (multi)problems among victims of PPV and non-PPV, we arranged two pairwise matched nonvictim comparison groups to prevent as much as possible differences that were confounded by differences in demographics. The number of victims of PPV and non-PPV limits the possibilities to control for potential confounders such as demographics. The matching was conducted based on 32 possible individual profiles (4age groups * 2marital status * 2work status * 2sex = 32 profiles) of the victims. For each affected respondent with a certain profile (e.g., female, 18-34 years old, employed, and living [married] together), we selected five nonaffected respondents at random from the total group of respondents not affected by PTEs or stressful LFEs in the past 12 months with the same demographic profile (in this case, female, 18-34 years old, employed, and living [married] together married). For victims identified (or included) in the first survey, nonaffected respondents were selected who participated in the first survey. For victims identified in the second survey, nonaffected respondents were selected who participated in the second survey. Both nonaffected comparison groups have, therefore, identical demographic characteristics as the two affected groups (see Table 1). Bivariate odds ratios (ORs) were computed using logistic regression to assess differences in problems between affected and matched nonaffected respondents. T tests were conducted to examine differences between study groups in the total number of distinguished problems. Because of the matching procedure, the assessment of possible differences in demographics between affected and comparison groups was redundant. For all analyses, IBM SPSS 25 was used.
Demographics of Victims of PPV and Non-PPV and Matched Nonvictims.
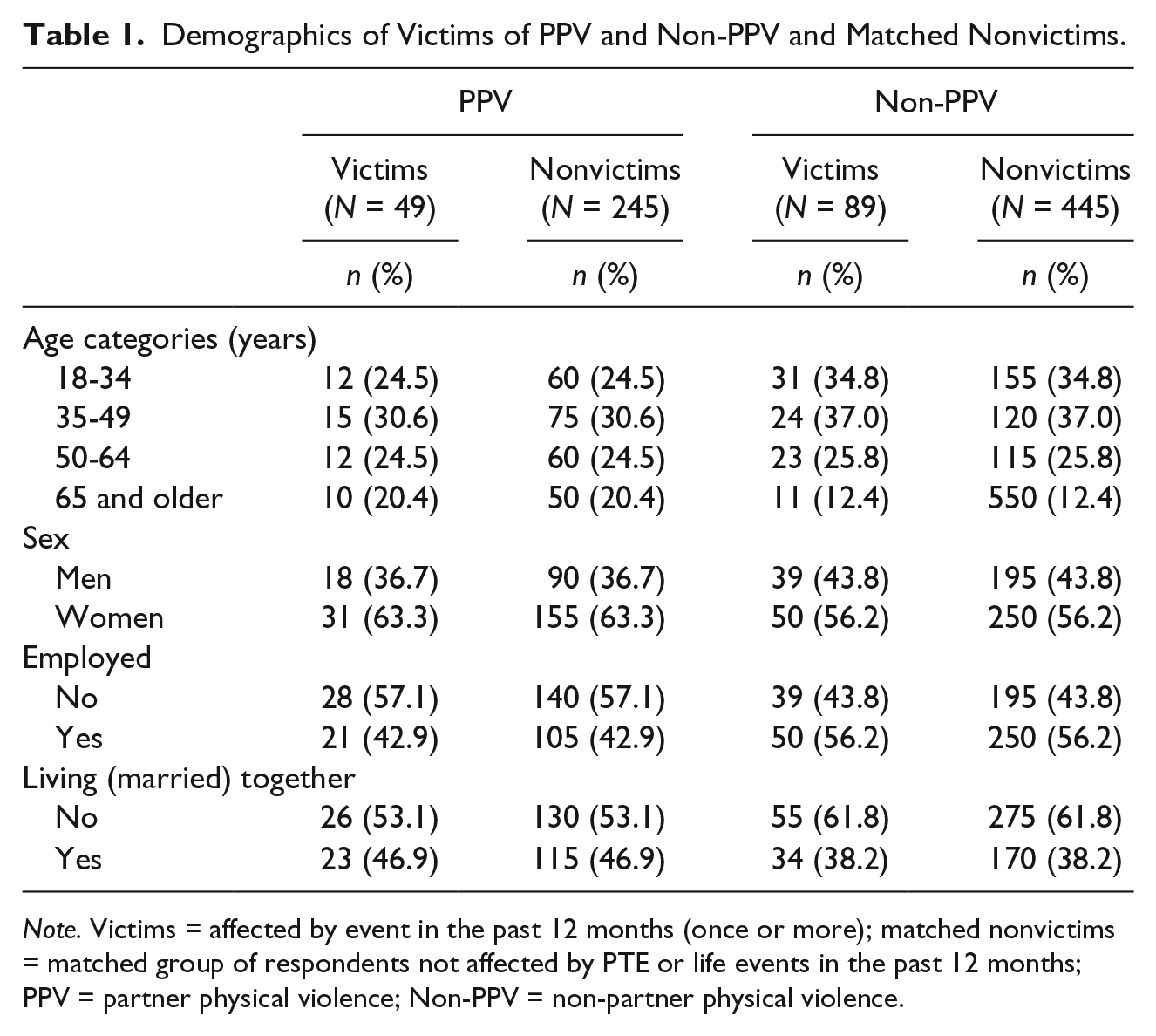
Note. Victims = affected by event in the past 12 months (once or more); matched nonvictims = matched group of respondents not affected by PTE or life events in the past 12 months; PPV = partner physical violence; Non-PPV = non-partner physical violence.
Results
Characteristics of Study Samples
In Table 1, the demographic characteristics of the four study samples are presented. Because of the matching procedure, the characteristics of the two victims groups are similar to their matched groups of nonvictims.
Problems Among Victims Versus Nonvictims
Table 2 presents the differences between the victims of PPV and their matched comparison participants. PPV victims had significantly more physical and mental health problems; problems with their religion, work, and family/partner; financial and administrative problems; high levels of depression and anxiety symptoms; a lack of appreciation and emotional support, and listening ear. Table 2 also shows that the victims of non-PPV compared with nonaffected respondents significantly more often had each of the listed problems than the nonaffected matched respondents, except a lack of a listening ear. The differences in assessed problems between the non-PPV victims and matched control group are smaller than the differences between PPV victims and matched control group.
Problems Among Victims and Matched Nonvictims.
