
Abstract
There are many impediments to family planning uptake by migrant women, which are likely to hinder their right to decide and use contraception. In this study, the authors investigated migrant women’s family planning practices. The researchers conducted 22 qualitative interviews with migrant female head porters in a suburban community in Ghana. Our analysis showed that a combination of social and cultural barriers impede effective family planning uptake by migrant female head porters. Further analysis revealed institutional challenges as constraining in access to and utilization of family planning services by migrant female head porters. Based on our analysis, we conclude that migrant female head porters face many barriers to family planning uptake and thus recommend that the government of Ghana (Ministry of Health), policy makers, and other stakeholders take measures to ensure universal access to sexual reproductive health services and reproductive rights.
Sociocultural norms and beliefs largely influence family planning decisions among internal economic migrants in Ghana. The migration trajectory from north to south is highly dominated by women, indicating a great departure from the previous trends which showed dominance by men. Records from the Ghana Living Standards Survey show a higher percentage (43%) of female migrants from northern Ghana as compared to male migrants (37%) from the same region (Ghana Statistical Service [GSS], 2008). Women migrate to escape poverty, harmful cultural practices and to seek better welfare prospects in the south (Awumbila & Ardayfio-Schandorf, 2008; Owusu-Ansah & Addai, 2013; Yeboah, 2010).
Economic migrants to the south find employment opportunities in the informal economy, as head porters (individuals, typically women, who carry wares and goods for retailers and consumers from one place to the other for a fee), domestic workers, bartenders, and street hawkers (individuals who sell merchandise or products on the streets; Adaawen & Jorgensen, 2012). Despite these prospects, women migrants still face challenges associated with lack of decent accommodation, poor working conditions (Owusu-Ansah & Addai, 2013), and limited access to family planning services (Lattof et al., 2018).
Family planning promotes the well-being of individuals and communities, making access to services important. Family planning services may encompass the provision of contraception, pregnancy testing and counseling, infertility services, sexually transmitted infections prevention, and pre- and postnatal services (World Health Organization, 2005). In this article, we focus on contraception as an important dimension of family planning. Specifically, we refer to decisions on the number and spacing of children using modern contraceptive methods (e.g., injectables, pills, condoms, and intrauterine devices [IUDs]), with the exception of elective abortion which is not considered. Ghana has made strides toward achieving universal access to family planning services. The most recent initiative is the Ghana Family Planning Costed Implementation Plan 2016–2020, aimed at providing high-quality, rights-based family planning information and services (Ghana Health Service [GHS], 2015). However, access by migrants is still limited due to their vulnerability, discrimination, and limited health care (Lattof et al., 2018; Owusu-Ansah & Addai, 2013; The United Nations Development Programme, 2009).
Review of the Literature
Social and Cultural Constraints to Family Planning
Even though much research on internal migration has been conducted in Ghana (Adaawen & Jorgensen, 2012; Awumbila & Ardayfio-Schandorf, 2008; Kwankye et al., 2007; Lattof et al., 2018; Owusu-Ansah & Addai, 2013), little is still known about family planning behaviors of migrant populations. Given that migration alters reproductive health decisions, including contraceptive use, it is important and beneficial to explore constraints to family planning among migrant women. This is because access to family planning services is largely limited among migrant women due to some social and cultural factors that may be linked to the migratory process (White et al., 2005).
The process of migrating can predispose migrants to other social, financial, and cultural challenges that may influence access to and utilization of reproductive health services (Unnithan-Kumar, 2015; White et al., 2005). These social and cultural factors are well-documented in literature and include religion, misinformation about the side effects of contraceptives and gender norms (Awingura & Ayamba, 2015; Martenowska et al., 2010; Omedi & Nyauchi, 2015; Omondi & Ayiemba, 2003; Roger & Earnest, 2014; United Nations Population Fund [UNFPA], (2013); Zhang et al., n.d.).
Several studies have reported the profound influence of religion on family planning decisions and use. The desire to conform to religious norms has different contraception outcomes for individuals who belong to different religious groups (A. A Bawah et al., 1999; Degni et al., 2014; Omondi & Ayiemba, 2003). Generally, in some African countries including Ghana, traditional beliefs (A. A Bawah et al., 1999), Christianity (Omondi & Ayiemba, 2003) and Islam (Degni et al., 2014) significantly influence family planning decisions. For example, a study in Ghana by A. A Bawah et al. (1999) established the nonutilization of modern contraceptives by women of reproductive ages (18–49) due to the “fear of the wrath of the gods.” This provides insights into how the reliance in traditions could adversely impact women’s decisions to use contraceptives (Omondi & Ayiemba, 2003). In Kenya, while studying the relationship between migration and the determinants of contraceptive use, Omondi and Ayiemba (2003) observed a low acceptance rate of contraceptives among Muslim migrant women compared to Protestant migrant women. They associated the high prevalence of contraception among Protestants to the religion’s flexibility in using contraceptives to regulate fertility and the low prevalence among Muslim women to Quranic restrictions that forbid contraception (Omondi & Ayiemba, 2003).
