
Abstract
Sexual abuse is a major public health concern with detrimental effects on both mental and physical health. Several studies have reported that victims of sexual abuse have a decreased ability to recognize risk in potentially threatening situations compared with nonvictims, although others were not able to replicate this finding. In addition, although emotion dysregulation has been linked to risk perception and sexual victimization, results have been contradictory. To strengthen the theoretical framework needed for the development of interventions to reduce women’s likelihood of sexual assault, it is crucial to further examine the role of emotion dysregulation in relation to sexual victimization history and risk perception. The aim of the current study was to examine cross-sectional associations between sexual victimization, emotion regulation difficulties, and risk perception. In our sample of 276 female college students, 40% reported lifetime sexual victimization, 14% reported recent sexual victimization, and 12% reported childhood sexual abuse. In contrast to our hypothesis, we did not find risk perception to be related to lifetime sexual victimization, childhood sexual victimization, or recent sexual victimization. In addition, we did not find evidence for the expected relationship between sexual victimization, risk perception, and emotion regulation difficulties. The discussion of the current study specifically highlights the need for a clear conceptualization of risk perception and provides recommendations for future studies. More sophisticated measurement methods could lead to a higher applicability of findings to real-life situations. The potential relationships between victimization, risk perception, and emotion dysregulation need further clarification to reach the ultimate goal of contributing to the prevention of victimization.
Introduction
Sexual abuse is a major public health concern with detrimental effects on mental and physical health (Chen et al., 2010; Maniglio, 2009). Although sexual abuse affects both men and women, the current research focuses exclusively on women, who are more likely to experience sexual violence compared with men (Breiding, 2014). In childhood, global prevalence rates of sexual abuse are estimated at 18.0% in girls, compared with 7.6% in boys (Stoltenborgh, Van, Ijzendoorn, Euser, & Bakermans-Kranenburg, 2011). In a large cohort of 17-year-old girls in the United States, 26.6% had experienced lifetime sexual abuse (Finkelhor, Shattuck, Turner, & Hamby, 2014). Across all age groups, young adult women aged between 18 and 24 years have a disproportionally high risk of becoming victims of sexual violence (Sinozich & Langton, 2014). Research in college samples has documented prevalence rates of unwanted sexual contact ranging from 1.8% to 34%, with most studies reporting rates over 20% (see Fedina, Holmes, & Backes, 2018 for a review). Although the blame of sexual abuse lies solely with the perpetrator, it is important to study systemic structures and victim characteristics as well, to better understand the complex set of factors contributing to sexual violence. Understanding why some women are more vulnerable to become a victim of sexual abuse compared with others can contribute to the development of interventions aimed at increasing women’s resilience and reducing the likelihood of sexual assault.
Studies have consistently reported that victims of childhood or adolescent sexual abuse are at increased risk for revictimization in adulthood (Classen, Palesh, & Aggarwal, 2005; Walker, Freud, Ellis, Fraine, & Wilson, 2019). In a longitudinal study, Gidycz, Coble, Latham, and Layman (1993) showed that women with a history of rape or attempted rape in adolescence were almost twice as likely to become victim of a sexual assault during college compared with other women. A meta-analysis of sexual revictimization across various female samples (i.e., student, clinical, and population samples) reported an overall Cohen’s d effect size of .59 for sexual revictimization (Roodman & Clum, 2001). A recent meta-analysis in both female and male victims of child sexual abuse found the mean prevalence of sexual revictimization to be 47.9% (Walker et al., 2019). In an attempt to explain the relation between a history of sexual abuse and subsequent revictimization, a growing body of research has described the process of risk perception: The ability to perceive risk in potentially threatening situations (see Gidycz, McNamara, & Edwards, 2006 for a review).
Risk Perception
Several studies have reported that victims of sexual abuse have a decreased ability to perceive risk in potentially threatening situations compared with nonvictims (e.g., Neilson et al., 2018; Soler-Baillo, Marx, & Sloan, 2005; Walsh, DiLillo, & Messman, 2012); however, other studies were not able to replicate this finding (e.g., Carlson & Duckworth, 2016; Chu, DePrince, & Mauss, 2014; Vanzile-Tamsen, Testa, & Livingston, 2005). The operationalization and assessment of risk perception varied considerably across studies (see Gidycz et al., 2006 for a review).
