
Abstract
Women enter doctoral programs at higher numbers than ever before, earning half the doctoral degrees in the United States. Some women doctoral students experience pregnancy and parenthood during their studies. As infertility and pregnancy loss are common occurrences, likely many women doctoral students encountered these reproductive challenges as well. This research study (N = 328) explores the experiences of women doctoral students who experience infertility, fertility treatment, and pregnancy loss. Participants described the influence of these experiences on their doctoral education, productivity, and professional development, the institutional resources available to support them, and the gaps in supports. Women who accessed fertility treatment reported more of an impact on productivity and more desired institutional supports than those who experienced infertility without treatment or pregnancy loss. The implications of these findings are discussed, including the use of the mentoring relationship to support women doctoral students, the role of grief, and the creation of formal institutional policies that explicitly address these types of circumstances, allowing for accommodations such as flexibility and class absences.
Personal life events, such as childbirth, divorce, marriage, or the death of a family member, impact persistence and retention in doctoral education (Maher et al., 2004; Spaulding & Rockinson-Szapkiw, 2012). For some doctoral students, especially women (Maher et al., 2004), these experiences delay progression through the program or cause them to leave the program altogether (Maher et al., 2004; Protivnak & Foss, 2009; Spaulding & Rockinson-Szapkiw, 2012). Infertility and pregnancy loss are common, with 12%–15% of women experiencing infertility and 10%–25% of pregnancies ending in pregnancy loss (Deka & Sarma, 2010; Geller et al., 2010), but these events are rarely included in the discussions of persistence and retention in doctoral education beyond an occasional mention of pregnancy loss as an example of a negative life event (Maher et al., 2004; Spaulding & Rockinson-Szapkiw, 2012). Since pregnancy loss and fertility treatment have a significant cost in terms of time, energy, physical symptoms, and psychological impact (Brier, 2008; Belhouse et al., 2018; Harris, 2017; Kong et al., 2010; Meaney et al., 2017; Payne et al., 2019; Rowlands & Lee, 2010), this omission is problematic.
The phenomena of infertility and pregnancy loss occur when the process of pregnancy and childbirth do not go as planned or expected (Bellhouse et al., 2018; Carolan & Wright, 2017; Collins, 2018). Reproductive challenges, deviations from the ideal progression of events, are characterized by societal norms and expectations that women remain silent about these experiences, furthering a long tradition of women refraining from sharing their reproductive experiences (Gerber, 2017). This silence makes coping with reproductive challenges and finding social supports much more difficult (Bellhouse et al., 2018; Collins, 2018; Gerber, 2017; Hiefner, 2020). Within academia, the experience of motherhood is already silenced (Armenti, 2004; Kent et al., 2020; Lynch, 2008; Mirick & Wladkowski, 2018), which may further strengthen the taboo on publically sharing these experiences. It is unknown how pregnancy loss, infertility, and fertility treatment are experienced by women enrolled in doctoral programs, because the invisibility of these issues extends to most professional literature outside of healthcare (Hazen, 2006), including doctoral education literature (Romero-Hall et al., 2018) and even into feminist writings (Layne, 1997).
Literature Review
Women doctoral students with children face unique challenges during their doctoral education because of the gendered nature of academic institutions (Mason et al., 2013; Tower & Latimer, 2016). The persistent stigma associated with women holding the dual roles of academic and mother maintains a silence about motherhood in academia, perpetuating the invisibility of motherhood within doctoral education (Armenti, 2004; Kent et al., 2020; Lynch, 2008; Mirick & Wladkowski, 2018). A lack of consistent formal polices to support doctoral student mothers can make navigating these experiences difficult for students (Kent et al., 2020; Mirick & Wladkowski, 2020; Springer et al., 2009). Although often invisible, motherhood can influence women's experiences; some women report their decisions to have children during their doctoral program decrease access to professional development opportunities and affect their professional careers (Kulp, 2016, 2020; Mirick & Wladkowski, 2018, 2020). Many women experience reproductive challenges on the road to motherhood, including pregnancy loss, infertility, and fertility treatment. These experiences are not mutually exclusive and, in fact, have many characteristics in common, such as stigma and silence (Bellhouse et al., 2018; Boncori & Smith, 2019; Bute et al., 2019; Lahman, 2009; Romero-Hall et al., 2018), the need for social support (Carolan & Wright, 2017), and associated emotions such as sadness, depression, and grief (Gerber, 2017).
Pregnancy Loss
Pregnancy loss occurs in 10%–25% of identified pregnancies (Avalos et al., 2012; Michels et al., 2007; Mukherjee et al., 2013). Pregnancy loss takes place most frequently in the first 12 weeks of pregnancy, with only 1%–5% of pregnancies ending between 13 and 19 weeks (Avalos et al., 2012; Michels et al., 2007). Pregnancy losses before 20 weeks of pregnancy include miscarriage, ectopic pregnancies, and molar pregnancies. The risk of pregnancy loss varies by age, race, and other risk factors (Avalos et al., 2012; Mukherjee et al., 2013). Black women are 43% more likely to experience a miscarriage than White women (Quenby et al., 2021). This racial difference in outcomes is largest during weeks 10–20 of pregnancy; at this stage, Black women experience twice the risk of miscarriage as White women (Mukherjee et al., 2013). Pregnancy loss after 20 weeks, or stillbirth, is uncommon, affecting 0.3% of pregnancies between 20 and 28 weeks and 0.3% of pregnancies after 28 weeks (CDC, 2020; Michels et al., 2007). The rate of stillbirth is twice as high for Black women (10.32 per 1,000) and 50% high for American Indian/Alaskan Native women than White or Asian women, (7.22 per 1,000) (CDC, 2020).
Both physical and psychological symptoms follow a pregnancy loss (Quenby et al., 2021). Sadness, depression, grief, PTSD, disrupted relationships, and negative career impact are common sequelae to pregnancy loss (Brier, 2008; Bellhouse et al., 2018; Hazen, 2006; Kong et al., 2010; Meaney et al., 2017; Quenby et al., 2021; Rowlands & Lee, 2010), although it is incorrect to assume that all women experience grief or sorrow at the loss of a pregnancy (Reagan, 2003). The effects of a pregnancy loss vary by individual, influenced by differences in personal circumstances, feelings about the pregnancy, and the context of the loss (Brier, 2008; Meaney et al., 2017; Reagan, 2003). For example, gestational age, infertility, and previous pregnancy losses were associated with higher levels of distress, isolation, and guilt in a sample of predominately White, heterosexual women (Huffman et al., 2015). Walks (2007) suggests that because the pregnancies of same sex couples are planned and require medical intervention, these mothers may be at great risk of distress at the loss of the pregnancy.
Pregnancy loss impacts a woman's work in many ways, such as requiring absences from work due to medical care, psychological symptoms, or grief (Hazen, 2006; Porschitz & Siler, 2017). For a doctoral student, a pregnancy loss may lead to class absences or missed meetings, lab time, or teaching time. Women frequently do not share their loss with colleagues and supervisors at work, especially if the loss occurred within the first trimester, so their grief remains invisible to those around them (Boncori & Smith, 2019; Porschitz & Siler, 2017). Although very common, pregnancy loss is rarely mentioned in the workplace and the management and organizational studies literature remains silent on this topic (Boncori & Smith, 2019; Porschitz & Siler, 2017).