While family planning literature has documented actual health-related side effects of contraceptives (e.g., irregular bleeding, temporal cessation of menstruation, weight gain, headaches, nausea, and fibroids), researchers acknowledge the myths and misinformation surrounding their use within societies. These are often fueled by rumors and fear and to a large extent constrain contraception (Awingura & Ayamba, 2015; Farmer et al., 2015; Roger & Earnest, 2014). When contraceptives are perceived as physically and psychologically unfit (Roger & Earnest, 2014) and seem to interfere with sexual relationships (Farmer et al., 2015), users tend to refrain from using them. While examining motivations and constraints to family planning in Rwanda, Farmer et al. (2015) reported low acceptance of contraceptives due to their perceived interference with sexual relationships. Women participants in their study desisted from using contraceptives due to their experiences of low libido and vaginal dryness, which fueled fears of preference for other women by husbands (Farmer et al., 2015).
Studies examining the influence of gender norms on contraception highlight the importance of men and husbands’ agreement to contraception, which reinforces their control and dominance in reproductive health decisions (Awingura & Ayamba, 2015; A. A Bawah et al., 1999; Dereje et al., 2015; Eliason et al., 2014; Farmer et al., 2015). For example, Olaitan (2011) asserts that the higher the man’s involvement in family planning decisions, the more likely the decision to access and use contraceptives by the woman. This implies that the use of contraceptives without a husband’s approval as family head could lead to justifiable acts of physical abuse (Dereje et al., 2015; Owusu-Ansah & Addai, 2013; Roger & Earnest, 2014), preference for another wife, neglect by a male partner, and divorce (Awingura & Ayamba, 2015; A. A Bawah et al., 1999).
A study in Ethiopia by Dereje et al. (2015) reported physical abuse in the form of beatings as well as incidences of divorce among women who used contraceptives against their husband’s decisions. In Tanzania, Mosha et al. (2013) observed constant accusations of infidelity, which constrained women’s access and use of contraceptives. In this vein, A. A Bawah et al. (1999) argue that the fear of punishment and resistance from men are major factors contributing to women’s low contraceptive uptake.
Beyond physical abuse and accusations of promiscuity is the discrimination and stigmatization of women who seek services, particularly young women. A study in Rwanda by Farmer et al. (2015) reported low patronage of family planning services among women because of the stigma associated with seeking these services. Unmarried and young women are likely to be judged and labeled prostitutes when they attempt to seek family planning services (Mosha et al., 2013). Based on the literature, it is evident that accusations of infidelity of women who use contraceptives contribute to low acceptance of contraceptives.
Institutional Constraints to Family Planning
Evidence exists showing that lack of competency by health care providers, inadequate health care personnel, distance to facilities and times of operation, availability and accessibility to services act as barriers to family planning uptake (Awingura & Ayamba, 2015; Degni et al., 2014; Eliason et al., 2014). The cultural competency of service providers to address issues faced by minority groups is of significant importance to effective provision of family planning services. In a qualitative study of 70 Somali-born immigrant women’s experiences of reproductive health services in Finland, Degni et al. (2014) observed a general satisfaction with the availability of reproductive health services by participants, though challenges existed regarding the lack of cultural competence by the Finnish health care workers. Their findings further indicated complaints about the inappropriate and unfriendly attitudes of health care workers, which deterred participants from seeking family planning services.
Accessibility to health care facilities in terms of distance is another important determinant of contraceptive use (Awingura & Ayamba, 2015; Eliason et al., 2014). Eliason et al. (2014) adopted a case–control study to investigate the determinants of modern family planning methods among women of reproductive age. They established a likelihood of communities located within a distance of less than 5 km away from a family planning facility to use contraceptives compared to those located more than 5 km. Eliason et al. (2014) further observed that favorable operating schedules in terms of opening and closing times of facilities promoted contraceptive uptake, reaffirming the importance of providing tailored services in order to encourage utilization.