Most empirical studies on risk perception have used vignette methodology, in which participants first listen to or read a scenario describing a hypothetical interaction and are asked to indicate to what extent they consider the situation as risky or threatening (see Rinehart & Yeater, 2015 for a review). A frequently used measure of risk recognition is the audiotaped vignette developed by Marx and Gross (1995). The vignette describes a hypothetical interaction between a man who increasingly uses coercion and a woman who persistently refuses, which eventually culminates in a date rape (Marx & Gross, 1995). Participants are asked to stop the tape when they believe the man has “gone too far.” In an early, retrospective study among college women, multiple-incident victims demonstrated longer response latencies than nonvictims and single-incident victims, suggesting delays in risk recognition (Wilson, Calhoun, & Bernat, 1999). In another retrospective study that used the same audiotaped vignette, university women with a history of adolescent or adult sexual victimization had longer response latencies than women without a history of sexual victimization (Soler-Baillo et al., 2005). Contrarily, a study that attempted to replicate these findings in a community sample did not find a difference between victims and nonvictims in risk perception (Chu et al., 2014). Other studies have used largely similar written or videotaped vignettes in which participants are asked to rate how risky a situation is (see Rinehart & Yeater, 2015 for a review). Yeater, Treat, Viken, and McFall (2010) found an association between victimization history and impaired risk perception, whereas others did not (Breitenbecher, 1999; VanZile-Tamsen et al., 2005). Yet another study found better risk perception in participants who were victimized multiple times compared with single-incident victims (Yeater & O’donohue, 2002). In summary, these studies have provided mixed results regarding impaired risk perception in victims of sexual abuse.
Other studies on risk perception have used written or videotaped vignettes in which participants are asked to indicate at which moment in the scenario they would leave the situation. This so-called leave score represents a somewhat different conceptualization of risk perception, which is more related to responding to perceived threat, instead of perceiving the threat (Walsh et al., 2012). Messman and Brown (2006) developed the Risk Perception Survey (RPS): A written vignette consisting of two scenarios—one with a male acquaintance and the other with a male stranger—that gradually become more risky and end in forced sexual intercourse. Participants are instructed to imagine themselves interacting with the man in the scenario and to indicate when they would leave the situation. In their study among university women, victims of adult sexual victimization reported leaving both scenarios later than both nonvictims and victims of child sexual victimization only. Moreover, women who reported leaving the acquaintance scenario later at baseline were more likely to report having been victimized during the 8-month follow-up period (Messman & Brown, 2006). Correspondingly, a recent study found that female college students with a history of adolescent or adult sexual assault reported leaving the acquaintance scenario of the RPS later than students without a history of sexual assault (Neilson et al., 2018). In contrast with these results, however, other studies found no association between victimization history and leaving the acquaintance scenario later (Carlson & Duckworth, 2016; Eshelman, Messman, & Sheffer, 2015). One study suggested that leave scores may be relevant only to substance-related victimization (i.e., victimization when unable to give consent or resist due to alcohol or drugs), which was positively correlated with leaving the scenario later—as opposed to forcible assault (i.e., victimization when being threatened or physically forced; Eshelman et al., 2015).
Emotion Dysregulation and Risk Perception
Although results remain mixed, studies have provided some evidence to support a relationship between sexual victimization and decreased risk perception. In an attempt to further explain this association, researchers have examined the role of emotion regulation in this relationship (Carlson & Duckworth, 2016; Walsh et al., 2012). Emotion regulation involves (a) the awareness and understanding of emotions, (b) acceptance of emotions, (c) the ability to control impulsive behaviors and to behave in accordance with desired goals, and (d) the ability to use situationally appropriate emotion regulation strategies to modulate emotional responses to meet individual goals and situational demands, as described by Gratz and Roemer (2004). In their theoretical model, Marx, Heidt, and Gold (2005) described the putative role of emotion regulation and risk recognition in the association between childhood sexual abuse and adult revictimization. The authors argued that childhood sexual abuse elicits emotion dysregulation difficulties (e.g., unsuccessful attempts to regulate fear or arousal and avoidance of aversive emotional states) and theorized that these difficulties may in turn impair one’s ability to recognize risk cues and to adequately defense oneself, thereby increasing one’s vulnerability to future revictimization (Marx et al., 2005).
To our knowledge, only two previous studies have examined the associations between sexual victimization, emotion dysregulation, and risk perception, and their results are mixed (Carlson & Duckworth, 2016; Walsh et al., 2012). Walsh et al. (2012) explored these associations in a large sample of female college students (N = 714). First, they found a weak but statistically significant correlation (r = .09) between lifetime sexual victimization and risk perception as measured with the leave score in the acquaintance scenario of the RPS. Second, they found weak but significant correlations between these variables and most aspects of emotion dysregulation (all r ≤ .15), as measured with the Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004). Third, they found that the correlation between lifetime sexual victimization was partly explained by limited access to emotion regulation strategies and impulse control problems. In line with the model proposed by Marx et al. (2005), the authors suggest that victims who experience these emotion regulation difficulties may be focused on their emotional state to such an extent that they fail to detect environmental risk cues (Walsh et al., 2012). However, a more recent study found contradictory results. Carlson and Duckworth (2016) also examined the association between victimization history (defined as no victimization history, one victimization experience, and two or more victimization experiences), emotion dysregulation, and risk perception in a sample of 113 female college students. In contrast to previous studies (Messman & Brown, 2006; Walsh et al., 2012), the authors found no association between victimization history and the leave scores of both scenarios of the RPS. Victimization history was significantly correlated with emotion dysregulation (r = .35). Furthermore, emotion dysregulation was significantly correlated with the leave score of the RPS stranger scenario (r = –.23), but not the acquaintance scenario. Remarkably, their results indicate that women with higher levels of emotion dysregulation left the stranger scenario earlier than women with lower levels of emotion dysregulation, which contrasts the results of Walsh et al. (2012) regarding the acquaintance scenario.
