
Abstract
Mother–child dialogues about children’s emotional experiences are associated with children’s adaptive coping with stressful situations and mental health. Despite these findings, dialogues have not been examined yet in the context of child sexual abuse. This gap is surprising given that mother–child dialogues may particularly promote children’s recovery from traumatic events. The current exploratory study examined the quality of mother–child emotion dialogues, as well as the quality of child and maternal contributions to dialogues, among dyads with sexually abused children (n = 30; 60% female; M age = 8.03), as compared with dyads with nonabused children (n = 30; 60% female; M age = 8.20). Quality of dialogues was assessed using the Autobiographical Emotional Events Dialogue. Mothers reported on their own childhood maltreatment history and psychopathological symptoms. Results showed that dyads with abused children were more likely to engage in overwhelming/excessive dialogues and dialogues lacking content, as compared with dyads with nonabused children. After controlling for differences in background characteristics, mothers of abused children showed lower sensitive guidance. Although mothers of abused children had more experiences of childhood maltreatment and higher levels of psychopathology, they did not add to explain group differences in maternal sensitive guidance. Our findings suggest that the ability to discuss emotional experiences may be impaired among mother–child dyads with sexually abused children. This may be an important target in the treatment of sexually abused children and their families.
Keywords
Child sexual abuse (CSA) is associated with myriad negative short- and long-term mental health outcomes among victims, such as depression and anxiety (e.g., Cutajar et al., 2010; Maniglio, 2009; Trickett, Noll, & Putnam, 2011). A growing body of evidence, however, suggests that a supportive, sensitive, and responsive parent may attenuate and even protect children from the harmful effects of abuse (for reviews, see Elliott & Carnes, 2001; Yancey & Hansen, 2010). A key aspect may be mothers’ ability to support and guide abused children while discussing children’s emotional experiences. These mother–child emotion dialogues have been overlooked in CSA research so far. This gap in the literature is surprising, because high quality mother–child emotion dialogues are considered to facilitate children’s understanding of stressful experiences and their associated negative emotions, thereby contributing to children’s coping with these experiences (Liable & Panfile, 2009; Oppenheim, 2006). The present exploratory study sought to examine the quality of mother–child emotion dialogues in a sample of mothers and their sexually abused children.
Research indicates that mother–child emotion dialogues play a crucial role in children’s emotional development (Fivush, Haden, & Reese, 2006; Laible, Murphy, & Augustine, 2013; Laible & Song, 2006). Mother–child emotion dialogues are considered to shape children’s developing self-understanding (Fivush, 2007; Fivush, Berlin, Sales, Mennuti-Washburn, & Cassidy, 2003). Participating in parent-guided conversations about their emotional experiences helps children acquiring meaning making skills; they learn how to evaluate, interpret, and organize their emotional experiences (Fivush, 2007; Fivush et al., 2003). More specifically, children learn how to define themselves as an emotional person, how to express and share emotions with others, and how to cope with and resolve negative emotions (Fivush et al., 2003). Furthermore, high quality emotion dialogues may help children see their mother as a secure base from which to safely explore their emotional world (Koren-Karie, Oppenheim, Haimovich, & Etzion-Carasso, 2003b).
Mother–child emotion dialogues may be of critical importance for children who experienced highly stressful events, such as CSA. Support of the importance of dialogues in the context of trauma can be derived from research into the effectiveness of trauma-focused cognitive behavioral therapy (TF-CBT; Cohen, Mannarino, & Deblinger, 2006), of which a core component is having children develop a narrative about their traumatic experiences. Research shows that TF-CBT is particularly effective in reducing adjustment problems among sexually abused children (Deblinger, Mannarino, Cohen, Runyon, & Steer, 2011; Mannarino, Cohen, Deblinger, Runyon, & Steer, 2012). In addition, studies among adults suggest that the quality of narratives of stressful events is associated with psychological adjustment (Liable & Panfile, 2009). Adults who are able to meaningfully and coherently integrate these emotional experiences into their memory have higher well-being. Thus, creating a coherent narrative of the trauma may be critical in adjustment after trauma. Younger children typically lack the necessary cognitive and emotional skills to create narratives on their own and may thus particularly rely on their parents to develop a coherent trauma narrative (Fivush, 2007). Therefore, it may be that mothers who support, guide, and encourage their child while discussing CSA experiences facilitate the development of a coherent trauma narrative, thereby enhancing children’s meaning making of the traumatic event and promoting children’s recovery (Fivush, 2007; Oppenheim, 2006).
Only few studies examined whether variations in quality of parent–child emotion dialogues are associated with children’s adjustment following stressful events. Two studies showed that mothers who were more engaged, expressed more emotions, and provided more explanations during emotion dialogues about a chronic stressor (managing asthma) had children who showed more flexible coping (Fivush & Sales, 2006) and lower levels of emotional difficulties (Sales & Fivush, 2005). Surprisingly, these associations were not found in mother–child dialogues about acute trauma (a trip to the emergency room because of an asthma attack). A more recent study showed that maltreating mothers were less elaborative during mother–child emotion dialogues, which mediated the association between child maltreatment experiences and developmental outcomes (Valentino et al., 2015). These studies provide preliminary evidence of the possible importance of mother–child emotion dialogues for children’s recovery from traumatic experiences.
Despite the suggested importance of mother–child emotion dialogues, they have not been studied among sexually abused children. The study of Valentino et al. (2015) only included four CSA victims, and all mothers in this study were perpetrators of maltreatment. Yet, the quality of mother–child emotion dialogues may be particularly at risk among dyads with sexually abused children. First, mothers of sexually abused children often exhibit high levels of psychopathology (e.g., depression, anxiety) following disclosure of their child’s CSA (Cyr, McDuff, & Hebert, 2013; Elliott & Carnes, 2001; Hebert, Daigneault, Collin-Vezina, & Cyr, 2007). Parental psychopathology is a risk factor for lower parental availability (e.g., Visser, Schoemaker, de Schipper, Lamers, & Finkenauer, 2016) and lower observed emotional availability (sensitivity, nonhostility, and nonintrusiveness) (Easterbrooks, Biesecker, & Lyons-Ruth, 2000; Easterbrooks, Bureau, & Lyons-Ruth, 2012). Thus, it may be that higher levels of psychopathology among mothers of abused children reduce maternal sensitivity and availability as a partner in conversations in mother–child emotion dialogues.
