
Abstract
This study utilizes Head Start Impact Study data to examine whether Head Start is associated with teenage mothers’ experiences. Among 3,576 participants, 579 mothers were identified as teenage mothers (under 19 years old). Research questions included (1) compared to nonteenage mothers, do teenage mothers have different maternal experiences such as informal social support, formal social service use, mental health, and child-rearing skills? (2) does Head Start have any association with the experiences of teenage mothers? Teen mothers had less education, lower family incomes, and were less likely to be married than nonteenage mothers. Teenage mothers were most likely to identify as black and least likely to identify as Hispanic. Teenage mothers were more likely to speak English at home and live in rural areas. Further, regression analysis indicated that teenage mothers used less formal social services and displayed less mental health problems than nonteenage mothers. There was not a significant association on parental experiences for teenage mothers participating in Head Start. Study implications include using teen mothers’ voices to inform service needs, increasing strengths-based interventions, and raising awareness or creating nonstigmatizing programs for teen mothers.
In the United States, the teen birth rate in 2016 was 20.3 per 1,000 girls aged 15–19, and approximately one in four teens were likely to be pregnant before age 20 (National Conference of State Legislatures, 2018). Whereas, in 2017, another drop in teen birth rates to 18.8 per 1,000 girls aged 15–19 occurred, a decrease of 7% from 2016 (Center for Disease Control and Prevention [CDC], 2019). The United States is one of 77 countries whose adolescent fertility rates decreased by more than 50% between 1990–1995 and 2015–2020 (United Nations, 2020). Even with these decreases, the United States still has one of the highest teen pregnancy rates among industrialized nations (CDC, 2019; Guttmacher Institute, 2015). The U.S. teen pregnancy rate may be higher for many reasons including stigmatizing teen’s sexual activity, inaccessibility to contraceptive services, and having more disadvantaged families compared to other countries (Power to Decide, 2019; Stanger-Hall & Hall, 2011).
Teen pregnancy is viewed as a social problem in the United States (Bonell, 2004) with many people focusing only on negative outcomes for teen mothers such as lower educational attainment, lower incomes (Combs et al., 2018), and higher rates of abuse and neglect to children (Bartlett et al., 2014). However, significant research shows that these negative experiences should not be looked at as a “cause” of teen pregnancy and that instead, the societal situations of teens who are at risk of getting pregnant should be considered (Anastas, 2016; Bonell, 2004; Breheny & Stephens, 2007; Duncan et al., 2010). More specifically, being disadvantaged is likely to put girls at risk for teen pregnancy, but these disadvantaged characteristics may have occurred regardless of being pregnant (Breheny & Stephens, 2007).
Further research is needed to better understand how interventions, such as Head Start, can support teen mothers and their children with a strengths-based perspective instead of a deficit-based perspective. This study aims to assess the societal challenges, support systems, mental health status, characteristics, and parenting practices of teen mothers to best understand what associations Head Start has with teen mothers’ experiences.
Societal Challenges and Teen Mothers’ Experiences
Research shows that significant sexism, stigma, discrimination, and social isolation occur to teen mothers in various countries including the United States (Anastas, 2016; Breheny & Stephens, 2007; Greene, 2007; Levac, 2013; Ponsford, 2011). For instance, Levac (2013) who examined young mothers aged 16–24 and Sniekers and Rommes (2020) who studied young mothers under 23 years old both found that young mothers when empowered can embrace their intersectionality and succeed. Statistics such as higher rates of depression (Hipwell et al., 2016; Hodgkinson et al., 2014) and substance use into adulthood (De Genna et al., 2009) have been found for teen mothers and could be due to the stigmatization and discrimination they face in many societies. Research is contradictory when it comes to deciding if teen motherhood is associated with negative outcomes or if circumstances that teens are in before they become mothers are associated with teen pregnancy (e.g., living in poverty, having less resources). Further, these disadvantaged circumstances may be correlated with higher rates of neglect toward children (Lounds et al., 2006) or less knowledge about effective parenting in general (Kim et al., 2018).
The highest rates of teen pregnancy are among Hispanic and black teens (Combs et al., 2018; Kost & Maddow-Zimet, 2016). According to Kost and Maddow-Zimet (2016), with 92.6 per 1,000 black females becoming teen mothers and 73.5 per 1,000 Latina females becoming teen mothers, while only 25.2 per 1,000 white females become teen mothers. Black and Hispanic teen mothers’ experiences of stigma and discrimination have been found greater than non-Hispanic white teen mothers (Manlove et al., 2013; Rosenthal & Lobel, 2016). Furthermore, black and Hispanic teens are more likely to live in poverty (CDC, 2019; Galloway et al., 2017; Manlove et al., 2013) which statistically has been found to increase their chances of becoming pregnant, having lower academic achievement, and having less access to quality contraceptive services (Bonell, 2004; Breheny & Stephens, 2007; CDC, 2019; Galloway et al., 2017). Many critical race theories exist (e.g., Delgado & Stefancic, 2001; Dixson & Rousseau, 2006) to better understand the challenges minority teen mothers experience, and it is critical for societies to utilize these theories and the voices of this population to ensure mother’s needs are being met.
Despite the difficulties teen mothers experience, many studies find that they often display significant strengths when they have adequate support (Ponsford, 2011; Rolfe, 2008; Shea et al., 2015; Sniekers & Rommes, 2020). For instance, Ponsford (2011) examined young mothers aged 13–22 and argued that consumption practices should be viewed as a display of resilience in a culture that is constantly judging and condemning these mothers. Furthermore, Rolfe (2008) studied 33 young mothers that gave birth before the age of 21 and found significant trends of resilience and growth among these mothers. Unfortunately, studies show teen mothers on average have lower social support (Assini-Meytin et al., 2018) and are less likely to use formal social services than older mothers (Angley et al., 2015; Leplatte et al., 2012). More specifically, Angley et al. (2015) examined adolescent parents aged 14–21 and found that social support is associated with greater levels of parenting satisfaction. However, Greene (2007) examined parents aged 15–22 and found that often there are structural barriers limiting teen mothers from participating in community engagement. It is clear that social support is an important protective factor for teen mothers, but perhaps due to the intense stigma and discrimination surrounding teen motherhood in many countries, teen parents may be less likely to seek out support. Decreases in societal stigma and more support from families, programs, and policy makers are required to ensure that teen parents and their children can succeed (Arai, 2009; SmithBattle, 2006).