The Current Study
In summary, previous studies on the association between sexual victimization history and risk perception have reported mixed results. Hence, it remains unclear whether sexual victimization is related to risk perception. In addition, although emotion dysregulation has been linked to victimization (Carlson & Duckworth, 2016; Messman, Ward, & Zerubavel, 2013; Walsh et al., 2012), results have been contradictory in terms of the direction of association between emotion dysregulation and risk perception. It is crucial to further examine the role of emotion dysregulation in relation to sexual victimization history and risk perception, to strengthen the theoretical framework needed for the development of interventions to reduce women’s likelihood of sexual assault. Therefore, the current study aims to examine the associations between sexual victimization—differentiating between lifetime, recent, and childhood sexual abuse—emotion regulation difficulties, and risk perception, as measured with the leave score of the RPS acquaintance scenario (Messman & Brown, 2006). In line with Walsh et al. (2012), we hypothesized that lifetime sexual victimization would be positively associated with both emotion regulation difficulties and the leave score. Furthermore, we hypothesized that emotion regulation difficulties would be positively associated with the leave score.
Method
Design and Procedures
This cross-sectional study was conducted at the Vrije Universiteit Amsterdam, the Netherlands, in collaboration with the research department of Arkin Mental Health Care, Amsterdam, the Netherlands. The data collection took place in April and May 2017. College students were recruited by research assistants through flyers posted on campus, Facebook, and online research recruitment platforms. All participants provided written informed consent prior to participation. Participants completed a set of self-report questionnaires administered in Net-Q: an online secured survey platform. Each assessment was supervised by one of two research assistants (MSc or BSc) and took approximately 45 min. Participants were compensated with €10 or 50-min course credit.
Participants
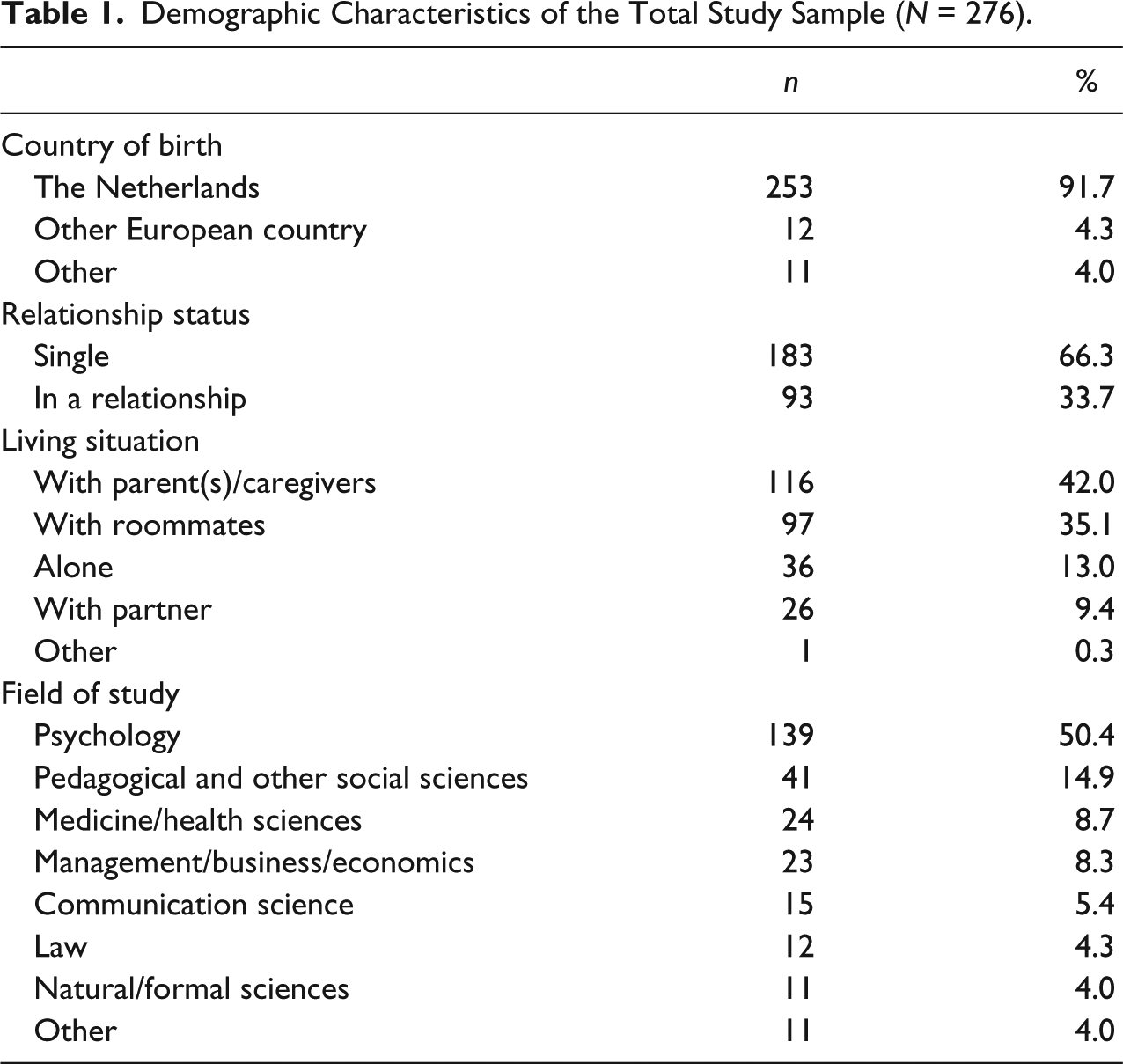
The inclusion criteria were as follows: being female, being currently studying in the Netherlands, and having sufficient understanding of the Dutch language to understand and complete self-report questionnaires. The study sample consisted of 276 female college students with a mean age of 21.7 years (SD = 2.38). As shown in Table 1, participants were predominantly born in the Netherlands (91.7%), single (66.3%), living with their parents (42.0%) or with roommates (35.1%), and studying psychology (50.4%).