Second, there is a high incidence of childhood maltreatment experiences among mothers of sexually abused children (e.g., Finkelhor, Moore, Hamby, & Straus, 1997; Robboy & Anderson, 2011). Although research revealed mixed results, most studies showed that maternal childhood maltreatment is associated with negative observed parenting behavior. For example, abused mothers had higher levels of observed hostility toward their children than mothers who had not been abused (Bailey, DeOliveira, Wolfe, Evans, & Hartwick, 2012). Consistent with these results, preliminary research suggests that mother–child dyads show lower quality emotion dialogues when mothers have not resolved childhood traumatic experiences (Koren-Karie, Oppenheim, & Getzler-Yosef, 2008). Talking about highly emotional themes may trigger negative emotions associated with mothers’ past experiences, which makes it difficult for mothers to separate their emotional reactions to mother–child emotional dialogues from their emotional experiences in the past (Koren-Karie et al., 2008). This may interfere with abused or traumatized mothers’ ability to regulate, organize, and contain their child’s negative emotional experiences. Similarly, this mechanism may also be present in sexually abused children. Trauma symptoms may cause abused children to experience difficulties in showing co-operation during emotion dialogues. For example, emotion dialogues may trigger memories of their abuse experiences and associated emotions, which may cause them to withdraw from the dialogue or show resistance to talk about emotions.
Finally, CSA may damage children’s perception of the mother as a secure base where they can seek safety and comfort (Lieberman, 2004). In line with this suggestion, research indicates that sexually abused children feel less safe and less comfortable expressing and sharing their emotions in the mother–child relationship than children who had not been abused (Shipman, Zeman, Fitzgerald, & Swisher, 2003; Shipman, Zeman, Penza, & Champion, 2000). This may cause sexually abused children distress during emotion dialogues with their mothers and prevent open communication about emotional experiences.
Taken together, the literature highlights the importance of studying mother–child emotion dialogues among dyads with sexually abused children. Insights in these dyadic processes may reveal essential and promising targets in the treatment of sexually abused children to enhance children’s recovery from and coping with CSA experiences.
To our knowledge, the present study is the first to examine the quality of mother–child emotion dialogues among dyads with sexually abused children. To fully capture both child and maternal quality of contributions to dialogues, as well as dyadic aspects of dialogues, we used the Autobiographical Emotional Events Dialogue (AEED; Koren-Karie, Oppenheim, Haimovich, & Etzion-Carasso, 2003a). Our first aim was to compare the quality of mother–child emotion dialogues between dyads with sexually abused children and dyads with nonabused children. We examined maternal and child contributions to dialogues, as well as the dyadic quality of mother–child emotion dialogues. We hypothesized that mothers and their abused children would have lower quality dialogues than mothers and their nonabused children. Our second aim was to explore associations between maternal psychopathology and maternal childhood maltreatment, on one hand, and quality of maternal and child contributions to dialogues on the other. We expected that both higher levels of psychopathology and having had childhood maltreatment experiences would be associated with lower quality of contributions.
Method
Participants
Participants were 30 nonoffending mothers and their sexually abused children (aged 4-13 years; M = 8.03, SD = 2.72; 60% female) and a control group of 30 mothers and their nonabused children (aged 4-13 years; M = 8.20, SD = 2.94; 60% female). As part of a larger (treatment) study, mothers and children in the CSA group were recruited from four outpatient treatment centers in the Netherlands specialized in childhood trauma (for full information about the sample and recruitment procedures, see Van et al 2015). Children were recruited during intake and were referred by Dutch Youth Care Agencies (in Dutch: Bureau Jeugdzorg), general practitioners, or mental health care professionals. Practitioners identified cases that included children aged 4 to 16 years who experienced (or were suspected of having experienced) sexual abuse. Statements about CSA were deemed highly credible by the practitioners who did the intake and diagnostic assessments.
Mothers and children in the control group were recruited from Dutch primary schools and through the social network of research assistants. Control dyads were excluded when the mother reported that the child experienced (or was suspected of having experienced) sexual abuse or a severe traumatic event, as indicated on the Parent Report Traumatic Impact (Friedrich, 1997) (i.e., two children who witnessed a shooting in which people were killed were excluded).
Furthermore, mothers and children in both groups were excluded when mother or child had an intellectual disability (IQ score below 70), and when mother or child were unable to complete the measures due to the inability to read or speak Dutch. For the purpose of the current study, we further selected children aged 4 to 13 years, because the AEED (Koren-Karie, Oppenheim, Haimovich, & Etzion-Carasso, 2003a) has not been used in older children. Also, we excluded children who were placed in foster care after experiencing CSA. Demographic characteristics of participants in the CSA and control group are presented in Table 1. Mother–child dyads in the CSA group and control group were matched on children’s gender and age, and did not differ in maternal ethnicity (Fisher’s exact; p = 1.00). However, mothers in the CSA group were significantly more likely to be a single-parent, χ2(1) = 6.65, p = .01; have lower levels of education (Fisher’s exact = 20.75, p < .001); and have a lower family income, χ2(1) = 12.27, p = .002, than mothers in the control group.
Demographics by Group.