Current Interventions Targeting Teen Mothers
Understanding the context of teen pregnancy in the United States involves an evaluation of funding priorities and current interventions. America is the only country that provides federal funds to abstinence-only programs, with US$90 million going to abstinence-only programs in 2017 (Fox et al., 2019), even when most research shows these programs have little effect on rates of teen pregnancy (Fox et al., 2019; Health & Human Services [HHS], 2019b). Further, in 2017, the federal government spent 364.7 million on pregnancy/STD/HIV prevention programs, and only 345.5 million on Family Planning services (HHS, 2019a). Whereas in 2008, the federal government spent US$176.5 million on abstinence-only programs, US$300.2 million on pregnancy/STD/HIV prevention programs, and US$309.1 million on Family Planning services (HHS, 2019a). This indicates that the United States has decreased funding to abstinence-only programs and increased funding for Family Planning and pregnancy prevention. In 2018, the United States spent US$3.6 trillion, so 800.2 million spent on pregnancy prevention and family planning seems low in comparison to the total health care expenditure of the United States (Centers for Medicare & Medicaid Services, 2019; HHS, 2019a).
The United States is one of the only developed countries that does not have universal health care, and as such, other countries often implement funding for pregnancy prevention and contraceptive use within their universal health care system (Doherty et al., 2020; Sedgh et al., 2015). This makes it difficult to compare funding spent between countries; however, it is well established that the United States spends more per capita on health care than other developed countries (Doherty et al., 2020) and that higher rates of teen pregnancy may be due to poor access to contraception or abortion services (Sedgh et al., 2015).
According to Power to Decide (2019), in America, 19 million women live in a “contraceptive desert” or an area where they cannot access the full range of birth control methods and need to travel more than an hour to get certain birth control. Further, rural areas (counties with a population of less than 50,000 people) reported teen birth rates of 30.9 per 1,000 which was significantly higher than urban counties with bigger populations (Santhanam, 2016). This may be due to rural areas having few interventions for teen pregnancy and limited access to contraception services (Amaral et al., 2007; Rohrback et al., 2019). Overall, even when prevention programs are comprehensive and educate teens on contraceptive use, often teens do not have access to these methods to practice safe sex, indicating a need for effective and accessible services for rural teen mothers.
There are few programs and funding for interventions that support teen parents and provide quality sex education including Family Planning which provides contraceptives, health centers, and pregnancy testing among other services to low-income and vulnerable populations (Amaral et al., 2007; HealthyPeople.gov, 2020). However, there are many barriers to teens using services from programs like Family Planning, including accessibility, costs, and limited insurance among low-income populations (Amaral et al., 2007; HealthyPeople.gov, 2020). America’s limited funding for supportive programs, contraceptive deserts, and inaccessibility to programs creates significant barriers for teen mothers to succeed and thus perpetuates the stigma and discrimination toward this vulnerable population.
Head Start
Head Start comprises two programs: Head Start and Early Head Start (EHS). Head Start is a federally funded, early education program provided to low-income families with children aged 3–5 (Office of Head Start [OHS], 2019). To be eligible, family income must not exceed the outlined 2020 federal poverty level of US$26,200 for a family of four (Office of the Assistant Secretary for Planning and Evaluation, 2020; Early Childhood Learning & Knowledge Center [ECLKC], 2019b). EHS offers similar services and has the same low-income eligibility but is available only to infants and toddlers 0-3 (ECLKC, 2020). While services differ across Head Start centers, targeted family outcomes include “family well-being, positive parent-child relationships, families as lifelong educators, families as learners, family engagement in transitions, family connection to peers and community, and families as advocates and leaders” (ECLKC, 2019a).
Head Start was chosen as the targeted intervention for this study because it targets low-income and vulnerable populations, offers strengths-based approaches such as utilizing an ecological and two-generational approach, and has a high-quality, nationally representative data set. An ecological approach incorporates multiple spheres of a child’s life when analyzing children’s behaviors or best ways to intervene (Horwitz, 2015). An ecological approach has been found to provide a more holistic view, and interventions are typically more successful when they have this approach (Bartlett et al., 2014). Additionally, Head Start uses a two-generational approach, or services and interventions that assist both children and their families, which has been found significantly helpful promote parent–-child bonding and increase positive parenting behaviors (Sommer et al., 2018). Finally, a nationally representative, high-quality data set is available through the Head Start Impact Study that was conducted between 2002 and 2005 (U.S. Department of Health and Human Services [DHHS], 2010).
Previous studies have found that 15.6% of children in Head Start were born to mothers under the age of 19. In 2018, families enrolled in Head Start identified as white (44%), black (30%), and biracial (10%; ECLKC, 2019b). These percentages for black and Hispanic families are significantly lower than national percentages, showing a discrepancy among what racial groups enroll in Head Start. Furthermore, with means-tested eligibility requirements, it is expected that Head Start would have increased enrollment among minority families; however, this is not the case, pointing to potential problems such as stigma, inadequate services, or poor recruitment to minority groups.
Few studies have been conducted on the associations of Head Start services with teen mothers’ experiences. As such, our study seeks to add to the literature by utilizing Head Start Impact Study Data (HSIS) data to answer the following research questions:
Method
HSIS
In 1988, Congress required the DHHS to determine the effectiveness and impact of the Head Start program on its participants. This led to the creation of the HSIS which began in the fall of 2002 and used a nationally represented, randomized population, consisting of newly entering 3- and 4-year-old children and their parents. A total of 4,442 entering children and parents were randomly chosen from 25 different states, 84 agencies, and 383 Head Start centers. Within the sample, 2,449 of the participants were 3 years old and 1,993 were 4 years old. The participants were randomly assigned into either a Head Start intervention group (n = 2,646) or a control group (n = 1,796), where parents could sign up for other early education services in their community (DHHS, 2010).
Following the completion of random assignment and obtaining informed consent from parents, local measurement teams were comprised of interviewers/assessors and observers. Under the supervision of a field site coordinator, the measurement teams completed the data collection tasks in each of the 25 geographic areas that comprised the study sample for each data collection wave. Data collection for the HSIS began in fall 2002 and continued through spring 2006, following the same children from age of entry into Head Start through the end of first grade. Comparable data were collected on parents of the 3- and 4-year-old child study cohorts randomly assigned to both the Head Start intervention group and the control group. The parental experience variables were collected by conducting in-person parent interviews (DHHS, 2010).
Target Sample
The current study used two HSIS data cohorts, data collected in 2002, which provides the initial child and family baseline information, and data collected in 2005, which provides maternal experiences for all parents of 3- and 4-year-old children. Between the initial HSIS data collection in fall of 2002 (n = 4,442) and the data collection in spring 2005, 899 families dropped (attrition 20.2%) from the HSIS, resulting in 3,576 families remaining in the study sample (Head Start treatment group = 2,211 [61.8%], control group = 1,365 [38.2%]). Among 3,576 families, 579 families were teenage mothers (Head Start = 324, non-Head Start = 255) and 2,997 families were nonteenage mothers (Head Start = 1,798, non-Head Start = 1,199).