Demographic Characteristics of the Total Study Sample (N = 276).
Measures
Lifetime, recent, and childhood sexual victimization
Lifetime sexual victimization and recent sexual victimization were measured with a subset of questions from the section “sexual assault” of the Safety Monitor: a survey that is developed by the Dutch Ministry of Security and Justice (Akkermans, Coumans, Kloosterman, Linden, & Moons, 2013). The Safety Monitor is the Dutch equivalent of the International Crime Victims Survey (ICVS; Killias, 2010) and is used by Statistics Netherlands to measure victimization on a large scale. There are no psychometric properties available. In the Safety Monitor, sexual assault is explained as being touched or grabbed, with sexual intentions, in an offensive way. Participants were asked to indicate whether this had ever happened to them to measure lifetime sexual victimization (yes/no). Recent sexual victimization was defined as having experienced a sexual assault in the 12 months preceding the assessment. The Safety Monitor does not provide scores to determine the severity of victimization experiences. More detailed questions were used for descriptive purposes only. In line with Walsh et al. (2012), sexual victimization was operationalized dichotomously.
Childhood sexual abuse (CSA) was measured with the CSA subscale of the Dutch version of the Childhood Trauma Questionnaire–Short Form (CTQ-SF; Bernstein et al., 2003; Thombs, Bernstein, Lobbestael, & Arntz, 2009). The CTQ-SF is a self-report questionnaire with items that are rated on a 5-point Likert-type scale with response options ranging from “Never true” to “Very often true.” Originally, the CSA subscale consisted of 5 items; however, previous psychometric analyses of the Dutch version indicated that one item of the CSA subscale (i.e., “During my youth, I was molested by someone”) had to be removed in the Dutch version of the questionnaire (Thombs et al., 2009). The sum score of the CSA scale was calculated as the sum of the four remaining items, multiplied by 5/4. The CTQ-SF manual provides several cut-off scores to describe the presence/absence of abuse, sensitive to different levels of abuse severity. Cut-off scores specifically for the Dutch version of the CTQ-SF have not yet been developed. In the current study, the cut-off score of >6 was used to indicate presence of CSA. This cut-off score corresponds best to the English CTQ-SF as presence of sexual abuse is indicated when a participant answers affirmatively on at least one of the sexual abuse items. Validity and reliability of the Dutch version of the CTQ-SF are good (Spinhoven et al., 2014; Thombs et al., 2009). In the current study, internal consistency was excellent for the CSA scale (α = .91).
Emotion dysregulation
Emotion dysregulation was measured with the Dutch version of the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004; Neumann, van Lier, Gratz, & Koot, 2010). The DERS is a 36-item self-report questionnaire that evaluates emotion regulation difficulties across multiple domains. The DERS showed high internal consistency and good test–retest reliability in a U.S. student sample (Gratz & Roemer, 2004). In the current study, all six subscales were used, which showed good to excellent internal consistency: nonacceptance of emotional responses (α = .89), difficulties engaging in goal-directed behavior (α = .87), impulse control difficulties (α = .87), lack of emotional awareness (α = .81), limited access to emotion regulation strategies (α = .90), and lack of emotional clarity (α = .84).
Risk perception
Risk perception was measured with the Risk Perception Survey (RPS; Messman & Brown, 2006). The RPS is a written vignette describing a college party scene that culminates in forced rape by an acquaintance. The vignette consists of 25 statements that become progressively riskier and include both clear (sexual comments, verbal persuasion) and ambiguous (alcohol consumption, physical isolation) risk factors for sexual victimization. Each statement is presented sequentially on a computer. Participants are instructed to imagine that they are participating in each activity as described and to press a button indicating one of four possible responses: (a) continue in the scenario, (b) uncomfortable and continue in the scenario, (c) leave the scenario, and (d) uncomfortable and leave the scenario. The primary variable in the analyses is the leave score, which is defined as the statement (screen) in the scenario at which the participant indicated she would leave the scenario—regardless of whether or not she indicated feeling uncomfortable. Hence, for women who chose to complete the entire scenario, a leave score of 26 was assigned. The display of the scenario was terminated when a participant had indicated to leave the scenario. For the purpose of this study, the RPS was translated into Dutch, with permission of the authors. To obtain conceptual equivalence, three researchers independently translated the statements into Dutch and formed a panel to resolve discrepancies in these forward translations. Subsequently, an independent, professional translator translated the statements back into English. One of the researchers discussed discrepancies with the translator until consensus was reached.