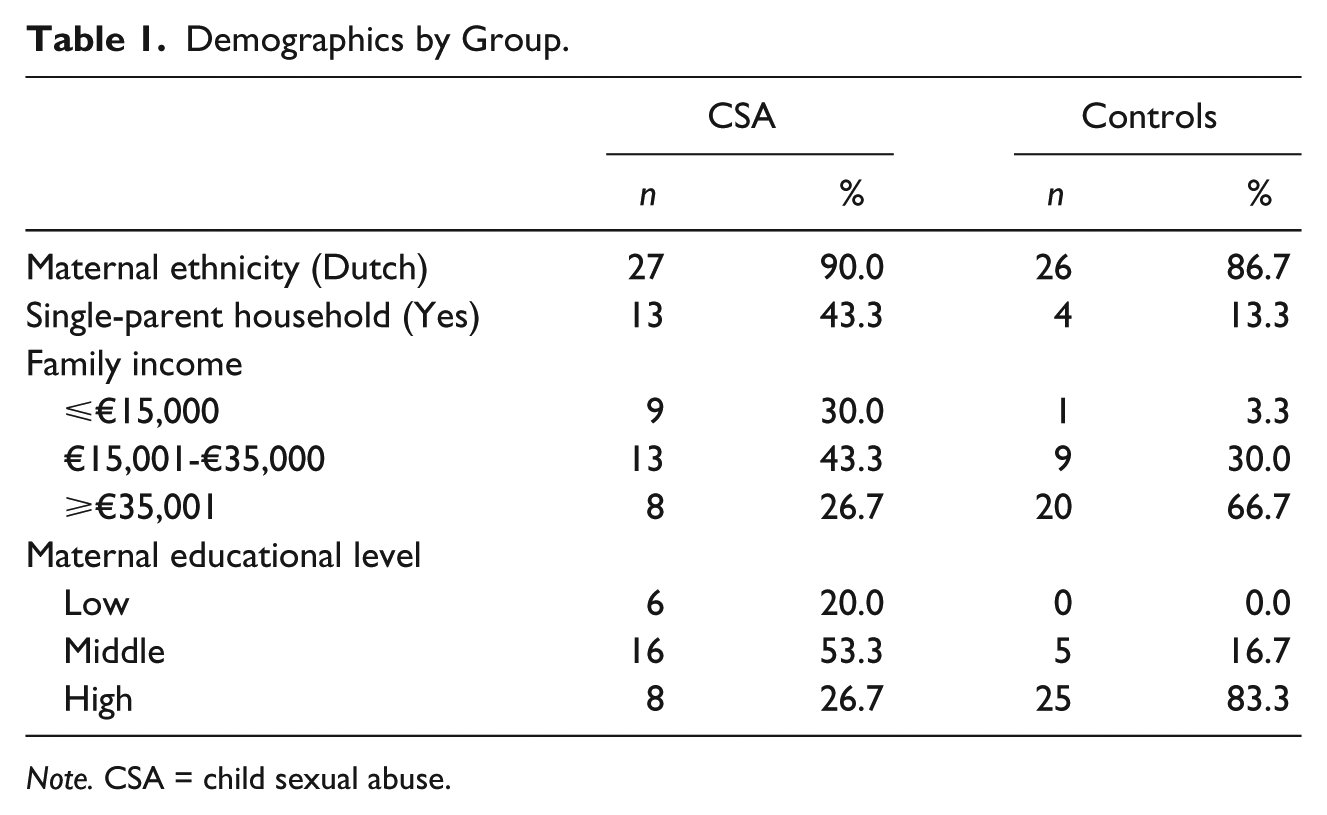
Note. CSA = child sexual abuse.
Procedure
Mothers in the CSA group were introduced to the study by a practitioner during intake, whereas mothers in the control group were introduced to the study by a teacher or research assistant. Mothers received an information letter and consent form and gave permission to be contacted by a researcher to provide further information. Mothers and adolescents older than 12 years provided informed consent for participating in the study. Participants in the CSA group also gave consent for access to the children’s treatment files. The Dutch law requires both custodial parents to consent to children participating in research. Therefore, we asked the mothers to inform the other parent by giving them an information letter and consent form. The other parent was asked to provide written consent for their child’s participation in the study. Dyads in the CSA group completed measures at the treatment center or during a home visit before the start of treatment. Similarly, mothers and children in the control group completed measures during a home visit or at the University. As a thank you for their participation, mothers received €25, children older than 12 years received a movie voucher of €10, and younger children received a small gift in exchange for participation (e.g., pen, game). The Medical Ethical Committee approved all of the procedures for this study (METc VUmc 2011/407/NL38753.029.11).
Measures
CSA characteristics
Mothers reported on the characteristics of their child’s sexual abuse, in particular, the identity and age of the perpetrator, the frequency of the abuse, and whether the perpetrator lived in the family home at the time of the abuse. Intake information in children’s treatment files was examined to gather information on CSA severity. CSA severity was scored by two independent coders using the Modified Maltreatment Classification System (MMCS; English & the LONGSCAN Investigators, 1997). Severity ranged from 1 (exposure to explicit sexual stimuli or activities) to 5 (forced intercourse or other forms of sexual penetration). Interrater reliability was adequate (Cohen’s Kappa = .72). Coder differences were resolved through discussion.
AEED
During the AEED (Koren-Karie et al., 2003a), mothers and children participated in a reminiscing task, in which they recalled and described autobiographical events during which the child felt happy, sad, angry, scared, and proud. Dyads were presented with five cards, each representing one of these emotions, and asked to discuss children’s emotional experiences. This resulted in five stories in which mothers and children jointly described events and talked about what the child felt, thought, and did during the events. Dyads determined the events they discussed, the order of discussed emotions, and the duration of the dialogue. Dialogues typically lasted between 5 and 15 min, and were videotaped and transcribed verbatim.
Transcripts of dialogues were rated on seven mother and seven parallel child scales and two scales measuring the overall quality of the dialogue. Descriptions of the scales are presented in Table 2. Scores ranged from 1 to 9, with a higher score indicating greater prevalence of the construct (Koren-Karie et al., 2003a). To increase statistical power, two composite scores were computed to assess child and maternal quality of contributions to the dialogues based on the mean score of all child scales (Child Cooperation and Exploration) and all maternal scales (Maternal Sensitive Guidance) (Koren-Karie et al., 2008). Composite scores had adequate internal consistencies (Cronbach’s α = .81 and .73, respectively). Based on these rating scales, mother–child dyads were classified as Emotionally Matched or Emotionally Unmatched (for full details of the classifications, see Koren-Karie et al., 2003a). Unmatched dyads were further categorized in one of three categories (Excessive, Flat, or Inconsistent). The AEED is developed based on (theoretical) discussions in the field of attachment about how the concept of attachment may evolve after infancy and how parent–child interaction dimensions further differentiate when language becomes an important mean for parent–child (emotion) communication to explore the child’s inner world (Koren-Karie, Oppenheim, Haimovich, & Etzion-Carasso, 2003b). As a result, in the AEED, more dimensions of emotion communication are included (i.e., resolution of negative feelings) and the structure of classifications show some similarity with the classification of attachment security (Ainsworth, Blehar, Waters, & Wall, 1978; Main & Solomon, 1990).