The authors applied to the institutional review board (IRB), and the IRB determined that the activity described in the application (study number: 00003796) was not “research” according to the Common Rule as codified in the DHHS regulations for the protection of human research subjects. This is the case since the current study obtained secondary deidentified data from the HSIS, the activity does not involve research data as defined by the DHHS [45.CFR.46.102(f)]. The HSIS data were collected using ethical standards and approved channels, and since our data utilized this deidentified data, there are no anticipated ethical concerns for this study.
Measures
Data collection for the HSIS began in fall 2002 and continued through spring 2005, following the same children and their parents from age of entry into Head Start to first grade. Data were collected based on face-to-face interviews conducted by professionally trained interviewer/assessors approximately 1-hr in length, with a parent/primary caregiver living with and responsible for raising the study children. Interviews typically were conducted in the family’s home, or alternatively, if the parent preferred, in a suitable public location (DHHS, 2010). The respondents were mothers (92.4%), fathers (4.3%), and others (e.g., grandparents, relatives) in 2002 and mothers (91.7%), fathers (4.1%), and others in 2005. For the current study, baseline variables measured in 2002 and parental experiences measured in 2005 were used. Among 3,576 families, no response rate for the study variables was between 0.3% (safety practice) and 2.1% (informal social support).
Parental Experiences
Informal social support
Parents were asked to rate how helpful the following individuals were: spouse, mother, father, grandparents, other relatives, friends, social workers, religious groups, and others. Parents responded to questions such as “How helpful is your spouse/partner?” “How helpful are social workers?” and “How helpful are religious/social group members?” using a rating scale from 1 (not very helpful) to 3 (very helpful). Total informal social support scores were comprised by adding the perceived helpfulness for each item.
Formal social service use
Parents were asked whether they received any of the following services over the past year (1 = yes, 0 = no): income assistance, nutrition assistance, housing assistance, utilities, job training, alcohol/drug abuse services, mental health services, family violence services, and foster care payments. Total social service utilization scores measured in 2005 (range 0–7) were computed by adding all individual items.
Parental safety practices
Parents answered a 10-item scale that assessed how often 10 different safety precautions were used, which included keeping harmful objects out of reach, using car seats, supervising the child during bath time, and having a first aid kit and working smoke detector at home. Possible responses ranged from 1 (never) to 4 (always). Mean parental safety practice scores were computed by averaging all individual items.
Parental depression
The shortened, 12-item, version of the Center for Epidemiological Studies’ Depression Scale (CES-D) was used to measure parental depression. The CES-D was originally published by Radloff (1977) and asks caregivers to rate how often over the past week they experienced symptoms associated with depression, such as restless sleep, poor appetite, and feeling lonely. Response options ranged from 0 to 3 (0 = rarely or none of the time, 1 = some or little of the time, 2 = moderately or much of the time, 3 = most or almost all the time). Total scores were computed by adding all scores for 12 items.
Neglectful parenting style
Parents were asked to respond to selected items from the Child-Rearing Practices Report (Dekovic et al., 1991). Parents answered items such as “I teach my child that misbehavior or breaking the rules will always be punished one way or another” and “I believe physical punishment to be the best way of disciplining” using a Likert-type scale that ranged from 1 (exactly like you) to 5 (not at all like you). Parenting styles were derived using Baumrind’s (1971) typology to assess the degree to which the two dimensions of warmth (nurturing and supportive behaviors) and control (disciplinary strategies, restrictive behaviors) exist in the parent–child relationship based on parents’ reports. Neglectful parenting was classified if parents were low in both warmth and control.
Baseline Variables
Parental characteristics such as maternal race (1 = white, 2 = black, 3 = Hispanic), education (1 = less than high school, 2 = high school graduated, 3 = college or more education), and marital status (1 = married, 0 = else) were included. Family characteristics included language spoken at home (1 = English, 0 = else), recent immigration status (1 = recently immigrant mothers, 0 = else), residential location (1 = urban, 0 = rural), monthly family income, and household risk factors. Household risk index was determined by the number of the following characteristics reported in the baseline parent interview, these included (1) receipt of Temporary Assistance for the Needy Families or Food Stamps, (2) neither parent in household has high school diploma nor a GED, (3) neither parent in household is employed nor in school, (4) the child’s biological mother/caregiver is a single parent, and (5) the child’s biological mother was age 19 or younger when child was born. A total household risk index score could range from 0 to 5 points. Three categories were created: low/no risk (0–2 risk factors), moderate risk (3 risk factors), and high risk (4–5 risk factors). All baseline variables were measured when children were 3–4 years old during in-person parent interviews that were conducted in the fall of 2002 (DHHS, 2010).
Analysis
T tests were used to compare the baseline characteristics between teenage mothers and nonteenage mothers. Regression analyses were used to determine whether parental experiences differ between teenage mothers and nonteenage mothers after controlling for all baseline characteristics (Research Question #1). Linear regressions were conducted for safety practices and maternal depression, loglinear regression was used for informal social support and formal social service use, and logistic regression was used for neglectful parenting practices. Control variables included maternal race, education, marital status, language spoken at home, immigration status, residential location, family income, and household risk factors. To examine the associations between Head Start and maternal experiences, interaction effects between Head Start enrollment and status of teen mothers were entered in the model (Research Question #2). Analyses were conducted using SPSS Version 25, and missing data were treated with the listwise deletion method.
Results
Characteristics for the Sample
As shown in Table 1, there were significant differences between teenage mothers and nonteenage mothers for most baseline variables. The percentage of teenage mothers was higher for black mothers (38% vs. 28%) and lower for Hispanic mothers (28% vs. 37%, p < .001). Compared to nonteenage mothers, teenage mothers were less likely to be married (46% vs. 82%, p < .001). Teenage mothers were more likely to have less than a high school education (46% vs. 37%) and less likely to have a college degree or higher education (21% vs. 30%, p < .001). Teenage mothers were more likely to speak English at home (67% vs. 83%, p < .001), less likely to be an immigrant (11% vs. 21%, p < .001), less likely to live in urban areas (81% vs. 84%, p < .05), and more likely to have lower household incomes (US$1,728 vs. US$1,890, p < .001) than nonteenage mothers. Compared to nonteenage mothers, teenage mothers had high household risk factors (33% vs. 3%) and were less likely to have fewer household risk factors (37% vs. 81%).
Descriptive Information on Study Variables Between Teenage Mothers and Nonteenage Mothers.