The reviewed literature has established that family planning uptake by women is influenced by many social, cultural, and institutional factors that affect women, regardless of location and status. In Ghana, while numerous efforts have been made to improve family planning access and utilization, uptake by women, particularly migrants, is still minimal. This underscores the importance of exploring constraints to family planning by migrant women.
Objectives of Research
To investigate the sociocultural norms and beliefs that influence decisions and use of contraceptives among northern migrant women in Madina.
To explore the institutional challenges that hinder access to family planning services by northern migrant women in Madina.
Method
To understand the decision-making processes of migrant women head porters in Madina, the researchers used qualitative methods. The main goal was not to make generalizations but rather to obtain insights into the phenomenon (Onwuegbuzie & Collins, 2007) since this phenomenon is underresearched.
Study Context and Population
The study was conducted in Madina, a suburb in Accra the capital city of Ghana, which has a high population of internal migrants. Statistics from the last (2010) population census indicate that out of a total population of 111,926, 73,545 are migrants who are attracted from all over the country to the area in search of jobs and other economic opportunities (GSS, 2012). This makes the La-Nkwantang Madina Municipality one of the most cosmopolitan municipalities in the country and a good site for this research. Madina is home to a popular market, where migrant women work as head porters transporting traders’ and customers’ goods from point A to B. The study population consisted of migrant female head porters between the ages 18 and 49, who were living in Madina and working within the market and had resided in Madina for a year or more. The study also included key informants who were officials from Ghana Health Services and Marie Stopes International, an organization that provides sexual and reproductive health care to underserved women. The key informants contributed important knowledge about the setting to the researchers who were outside observers (Patton, 2002).
Sampling Procedure and Sample Size
Participants were purposively selected based on the researchers’ criteria. Purposive sampling was adopted for two reasons (a) it is often associated with qualitative research and (b) it allowed the researchers to deliberately sample information-rich study units (Patton, 2002). Two gatekeepers helped the researchers to gain access to the research location: namely the Director and Administrator of Positive Action for Porter Girls (PAPG), an agency that provides services to female head porters in the Madina market.
Once access was gained, the researchers distributed information leaflets about the study to the head porters. Those who qualified and wished to participate were encouraged to write their names and telephone numbers on a sign-up sheet left by the researchers at the PAPG office. Subsequently, an informational session was held at PAPG to share details about the study after which interview dates, place, and time were scheduled according to participants’ convenience. The key informants were invited to participate through formal letters that were sent in person to their offices. This was followed by an exchange of phone calls and emails to verify participation, and finally, the setting of convenient dates and venues for interviews.
Scholars (Bryman, 2012; Creswell, 2007) assert that, for a research based on qualitative inquiry, 15–30 participants are sufficient and that, each unit in a qualitative study produces a lot of information, thus in order to undertake thorough and meaningful data analysis, sample sizes need to be kept reasonably low. It is based on this assertion that the researchers estimated 30 participants at the onset of the fieldwork. In the end, 22 were interviewed, consisting of 19 migrant women, two key informants, who were family planning providers, and one key informant from Marie Stopes International. Data collection from participants ended at 22 because saturation had been achieved, as no new themes were observed.
Methods of Data Collection and Analysis
The researchers used an interview guide to conduct in-depth interviews with migrant women and key informants. In-depth interviews were useful because they allowed the researchers to inquire about participants’ feelings, motives, and interpretations of events and to probe the responses given by participants (Green & Thorogood, 2009; Singleton & Straits, 2010). The in-depth interviews were conducted in both English language and “Twi” (a local dialect which is widely spoken in many parts of Ghana). The Twi interviews were translated into English during transcription for analysis. Qualitative analysis of the data was then carried out using Creswell’s (2009) thematic framework for qualitative data analysis. Data from the field were first transcribed, organized, and typed. The researchers then sorted the data and proceeded to search for patterns and arranged them into different categories based on the objectives of the study. The process was subsequently followed by a thorough reading of all the data. Reading through the data enabled the researchers to make sense of what the participants were saying, thus dictating the tone of ideas. The data then went through the coding process which involved the organization of material into sections of text; identification of recurrent words, concepts, or themes; and labeling them. Themes were then generated, and these were presented as the major findings of the study. Finally, an interpretation of the meaning of the data was carried out by relating the findings to the reviewed literature.