Descriptions of AEED Scales.
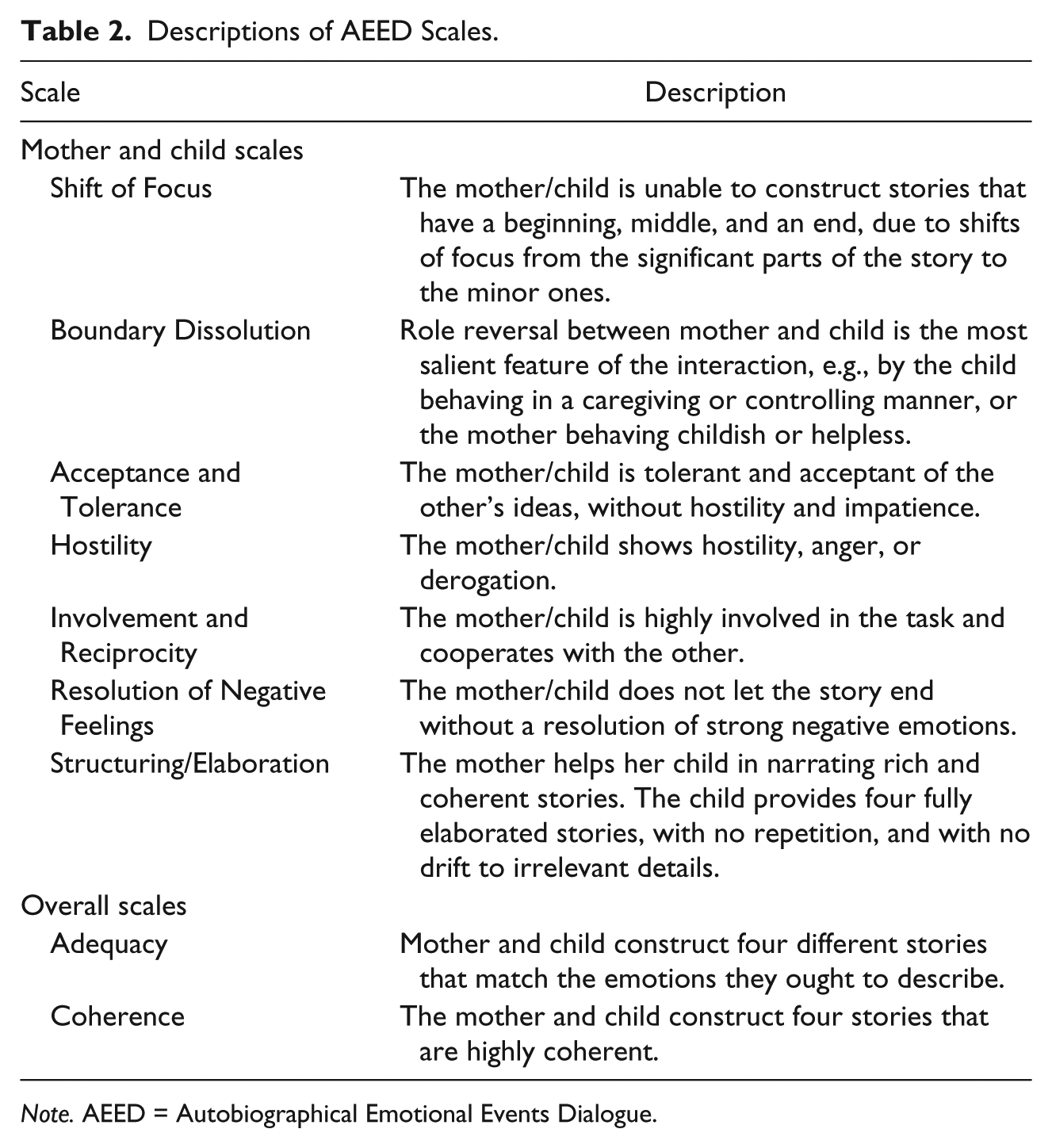
Note. AEED = Autobiographical Emotional Events Dialogue.
Dyads classified as Emotionally Matched are characterized by their capacity to create understandable, appropriate, believable, and structured dialogues about emotional experiences of the child. Mother and child are equally involved in the dialogue, and show patience and acceptance toward each other. Discussions about negative emotions are guided by the mother toward positive endings to contain negative feelings of the child. Overall, the dialogue is coherent and fluent, and the atmosphere is comfortable. Dialogues classified as Emotionally Unmatched Excessive are characterized by incoherence, lack of structure, extreme and negative themes, shifts of focus to irrelevant details, exaggeration, and repetitiveness. The dialogues are confusing, stories are not appropriately closed, and negative feelings remain unresolved. Typically, either the mother or the child dominates the dialogue, and there may be hostile and judgmental dialogue toward the other. Also, mothers often have difficulty following their child’s pace. Dialogues classified as Emotionally Unmatched Flat are characterized by a lack of dialogue and story development. Dialogues are short and the mother does not guide or encourage the child to develop the stories or to express his or her emotions. There is a general lack of interest and involvement and dyads may not be able to complete the task. Dialogues classified as Emotionally Unmatched Inconsistent are characterized by a wide gap in the performance of mother and child across stories. There are three possible patterns within this category. First, mother and child show contradictory patterns of behavior during the dialogue. Second, the behavior of mother and child match only partially during the construction of the stories. Third, either mother or child shows appropriate behavior during one part of the procedure, while showing inappropriate behavior in another part of the procedure.