Infertility and Fertility Treatment
Like pregnancy loss, infertility is a common experience. Infertility, defined as the inability to become pregnant after 12 months or the presence of recurrent pregnancy losses, affects 12%–15% of couples (Deka & Sarma, 2010; Kelley et al., 2019; Stanford, 2013). The psychological impact of infertility includes depression, anxiety, and anger (Deka & Sarma, 2010). Like miscarriage, the invisibility of this experience can lead to insufficient social support, loneliness, distress, depression, and isolation (Bell, 2012; Collins, 2018). Black and Latina women are more likely to experience infertility than White women (Greil et al., 2011).
The use of fertility treatments has become more common (Deka & Sarma, 2019), although there are many reasons that a woman may decide not to use fertility treatment. Bell (2016) describes the “heteronormative, classist, and gendered assumptions of reproduction and infertility” that impact women's ability to access and utilize fertility treatment in the United States. Women in same sex relationships are constrained by heteronormative assumptions of fertility, and women of color, especially those of low socioeconomic class, face stereotypes of hyperfertility and assumptions that they do not experience infertility (Bell, 2015; Ceballo et al., 2015). Infertility is seen as a problem encountered by older, White, upper middle class, heterosexual women (Bell, 2015). While infertility is experienced by women of color, women of lower socioeconomic status, and women in same-sex relationships (Bell, 2015), access to fertility treatment is affected by race, ethnicity, education level, income, citizenship, and access to health insurance (Kelley et al., 2019). In particular, Black and Latina women are less likely to seek medical care for infertility than White or Asian/Pacific Islander women (Greil et al., 2011). Doctoral students experiencing infertility may find university health centers unsupportive, with limited resources due to an assumption that students need focus on contraception and pregnancy prevention, not infertility support, resources, and treatment (Wagi et al., 2020). Concerns about infertility are typically dismissed and ignored.
For women who can successfully access treatment, pursuing and engaging in fertility treatment often causes psychological distress and creates an unmet need for support from medical professionals, mental health providers, family, and friends (Bell, 2012; Collins, 2018; Payne et al., 2019). The need for frequent medical appointments increases distress, especially for women who are working and concerned about the impact of regular absences from work (Payne et al., 2019). In addition to intensive time-consuming medical interventions requiring absences from work, fertility treatment involves multiple losses that are rarely acknowledged or well understood by others (Harris, 2017; Patel et al., 2018). When fertility treatment is unsuccessful, distress and grief can be intense, especially as couples lose hope that fertility treatment will result in a pregnancy and live birth (Fieldsend & Smith, 2020; Holley et al., 2021; Patel et al., 2018).
Some women report infertility treatment affects their daily functioning, work, and career (Collins, 2018; Payne et al., 2019). In one study, 50% of women believed that fertility treatment impacted their career options and one-third reported their career was negatively impacted; these numbers increased with the number of treatment cycles (Payne et al., 2019). Doctoral students may find themselves with multiple class absences, missed meetings, or more limited time to devote to scholarship. When fertility treatment persists across multiple months or years, so do these consequences.
Dominant Discourses about Reproductive Challenges
In the United States, there is a societal silence around unsuccessful reproductive journeys, such as pregnancies that do not begin easily, due to infertility, and those that do not end with a healthy, full-term baby (Ceballo et al., 2015; Layne, 1997; Walks, 2007). Without societal scripts on how to support women going through these experiences, potential supports (i.e., family members, friends, colleagues, and medical professionals) can be awkward, invalidating, discouraging, insensitive, or unhelpful, resulting in implicitly or explicitly encouraging women not to share their experiences or refusing to recognize or validate their grief (Bellhouse et al., 2018; Boncori & Smith, 2019; Carolan & Wright, 2017; Hazen, 2006; Meaney et al., 2017; Porschitz & Siler, 2017). When women experience grief due to reproductive challenges, it is sometimes perceived as an “exaggerated, even pathological, response to a minor occurrence” instead of recognized as a legitimate loss (Gerber, 2017). A lack of support increases feelings of isolation, distress, and depression, and the loss is unacknowledged and unrecognized by those around them (Bellhouse et al., 2018; Boncori & Smith, 2019; Carolan & Wright, 2017; Layne, 2003; Hazen, 2006; Porschitz & Siler, 2017; Romero-Hall et al., 2018; Rowlands & Lee, 2010).
These societal norms reflect a long history of silencing women's discussions about their bodies and reproductive experiences (Gerber, 2017) and these experiences remain misunderstood and unrecognized by many (Hiefner, 2020). Additionally, societal narratives of infertility and pregnancy loss highlight the experiences of White, heterosexual, middle class women (Ceballo et al., 2015; Peel & Cain, 2012; Walks, 2007). Ceballo et al. (2015) argue that individuals with non-dominant identities (e.g., race, sexual orientation, gender, and social class) are socially invisible, without access to cultural narratives that describe their experiences. Specifically, women of color, women in same sex relationships, and transgender and non-binary individuals are neglected in the literature on infertility and pregnancy loss while their experiences can be challenging due to discrimination and bias in medical care during these experiences (Ceballo et al., 2015; Peel & Cain, 2012; Walks, 2007).
Since the 1960s, the American women's health movement has worked to restore women's power and control over their own bodies, gain reproductive rights, and separate natural processes (i.e., childbirth) from a “paternalistic and condescending” medicalized model (Nichols, 2000, p.56). Layne (2003), writing about White middle class women, argues that this health movement unintentionally creates the assumption that women have the power to create happy endings to a reproductive journey, governed by their own choices about when and how the baby is conceived, carried, and birthed. In some ways, this narrative is similar to the biomedical model, except in that model, it is the use of available medical services that leads to a healthy pregnancy and a “natural joyful birth” (Layne, 2003, p.1889). Layne suggests that both infertility and pregnancy loss disprove this narrative because the feminist movement has traditionally “systematically minimizes and marginalizes negative reproductive health outcomes” instead of acknowledging these “stories of failure” (Layne, 2003, p.1887).
The reproductive justice movement, begun in 1994 by twelve Black women, used an intersectional lens and expanded this limited concept of reproductive rights to include an intersectional lens of oppression and systemic inequality, arguing that Black women's experiences must be understood through this lens (Ross, 2017). Even the reproductive justice movement, however, has not focused on pregnancy loss (Lens, 2020). This silence is further supported by the pro-choice movement and the complicated overlap between the issues of infertility, pregnancy loss, and abortion (Layne 1997, 2003; Lens, 2020), and therefore, many feminists have struggled to acknowledge women's grief and trauma after a pregnancy loss while simultaneously supporting abortion rights.
Due to these dominant discourses and the resulting taboo of open discussion of reproductive challenges, these experiences typically remain private; others may not ever understand the significance of the loss, and the legitimacy of the grief (Collins, 2018; Gerber, 2017; Hiefner, 2020). Doka (2000) defines disenfranchised grief as “grief that persons experience when they incur a loss that is not or cannot be openly acknowledged, socially sanctioned, or publicly mourned” (p.4). The lack of associated mourning rituals for these experiences further disenfranchises women from traditional grieving processes (Carolan & Wright, 2017; Lang et al., 2011) and the acknowledgement of loss that alleviates distress (Boncori & Smith, 2019; Meaney et al., 2017; Porschitz & Siler, 2017). A feminist approach suggests critical reflection on the dominant discourses and cultural norms around these experiences, and the ways in which these narratives may silence women, prevent them from obtaining needed support around these experiences, and pathologies the grief they may be experiencing (Gerber, 2017; Hiefner, 2020).