Researchers’ Positionality
In doing qualitative research, the values, philosophies, experiences, beliefs systems, and social identities of researchers cannot be ignored since these play a role in the way in which the research process is shaped (Palaganas et al., 2017). In this study, we assumed both outsider and insider positions. Our position as outsiders stemmed from differential social statuses (privileged academicians) in relation to that of the study participants. We considered ourselves insiders because of our identity as women with an interest in the welfare of migrant female head porters and our prior knowledge about some aspects of migrant female head porters’ lives. One of the researchers had previous encounters with migrant female head porters through other projects, which afforded us the opportunity to establish relationships and collect data with ease. At the same time, we were mindful and minimized the biases that could have occurred as a result of our compassion and empathy for participants. In acknowledging the potential influence of our individual circumstances on the research process, we reflected on our personal values and experiences through a process of journaling and debriefing after each day of fieldwork and throughout the research process.
Theoretical Underpinning
This study is grounded in Marxist feminists’ theoretical critiques of patriarchy, defined as male domination in both public and private arenas of social life (Sultana, 2010; Wilson, 2000). Feminist critiques of patriarchy serve an important lens through which the sociocultural and institutional systems that extremely favor men in Ghana are used as tools to control access to and use of reproductive health services including family planning. In developing countries of the global “South” for instance, patriarchy is largely characterized by certain cultural and social forms of male domination “rooted in kinship, production and ideology” (Wilson, 2000, p. 1495). Likewise, culture is very much pervasive in determining women’s disadvantaged position in society. Cultural practices in northern Ghana, for example, bridewealth and forced marriages typify patriarchy (J. Bawah, 2012) and limit women’s power to make family planning decisions. Scholars have argued that many societies in Africa are highly patriarchal and, as such, undermine women’s authority and decision-making power, particularly decisions related to family planning (Dereje et al., 2015; Farmer et al., 2015; Mosha et al., 2013). This suggests women’s lack of authority over fertility rights as these are the preserve of men, a fact that may prevail in northern Ghana, from where study participants come.
Results
Demographic Profiles of Participants
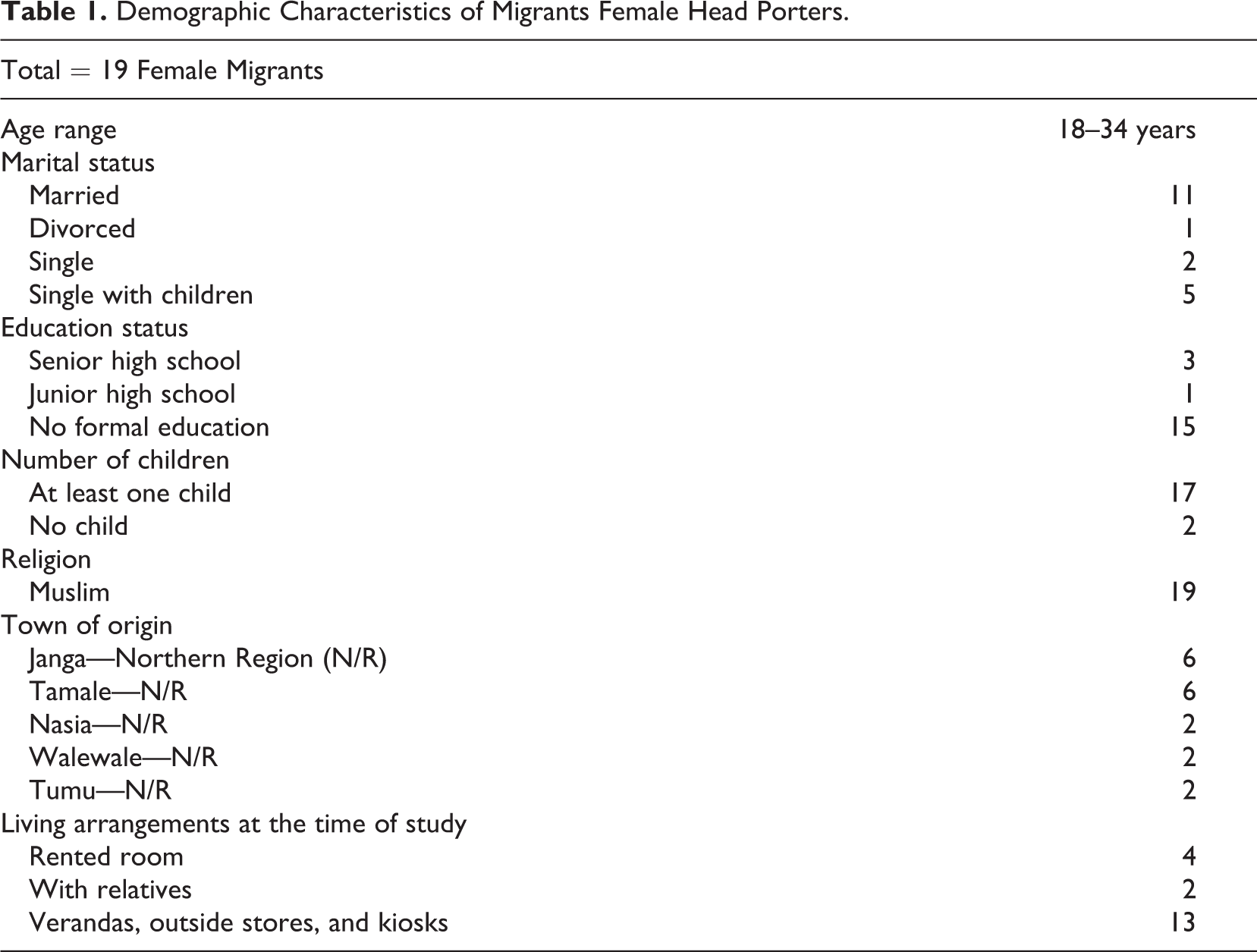
As presented in Table 1, 19 migrant women working as female head porters and three key informants, totaling 22, participated in the study. Two of the three key informants were family planning providers working in family planning units at clinics in the La-Nkwatanang (Madina) District as well as the Family Planning Regional Resource Personnel for Greater Accra Region. The other was a Youth Coordinator at Marie Stopes International, Ghana, and works on the “kayayei” (female head porter) project, which offers family planning and other reproductive health services to migrant female head porters. Most participants were married (57.7%), many had no formal education (79%), majority had at least one child (89%), and all identified as Muslim from various towns of the northern region of Ghana.
Demographic Characteristics of Migrants Female Head Porters.
Sociocultural Barriers to Family Planning Uptake
The three main themes that emerged as inhibitors of family planning uptake were (a) lack of partner’s consent, (b) misinformation about the side effects of contraceptives, and (c) association with promiscuity. These identified sociocultural factors influence migrant women’s decisions on contraception, which has implications for their autonomy and well-being.
Partner Consent
Participants cited how it is culturally appropriate to discuss and seek permission from a male partner before taking the decision to use contraceptives. Men as heads of households, according to the participants, should be the ultimate decision makers, and as such, their consent is considered important before decisions to use contraceptives are made. Findings of this study show that using contraceptives without the consent of male partners was a source of tension and conflict for the participants, leading in some cases to divorce or intimate partner violence. On the other hand, findings also show that when male partners consent and are involved in family planning, women can utilize with greater ease.
Divorce