A trained researcher blindly coded all transcripts, which only revealed information about children’s age and gender. The researcher was trained by the developer of the coding system (N. Koren-Karie) and established adequate reliability. To further improve coding abilities and establish interrater reliability, a subgroup of trained researchers coded transcripts of mothers and their traumatized children using a different sample of our lab, consulted by the developer. Adequate interrater reliabilities were reached for the four classifications (Cohen’s kappa = .80) and the two-way classifications (Emotionally Matched and Emotionally Unmatched; Cohen’s kappa = 1.00). Interrater reliability of the composite scores assessed using intraclass correlations were .95 for Maternal Sensitive Guidance and .95 for Child Cooperation and Exploration.
Maternal childhood maltreatment
The Adverse Childhood Experiences questionnaire (ACEs; Felitti et al., 1998) was used to assess maternal childhood maltreatment. Mothers were asked to report on physical abuse, emotional abuse, sexual abuse, witnessing domestic violence, and emotional and physical neglect during their first 18 years of life. All ACEs were coded following Dong et al. (2004). A dichotomous variable was created with mothers who experienced one or more types of maltreatment coded as 1 and nonabused mothers were coded as 0.
Maternal psychopathology
A short version of the Young Adult Self-Report (YASR; Achenbach, 1997, Dutch translation by Verhulst, Van der Ende, & Koot, 1997) consisting of 29 items was used to assess maternal psychopathology. Earlier research showed that these items discriminated best between referred and nonreferred subjects (Achenbach, 1997). Items were rated on a 3-point scale (0 = not true, 1 = sometimes true, 2 = very true or often true). Mean scores were calculated with a higher score indicating higher levels of psychopathology. Reliability and validity of the Dutch version were found adequate (Wiznitzer et al., 1992). In our study, Cronbach’s alpha was .88.
Statistical Analyses
First, descriptive analyses were conducted to examine CSA characteristics, the incidence of maternal childhood maltreatment, and zero-order correlations among all study-related variables. Second, we conducted a chi-square test and an independent t test to examine whether mothers of CSA victims had higher levels of childhood maltreatment experiences and psychopathology than mothers of nonabused children. Third, we analyzed contingency tables using Fisher’s exact test to examine associations between CSA and AEED classifications. Fourth, a multivariate analysis of variance (MANOVA) was conducted to compare the quality of child and maternal contributions to dialogues (i.e., AEED composite scores) between dyads with sexually abused children and dyads with nonabused children. We controlled for differences in background characteristics between groups to rule them out as confounding variables. Finally, a multivariate analysis of covariance (MANCOVA) was conducted in which maternal childhood maltreatment (maltreated or nonmaltreated) and maternal psychopathology (continuous) were added to the model. The MAN(C)OVAs were followed-up with univariate analyses of variance (ANOVAs) to examine the AEED composite scores of mothers and children separately, using the Bonferroni correction to counteract the problem of multiple comparisons (i.e., threshold for significance was set at .02).
Results
Descriptive Analyses
CSA characteristics
One third of children (36.6%) in the CSA group experienced severe sexual abuse with penetration. One fourth (26.7%) experienced sexual touching and 3.3% were exposed to explicit sexual stimuli or activities, were asked for sexual contact, or were exposed to the genitals of the perpetrator. CSA severity was unknown at the time of intake for 30% of children, and for one child, intake information about CSA severity was not available. Mothers reported at intake that 26.7% of children experienced chronic sexual abuse, and 20% experienced a single occurrence of sexual abuse. Almost half of the mothers (43.3%) did not know the frequency of abuse, and for 10% of the children, mothers failed to give specific information about the abuse. Almost all perpetrators were known to the child (96.7%), with 30.0% being described as father-figures, 26.7% relatives, 40% familiar but unrelated persons, and 3.3% unknown. Most children (63.3%) did not live with the perpetrator at the time of the abuse; one mother failed to answer this question. Also, 70% of the perpetrators were older than 18 years; one mother failed to answer this question.
Zero-order correlations
Bivariate associations among study-related variables are presented in Table 3. Children cooperated and explored more when they were older (p = .02), were female (p = .04), had a nonmaltreated mother (p = .03), had a mother with a higher education level (p < .001), lived in a family with a higher income (p = .03), lived in a two-parent household (p = .003), and had a mother with lower levels of psychopathology (p = .02). Mothers showed higher levels of sensitive guidance when they had a higher education level (p = .001) and a higher family income (p = .03). Mothers who experienced maltreatment reported higher levels of psychopathology (p < .001), had older children (p = .04), had a lower family income (p < .001), and were a single-parent (p = .003). Higher levels of maternal psychopathology were associated with lower levels of family income (p = .02) and education (p = .02). Finally, Child Cooperation and Exploration and Maternal Sensitive Guidance were significantly positively associated (p < .001).
Zero-Order Correlations Among Study-Related Variables.