A Knowledge Gap
The silence around motherhood in academia intersects with the cultural stigma of publically sharing reproductive losses and challenges, resulting in limited information on the impact of these experiences on women doctoral students. As academics are uniquely vulnerable early in their career (Mason et al., 2013; Springer et al., 2009; Tower & Latimer, 2016), this gap has concerning implications in terms of our lack of understanding about women's trajectory through doctoral programs. There is no knowledge of the supports available to women, how these experiences could affect women's progression through doctoral programs and their career trajectory, or the ways in which programs can most effectively support women who are undergoing reproductive challenges such as infertility, pregnancy loss, or fertility treatment.
Methods
Data for this study came from a broader study of women's experiences with trying to conceive, pregnancy, and parenting in doctoral education (Mirick & Wladkowski, 2020). This paper includes the participants (N = 348) who had experienced infertility or a pregnancy loss while enrolled in a doctoral program. Data were collected via a national online survey in Qualtrics using purposive and snowball sampling. Participant recruitment occurred through several channels including social media and professional networks, and direct emails to Doctoral Program Directors in six fields (e.g., Nursing, Social Work, English, Biology, Computer Science, and Sociology) at U.S. programs with requests to share the study information and survey link with current and former students. The researchers are situated within this inquiry as we identify as White, academic mothers in tenured positions, who are married to employed male partners. Positionality within this study required consistent reflection to ensure sound data collection methods and the construction of survey questions, with careful consideration to the inclusivity of varied experiences.
Previous research was used to inform and guide the creation of the survey questions, with attention to obtaining diverse perspectives on the experiences. Eighteen yes/no questions asked about the impact of reproductive challenges on doctoral work. Ten yes/no questions asked about available supports for doctoral students experiencing infertility, fertility treatment, and pregnancy loss. There were two open-ended questions, “How did your pregnancy loss(es) impact your doctoral work?” and “What advice would you give to a woman, if any, who has just experienced a pregnancy loss during her doctoral program?”
The quantitative data was uploaded to SPSS (version 25), and descriptive statistics were used to analyze the data. Open coding was used to analyze the two open-ended questions. The responses were uploaded into Microsoft Word, and using thematic analysis (Braun & Clarke, 2006), an initial coding structure was developed by two members of the research team using the first 20% of the responses. The two initial sets of codes were compared, and any inconsistencies discussed until an agreement was reached. Through this process, a set of preliminary codes were created. Then, the two members of the research team coded the remaining data. Upon the completion of the coding, codes were compared for consistency and any discrepancies addressed through discussion. Then, similar codes were collapsed into broader themes. Exemplars are shared in the participants’ own words to further clarify these themes. Each shared exemplar is from a different participant to increase the diversity of participant perspectives.
Results
Sample
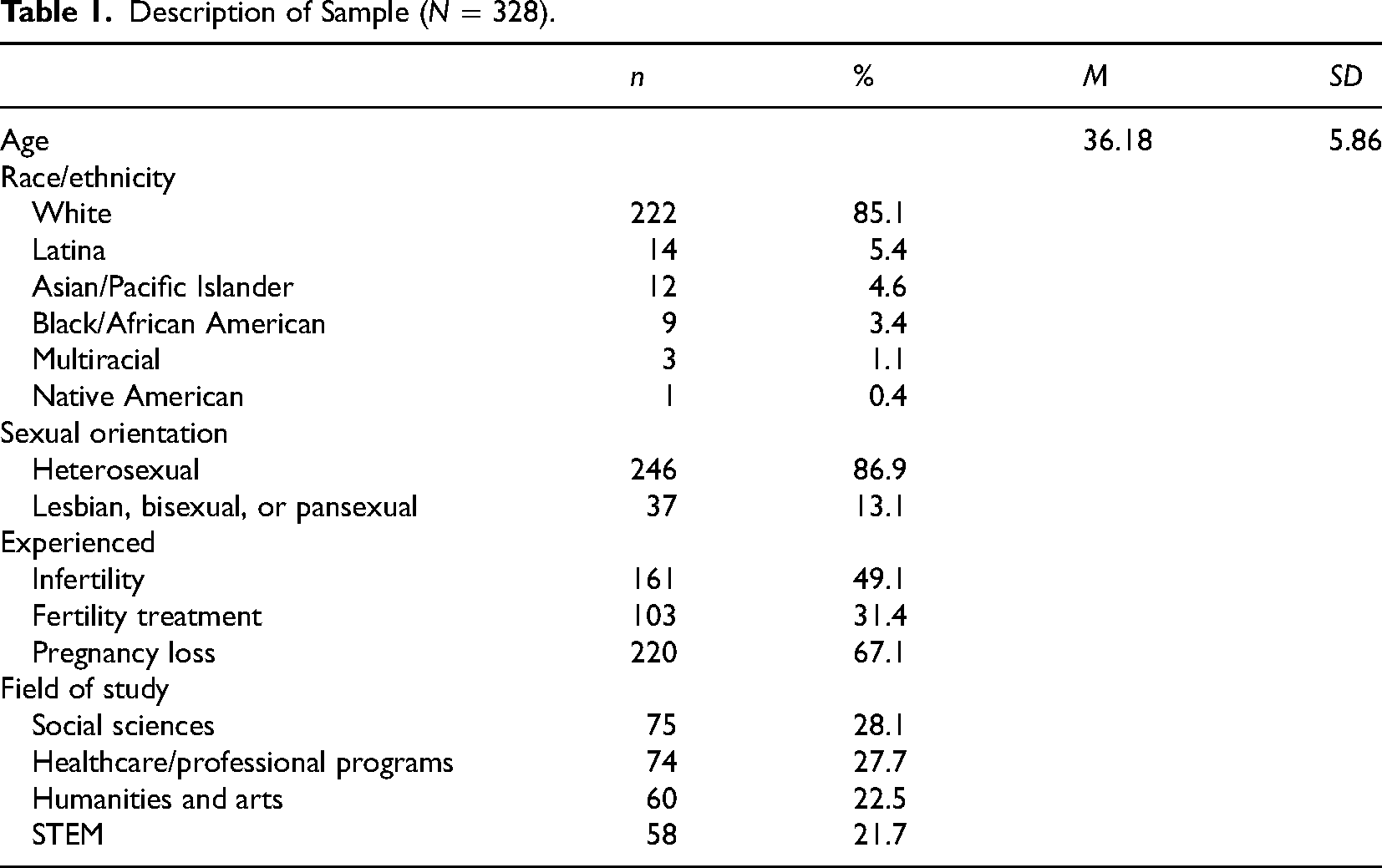
The sample (N = 328) included 161 (49.1%) participants who experienced infertility, 103 (31.4%) participants who accessed fertility treatment, and 220 (67.1%) participants who experienced pregnancy loss. The mean age was 36.18 (SD = 5.86) years. The sample was geographically diverse, with participants from all regions of the United States. The most commonly represented regions were the Midwest (n = 68, 20.7%) and the South (n = 76, 23.1%). In terms of race/ethnicity, 85.15% (n = 222) were White, 5.4% (n = 14) Latina, 4.6% (n = 12) Asian/Pacific Islander, 3.4% (n = 9) Black/African American, 1.1% (n = 3) Multiracial, and 0.4% (n = 1) Native American. The majority (86.9%) identified as heterosexual (n = 246), and 13.1% (n = 37) described their sexual orientation as lesbian, bisexual, or pansexual. Participants were in a variety of fields, with 28.1% (n = 75) from the social sciences, 27.7% (n = 74) healthcare/professional programs, 22.5% (n = 60) humanities and arts, and 21.7% (n = 58) STEM (see Table 1).