Participants shared experiences of serious marital problems between couples and even the extended family as resulting from using contraceptives without spousal approval. Participants stated dissolution of marriage or divorce as the worst consequence of using contraceptives without permission from a male partner. Emphasizing the link between contraception without spousal consent and divorce, a participant affirmed: Husband’s permission is important; once permission has been sought and granted one can go ahead and use contraceptives. But if the husband disapproves, then there is no need to use contraceptives because it can result in divorce…. (Head porter, 9) Before using contraceptives, a woman should consult her husband because failure to do so would result in problems in the marriage. If you are not lucky, you can be sent packing out of the house. In my hometown one woman started using contraceptives without telling the husband, as I am speaking to you now, she is in her father’s compound, when the husband found out he threw her out of their marital home. (Head porter, 8) I have witnessed so many instances where female head porters were thrown out of their marital homes by their in-laws just because they used contraceptives. (Key informant 1, Marie Stopes International) As a woman, you have to talk to your husband and go and see the health worker, you select the method you want, but if the man refuses for you to use it, then you have to comply otherwise you will be divorced and sent back to your parents. (Head porter, 6)
Intimate partner violence
Intimate partner violence could also result from using contraceptives against a male partner’s objections. For many of the migrant female head porters, physical abuse such as beatings is real and impedes contraception. Male partners can even sometimes order the removal of methods such as IUDs, disregarding the woman’s feelings. One head porter disclosed how her sister-in-law endured beatings at the hands of her husband: …. you know up north, if you disregard your husband’s advice, it will land you in trouble, because he can decide to divorce or even beat you up. My sister in-law was beaten seriously by her husband when he found out she had inserted the IUD. He ordered her to go and get it removed if she wanted to stay in the marriage. (Head porter, 9) A woman should seek permission from her husband, because if the husband is not aware and complications arise, it can result in severe beatings from him. (Head porter, 16) Many female head porters do not get spousal consent. The husband or boyfriend warns them against using contraceptives. Therefore, decisions to use contraceptives without spousal consent by “kayayei” (head porter) contribute to intimate partner violence…. (Key informant 1, Marie Stopes International) For the migrant women especially, they are really in a deplorable situation. We try our best to help. Sometimes they come for counselling, but then they will be thinking that if my partner finds out he will beat or divorce me. They have so many fears about what their partners will do in case they find out that they are using family planning. (Key informant 2, Abokobi Health Centre)
Partner support and contraceptive uptake
Despite the lack of spousal support for many of the migrant participants, there were a few instances where partners or husbands were in support of family planning. For such women, it becomes easier to use contraceptives because there is a clear understanding and appreciation of the benefits associated with family planning between the parties. One such participant who had support from her husband explained his role in the selection of a contraceptive method: In some cases, it is the man who would encourage you to adopt family planning, so that you can take good care of the children. In my case, I got support from my husband and he even suggested a method for me. (Head porter, 2) Personally, I pleaded with my husband that I wanted to use contraceptives to space childbirth and he agreed. This gave me confidence to go for the pill, which I am currently using. (Head porter, 13) My husband supported me and today I have my two children. We are able to cater for them well. I am also free to work and earn more money. (Head porter, 10)
Contraceptive Uptake and Misinformation of Undesired Effects
Despite the fact that family planning education covers issues of its related benefits and effects (irregular bleeding, temporal cessation of menstruation, headaches, and weight gain) of various methods, rumors are usually the main source of information regarding the effects of contraceptives, particularly among migrant groups. Many migrant female head porters narrated how some family planning methods could result in irregular bleeding, cessation of the menstrual cycle, weight gain, infertility, injury to their partner’s manhood, and even death.