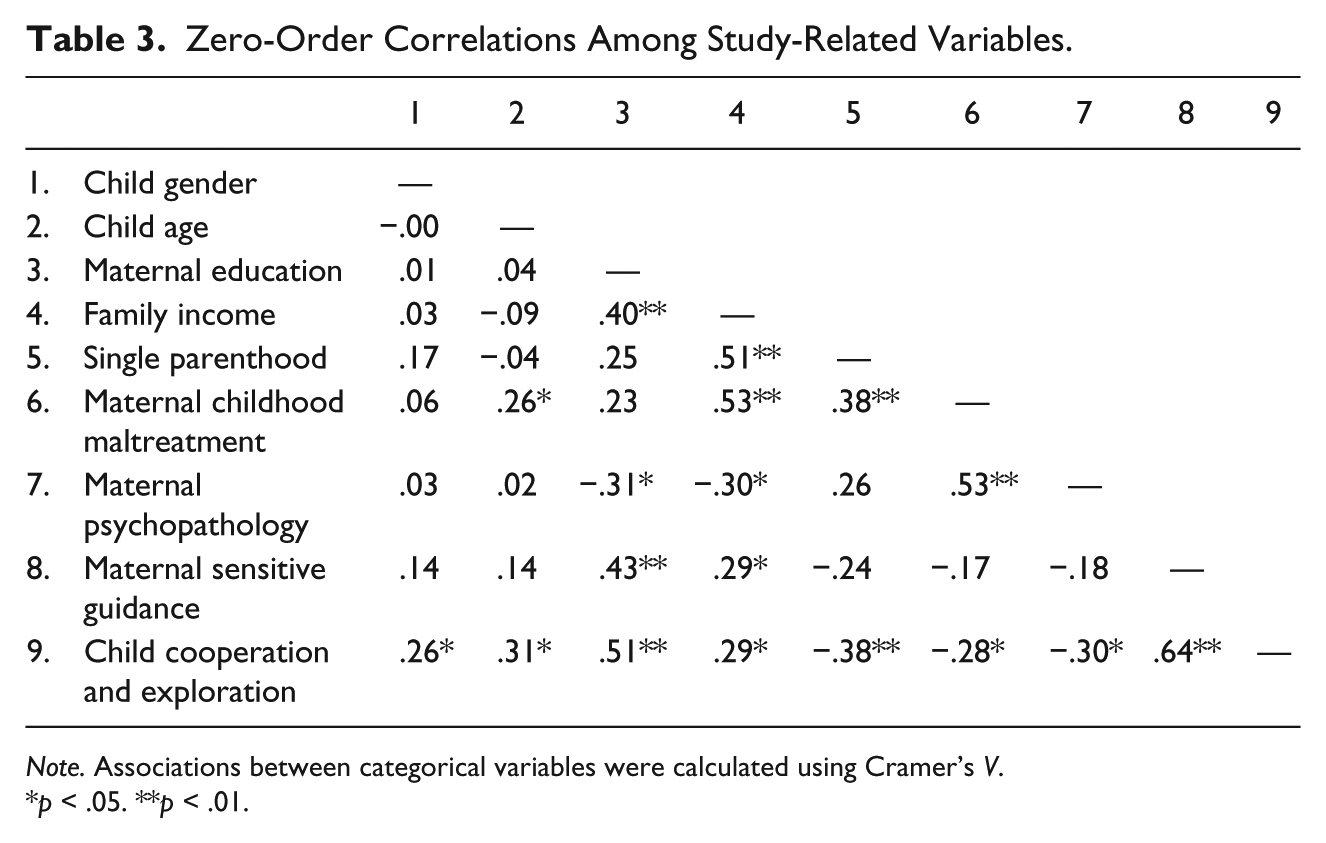
Note. Associations between categorical variables were calculated using Cramer’s V.
p < .05. **p < .01.
Group Differences in Maternal Maltreatment and Psychopathology
Maternal childhood maltreatment
Mothers of abused children were significantly more likely to report having experienced childhood maltreatment than mothers of nonabused children, χ2(1) = 13.13, p < .001. Twenty-one (70%) mothers of sexually abused children reported having experienced maltreatment in childhood, of whom 13 (43.3%) mothers reported two or more types of maltreatment. In the control group, seven (23.3%) mothers reported having experienced childhood maltreatment, of whom three (10%) mothers reported having experienced two types of abuse. The distribution across maltreatment subtypes is presented in Table 4.
Maternal Childhood Maltreatment Subtypes by Group.
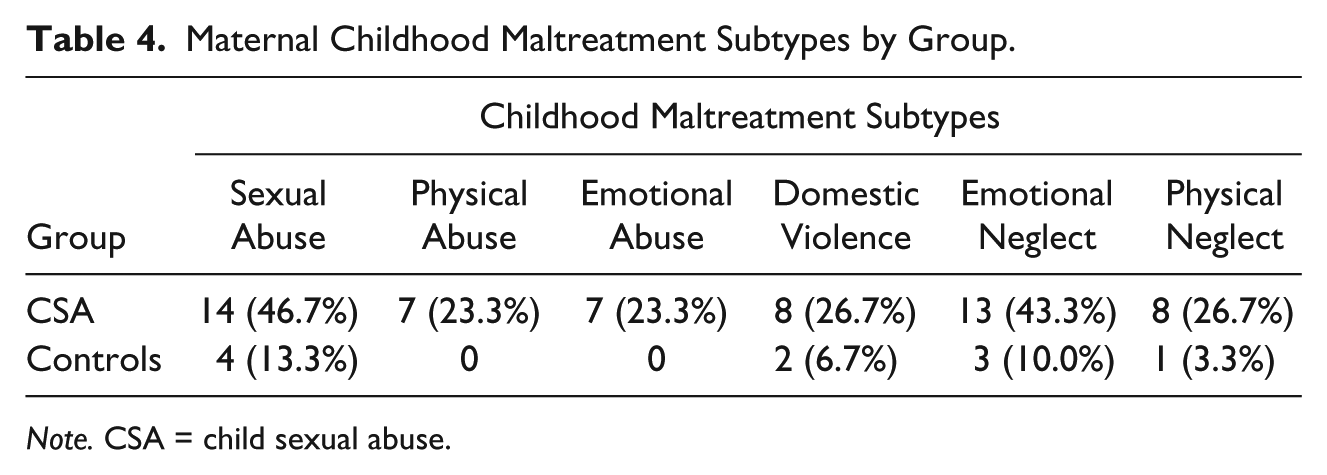
Note. CSA = child sexual abuse.
Maternal psychopathology
An independent t test revealed a significant difference in maternal psychopathology, t(41.48) = 3.90, p < .001, unequal variances, between mothers of abused and nonabused children. Although means were low in both groups, mothers of abused children reported significantly higher levels of psychopathology (M = 0.39, SD = 0.26) than mothers of nonabused children (M = 0.17, SD = 0.15).
Group Differences in AEED Classifications and Composite Scores
AEED classifications
Contingency tables (Table 5) revealed strong associations between CSA and two-way (Emotionally Unmatched or Emotionally Matched) and four-way AEED classifications (Emotionally Matched, Excessive, Flat, or Inconsistent). First, the association between CSA and two-way classifications showed that mothers and their sexually abused children were significantly more likely to be classified as Emotionally Unmatched as compared with mother–child dyads in the control group, χ2(1) = 12.38, p < .001. Fisher’s exact test was used to examine associations between CSA and four-way classifications, because more than 20% of cells had an expected cell frequency lower than five. Sexually abused children were less likely to engage in Emotionally Matched dialogues, and more likely to engage in Flat and Excessive dialogues (Fisher’s exact = 17.63, p = .001).