Description of Sample (N = 328).
Infertility
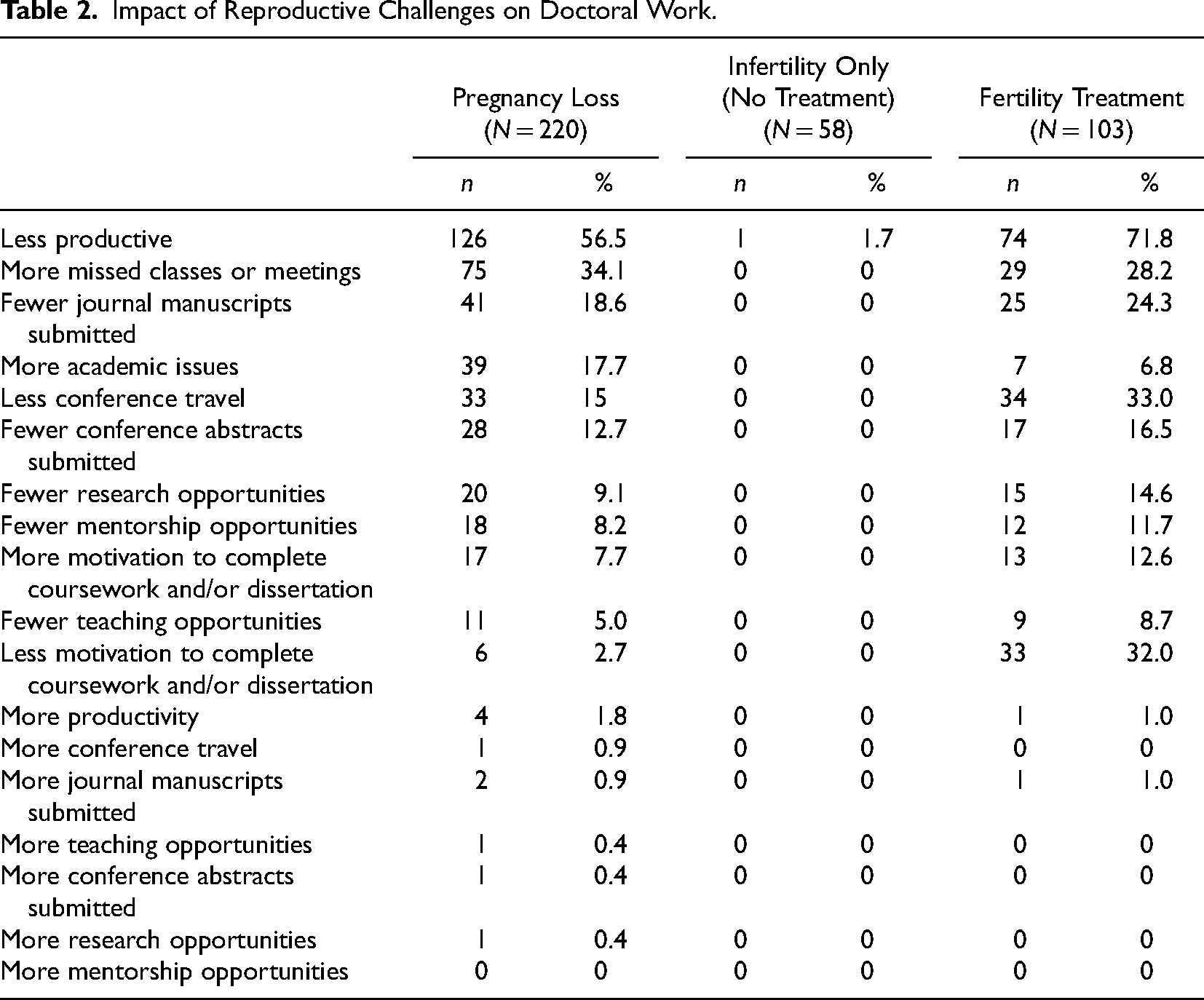
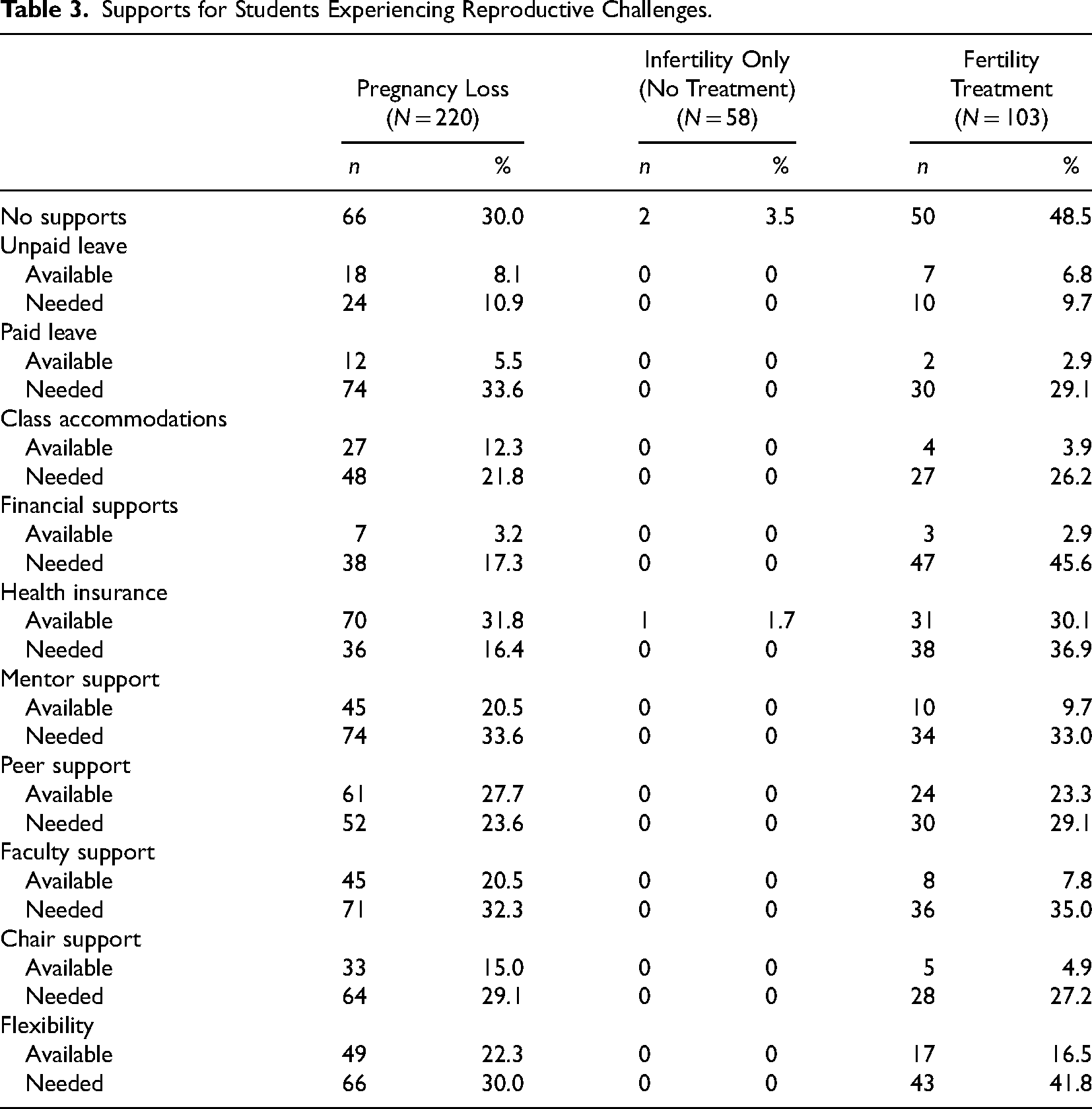
Participants (n = 161) experienced infertility during their doctoral program. Of this group, 64.0% (n = 103) accessed fertility treatment with a mean of 15.95 (SD = 13.84) months of treatment. Most participants who used fertility treatment (71.8%, n = 74) identified decreased productivity in their doctoral programs. Specifically, 33.0% (n = 34) reported less conference travel, 32.0% (n = 33) reported less motivation to complete coursework and/or dissertation, and 24.3% (n = 25) submitted fewer journal manuscripts for publications due to their experiences with infertility and fertility treatment. In contrast, only one (1.7%) of the participants who did not use fertility treatments reported decreased productivity (see Table 2). Almost half of the participants (48.5%, n = 50) who accessed fertility treatment reported there were no programmatic supports for them during this period. Some participants who had used fertility treatment reported supports had been available to them during this time, the most common being health insurance (30.1%, n = 31) and peer support (23.3%, n = 24). These participants identified the need for the following programmatic supports: financial supports (45.6%, n = 47), flexibility (41.8%, n = 60), health insurance (36.9%, n = 65), and support from a mentor (33.0%, n = 69). Participants who did not seek treatment reported almost no available supports and did not perceive a need for any additional supports (see Table 3).