Rumors emerged as a deterrent to contraceptives use and served to scare the head porters from going for family planning methods. Concerns for weight gain, infertility, and death were expressed, though they were hearsay. Among the participants (n-17) who had taken contraceptives, two shared some negative effects they experienced because of contraceptives. None of the other participants (n-15) had experienced these undesired effects. The three excerpts below demonstrate some of the misconception surrounding the effects of contraceptives: I heard of someone who had the IUD inserted, that she gained so much weight. So, she was warned to go and remove it if she did not want it to affect her womb. (Head porter, 2) There is this incidence where one woman did family planning here in Accra and went back home. She got sick but did not mention that she did family planning until the sickness became serious. She then went to the hospital complaining of abdominal pain, after finally disclosing that she did family planning, she died. (Head porter, 7) Some of the men especially up north advise us not to use contraceptives because they claim it would make us infertile, they warn you that, if you hide and use contraceptive secretly, they will know because you will not be getting pregnant. (Head porter, 4) If a woman starts using contraceptives and she experiences bleeding, she becomes alarmed and tells everyone who comes around that, the bleeding is associated with this particular contraceptive. The fears spread like wildfire, and before you know it, all her friends and family would never like to use contraceptives. Sometimes, even their partners tell them that, when you go for contraceptives, especially the ones inserted in the uterus, the device will pierce their manhood during sexual intercourse. (Key informant 1, Marie Stopes International) I went for the 3 months injection. Please, to be honest with you, after doing it, I did not have my menses (no menstruation) for those 3 months. I also suffered from severe lower abdominal pains. Because of this experience, I decided to use the pill instead. The bitter experience had scared me from going for another injection. Since adopting the pill, I have not experienced any bad effects. (Head porter, 12) I got the IUD inserted and I began bleeding nonstop. When I told my sister, she said that it would affect my womb and I may not give birth again. I got scared and went back to Marie Stopes for it to be removed. I don’t think I will use any methods again for now. (Head porter, 14)
Contraceptive Use and Association With Promiscuity
The views on family planning uptake and its association with promiscuity are from the key informants who over the years have worked closely with migrant female head porters. Participants shared views on how accusations of infidelity often accompany the use of contraceptives and are often made by husbands, family members, friends, and even community members. The key informants affirmed that women who use contraceptives are accused of being prostitutes because of the belief that a married woman has no need for family planning. The same applies to single women who are not expected to engage in sexual activities: There is the belief that you are promiscuous when you use contraceptives, so it discourages many head porters from accessing services. I have witnessed so many instances where women were accused of being prostitutes and were thrown out of their marital homes by their in-laws just because they used contraceptives. (Key informant 1, Marie Stopes International) Female head porters’ inability to patronise family planning is mostly cultural, because when they migrate to Accra, they always move in groups, and once they see that you are practising family planning, you are in trouble. They will criticise you and say that you came to Accra to flirt with men that is why you are using family planning; they will then go and report you to your husband. (Key Informant 3, Madina Poly-Clinic) …. All those “kayayei” (female head porters) who come here, left their husbands in the north, so if a sister or friend knows that the husband is in the north, they would be wondering why the woman is using family planning. And you know in the north, the perception is that when you do family planning, it means you are a prostitute, implying that you want to go behind your husband and sleep around. (Key informant 2, Abobokobi Health Centre) We organized a programme for them here with Marie Stopes International; we gave them some T-shirts and money and gathered them outside on the benches. We then said they should come in the consulting room one by one and choose a family planning method. Ooh! Nobody was willing to take the service. They did not want their friends to know about their uptake because it would be reported to their husbands in the north. Some friends will even say that eei!, you came to Accra to do family planning, it means you want to flirt with men. (Key informant 3, Madina Poly-Clinic)
Institutional Challenges That Hinder Access to Family Planning Services by Migrant Women