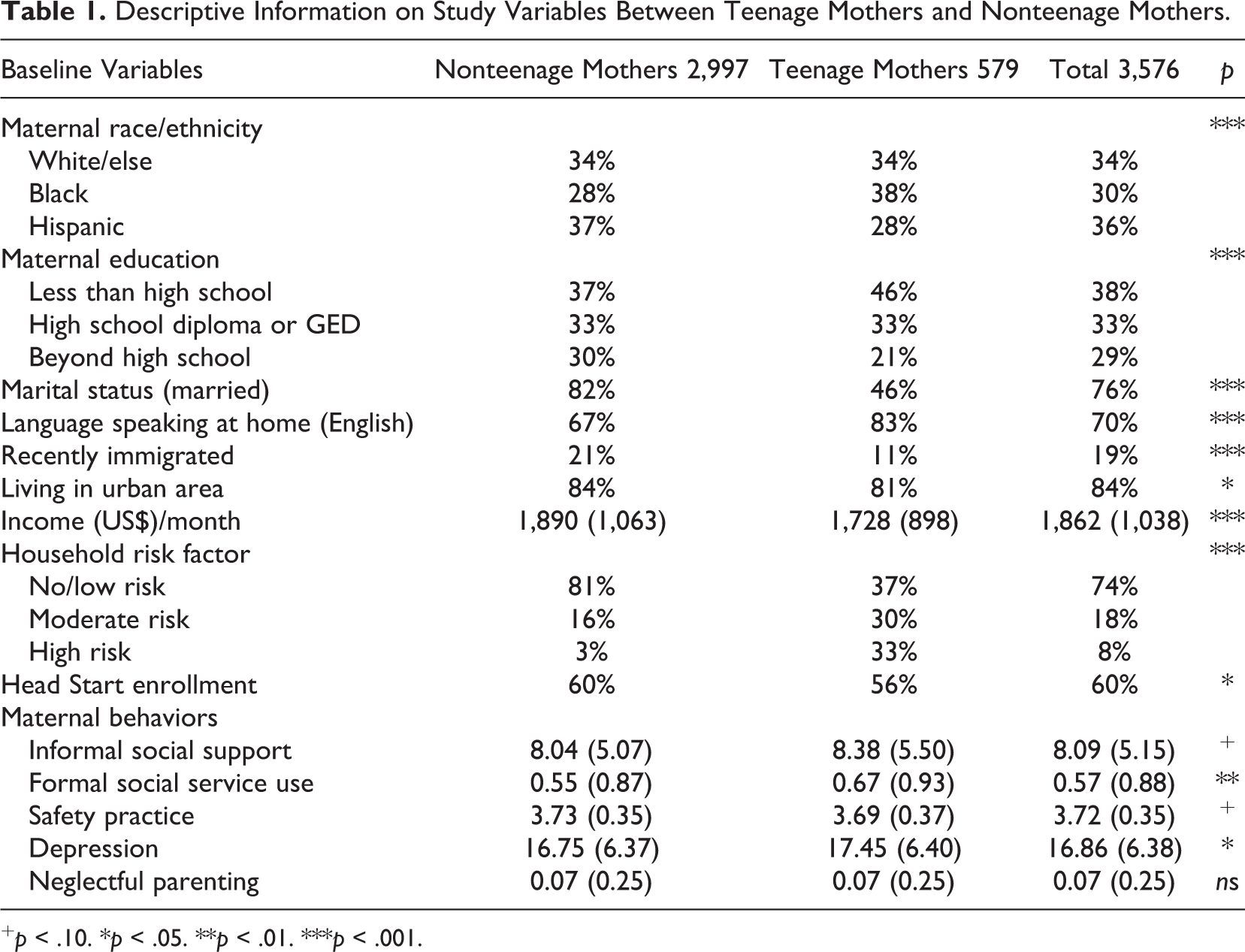
+ p < .10. *p < .05. **p < .01. ***p < .001.
Research Question 1: Parental Experiences Between Teenage and Nonteenage Mothers
Table 2 indicates that teen mothers had less informal social support (b = −0.05, SE = .02, p < .001) and used less formal social services than nonteenage mothers (b = −0.19, SE = .07, p < .01). Compared to nonteenage mothers, teen mothers had lower rates of depression (b = −1.29, SE = .35, p < .05). Teen mothers used marginally more safety practice support (b = 0.03, SE = .02, p < .10) and provided less neglectful parental practices support (b = −0.41, SE = .22, p < .10) than nonteenage mothers. Mothers identifying as white had significantly more informal social support (b = 0.09, SE = .02, p < .001), used more formal social services (b = 0.20, SE = .07, p < .01), provided safer parenting practices (b = 0.05, SE = .02, p < .001), and used neglectful parenting practices (b = 0.43, SE = .20, p < .05) than those identifying as Hispanic. Compared to mothers who had more education, mothers who had less than a high school education had less informal social support (b = −0.12, SE = .01, p < .001), used more formal social services (b = 0.20, SE = .06, p < .001), and had higher depression rates (b = 0.90, SE = .29, p < .01).
Parameter Estimate, Standard Error, and 95% Confidence Interval Predicting Associations Between Head Start Enrollment and Parental Experiences.