Impact of Reproductive Challenges on Doctoral Work.
Supports for Students Experiencing Reproductive Challenges.
Pregnancy Loss
Participants (n = 220) experienced a pregnancy loss during their doctoral program. Many of these participants described a decrease in their productivity (56.5%, n = 126) in their doctoral program, specifically fewer manuscripts submitted to journals for publications (18.6%, n = 41), less conference travel (15.0%, n = 33), and fewer conference abstract submissions (12.7%, n = 28) (see Table 2). In terms of sharing their pregnancy loss, 43.7% (n = 93) talked to peers, 29.9% (n = 64) spoke to faculty, 40.7% (n = 87) talked to their chair or advisor, and 38.1% (n = 80) said they told no one at their program. Almost one-third (30.0%, n = 154) reported there were no institutional supports to help them through this experience. The most commonly available supports were health insurance (31.8%, n = 16.4), peer support (27.7%, n = 61), flexibility (22.3%, n = 49), mentor support (20.5%, n = 45), and faculty support (20.5%, n = 45). These participants reported a need for the following supports: paid leave (33.6%, n = 74), support from a mentor (33.6%, n = 74), support from a faculty member (32.3%, n = 71), flexibility (30.0%, n = 66), and support from their dissertation committee chair (29.1%, n = 64) (see Table 3).
Advice for Women Who Experience a Pregnancy Loss
Approximately three-quarters (71.4%, n = 157) of the participants who experienced a pregnancy loss described the advice they would give to a woman doctoral student who was going through a loss. Three main themes emerged: take time to take care of yourself and grieve (n = 90), find support, knowing you are not alone (n = 56), and be careful with communication (n = 45).
Take Time
Participants (n = 90) said women should take the time they needed to grieve and physically recover, by taking time off from school, requesting extensions on assignments, or just slowing down for a little while. Recommendations acknowledged women have different needs. For example, a 44-year-old, White, bisexual, woman in social work described the need to grieve, but also honor that each woman will be impacted by the experience differently: Please allow yourself the time to grieve. This looks different for everyone but if for you, it means your process slows down and you're not “the same,” that's okay. It doesn’t mean you are "less serious" or "less than" you were. Or if it means you throw yourself into your work and are more determined than ever, that's okay too.
Find Support
Participants (n = 58) emphasized the need to find a support system, through friends, support groups, and women who have experienced pregnancy loss. Supports ranged from friends, peers, mentors, and family to more formal supports like online support groups and mental health counseling. Accessing these supports could decrease feelings of isolation and help women obtain accommodations following a loss. A 37-year-old White heterosexual woman in the sciences described the support she received from an academic colleague: I miscarried right before a conference, and I was very concerned about going and a [female] colleague of mine reminded me that this is my life and I don't have to worry about a conference. I should worry about and take care of myself. I took nearly a week off. Build a support group of people you trust. I had my husband, my mom, and my best friend. I talked to them almost every day while I was going through the loss. I wish I had someone in the doctoral program to speak with. I told my department chair, who was very understanding, because I needed to postpone my comprehensive exams. I told to other faculty members with whom I was working, they were not supportive.
Some participants described negative experiences trying to access support. For example, a 38-year-old White heterosexual woman said, “My advisor basically told me, ‘Get over it.’” Another student, a 36-year-old White heterosexual woman in Education recommended, “Look outside of your program for assistance in dealing with the loss. There may not be anyone there who will understand.” These recommendations recognized the societal norms that emphasize keeping reproductive challenges private; many recommended breaking that silence by reaching out to others to access support.
Communication
Participants (n = 45) discussed decision making about the disclosure of a pregnancy loss to colleagues, faculty, and mentors in the doctoral program. While the benefits of sharing information were recognized by many participants in terms of being able to access needed supports around grief and loss, some recommended carefully considering if and how to communicate, with the understanding that sharing might have negative consequences due to a stigma around pregnancy and medical leave or could elicit unhelpful feedback and unsupportive comments. Reflecting this dichotomy, some advice encouraged open disclosure, suggesting women should not be afraid to disclose a pregnancy loss. A 41-year-old White woman in a same sex relationship advised, “Don’t keep it a secret.” Other participants recommended keeping silent. One sociology student, a 24-year-old Black woman, said, “Be open with your mentors and professors. Pregnancy loss will impact your attendance and coursework. They will be more willing to work with you if you are open and honest.”
Others recommended being cautious with disclosures or refraining altogether. A White, heterosexual 34-year-old in Public Health explained, “As terrible as this is and counter to the greater need, I'd suggest she not tell anyone. If she can get through it logistically without needing to say anything, it’d be better academically.” Being prepared for unhelpful or negative responses was important, as a 32-year-old White heterosexual Clinical Psychology student shared: Experiencing a pregnancy loss is difficult when you are part of any profession, as there are few social rituals that help us share and process this event with others. Share the news with those you know will support you. Expect that many may wish to support you but this may come out awkwardly or even offensively. For example, some faculty I spoke with wanted to know how far along I was and implied that being at a certain week during the time of loss would justify my reaction of grief, whereas they deemed grief prior to this time to be unjustified.
Pregnancy Loss and Career
Approximately one-fifth (22.3%, n = 49) of the participants who experienced a pregnancy loss reported that the loss affected their professional career, with 39 describing the impact. Specific themes included a shift in career goals or priorities (n = 23), a direct impact on their education (n = 20), and an intrapersonal change, such as mental health or general outlook (n = 19).