Ethics
The study was reviewed and approved by the ethics committee of the Vrije Universiteit Amsterdam, The Netherlands (VCWE-2017-009R1). Participation in the study was voluntary, and all participants provided written informed consent.
Statistical Analyses
Data were analyzed using SPSS Statistics 24.0. There were no missing values. Pearson correlations and point-biserial correlations were used to examine associations between lifetime sexual victimization (yes/no), recent sexual victimization (yes/no), CSA (yes/no), emotion regulation difficulties (continuous), and the outcome measure: the leave score (continuous). Computing the point-biserial correlation between one dichotomous and one continuous variable, for example, lifetime sexual victimization (yes/no) and the leave score, is equivalent to comparing two groups in an independent t test with a continuous dependent variable.
Results
Victimization Rates and Characteristics
Approximately, 40% of the sample (n = 111) reported lifetime sexual victimization, and approximately, 14% of the sample (n = 38) reported sexual assault in the year preceding the assessment. Of the women who reported past year sexual assault, 47% (n = 18) reported that it had occurred once in the past year, 26% (n = 10) reported that it had occurred twice, and 26% (n = 10) reported that it had occurred between 3 and 10 times. Approximately, 58% of the victims of past year sexual assault (n = 22) reported assault by a stranger only, 29% (n = 11) reported assault by an acquaintance only, and 13% (n = 5) reported assault by a stranger as well as assault by an acquaintance in the past year. Approximately, 47% of the victims of past year sexual assault (n = 18) reported to have experienced assault only while being under the influence of alcohol and/or drugs, 32% (n = 12) reported to have experienced assault only while being sober, and 21% (n = 8) reported to have experienced assault both while being under the influence of alcohol and/or drugs and while being sober.
Approximately, 12% of the sample (n = 32) reported CSA. For women reporting CSA, the mean CTQ sexual abuse score was 11.2 (SD = 5.1), which falls within the moderate range of sexual abuse severity. Of the 38 women who reported past year sexual assault, 8% (n = 3) reported CSA.
Mean scores for each of the DERS subscales ranged from 10.7 (SD = 4.4) for lack of emotional clarity to 16.8 (SD = 6.4) for limited access to emotion regulation strategies, which is consistent with DERS scores observed among a U.S. sample of female college students (Gratz & Roemer, 2004).
On average, participants reported that they would leave the scenario at the 13th screen (SD = 6.8), which corresponds to the portion of the vignette when the man invites the participant to go with him to his apartment. The modal screen that participants left on was 9 (n = 53), which corresponds to the portion of the vignette when one of the participant’s friends gets sick at the party and the rest of the friends decide to take her home. This corresponds to the modal screen observed in Walsh et al. (2012). Other screens at which relatively many participants decided to leave the scenario were the 10th screen (n = 30), which corresponds to the portion of the vignette when the participant’s friends are leaving and agree to come back for the participant later, and the 13th screen (n = 29), which is described at the beginning of this paragraph. Approximately, 10% of the sample (n = 28) chose to continue all the way through the scenario, until the portion of the vignette when the participant tries to push the man off, but he has sexual intercourse with her.
Bivariate Associations Between Victimization, Emotion Dysregulation, and Risk Perception
As shown in Table 2, all three measures of sexual victimization—lifetime sexual victimization, recent sexual victimization, and CSA—were not significantly associated with leaving the risk vignette later (the leave score). The mean leave score for victims of lifetime sexual victimization (n = 111) was 13.4 (SD = 7.3), and the mean leave score for nonvictims (n = 165) was 12.5 (SD = 6.5). For both groups, the modal screen that participants left on was 9. The mean leave score for victims of recent sexual victimization (n = 38) was 13.5 (SD = 7.2), and the mean leave score for women without past year sexual victimization (n = 238) was 12.7 (SD = 6.8). The mean leave score for victims of CSA (n = 32) was 15.0 (SD = 7.9), and the mean leave score for women without history of CSA (n = 244) was 12.6 (SD = 6.6). Furthermore, lifetime sexual victimization, recent sexual victimization, and CSA were not significantly associated with any of the types of emotion regulation difficulties, except for a weak negative association between lifetime sexual victimization and limited access to emotion regulation strategies (rpb = –.13). Finally, the leave score was weakly negatively correlated with impulse control difficulties (r = –.12) and was not significantly correlated with any of the other types of emotion regulation difficulties.
Correlations Between Sexual Victimization, Emotion Dysregulation, and Leave Score in Female College Students (N = 276).