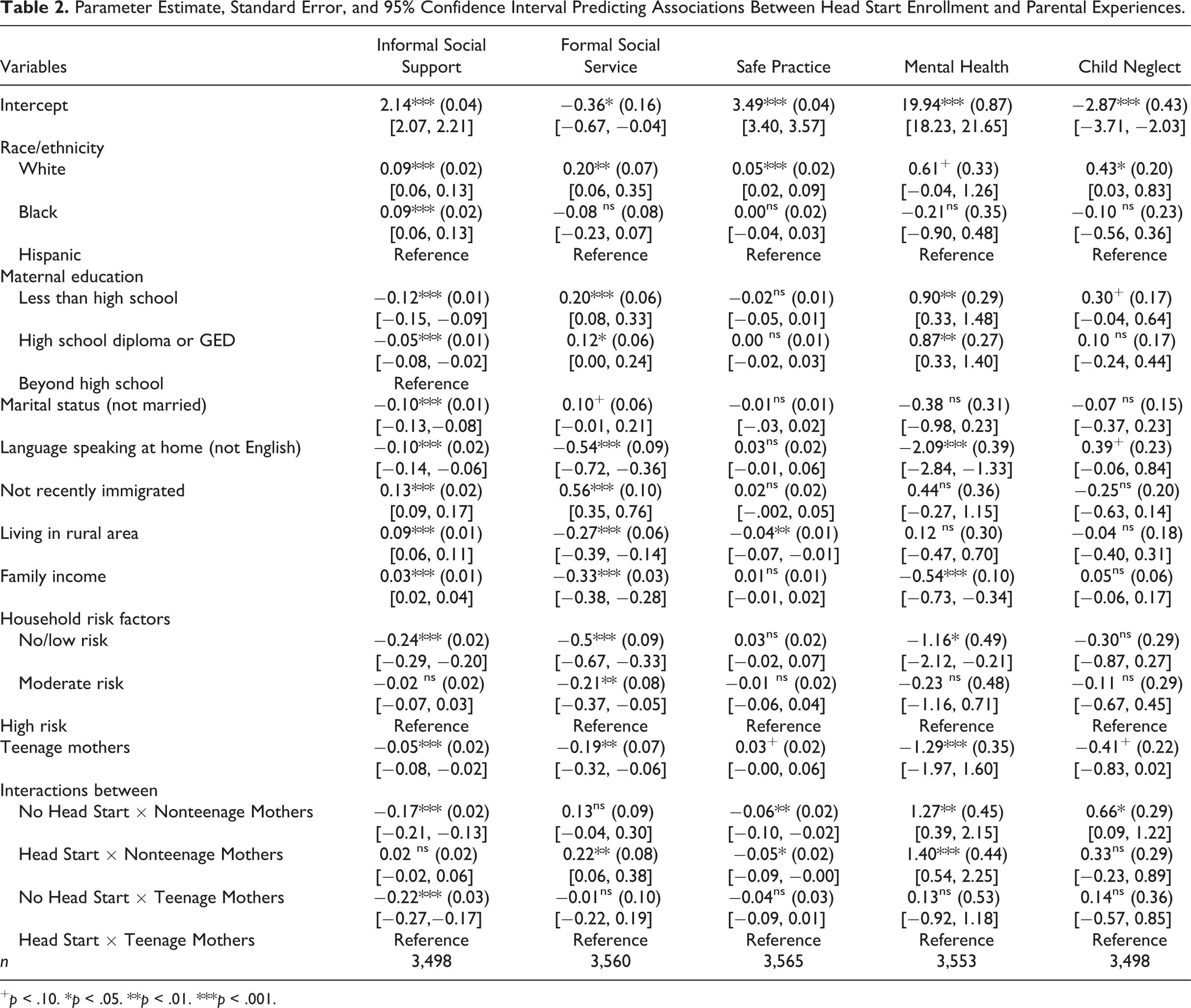
+ p < .10. *p < .05. **p < .01. ***p < .001.
Mothers who spoke a language other than English at home had less informal social support (b = −0.10, SE = .02, p < .001), used less formal social services (b = −0.54, SE = .09, p < .001), reported lower depression rates (b = −2.09, SE = .39, p < .001) than English speaking mothers. Recent immigrant mothers had less informal social support (b = −0.13, SE = .02, p < .001) and used less formal social services (b = −0.56, SE = .10, p < .001). Mothers who live in rural areas had more informal social support (b = 0.09, SE = .01, p < .001), used less formal social services (b = −0.27, SE = .06, p < .001), and used less safe parenting skills (b = −0.04, SE = .01, p < .01). Mothers who had higher family incomes had more informal social support (b = 0.03, SE = .01, p < .001), used less formal social services (b = −0.33, SE = .03, p < .001), and reported lower depression rates (b = −0.54, SE = .10, p < .001). Mothers who have fewer household risk factors had less informal social support (b = −0.24, SE = .02, p < .001), used less formal services (b = −0.50, SE = .09, p < .001), and had lower depression rates (b = −1.16, SE = .49, p < .05).
Research Question 2: Head Start Associations With Experiences of Teen Mothers
Head Start enrollment was associated with informal social support for teen mothers. As shown in Figure 1, compared to those who did not participate in Head Start, teen mothers who participated had more informal social support (M = 9.12 vs. M = 7.34, p < .001). Figure 2 indicated that compared to nonteen mothers who did not participate in Head Start, nonteen mothers who participated in Head Start used more formal social services (37% vs. 40%, p < .10). For teen mothers, the difference between Head Start and non-Head Start was not significant. Figure 3 shows Head Start was significant for nonteenage mothers (11% vs. 8%, p < .05) who participated in Head Start compared to those who did not (7% vs. 6%, ns).
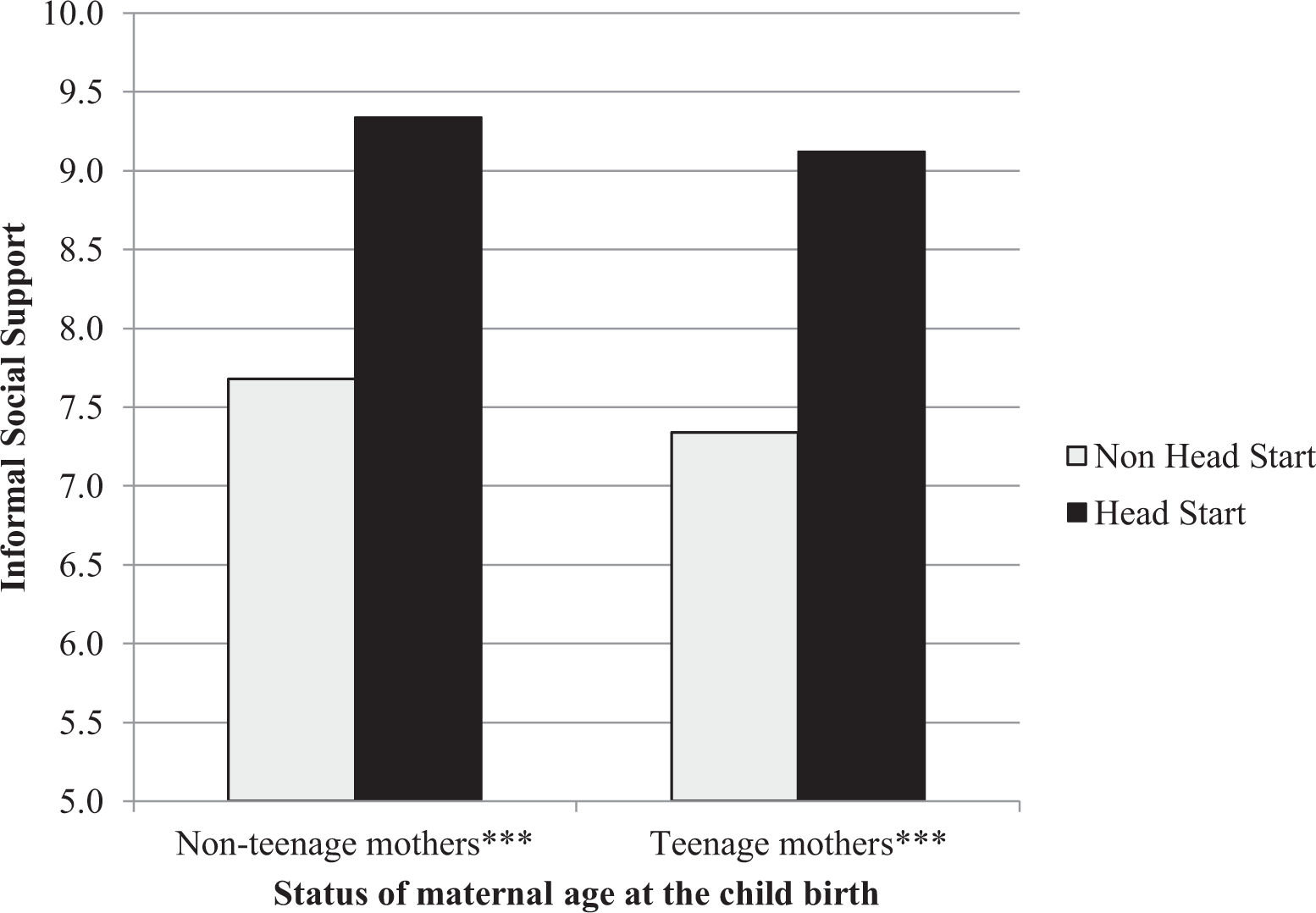
Interaction effects between Head Start enrollment and teenage mothers on informal social support. ***p < .001.