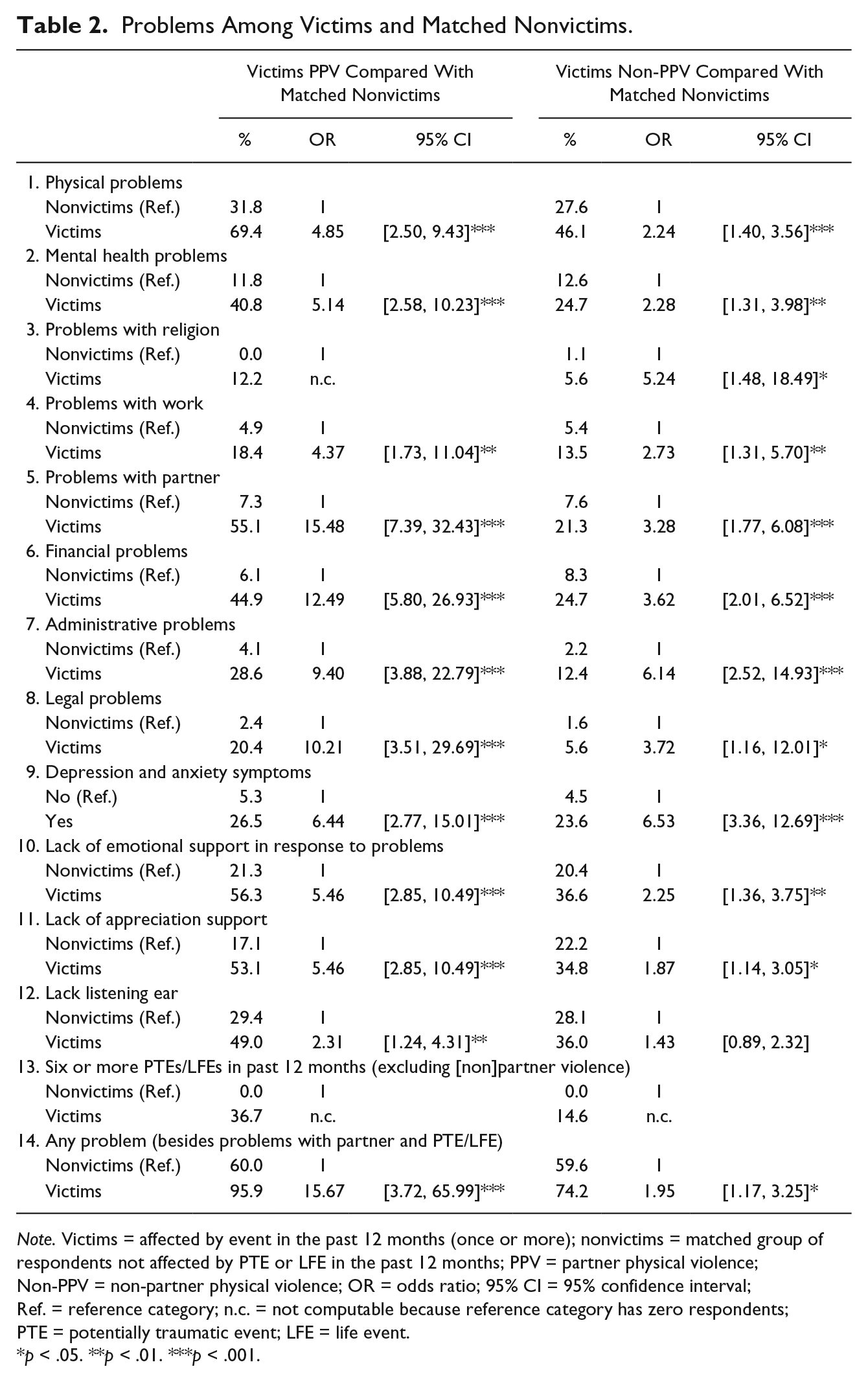
Note. Victims = affected by event in the past 12 months (once or more); nonvictims = matched group of respondents not affected by PTE or LFE in the past 12 months; PPV = partner physical violence; Non-PPV = non-partner physical violence; OR = odds ratio; 95% CI = 95% confidence interval; Ref. = reference category; n.c. = not computable because reference category has zero respondents; PTE = potentially traumatic event; LFE = life event.
p < .05. **p < .01. ***p < .001.
Problems Among PPV Victims Versus Non-PPV Victims
Victims of PPV and victims of non-PPV did not differ significantly in demographics (for demographics of the two subgroups, see Table 1).
Bivariate analyses showed that victims of PPV compared with non-PPV victims significantly more often had physical problems (OR = 2.65, 95% confidence interval [CI] = [1.27, 5.54], p = .009), problems with family/partner (OR = 4.52, 95% CI = [2.12, 9.65], p < .001), financial problems (OR = 2.48, 95% CI = [1.18, 5.21], p = .016), administrative problems (OR = 2.84, 95% CI = [1.17, 6.87], p = .021), legal problems (OR = 4.31, 95% CI = [1.38, 13.45], p = .012), lack of emotional support (OR = 2.23, 95% CI = [1.08, 4.61], p = .031), lack of appreciation support (OR = 2.12, 95% CI = [1.04, 4.30], p = .039), and being exposed to other PTEs (OR = 3.40, 95% CI = [1.49, 7.76], p = .004). No significant differences were found in problems with religion, problems at work, mental health problems (p=.051), and anxiety and depression symptoms (p = .702) according to the MHI-5.