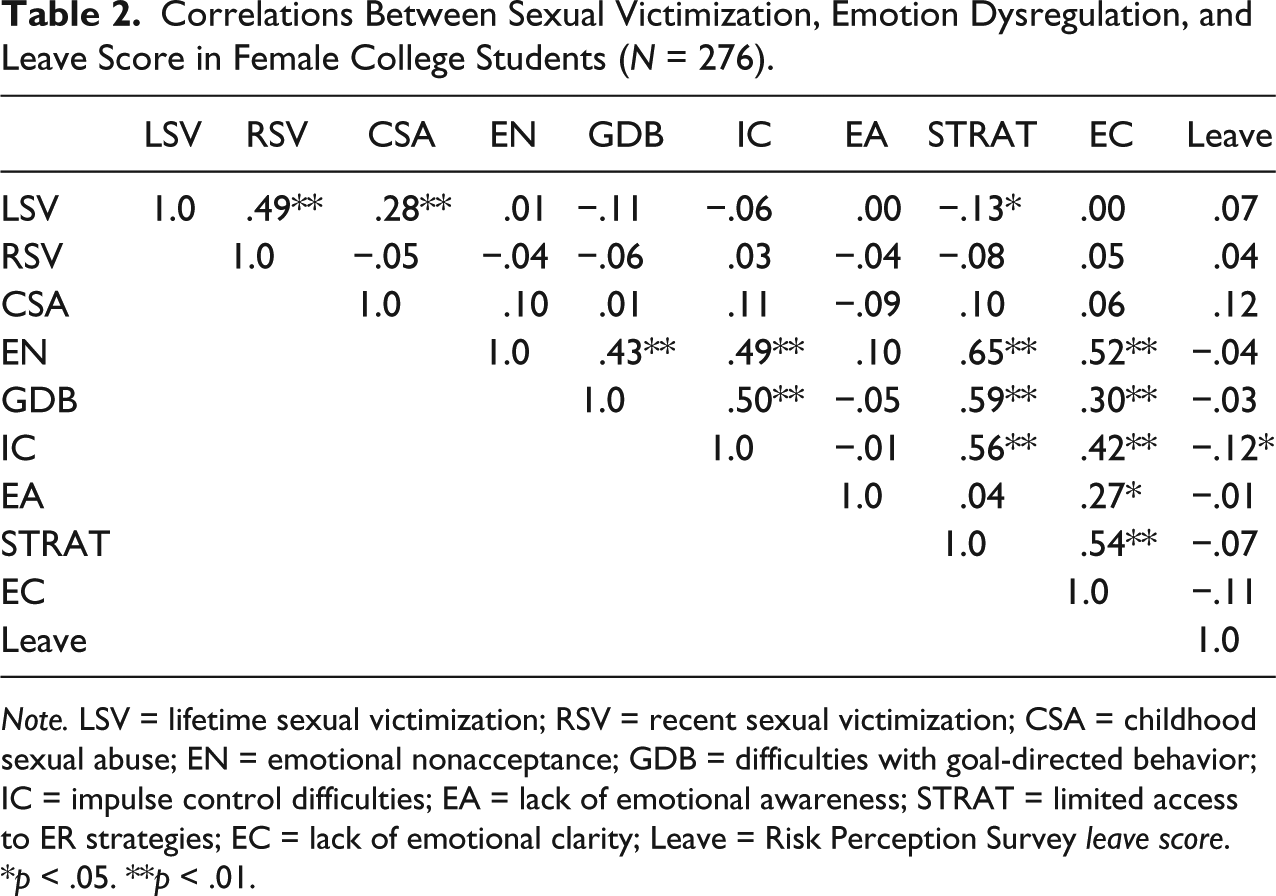
Note. LSV = lifetime sexual victimization; RSV = recent sexual victimization; CSA = childhood sexual abuse; EN = emotional nonacceptance; GDB = difficulties with goal-directed behavior; IC = impulse control difficulties; EA = lack of emotional awareness; STRAT = limited access to ER strategies; EC = lack of emotional clarity; Leave = Risk Perception Survey leave score.
p < .05. **p < .01.
Discussion
In a sample of female college students, 40% reported lifetime sexual victimization, 14% reported recent sexual victimization, and 12% reported CSA, which largely corresponds to previous studies on prevalence of sexual victimization in young adult women (Fedina et al., 2018; Gidycz, Hanson, & Layman, 1995; Stoltenborgh et al., 2011). In contrast to our hypothesis, we did not find an association between lifetime sexual victimization and risk perception. In addition, we did not find risk perception to be related to childhood sexual victimization or recent sexual victimization.