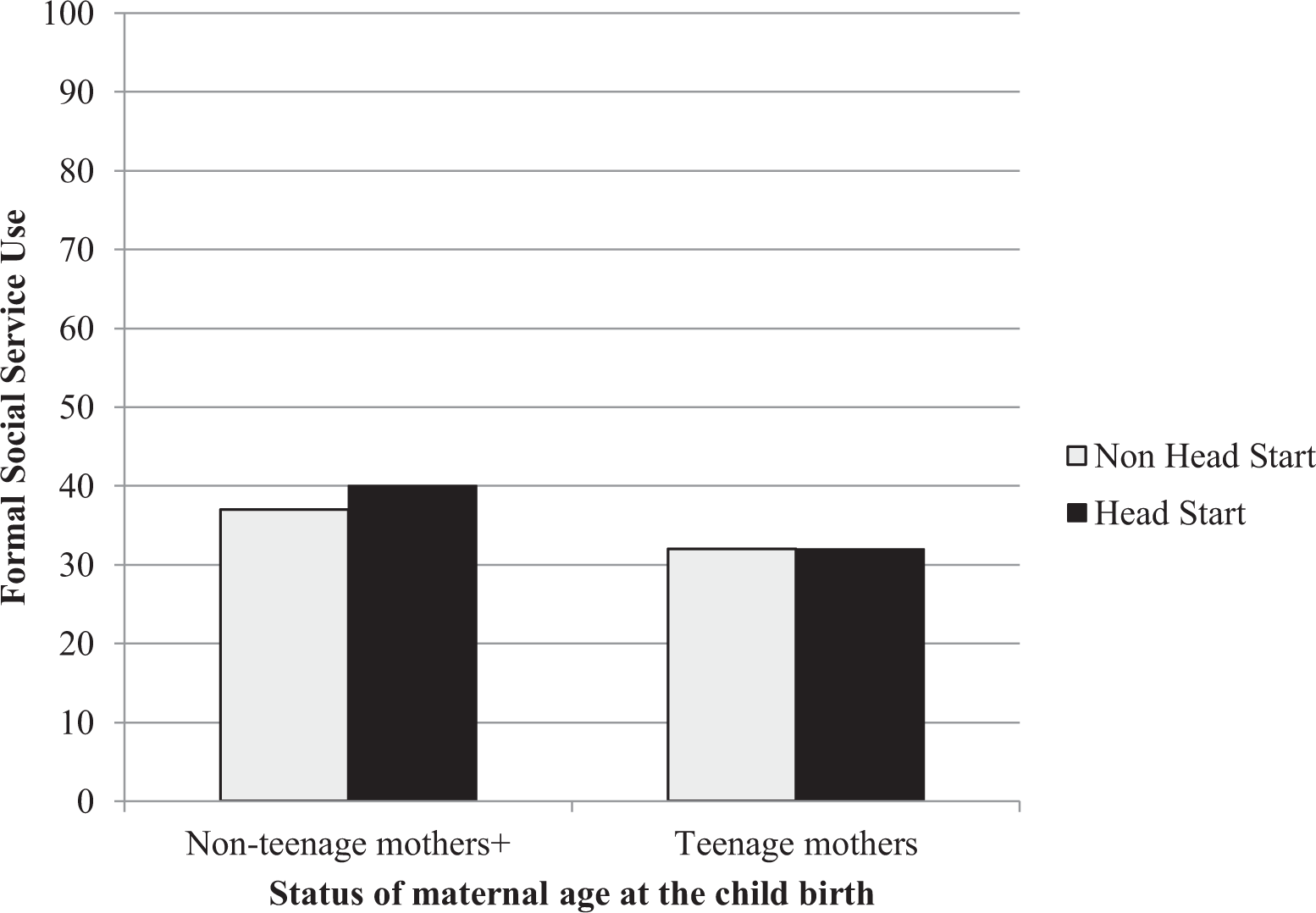
Interaction effects between Head Start enrollment and teenage mothers on formal social service use. + p < .10.