Group Differences in AEED Classifications.
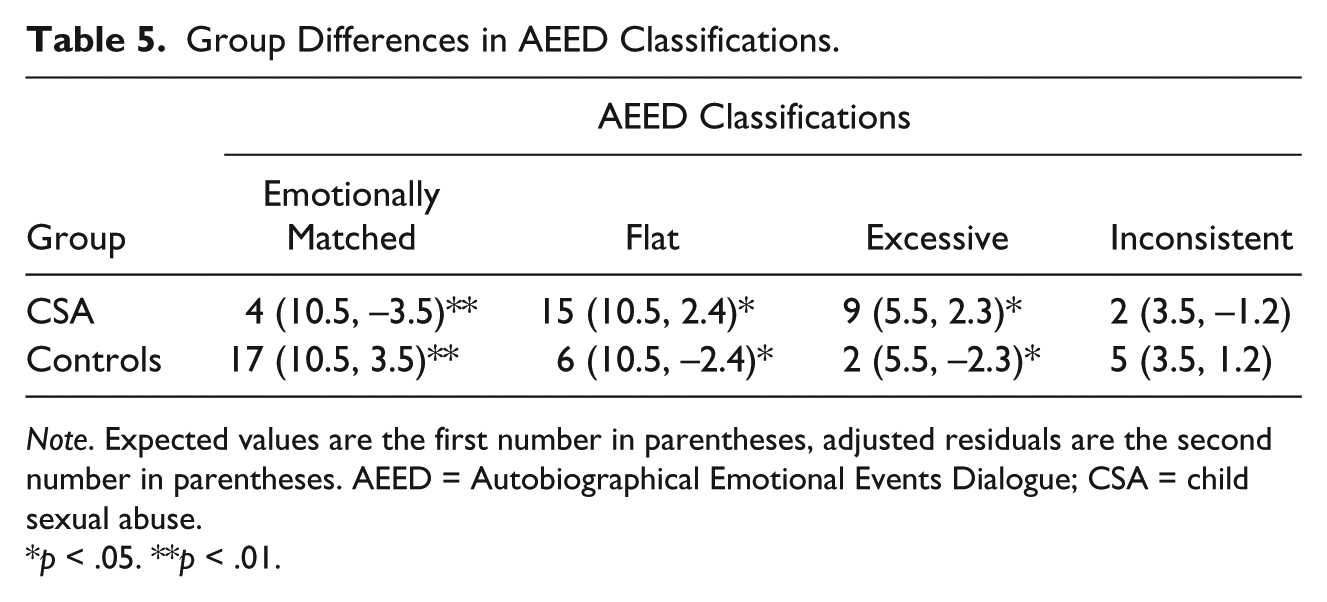
Note. Expected values are the first number in parentheses, adjusted residuals are the second number in parentheses. AEED = Autobiographical Emotional Events Dialogue; CSA = child sexual abuse.
p < .05. **p < .01.
AEED composite scores
An independent t test revealed significant group differences in Maternal Sensitive Guidance, t(58) = 4.47, p < .001, and Child Cooperation and Exploration, t(58) = 4.25, p < .001. Mothers of abused children (M = 5.82, SD = 0.97) showed less sensitive guidance than mothers of nonabused children (M = 6.86, SD = 0.85). Similarly, abused children (M = 5.91, SD = 0.90) showed lower levels of cooperation and exploration than nonabused children (M = 6.83, SD = 0.76).
Multivariate Analyses
AEED composite scores
First, because the groups differed in background characteristics associated with harsh environments (i.e., single parenthood, low maternal education level, and low family income), we examined associations between CSA and AEED composite scores using a MANOVA while controlling for these background characteristics. Maternal education level and family income were transformed into binary variables (0 = low and moderate, 1 = high; 0 = ⩽35,000; 1 = ⩾35,001, respectively) due to low cell frequencies in the low-education (six mothers had a low-education level) and low-income categories (10 mothers had an income lower than 15,000). CSA (abused or nonabused children) emerged as a significant predictor of composite scores, F(2, 53) = 3.19, p < .05,
Second, associations between CSA, maternal childhood maltreatment, maternal psychopathology, and AEED composite scores were examined using a MANCOVA, controlling for maternal education level. Maternal education was included as a background variable in the second analysis, because the p value was .05 and the effect size was equal to the effect size of CSA. Other background variables were excluded from the main analysis to prevent loss of power. Contrary to our hypothesis, the main effects of maternal psychopathology, F(2, 51) = .37, p = .69,
Discussion
This exploratory study aimed to shed light on the quality of mother–child dialogues about children’s emotional experiences among dyads with sexually abused children as compared with dyads with nonabused children. Consistent with our expectations, mothers and their abused children had more difficulties with co-constructing organized, structured, and coherent emotion dialogues. After controlling for differences in background characteristics, mothers of abused children showed lower sensitive guidance. Lower levels of child cooperation and exploration were associated with lower maternal education levels. Contrary to our expectations, maternal psychopathology and maternal childhood maltreatment experiences did not add to explain differences in maternal sensitive guidance between groups. To our knowledge, this is the first observational study to explore mother–child emotion dialogues in CSA victims. Our results add to the limited but growing body of literature examining dyadic processes in the aftermath of CSA.
Specifically, our findings show that mother–child emotion dialogues among dyads with sexually abused children were mostly characterized by a lack of dialogue, that is, they were classified as Emotionally Unmatched Flat (Koren-Karie et al., 2003a). In these dialogues, mothers failed to guide and encourage their children to elaborate on their emotions and both mothers and children showed low levels of involvement and interest. Some mother–child dyads managed to be more elaborative; however, they discussed many extreme and/or negative emotional themes, and were thus classified as Emotionally Unmatched Excessive (Koren-Karie et al., 2003a). These dyads showed high levels of hostility and/or were dismissive of each other’s ideas and feelings. Most important, discussions about negative emotions were not appropriately closed by these dyads and remained unresolved.