These findings are in contrast with an earlier study by Walsh et al. (2012), in which lifetime sexual victimization was associated with impaired risk perception. There are several possible explanations for this discrepancy. One explanation is that no meaningful relationship exists between sexual victimization history and impaired risk perception. The observed correlation in Walsh et al. (2012) was very weak (r = .09), generally similar to the correlation observed in the current study (r = .07), and may have been statistically significant due to a relatively large sample size (N = 714) compared with ours (N = 276). Earlier studies have provided mixed results: Although several studies have found evidence for the existence of a relationship between sexual victimization history and impaired risk perception (Neilson et al., 2018; Soler-Baillo et al., 2005; Walsh et al., 2012; Wilson et al., 1999; Yeater et al., 2010), a considerable amount of others studies have not (Breitenbecher, 1999; Carlson & Duckworth, 2016; Chu et al., 2014; VanZile-Tamsen et al., 2005). Moreover, one study even reported improved risk perception in participants who were victimized multiple times compared with single-incident victims (Yeater & O’donohue, 2002). Studies that provide evidence for an association between victimization and risk perception may be overrepresented in the literature due to publication bias: The tendency for authors to submit and for editors to accept a study for publication based on the direction or strength of its findings (Dickersin, 1990). If publication bias is present, researchers could currently be overestimating the probability of a relationship between victimization and risk perception.
Another explanation for the inconsistency of findings could be the varying ways in which risk perception is conceptualized and measured. Although some studies, including ours, examined when a participant would leave a situation (Carlson & Duckworth, 2016; Neilson et al., 2018; Walsh et al., 2012), others have asked participants when they would feel on guard or uncomfortable in a situation (Breitenbecher, 1999; Messman & Brown, 2006) or have asked participants to explicitly identify risk factors or the degree of risk depicted in vignettes (VanZile-Tamsen et al., 2005; Yeater & O’donohue, 2002). As outlined in the introduction, indicating when one would leave a scenario is more related to responding to perceived threat, instead of perceiving the threat, and thus includes a decision-making process based on perceived risk cues. Remarkably, a recent study that used the same risk perception vignette as the current study was unable to confirm the expected association between the perceived likelihood of incapacitated sexual assault and the decision to leave a situation (Neilson et al., 2018). This suggests that women may be able to perceive risk cues but may decide to continue through the scenario due to other concerns, such as worries about ruining the relationship with the man or other psychological barriers (Norris, Nurius, & Dimeff, 1996). This highlights the urgent need for a clear, theory-driven conceptualization of risk perception and the cognitive processes involved. However, the mixed findings cannot be fully explained by differences in conceptualization and measurement methods as studies that used the same measurement instruments have also found contradictory results (Carlson & Duckworth, 2016; Neilson et al., 2018; Walsh et al., 2012).
The inconsistency of findings could also be explained by differences in the measurement and operationalization of sexual victimization. In most studies mentioned, including the current study, sexual victimization by definition included physical contact between the perpetrator and the victim. The majority of studies incorporated the Sexual Experiences Survey (SES; Koss & Gidycz, 1985); however, many studies used a self-modified version and/or combine the SES with other questionnaires to construct a variable sexual victimization, operationalized as a dichotomous variable (Soler-Baillo et al., 2005; Walsh et al., 2012), categorical variable (e.g., no victimization, single incident, or multiple victimization; Carlson & Duckworth, 2016; Chu et al., 2014; Wilson et al., 1999), or continuous variable based on severity (Neilson et al., 2018; VanZile-Tamsen et al., 2005; Yeater et al., 2010). The dichotomous variable used in the current study does not differentiate between relatively mild forms of sexual assault, such as being groped, and severe forms, such as being raped. Studies combining such heterogeneous experiences of sexual assault into one variable may yield different results than studies using a measure of severity. As with risk perception measures, however, the mixed findings cannot be fully explained by differences in measurement and operationalization of sexual victimization as studies using similar operationalizations have also reported contradictory results. It is not always clear why authors chose a specific operationalization of sexual victimization. In future studies, researchers should operationalize their study variables a priori, and ideally even register them, to prevent information bias and increase reliability.
In contrast to our hypothesis and previous research (Carlson & Duckworth, 2016; Messman et al., 2013; Walsh et al., 2012), we did not find evidence for the expected relationships between CSA, recent or lifetime sexual victimization, and emotion regulation difficulties. Furthermore, we did not find evidence for the expected relationship between emotion regulation difficulties and impaired risk perception. These results do not correspond with the theoretical model proposed by Marx et al. (2005), who hypothesized that victims of CSA develop emotion regulation difficulties and, consequently, become less able to recognize risk cues. Our findings are also inconsistent with those found in the study of Walsh et al. (2012) among college women in the United States. Although differences between women from Europe and women from the United States could be assumed to have influenced the results, there was no indication of a cross-cultural difference: Both the emotion dysregulation scores and the modal leave score were highly similar in both samples. The inconsistent results may be explained by the difference in sample size as the observed correlations in their study were all weak (all r ≤ .15) and may have reached statistical significance due to the large sample size. Our findings are partly in line with a recent study in a U.S. sample by Carlson and Duckworth (2016), which was also unable to detect an association between emotion dysregulation and leaving an increasingly risky scenario involving a male acquaintance. Carlson and Duckworth (2016) did report an association between emotion dysregulation and leaving a “stranger scenario,” but in the opposite direction of Walsh et al. (2012): Women with higher levels of emotion dysregulation left the scenario earlier.