Shift in Goals/Priorities
Some participants (n = 23) felt this experience changed their priorities and goals. In choosing a position following their doctoral program, these participants were more likely to prioritize their family's needs, including location, schools, healthcare, part-time work, and family leave. Others, like this 30-year-old White heterosexual sociology student, felt disconnected from academia: My experience of pregnancy loss made me question my willingness to plan my family around graduation and tenure. Having no financial support as a graduate student also made me rethink my commitment to the system, which seems especially inhumane in light of the loss. It made me increasingly aware of the subtle ways that academia disadvantages women… of needing more work-life balance, and also motivated me to demonstrate my worth as a student and researcher in the aftermath [of miscarriage]. I [traveled] for a task related to one of my grants while miscarrying even though I had been given the option not to go. I'd experienced a lot of questioning of my commitment to that project previously (due to family obligations) … and wasn't able to let that perception happen again on one of the worst days of my life.
For some participants, the experience of pregnancy loss led to a reassessment of priorities while others perceived the goals and culture of academia as less attractive or desirable.
Doctoral Program Changes
Some participants (n = 20) described ways that a pregnancy loss directly affected their advancement through their doctoral program. Some participants’ progression was slower, due to decreased productivity and motivation, depression, and grief, while others missed out on professional development opportunities. A White, heterosexual 34-year-old psychology student described her experience, “Radically decreased productivity due to emotional stress, physical trauma, and severe depression after three pregnancy losses and desperately searching for a reason, a treatment, some hope. Worst experience of my life.”
Other participants described decreased productivity in specific ways that impacted their success on the job market. For example, a 29-year-old White heterosexual computer science student described experiencing “missed opportunities for networking, publishing, and just the pure enjoyment of research” following her miscarriage. A 35-year-old bisexual White sociology student said, “It [the pregnancy loss] decreased motivation to do the kind of networking and pro-active stuff that it takes to get hired.” Productivity affected current relationships with faculty and standing in the program, not just competitiveness on the job market.
A 39-year-old, White heterosexual woman in a sociology program said her loss “put me behind and in poor graces with my committee. We have no space for grieving in academia.”
For some participants, the long-term impact was significant. For example, this White, heterosexual, 30-year-old woman studying biology said: Due to two pregnancy losses within the first year of my doctoral program and a lack of support and understanding from peers and faculty, I chose to switch to a new doctoral program because despite my excellent work, several faculty members were skeptical and unsupportive of my work due to delays from pregnancy and miscarriage.
Personal Changes
Participants (N = 17) described changes in mental health, motivation, and perspective following a pregnancy loss. Negative affective responses included depression, anxiety, grief, and hopelessness. This participant, a 36-year-old White English student, shared her cumulative experiences with grief: Grief. … How to define grief the impact of grief? During my PhD program, I have been through four rounds of IVF for infertility issues. All four resulted in miscarriages. Four losses. That is a lot of grief… the amount of grief that I have experienced is sometimes overwhelming to think about. Since the loss of my son, I’m hanging on by a thread…I do not know if I will be able to complete the doctoral program and my career plans have changed in that my expectations are much lower. I’ll be doing well if I can even obtain a PhD.
Some participants found that grief changed them in fundamental ways.
Discussion
Infertility, fertility treatment, and pregnancy loss are missing from the academic literature on doctoral education. This study describes these experiences, which may be occurring more often than is assumed by looking at doctoral education statistics (Kulp, 2020). Frequently, participants’ experiences were invisible to many of their peers, faculty, and mentors (Bellhouse et al., 2018; Boncori & Smith, 2019; Bute et al., 2019; Lahman, 2009; Romero-Hall et al., 2018). Participants identified the difficulty of these experiences and highlighted the impact on their doctoral work, specifically overall productivity, conference attendance, and submission of journal articles. While not all participants found their productivity went down, 56.5% of those who experienced a pregnancy loss and 71.8% who engaged with fertility treatment were less productive due to their experiences. Overall, fertility treatment seemed to have a larger impact on doctoral work than pregnancy loss, with 24.3% submitting fewer journal articles and 33% attending fewer conferences due to their experiences. These resources and opportunities are critical to professional development and influence graduates’ ability to obtain prestigious tenure track positions (Kulp, 2020; Mirick & Wladkowski, 2019); it appears that, like students raising children, some women who encounter these reproductive challenges during graduate school may find themselves less competitive on the job market, especially for positions at research-intensive universities (Mirick & Wladkowski, 2020).
Participants wanted more support from peers, faculty, and mentors. The doctoral education literature suggests that women students desire mentorship that acknowledges all their roles and offers psychosocial support (Gutierrez, 2012; Wladkowski & Mirick, 2019a). Mentors need to be able to support students who experience marginalization and discrimination due to their social identity, including students of color and LGBTQ + students and understand the ways in which intersectionality impacts their experiences (Lens, 2020; Sarna et al., 2021). The reproductive health literature consistently identifies a need for social support for women with reproductive challenges (Bellhouse et al., 2018; Boncori & Smith, 2019; Carolan & Wright, 2017; Collins, 2018; Layne, 2003; Hazen, 2006; Porschitz & Siler, 2017; Romero-Hall et al., 2018; Rowlands & Lee, 2010), suggesting that a lack of support adds to feelings of isolation, shame, stigma, and distress (Ceballo et al., 2015). In addition to psychosocial support, mentors may be able to support students in navigating identified issues such as decreased productivity, difficulties attending academic conferences, and the need for flexibility and class accommodations. A need for flexibility was identified by almost half (41.8%) of women who used fertility treatment and about a third (30.0%) of those who had a pregnancy loss. Mentors may be able to play an important role in helping students access these types of accommodations while other faculty can support students in requesting and utilizing them.
Although some type of disclosure is required in order to obtain flexibility, understanding, and psychosocial support (Bellhouse et al., 2018; Collins, 2018), some of the open-ended responses reflected on possible negative consequences of sharing personal information. Some participants wanted to avoid assumptions that they were less committed to the program (Armenti, 2004; Drago et al., 2006; Kent et al., 2020; Lynch, 2008; Mirick & Wladkowski, 2018) while others were wary of unsupportive or unhelpful responses (Bellhouse et al., 2018; Boncori & Smith, 2019; Carolan & Wright, 2017; Hazen, 2006; Meaney et al., 2017; Porschitz & Siler, 2017). Secrecy has implications outside of access to resources and accommodations. When women do not share their experience, they are unable to obtain social support around their loss, and their grief goes unrecognized, which can make the experience more difficult (Boncori & Smith, 2019; Collins, 2018; Porschitz & Siler, 2017). The negative psychological impact of these unacknowledged losses can affect motivation, productivity, and career progression (Collins, 2018; Hazen, 2006; Payne et al., 2019); a lack of disclosure may protect women from implicit bias, insensitive responses, and preserve privacy but negatively impact their reputation and relationships in the program if productivity, motivation, and engagement decrease without explanation.
Those engaged with fertility treatment reported the greatest decrease in productivity, motivation, and scholarship, compared to those with infertility who did not access treatment or women who experienced a pregnancy loss. The literature emphasizes the significant impact of fertility treatment on women and their careers (Collins, 2018; Payne et al., 2019). The long-term nature of some women's experiences with fertility treatment might heighten this effect (Ceballo et al., 2015). Long-term treatment leads to ongoing absences due to medical treatment (Payne et al., 2019), missed time for research and scholarship, and difficult planning for conference attendance, potentially compounded by grief following failed attempts to conceive or a loss of a pregnancy after fertility interventions (Fieldsend & Smith, 2020; Patel et al., 2018). This group may have a greater need for mentor support, problem-solving, and advocacy, especially when treatment is long term.