Multiple Problems
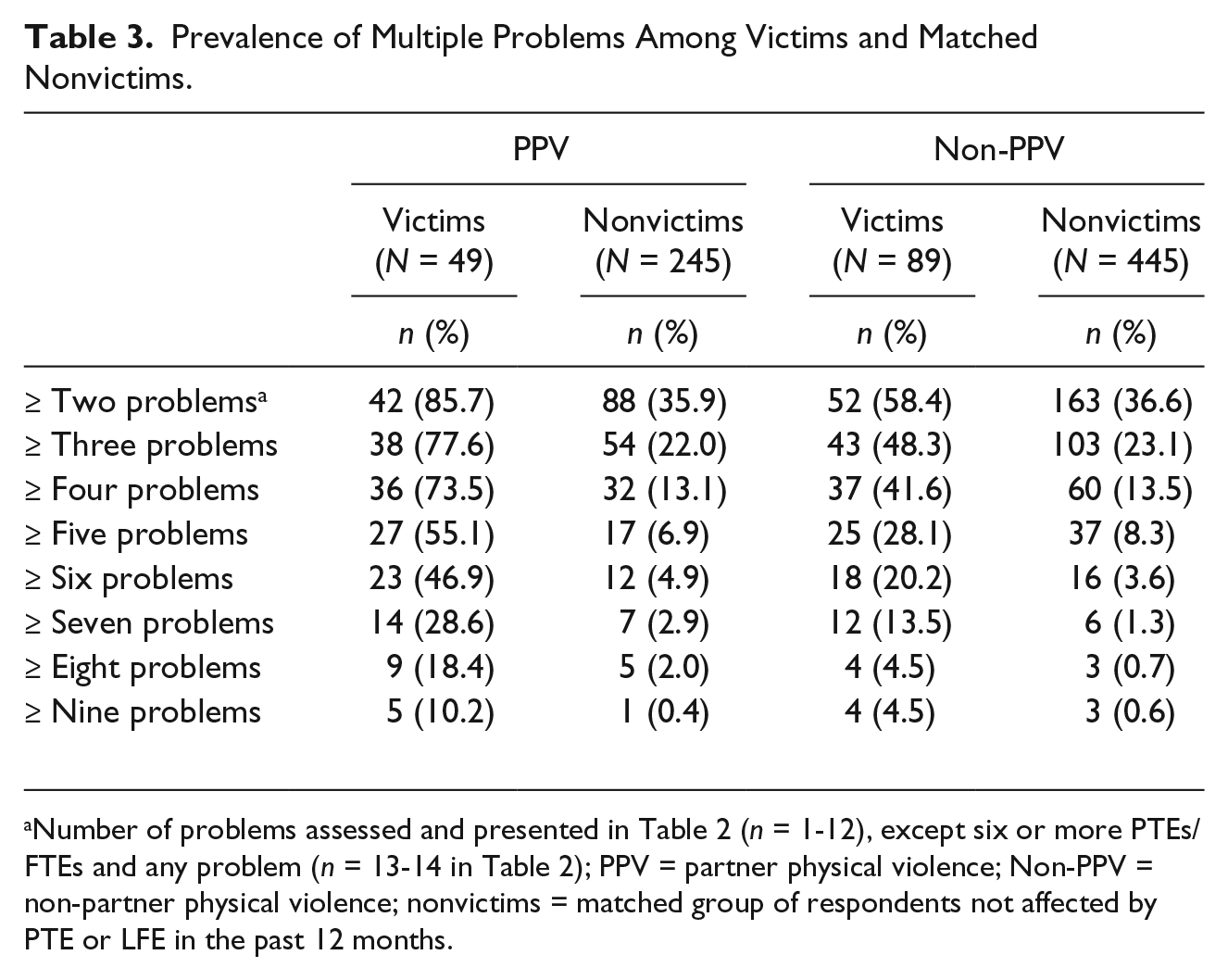
With respect to multiple problems, Table 2 shows that PPV victims more often faced multiple problems (any problem) than matched nonvictims (we excluded problems with partner and experiences with PTE/LFE from the category “any problem,” because of the selection procedure). The mean number of problems among PPV victims and matched nonvictims was 4.96 (SD = 1.72) and 1.48 (SD = 1.85), respectively, t(−57.2) = 8.58, p < .001. The differences in multiple problems between non-PPV victims and matched nonvictims showed a similar but less drastic difference (see Table 2). The mean number of problems (excluding problems with partner and PTE/LFE) among non-PPV victims and matched nonvictims was 2.93 (SD = 2.69) and 1.48 (SD = 1.80), t(104.1) = 4.89, p < .001. Finally, analyses showed that PPV victims more often had any problem than non-PPV victims (OR = 8.19, 95% CI = [1.84, 36.43], p = .006). The mean number of problems among PPV victims (M = 4.96) was higher than among non-PPV victims, M = 2.93, t(98.3) = −4.21, p < .001. In Table 3, the prevalence is presented of multiple problems among the four groups, starting with the prevalence of having two or more problems among each group. As described, for the pairwise matching, we selected nonaffected respondents at random. To rule out the possibility that findings can be attributed to a specific single randomization of the selected respondents for the matched comparison groups, we repeated all analyses using three new randomization rounds. Reanalyses showed minimal differences.