There are problems inherent in reproductive health care institutions that are beyond migrant women’s control, which impede contraceptive uptake. These challenges stem from unfavorable locations and operation of family planning clinics and impede contraception by migrant women. In relation to institutional problems, two themes emerged, and these are (a) poor service provision by family planning nurses and lack of physical access.
Poor Attitudes of Family Planning Nurses
Despite the fact that many migrant female head porters do not have time to visit health facilities for family planning services, key informants were nonetheless in agreement that the poor attitudes of family planning nurses toward migrants contributed to low patronage of services. The nurses’ unfriendly and judgmental attitudes as well as a lack of good customer service skills discourage migrant women from seeking services: …. Then perhaps for me, the most painful thing is the way they are treated when they go to the hospital to take up family planning services. The attitude of the workers, the way they treat head porters, does not encourage patronage of family planning services. In some cases, they are treated with disdain as if they do not deserve access to such services. (Key informant 1, Marie Stopes International) Attitudes of family planning nurses are a major issue. Many head porters are young even though they may be married and have children. The Ghanaian culture frowns upon young people coming in at their own volition to access family planning services because it implies that they are spoilt. It is important to understand the cultural and religious backgrounds of these migrants so that we can be sensitive to their needs. The way health care providers sometimes talk harshly to migrants deters them from coming to the clinics for services. (Key informant 2, Abokobi Health Centre)
Lack of Physical Access
Lack of physical access in terms of proximity, opening and closing times, as well as days of opening was cited by the key informants as another major challenge that inhibits family planning uptake by migrant women. Many migrant women working as head porters are busy 6 days in a week (Monday to Saturday) and work very long hours. As a result, they have little time for other activities. The limited operating hours of many facilities impacted migrant women’s access: We also have problems with proximity in terms of accessibility, sometimes the facility is far from head porters, so they cannot come to us, and even accessibility in terms of closing times. Our times of opening and closing are not favorable to many migrant women. Some would like to come in the evenings, but here is the case that we open from 8 a.m. to 4 p.m., what can we do about those people? We therefore tend to sometimes extend our opening and closing times just to cater for their reproductive needs. (Key informant 2, Abokobi Health Centre) It is important to understand that population, it’s a different population because the primary reason they came to Accra is to make money. They spent 8–12 hr of the day working, meaning they don’t have time to come for family planning services. So, in dealing with them, it is important to go to them. (Key informant 1, Marie Stopes International) Often times, they do not have physical access to the facilities. The nearest facility around Agbobloshi (the main market in Ghana, where migrant female head porters ply their trade), where we work with head porters, is far away from where they work. They therefore cannot readily access services when the need arises. (Key informant 1, Marie Stopes International)
Discussion
Female head porters consistently expressed fear that using contraceptives without a husband’s permission could lead to marital and relationship problems. This was evident in participants’ narratives of how the use of contraceptives without the agreement of a partner could result in beatings, denial of affection, neglect, and divorce. The view that contraceptive use should be agreed to by men and husbands was expressed by many women in the study, even though a few noted that they would use contraceptives without seeking permission from a male partner. Women might feel that based on cultural or religious restrictions, it is inappropriate to initiate family planning discussions with spouses, reaffirming the role and importance of men in such decisions. These findings suggest that decision-making power by men and husbands on family planning and male dominance in decision making within the home among migrant women in Ghana constrain access to and utilization of family planning services by women. It is thus no surprise that they are unable to make independent decisions on family planning, corroborating findings on the importance of spousal agreement and consequences of using contraceptives without male partner approval by J. Bawah (2012), A. A Bawah et al. (1999), and Dereje et al. (2015) in Ghana and Ethiopia, respectively.