These results may have important implications for sexually abused children’s adjustment. Mother–child dialogues may act as a moderator in the association between CSA and mental health (Oppenheim, 2006). On one hand, high quality mother–child emotion dialogues can help children to understand, structure, and cope with stressful experiences and concomitant negative emotions (Fivush, 2007), promoting children’s recovery process. On the other hand, overwhelming mother–child emotion dialogues or dialogues lacking content may hamper children’s meaning making of stressful experiences, thereby increasing abused children’s adjustment problems. Longitudinal studies and studies assessing daily dialogues in everyday conversations are needed to examine this possible moderating role of mother–child emotion dialogues in the development of mental health problems among sexually abused children.
Replicating earlier research, mothers of abused children, as compared with mothers of nonabused children, showed higher levels of psychopathology and had a higher incidence of childhood maltreatment (e.g., Elliott & Carnes, 2001; Finkelhor et al., 1997; Hebert et al., 2007). In contrast to our hypothesis, neither factor explained group differences in quality of contributions to emotion dialogues. The relatively low level of psychopathology in our sample may have prevented us from finding significant associations. Also, Koren-Karie et al. (2008) suggest that posttraumatic stress symptoms and level of resolution of loss and trauma among mothers are more detrimental for mother–child dialogues than general psychopathology levels. Furthermore, we were unable to differentiate between subtypes of maternal childhood maltreatment due to our small sample size and high co-occurrence of subtypes. This differentiation is necessary to fully understand the impact of maternal childhood maltreatment on mother–child emotion dialogues. For example, mothers who experienced physical abuse show more aggressive parenting behavior than sexually abused mothers (Lyons-Ruth & Spielman, 2004). Future studies addressing these issues would be promising.
Our study indicates that in clinical practice, mother–child dyads with sexually abused children may present difficulties in discussing children’s emotional experiences. Although the impact of mother–child emotion dialogues on children’s recovery is yet unknown, improving these dialogues may be a promising target in the treatment of sexually abused children. To date, interventions with a specific focus on strengthening dyads’ abilities to talk sensitively about children’s emotional experiences are lacking. However, child–parent psychotherapy (CPP; Lieberman & Van Horn, 2005) is suggested to improve mother–child emotion dialogues (Oppenheim, 2006). CPP is a relationship-based intervention that aims to change maladaptive parent–child interaction patterns among dyads with traumatized young children (e.g., Lieberman, Van Horn, & Ippen, 2005). For older children, parent–child interaction therapy (PCIT; Hembree-Kigin & McNeil, 1995) may be a useful approach to improve mother’s parenting skills and parent–child interaction in children exposed to trauma (e.g., Timmer, Ware, Urquiza, & Zebell, 2010). Researchers have yet to examine whether improvements in mother–child emotion dialogues is one of the mechanisms through which these treatments may promote children’s recovery.
Some theoretical and methodological issues warrant attention and should be taken into account when interpreting our results. First, our sample was small. Despite this small sample size, we found significant group differences and effect sizes were medium (.0588) to large (.1379) (Richardson, 2011). Nevertheless, the small sample undermines external validity and prevented us from considering other relevant factors such as CSA characteristics (i.e., severity, frequency, and perpetrator). This may be important, because, for example, the quality of mother–child emotion dialogues may be particularly low among children who experienced severe abuse. Future studies should include larger sample sizes.
Second, although our study highlights difficulties in mother–child emotion dialogues among dyads with sexually abused children, more research is needed to examine why and how CSA is associated with lower quality mother–child dialogues. One possible explanation may be that CSA is associated with harsh environments. For example, lower socioeconomic status and single-parent households are common among sexually abused children (e.g., Bebbington et al., 2011; Hussey, Chang, & Kotch, 2006). Although we controlled for these differences in our analysis of AEED composite scores, studies using samples matched on background characteristics are needed to disentangle associations between CSA, harsh environment, and mother–child dialogues.
Third, sexually abused children and their mothers were recruited from outpatient treatment centers. This resulted in only including children and mothers who were in need and sought treatment. Our findings may therefore not be generalized to abused children and mothers who did not need or seek treatment in the aftermath of CSA. Studies are needed that include both children and mothers who did and who did not seek treatment to examine generalizability of our results.
Fourth, we did not differentiate between mother–child dialogues about positive and negative emotional events, nor between dialogues discussing or not discussing (aspects of) children’s sexual abuse. As research suggests that dialogues about negative emotional events are particularly important for child outcomes (Laible, 2011), they may be most relevant to study in the context of CSA. Furthermore, although mother–child dyads use similar approaches when discussing traumatic and nontraumatic events (Bauer, Burch, Van Abbema, & Ackil, 2007; Sales, Fivush, & Peterson, 2003), dialogues about CSA may provide specific insight into how mothers facilitate children’s meaning making of CSA experiences.
Fifth, we did not include fathers in our study. This hampers the generalizability of our findings to the father–child relationship. Previous studies indicated that mothers and fathers have different styles in parent–child dialogues. For examples, fathers were less elaborate and had a more consistent dialogue style across event type than mothers (Fivush, Marin, McWilliams, & Bohanek, 2009). These differences suggest that we may find different results when including fathers.
Finally, observed group differences may reflect differences between children who were exposed to any type of trauma versus children who did not experience a traumatic event. Thus, our results may not be specific for children who experienced sexual abuse. Future studies should consider including children who experienced other types of abuse and/or traumatic events, such as physical abuse, neglect, and witnessing domestic violence.
Despite these limitations, our study is the first to present an in-depth assessment of mother–child emotion dialogues among sexually abused children. Findings provide evidence for a lower quality of emotion dialogues among sexually abused children, as well as a lower quality of maternal contributions to these dialogues. Maternal psychopathology or childhood maltreatment experiences did not add to explain differences in quality of these dialogues. Future studies should replicate our findings, preferably with larger samples using a prospective, longitudinal design to disentangle associations between CSA, mother–child emotion dialogues, and children’s recovery over time.
Footnotes
Authors’ Note
This study was part of a PhD project carried out at the Section of Clinical Child and Family Studies, VU University Amsterdam.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ZonMw, the Netherlands organization for health research and development (grant number 80-82470-98-017).