Prevalence of Multiple Problems Among Victims and Matched Nonvictims.
Discussion
Aim of the present population-based study was to assess the prevalence of multiple problems among victims of PPV and non-PPV compared with pairwise matched groups not exposed to traumatic events or LFEs in the past 12 months. The results showed a very clear but drastic pattern: Victims of PPV faced many problems besides the partner violence and may be considered a multiproblem group (cf. Adams et al., 2013; Dias et al., 2018; Jordan, 2004; Schwab-Reese et al., 2016; Showalter, 2016; Tarrezz Nash et al., 2013). The prevalence of each of the distinct problems among victims of PPV was significantly and much higher than among the matched nonaffected comparison group. Thirty-seven percent were exposed to six or more PTEs or stressful LFEs in the past 12 months (excluding partner violence). The mean number of distinct problems was 5.0 versus 1.5 among the PPV victims and comparison group and the prevalence of five or more problems was 55% versus 7%, respectively. A similar but somewhat less drastic pattern was found when comparing the prevalence of the problems among victims of non-PPV and the matched nonaffected comparison group. With respect to demographic characteristics of the victims, results showed that PPV and non-PPV were prevalent among all age categories, among women and men, employed, and unemployed (cf. NIPSVS; Black et al., 2011). As could be expected, PPV victims more often had problems with family/partner, than non-PPV victims. They also more often had physical, financial, administrative, and legal problems; more often lacked social support; and were more often exposed to six or more traumatic LFEs in the past 12 months. PPV victims reported a significantly higher number of problems than non-PPV victims. Contrary to our expectations, both victim groups did not differ in the prevalence of mental health problems. We have no clear explanation for this finding and can only speculate about the cause. However, one explanation could be some kind of “ceiling effect”: after a certain number of problems or stressors, mental health problems among PPV victims (and perhaps other victims) do not further increase when victims are confronted with other or new problems above existing problems. For example, it could be that when victims suffer from physical, work, and legal problems, the likelihood that they suffer from mental health problems does not increase when they, besides physical, work, and legal problems, also start to suffer from financial problems. In sum, non-PPV victims had more problems and multiple problems than nonvictims, and PPV victims had more problems and multiple problems than non-PPV victims and nonvictims: PPV victims face a drastic accumulation of problems, also compared with victims of non-partner violence. We are not aware of any comparative empirical study to compare our findings with.
Limitations and Strengths
Larger samples of PPV and non-PPV victims would have enabled further analyses among, for instance, men and women, younger and older adults, and victims (not) receiving or searching for professional help. In addition, we did not examine other forms of partner violence such as psychological violence and economic abuse (Azam Ali, Dhingra, & McGarry, 2016; Bagwell-Gray, Messing, & Baldwin-White, 2015). We have no information about to what extent, assessed problems were already (partly) present before the events, and have no information about partner violence in the years before the year prior to the surveys. In addition, we did not collect data on the perpetrator of PPV and, as a result, do not know how multiple problems relate to dyadic forms of PPV, whereas previous research has shown that a substantial amount of PPV is part of dyadic violence (e.g., Babcock, Snead, Bennett, & Armenti, 2019; Kessler, Molnar, Feurer, & Appelbaum, 2001). Previous research on perpetrators convicted of PPV has shown that, like victims, these perpetrators experience multiple problems (van der Knaap, el Idrissi, & Bogaerts, 2013), and in terms of preventing recurring PPV, it may prove useful to further assess these relationships in future research. The sample size of the victim groups did not permit comparisons between male and female victims of PPV with respect to the prevalence of separate and multiple problems. Future research on these potential differences is warranted. Future research on these potential differences, including other forms of partner violence and abuse, as assessed by, for instance, the International Violence Against Women Survey (IVAWS), as well as on subgroups that are more at risk is warranted. It was outside the aim of the present study to examine conducted preventive measures for PPV and non-PPV victims. For preventive measures against partner violence, we refer to Ellsberg et al. (2015); de Koker, Mathews, Zuch, Bastien, and Mason-Jones (2014); the reports of the WHO (2010); and the Centers for Disease Control and Prevention (CDC; Niolon et al., 2017). Nevertheless, a major strength of the present study is that results are based on a large representative population-based study with a high response rate and pairwise matched nonaffected comparison groups.