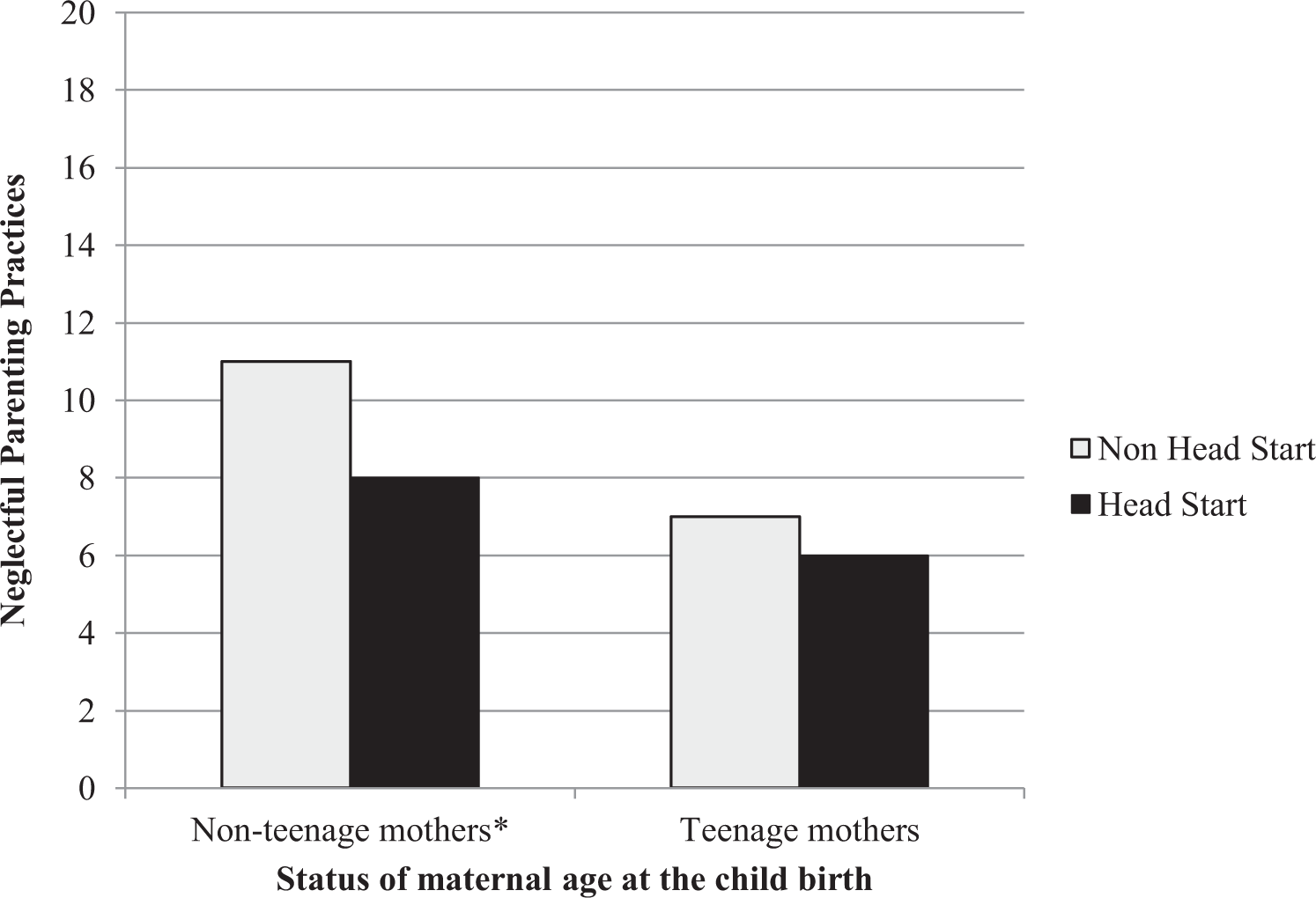
Interaction effects between Head Start enrollment and teenage mothers on neglect parenting practices. *p < .05.
Study Limitations
Although the current study utilized HSIS data which used a multistage cluster sampling, the teen mother variable was not used as a separate cluster. Accordingly, proportionally fewer teen mothers were included in the current study. Thus, selection bias could have occurred between teen mothers who enrolled in Head Start and those who did not. Despite various baseline variables being controlled, findings should be interpreted considering this potential selection bias. Although the primary respondents were mothers (more than 90%), parental experience variables were also collected from fathers or grandparents which might under- or overestimate parental experiences.
Further, the survey question from the HSIS data for the parental safety practices did not specify a time frame in a week, day, or year format, which could result in significant variances. Informal social support and formal social service use variables were based on self-report on conceptual satisfaction about social supports and the number of social services used. Which may alter study findings as some teens may have more barriers to accessing social support, and the HSIS data did not have data on the equity of the resources and the need for social support and social services. In addition, the HSIS data do not provide the same level of data on fathers as mothers; therefore, this study is limited in its ability to analyze Head Start’s associations with teenage fathers’ experiences. Due to lack of data, we were not able to classify which Head Start program component (number of times enrolled in parental workshop, type of workshop enrolled) which may have affected teen mothers. Furthermore, this article views teenage mothers as a homogenous group without examining the differences such as race and ethnicity. In addition, the HSIS data do not provide the same level of data on fathers as mothers; therefore, this study is limited in its ability to analyze Head Start’s associations with teenage fathers’ experiences. Due to lack of data, we were not able to classify which Head Start program component (number of times enrolled in parental workshop, type of workshop enrolled) which may have affected teen mothers. Furthermore, this article views teenage mothers as a homogenous group without examining the differences such as race and ethnicity.
These survey limitations should be considered when interpreting study results. A future study that specifically targets teen mothers based on randomized intervention study should be conducted to fully understand the resilience and risk factors of teen mothers as well as the associations of Head Start with teen mothers’ experiences. Despite these limitations, our study contributes to the literature on teen mothers and Head Start by utilizing a high-quality data set, which makes this study unique and significant for the well-being of teen mothers.
Discussion
Teen Mothers’ Characteristics
Our study found that teen mothers in this sample had less education, lower family incomes, and were less likely to be married, which corresponds with previous research (Combs et al., 2018). However, these findings could be correlated with the fact that disadvantaged teens are more likely to get pregnant and therefore, many of these experiences may have been present for these teens even if they were not mothers (Anastas, 2016; Bonell, 2004; Breheny & Stephens, 2007; Duncan et al., 2010). Therefore, social, individual, and contextual contexts of teen mothers are critical for programs and policies for teen mothers to consider (Breheny & Stephens, 2007), and Head Start seeks to incorporate each of these contexts in its interventions since it uses ecological and two-generational approaches.
Teenage mothers in this study were most likely to identify as black and least likely to identify as Hispanic, partially agreeing with previous research that shows the highest teen pregnancy rate is among black females (Combs et al., 2018). However, Combs et al. (2018) found Hispanic females to have the second highest rates and white females to have the lowest teen pregnancy rates, which do not align our finding. This discrepancy could be due to Head Start being a formal social service, and formal service utilization rates among Hispanics tend to be lower due to factors of stigma, cultural differences, and language barriers (Gordon, 2017).
Additionally, in the current study, teen mothers were more likely to speak English at home. Of the study’s sample, 86% of children born to teen mothers came from English-speaking households, showing that Head Start locations may not have the capabilities to run their program in other languages or may be choosing to not be accessible to those who do not speak English (Flores et al., 2005). Professional staff involved with programs should provide non-English speaking options, hire more bilingual staff members, and promote inclusion in their programs of non-English speaking parents and children.
Teen mothers in this study were more likely to live in rural areas than urban areas, which corresponds to previous research indicating that teen births are higher in rural areas (Santhanam, 2016). There are few effective programs for early education in rural communities, creating childcare deserts in rural America that correlate to increased poverty and lower cognitive and social–emotional skills for children and parents in these areas (Malik et al., 2018).