Approximately one-third (30.0%) of participants who experienced a pregnancy loss and almost half (48.5%) of those who accessed fertility treatments reported there was no support of any kind available to them from their doctoral programs or institutions. It is unknown whether supports were nonexistent, perhaps due to a lack of recognition of student need (Wagi, 2020), or inaccessible, because students refrained from disclosure due to societal norms of maintaining silence about these experiences (Bellhouse et al., 2018; Boncori & Smith, 2019; Bute et al., 2019; Lahman, 2009; Romero-Hall et al., 2018) and therefore were never informed about available supports. More research is needed to better understand the needs, if any, of the group with infertility who did not access infertility treatment. This group did not desire any additional supports from their program, but it is unknown whether they did not access treatment out of choice, or due to the failure of previous treatment, a lack of access to affordable treatment, or stigma (Kelley et al., 2019). This group might benefit from a different set of supports.
A primary theme in the open-ended responses was the need for self-care, including taking time to acknowledge a pregnancy loss and grieve, even within a system that, reflecting societal attitudes and norms about reproductive challenges, might not recognize that loss (Boncori & Smith, 2019; Carolan & Wright, 2017; Lang et al., 2011; Meaney et al., 2017; Porschitz & Siler, 2017). In contrast to this advice, academic culture emphasizes the ability to focus primarily on academic work without the intrusion or distraction of personal responsibilities (Armenti, 2004; Authors, 2018; Drago et al., 2006; Kulp, 2020). Women doctoral student mothers describe a pressure to continue to be just as productive and successful in doctoral programs as students without children in order to demonstrate their commitment to academia (Authors, 2018), and those pressures may influence a decision to maintain productivity during a pregnancy loss or fertility treatment, instead of taking time off to recognize and come to terms with a loss or engage with fertility treatment. For women of color, stigma and racism can impact the experiences of pregnancy loss, infertility, and fertility treatments. Black women sometimes experience gendered racism around pregnancy specifically related to cultural stereotypes about Black women, a stigma about Black pregnancy, and scrutiny on their behavior and decisions around reproduction (Mehra et al., 2020; Lens, 2020; Ross, 2017). There were few Black women in this sample, so these issues could not be fully explored. Future research should highlight an understanding of the intersection of racial/ethnic identity and women's experiences with reproductive challenges in doctoral education.
The silence and invisibility surrounding infertility, fertility treatment, and pregnancy loss further disenfranchise women's grief and highlight the lack of recognition for this type of loss (Boncori & Smith, 2019; Collins, 2018; Porschitz & Siler, 2017). Without naming the experience and creating supportive networks within academic programs, doctoral students have no guidance on how to navigate these experiences. More research should explore these experiences for women, including how doctoral programs can best to support women, protecting them from a loss of status and reputation in the program. In addition, it is important to further explore the diversity of women's needs and experiences in these situations. While some participants spoke of grief and the need for more support and resources, others did not (Reagan, 2003). It is critical that the breadth of women's reactions, responses, and needs are recognized and considered by programs.
It is important to consider how these findings might fit into the broader landscape of doctoral education. A substantial body of research has documented that doctoral student mothers are under-represented in tenure track positions at research intensive universities, especially in STEM fields (Kulp, 2016; Mason et al., 2013). Women with children are more likely to be hired into positions at teaching-intensive universities and community colleges (Kulp, 2016; Mason et al., 2013). Doctoral student mothers identify barriers to success that include a silence around the dual roles of motherhood and academia, difficulties accessing necessary professional development opportunities, a need for time away from academia, and stigma about motherhood as a doctoral student (Mirick & Wladkowski, 2018). The themes of the participants in this study are similar, although the need for time away from academia focused on coping with the physical and emotional responses to pregnancy loss versus. Acker & Armenti (2004) identify that academic mothers may experience a cumulative disadvantage in terms of missed networking opportunities, teaching experience, conferences attended, and papers published due to the responsibilities of parenting. These findings suggest that for women who experience fertility treatment and/or pregnancy loss, this cumulative disadvantage may begin even before conception, putting them at a further disadvantage in a competitive academic landscape.
Women of color face cumulative disadvantages in higher education and are disproportionately affected by infertility and pregnancy loss (Lens, 2020). Women in same-sex relationships use fertility treatments at much higher rates than heterosexual women. Due to the small number of women of color and women in same-sex relationships in this sample, differences in experiences, impact, and support could not be explored, but it is important to better understand the experiences of infertility and pregnancy loss outside of the experience of White heterosexual women (Lens, 2020; Ross, 2017). Future research should focus on intersectionality and the experiences of doctoral students to better understand their experiences.
Limitations
There are some limitations to this research study. First, there may be a response bias, with those with more negative or more positive experiences with their institutions or doctoral programs being more likely to respond. Doctoral program culture, and the ways in which it supports doctoral students with children, vary by program, field, and university (Kulp, 2016; Mirick & Wladkowski, 2018, 2020). Those programs with cultures that are more supportive of students who are mothers or program directors who are more aware of these issues due to personal experiences may have been more likely to share this study information with students. Women who left doctoral programs are much more difficult to access than those currently enrolled in programs, so the study may not have reached as many participants who withdrew from programs following these experiences; their experiences may be unique.
Second, the use of quantitative survey methods limits the depth of the responses, even to the open-ended questions, as there is no ability to ask follow-up or clarifying questions. The context of the experience is lost, so that the findings do not include factors that might impact their responses and need for supports. For example, it is unknown if a pregnancy occurred unexpectedly or after years of infertility treatment or if a pregnancy loss was a first loss, or one of many. The survey intentionally used the broader term of pregnancy loss, so it is unknown when in the pregnancy the loss occurred. Third, the sample includes only cisgender women and, therefore, does not reflect the experiences of transgender women and non-binary individuals with pregnancy loss and infertility, an experience that is likely more silenced in academia than those of cisgender women. Future research should explore this issue further.
Fourth, the survey included fewer questions about infertility and fertility treatment than pregnancy loss; this led to less information on the impact of fertility treatment, specifically in terms of career impact. Future research could explore these issues more in depth. The strength of the survey questions also highlight a limitation; they include only the perspectives of women students themselves, not that of faculty, administrators, or peers. It is unknown if others would have the same perspective on supports provided, gaps in supports, and the experiences of students.
Finally, similar to the majority of the research on women's reproductive health issues, the sample had limited racial and ethnic diversity, and was primarily composed of White heterosexual women (Ceballo et al., 2015; Reagan, 2003). While the findings are authentic to their experiences, there are a relatively few women of color in the sample, and these findings may speak only to White women's experiences with pregnancy loss and infertility in doctoral education. In reproductive medicine, there is a stereotype that fertility challenges impact only White heterosexual women, and to assume that that group's experience applies to all women (Ceballo et al., 2015; Reagan, 2003; Ross, 2017; Walks, 2007). In interpreting these findings, it is essential that care be taken in generalizing the results in order to avoid these assumptions, which can make invisible the experiences of women of color and LGBTQ + individuals.