Practical Implications
As expected, PPV victims run a high risk of multiple problems compared with a nonaffected matched group. In their systematic review, Shorey, Tirone, and Stuart (2014) provided a comprehensive overview of the possible individual components of a coordinated community response for victims of intimate partner violence. Although their review is especially aimed at intimate partner violence against women, it is unlikely that the described components (advocacy, criminal justice system, child services, counseling, vocational, education and media, health care) are not of relevance too for male victims of PPV as well. For the description of the components and description of the results of empirical studies aimed at these components, we, therefore, refer to their systematic review. Our results showed that many PPV victims had financial, administrative, and legal problems, which may not necessarily be related to the criminal justice system or vocational component. In addition, our study shows that administrative problems, although not assessed in previous studies, were as prevalent as legal problems. We, therefore, suggest that a multidisciplinary coordinated community response should include the assessment of financial, administrative, and legal problems among victims, apart from these two components (cf. Klein, Chesworth, Howland-Myers, Rizo, & Macy, 2021). In addition, a large proportion of PPV victims reported a lack of emotional support in response to problems, a lack of appreciation support, and a lack of a listening ear. It can be expected that all components, although in different ways, will contribute to an increase of emotional and appreciation support, and a listening ear (besides offering a supportive voice). However, in most cases, family and friends are the main sources of support for victims (as for nonvictims in normal life). We, therefore, would like to suggest that a coordinated community response includes interventions to assess and help to restore forms of social support provided by family and friends. In either way, findings with respect to the multiple problems of PPV victims as well as the results of previous research on the effects of partner violence strongly stress the necessity of multidisciplinary coordinated community response to target problems PPV victims are faced with. It is likely that when professionals such as police officers, physicians and nurses, financial experts, and governmental social agencies act together, the chance that multiproblems can be solved will increase.
Finally, although this study focused on multiple problems among PPV victims victimized in the past 12 months, the results with respect to non-PPV victims are of relevance too. As could be expected, given the results of numerous studies on the effects of violence on mental health (cf. Kessler et al., 2017), victims of physical violence more often had mental health problems and specific depression and anxiety symptoms than matched nonvictims. We are not aware of population-based studies using matched nonvictims as comparison groups, examining differences in all areas of functioning as assessed in the present study. However, results showed that non-PPV victims compared with matched nonvictims more often had physical, financial, administrative, and legal problems; problems with partner/family, work, and religion; lack of appreciation and emotional support, and having any problem. In general, these problems were significantly less prevalent than among PPV victims but still significantly more prevalent than among nonvictims. These findings clearly suggest that victim support for victims of non-PPV should also screen for problems among victims in these areas because these problems may hinder or complicate recovery and, therefore, should be addressed. For instance, a substantial minority lacked social support and/or had problems with the partner/family, suggesting that social relationships, an important resource for mental health and well-being according to Hobfoll’s conservation of resources theory (Hobfoll, 1989, 2002), were deterred among these victims. Victims support could further serve these victims by interventions to restore these relationships as much as possible.
Footnotes
Appendix
If you think about your experiences in the past 12 months, were you confronted with one of more of the following drastic or stressful events?
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the Victims in Modern Society (VICTIMS) study, granted by the Victim Support Foundation (Fonds Slachtofferhulp, FSH), the Netherlands.