Parental Experiences for Teen Mothers
The current study found that teen mothers tend to have less informal social support and use less formal social services than nonteenage mothers, which corresponds with previous literature (Angley et al., 2015; Leplatte et al., 2012). This finding may be due to disadvantaged teen mothers having less accessibility and awareness to affordable programs that they qualify for (Kim et al., 2018; Santhanam, 2016). Furthermore, teen mothers may report less formal and informal social support due to high rates of stigma and discrimination that typically happen in the United States against this group (Anastas, 2016; Breheny & Stephens, 2007).
Our study found that teen mothers reported lower mental health problems, used more safety practices, and provided less neglectful parenting practices compared to nonteenage mothers. These findings contradict research suggesting that teen mothers experience higher rates of depression than their peers (Hipwell et al., 2016; Hodgkinson et al., 2014) and instead aligns with more strengths-based research that indicates teen mothers show resilience, growth, care for their children, and have more positive mental health experiences (Arai, 2009; Breheny & Stephens, 2010; Shea et al., 2015; Sniekers & Rommes, 2020). Overall, professionals should recognize the strengths of teen mothers and work to target these in interventions as well as decrease the stigma and discrimination as a whole surrounding mothering as a teen (Breheny & Stephens, 2010).
Head Start Association With Parental Experiences
As a whole, Head Start was not associated with teen mother’s parental experiences, except informal social support (Figure 1). That is, teen mothers who attended Head Start reported increased informal social support compared to teen mothers who did not attend the program. Additionally, Head Start nonteenage mothers used more formal social services, used more safety practices, and provided less neglectful parenting than nonteenage mothers who did not participate in Head Start. These findings indicate that perhaps Head Start is not as effective for teen mothers as is it for nonteen mothers. Research has shown that programs are most effective with participants who are at greater risk for the target problems the intervention was designed to address (Shelleby & Shaw, 2014). Therefore, programs such as Head Start should assess the strengths and needs of enrolled teen mothers to better design and implement evidence-based interventions that most effectively address teen mothers’ concerns (Breheny & Stephens, 2010). In this way, by including the voices of teen mothers, Head Start can better serve this population.
Implications
This study contributes to feminist theory since teen mothers are frequently stigmatized and discriminated against in many societies (Anastas, 2016; Breheny & Stephens, 2007), and our study supports the idea that teen mothers are not deficient, and instead programmers and policy makers need to incorporate these female voices more to assess the needs and contextual contributors to these teenagers becoming pregnant (Arai, 2009; Breheny & Stephens, 2007). Further, this study adds to the strengths-based literature, as it supports research indicating that teen mothers display many strengths including resilience, care for their children, and positive parenting behaviors (Rolfe, 2008; Shea et al., 2015; Sniekers & Rommes, 2020).
This study showed that Head Start promoted positive parenting experiences among nonteen mothers; however, the program was not significantly associated with positive parental experiences for teen mothers, except an increase in reports of informal social support. Head Start is one of the few programs designed for disadvantaged, low-income populations, which provides an optimal opportunity for the program to recruit more teen mothers, ask them what their needs are, and target these specific problems with individual and contextual factors in mind. However, in its current form, Head Start is not seeming to implement this approach fully across all centers, as teen mothers were not found to significantly benefit from the program. If Head Start implements more strengths-based and feminist approaches by incorporating voices and assessing discrimination and stigma against teen mothers, the program could better accomplish its goal of stopping the cycle of poverty among vulnerable populations (Breheny & Stephens, 2010).
The current study showed that Head Start is not receiving optimal enrollment from minority groups of teen mothers. Thus, centers utilizing Head Start curriculum should assess whether they are recruiting and raising awareness in minority neighborhoods, if their program is inclusive and offers bilingual options, and if staff perspectives of teen mothers are from a strengths-based model, not a deficit model. Furthermore, Head Start and other federal programs need to ensure that they are affordable and accessible to teen mothers with limited English proficiency and those living in rural areas. Current enrollment statistics and our findings show that there are limited numbers of teen mothers enrolling in Head Start, and it is the program’s responsibility to ensure they are raising awareness and explaining eligibility requirements to this population in an inclusive and strengths-based manner.
Social Workers’ Role
Social workers were once viewed as experts on teen pregnancy and teen motherhood; however, at some point, there was a pedagogical shift to a more deficit-based research and practice approach (Anastas, 2016). This shift negatively affects disadvantaged populations on various levels, with Hispanic and black teen mothers being the most likely to receive inadequate services since this perspective increases stigma and discrimination against them. On a macrolevel, social workers should promote feminist theory in research and practice by decreasing their own unintentional stigma and discrimination against teen parents and encouraging teen parents to share their voices in safe spaces (Anastas, 2016). The first step to changing deficit-based perspectives is for the social work profession to take a strengths-based, empirical stance against the concept that teen parenthood is inherently negative. Instead, social workers should promote more funding for programs that assist teen parents and their children in inclusive ways and ensure teen voices are considered when deciding which services to provide (Anastas, 2016).
Furthermore, social workers need to utilize research to show policy makers and society as whole that teen pregnancy is not necessarily the cause for poor outcomes, and disadvantaged teens are the victims of poverty and larger systemic problems (Breheny & Stephens, 2010). This call for action does not discourage the use of preventative programs but instead encourages social workers to support teens by advocating for low cost, accessible contraception under the stance that teen sexual activity is normal (Fox et al., 2019).
On both macro- and microscales, social workers need to respond to the needs of teen parents and their children by taking their opinions into account when designing and implementing programs (Bonell, 2004). Research shows that teen mothers are constantly lacking support from formal agencies, schools, and organizations (SmithBattle, 2006). Therefore, school social workers are uniquely positioned to link teen parents to resources and advocate for more inclusive and strengths-based models to be put in place to lessen stigma and promote high school graduation. Furthermore, when social workers are creating programs, it is imperative that they are aware of the terminology they use. For instance, when interventions say they focus on helping “troubled families” or promote “good parenting,” these statements are insensitive and highly stigmatizing of teen parents since they make assumptions of the family (Rudoe, 2014). Inclusive, strengths-based language should be the focal point in interventions seeking to help this population to ensure they are not stigmatized and discriminated against in these spaces.
Finally, social workers should seek to raise awareness of accessible, affordable, and inclusive programs for rural, minority, and disadvantaged populations. To follow the National Association of Social Workers’ Code of Ethics, social workers should ensure they are providing adequate, nondiscriminatory resources to disadvantaged populations and if there are no programs in existence, social workers are in a unique position with the ability to advocate for funding to create the necessary programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.