Implications
Policies
The highlighted need for accommodations, flexibility, and support suggests the development of policies that explicitly address reproductive challenges, especially around medical care and bereavement (Porschitz & Siler, 2017). The absence of formal policies perpetuates the invisibility of reproduction and motherhood within doctoral education (Armenti, 2004; Kent et al., 2020; Lynch, 2008; Mirick & Wladkowski, 2018). In contrast, specific policies addressing the needs of women undergoing fertility treatment or experiencing a miscarriage could both support women and reduce the stress and other negative psychological symptoms that can result from multiple, ongoing absences (Payne et al., 2019). Women with a longer involvement with fertility treatment might benefit most significantly from these types of policies because psychological distress increases with more cycles of treatment and the resulting need for more absences (Payne et al., 2019).
For full-time employees, institutional benefits are usually clear, and human resources can support employees as they determine available resources. Doctoral students may be ineligible for the benefits enjoyed by full-time employees or faculty and students may not be aware of available institutional supports for doctoral students (Mirick & Wladkowski, 2020; Springer et al., 2009). Even when policies exist, they might not apply to reproductive challenges such as early pregnancy loss or medical treatment such as fertility testing. When universal policies are not available to students, students are required to approach individual faculty to request accommodations on a case-by-case basis (Springer et al., 2009; Wladkowski & Mirick, 2019b). With a pregnancy loss, women may need to justify their grief, as this type of loss is often not recognized or acknowledged. Servaty-Seib and Colleagues (2019) developed a Grief Absence Policy for Students (GAPS), which provided excused absences and the ability to complete or make up missed work following a loss, to be adopted by institutions interested in providing more substantial leave policies to their students. Universities could use this policy as a framework, explicitly including reproductive losses. Alternatively, universities could create a policy to support students experiencing reproductive losses, such as a pregnancy loss or failed IVF attempt, and students who are engaged in fertility treatments. At minimum, doctoral students need flexibility within their doctoral programs and leave policies for students that are parallel to policies for employees. Due to the vulnerable position of students, they may need more institutional protection, in the form of formal policies, than full-time employees, especially in the case of pregnancy and/or parenting, where policies and supports for full-time academic women are sometimes underdeveloped.
Universal policies would benefit not only women undergoing fertility treatment or a pregnancy loss, but also students with other challenges, such as an acute illness or a loss. The provision of flexibility during these crises could provide critical support to doctoral students, allowing them to progress smoothly through their programs and decreasing their distress (Payne et al., 2019). Naming fertility treatment and pregnancy loss explicitly in polices would break the silence within doctoral programs about these experiences, perhaps making it easier for women to disclose and access needed flexibility and accommodations. Formal policies would allow women to rely less on the generosity and understanding of individual faculty members; instead accommodations would be a benefit to which all students are entitled, creating equitable access to supports for all students (Mirick & Wladkowski, 2020; Springer et al., 2009).
In addition to formal policies, some participants desired formal supports such as financial resources or healthcare. Overall, institutions tend to provide insufficient formal supports for doctoral student parents (Bodkin & Fleming, 2019; Kent et al., 2020; Mirick & Wladkowski, 2018; Springer et al., 2009). This study extends these findings to women experiencing reproductive challenges. Programs and institutions wanting to better support student parents—or those on the path to parenthood—may want to consider how to address these deficits. In particular, women undergoing fertility treatment desired more resources from their programs, such as financial supports (45.6%) and healthcare resources (36.9%). Programs should consider the responsiveness of the university system to the needs of this group of students, including assessing the availability of health and mental services on campus, the existence of leave policies that include these students, and awareness of how to accommodate a medical issue such as infertility. For example, health services should able to asses and refer to fertility testing and treatment when necessary (Wagi et al., 2020). Mental health services should able to provide grief counseling for pregnancy loss or failed fertility treatment, counseling focused on coping with fertility treatment, or support groups for women who have experienced a pregnancy loss (Bell, 2012). As many women are reluctant to share these experiences with co-workers and supervisors (Payne et al., 2019), programs need to consider how to make these types of supports universally available to students, as faculty will not be able to identify the students having these experiences.
Mentor Support
Good mentorship is a critical component of a doctoral student's experience and integral to their success (Curtin et al., 2016; Gutierrez, 2012; Protivnak & Foss, 2009; Wladkowski & Mirick, 2019a). For women of color, especially in predominately White institutions, mentorship is essential to “increase tenure rates, overall success in academia, and the retention and recruitment of Latina and African American female students” (Duran, 2016, p.111). For doctoral student mothers, mentors can help them navigate the intersection of motherhood and doctoral work, providing advice, guidance, and advocacy when needed; mothers consider this support a key component of success (Kent et al., 2020; Mirick & Wladkowski, 2019).
In this study, many participants desired support from mentors around reproductive health issues, reflecting these previous findings. The mentoring relationship is a logical location for this type of support, as mentors often advise, guide, and advocate for their doctoral students, as well as provide important psychosocial support (Gutierrez, 2012; Kent et al., 2020; Wladkowski & Mirick, 2019a). Programs should assess mentors’ preparedness to do this type of work. Some many need more information about instructional supports (Springer et al., 2009) or guidance on how to provide effective, empowering support (Wladkowski & Mirick, 2019b). Mentors can create a space where both the professional and personal are welcome, and then explicitly welcome the sharing of personal information like reproductive challenges, providing guidance and advice, and advocating on the student's behalf (Hazen, 2006; Kaufman, 2021; Kent et al., 2020; Wladkowski & Mirick, 2019a). The mentoring relationship can be a space in which these challenges and losses are visible, acknowledging the impact and meaning of these experiences. Women of color, who often feel isolated due to a cultural assumption that infertility and pregnancy loss are uncommon in their community (Bell, 2015; Ceballo et al., 2015), may experience an even greater benefit of good mentorship, such as having access to a peer or faculty mentor of color who could dispute this assumption as well as support their advancement in what are often predominately White programs and institutions. Similarly, LGBTQ + individuals might benefit from a mentor who identifies as a part of the LGBTQ + community and can provide affirming, supportive mentorship.
On the other hand, the mentoring relationship can be disrupted or damaged when reproductive challenges, pregnancy, or childbirth occur (Wladkowski & Mirick, 2019a). The participants in this study described responses from mentors and faculty members could be dismissive, unsupportive, and even painful, reflecting experiences women have outside of academia (Bellhouse et al., 2018; Boncori & Smith, 2019; Carolan & Wright, 2017; Hazen, 2006; Meaney et al., 2017; Porschitz & Siler, 2017). Sometimes, the mentoring relationship is the source of acculturation to the norms of academia, including implicit bias about caregiving, accepted silence about parenting and reproductive issues, and pressure to “push through” difficult life experiences without them impacting work (Mirick & Wladkowski, 2018, 2019). Explicitly discussing these issues with faculty mentors, developing support systems and processes, and training those who are not prepared to do this work would benefit students during these personal crises.
Conclusion
The invisible experiences of fertility treatment and pregnancy loss affect women doctoral students’ productivity and experiences in doctoral education. The silence around these experiences, supported by both societal stigma about women's reproductive health and an academic culture that silences discussions of motherhood, means that these topics are rarely discussed and poorly understood. This study shines a light on these experiences, clarifying the impact of them on women doctoral students and the need for doctoral programs to consider how they can accommodate and support women going through these experiences, preventing women from turning away from academia or feeling unqualified or unprepared for academic positions. It is critical that doctoral programs consider how to support women, in order to ensure equitable experience in doctoral programs and beyond.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.