In summary, the current study found no evidence for relationships between sexual victimization, emotion dysregulation, and risk perception. Although absence of evidence should not be interpreted as evidence of absence, our findings reflect the inconsistent results of previous research. Overall, it remains unclear whether a relationship between sexual victimization and risk perception exists. With regard to the potential role of emotion regulation in this relationship, results of scarce previous research are particularly contradictory.
Future studies are needed to clarify these mixed findings in the literature, which should use improved and theory-driven assessment of risk perception. Unexplored opportunities lie in the use of more sophisticated techniques to measure risk perception and risk response, such as virtual reality. Studies testing the practicing of rape-resistance skills found that interaction with a virtual aggressor is realistic enough to trigger an emotional response and made participants feel more emotionally involved compared with when the same scenario is played with an actor (Jouriles et al., 2009; Jouriles, Rowe, McDonald, Platt, & Gomez, 2011). Presenting a risky situation in a virtual environment may prompt a more realistic reaction and thus result in a more valid measure of risk perception and risk response compared with a written or audiotaped vignette as it does not depend on participants’ ability to imagine a situation and then forecast one’s own behavior (Jouriles et al., 2011). In addition, virtual reality enables more flexibility as scenarios can be easily updated to reflect current language and trends in college women’s social and dating experiences and to incorporate potential new insights into risk cues. A recent study by Loranger and Bouchard (2017) showed that an experiment in which a participant is sexually assaulted in a virtual environment is tolerated by participants, also by those who have been victims of sexual assault in the past. None of the participants mentioned having been overly troubled by the experiment or needing postexperiment support, indicating that virtual reality can be safely used. Virtual reality has successfully been used in experiments examining women’s responses in sexually threatening situations (Jouriles et al., 2011) and negative consequences of intervening as a bystander in risky situations (Krauss et al., 2021). As virtual reality equipment is becoming more affordable, the potential of using it to measure risk perception and risk response should be further explored.
Limitations
The current study added to the sexual victimization literature by examining associations that demonstrated highly mixed findings in previous studies, in a European sample. Several limitations of the current study should be addressed in future studies. First, as participants were predominantly born in the Netherlands, were all well-educated, and were predominantly studying psychology, findings are not necessarily applicable to young women in general. Replication of the current study in a more diverse sample of women would increase the generalizability of the findings. Second, future studies should inquire about sexual orientation. Possibly, the risk perception vignette has less validity for lesbian women compared with heterosexual or bisexual women. Third, we did not examine risk perception in a stranger scenario, whereas 58% of the victims of past year sexual assault reported assault by a stranger only, and a previous study reported distinct findings for a stranger and acquaintance scenario (Carlson & Duckworth, 2016). Finally, as sexual victimization was operationalized as a dichotomous variable, we were unable to make statements about the severity of the incidents. The associations of sexual victimization with risk perception and emotion dysregulation may differ between relatively mild forms and severe forms of sexual assault. Future studies should differentiate between these forms of sexual assault, to measure their specific impact on mental health, risk perception, and emotion regulation.
Conclusion and Recommendations
Results of the current study indicate that it is yet unclear whether the proposed relationships between sexual victimization, risk perception, and emotion dysregulation exist, and if they do, in what direction. This study specifically highlights the need for a clear conceptualization of risk perception. In addition, more sophisticated measurement methods, such as virtual reality, could potentially lead to a higher applicability of findings to real-life situations.
Understanding why some people are more vulnerable to be victimized compared with others is particularly important as it can contribute to the development of interventions aimed at reducing the likelihood of victimization. Enhancing emotion regulation skills is an important component of two recently developed interventions aimed at reducing risk of victimization in another vulnerable group: people with mental illness (Christ et al., 2018; de Waal, Kikkert, Blankers, Dekker, & Goudriaan, 2015). Although emotion dysregulation has been linked to victimization (Carlson & Duckworth, 2016; Messman et al., 2013), it remains yet unclear whether impaired risk perception is involved in this relationship. The potential relationships between victimization, risk perception, and emotion dysregulation need further clarification to reach the ultimate goal of contributing to the prevention of victimization.
Footnotes
Acknowledgements
The authors thank all students for their participation in this study, and Iris van Kuijk and Willemijn van Ginneken for her contribution to the data collection. We also thank the Royal Netherlands Academy of Arts and Sciences for the opportunity to collaborate with Miami University in Oxford, Ohio, USA.
Authors’ Note
Marleen M. de Waal and Carolien Christ contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.M.d.W. and C.C. received a Van der Gaag Grant of the Royal Netherlands Academy of Arts and Sciences (KNAW) for this study. This research was also funded by grants from the Netherlands Organization for Scientific Research (NWO), within the program “Violence Against Psychiatric Patients” (grant number: 432-12-804, awarded to J.J.M.D, and grant number: 432-13-811, awarded to A.T.F. Beekman). T.L.M.-M. received funding from the O’Toole Family Professor endowment. The funding agencies had no role in the planning of the study design; the collection, analysis, and interpretation of the data; the writing of the manuscript; and the decision to submit the article for publication.