The participants shared concerns over the adverse side effects of contraceptives on men and women’s health and fertility. In this theme, participants focused on and cited instances where women reportedly had died, gained weight, bled irregularly, had physical injuries, experienced fertility problems, and in some cases cessation of the menstrual cycle, as a result of the use of contraceptives. These occurrences acted as deterrence to family planning uptake. Interestingly, for many participants, these fears were fueled by rumors from friends and family. This observation is in line with Roger and Earnest’s (2014) and Farmer et al.’s (2015) qualitative findings on how the fear of side effects of contraceptives prevents uptake and the overexaggeration and spread of these fears through hearsay among African migrant women in Australia and women in Rwanda.
Decisions to use contraceptives by migrant female head porters were associated with promiscuity and infidelity, which largely influenced uptake. Participants opined that such allegations made it difficult to access family planning services, as this could have ramifications for their marital statuses. Due to the nature of their economic activities, many female head porters resided in rented rooms with colleague head porters, while their partners lived elsewhere. Participants expressed fear of friends, family members, and husbands finding out about their contraceptive uptake, which could lead to accusations of prostitution and unfaithfulness. There was a widespread perception among migrant female head porters that, once women start using contraceptives, they become promiscuous as they can avoid pregnancy. These accusations can be viewed as mechanisms to control women’s reproductive health decisions, which corroborates evidence from Ghana by A. A Bawah et al. (1999) and Rwanda by Farmer et al. (2015), which pointed to the association between contraceptive use and accusations of infidelity or promiscuity, often leading to divorce among married women.
Even though women in urban areas are noted to have increased access to family planning services, there still exist institutional barriers such as poor provider attitudes and lack of physical access to such services. In this study, these were identified as challenges that hindered utilization of family planning services by migrant female head porters. Key informants described disrespect and ridicule by health care providers as barriers to family planning uptake. Even though migrant female head porters have limited time to visit health care facilities for family planning services, the poor attitudes exhibited by health care providers contributed to their reluctance in seeking services. It is also evident that lack of physical access in terms of proximity, opening and closing times, as well as days of opening were constraining to family planning uptake by migrant female head porters. The further away reproductive health care facilities are to migrants, the less likely they are to utilize services. Many facilities that provide reproductive health services are located far from where female head porters live and work, close early, and do not open on weekends, making it difficult for female head porters to access services. Findings on poor attitude of service providers and lack of physical access substantiate observations by Awingura and Ayamba (2015) and Eliason et al. (2014) in Ghana, Degni et al. (2014) on Somali immigrants in Finland, and Farmer et al. (2015) in Rwanda.
The findings from this study give credence to theoretical critiques of patriarchy developed by feminist scholars. The factors that inhibit migrant women’s access to and use of family planning as identified in this study have roots in the patriarchal system and organization of the Ghanaian society. This system is very much prevalent in northern parts of Ghana, where men have authority and decision-making power in all facets of social organization as observed by J. Bawah (2012) and A. A Bawah et al., 1999. The prevalence of male domination in fertility decisions explains the need for spousal approval and the public scrutiny, accusations, and humiliation women face when they go for family planning. Thus, the sociocultural and institutional factors found in the study help to maintain the patriarchal system in the Ghanaian society.
The findings from this study suggest that migrant female head porters’ ability to access and use contraceptives is mostly constrained by sociocultural and institutional factors. The empirical evidence from the study suggests that many migrant women working as head porters in Madina do not use contraceptives. Understanding the socioeconomic background of female head porters is crucial in providing effective family planning services. Since they are always on the move working, the best approach for effective service provision is to take the services to their doorsteps. The findings have demonstrated that migrant women lack decision-making power in reproductive health matters, and as such, their reproductive needs should begin to take center stage in policy dialogues.
Implications for Social Work Practice in Ghana
Findings from this study have demonstrated the social, cultural, and institutional impediments to contraceptive uptake by migrant female head porters in Accra, Ghana. These findings clearly underscore the importance of health social workers in implementing interventions that ensure universal access to family planning services by all social groups. Although social work as a profession in Ghana is still developing, the findings could provide empirical evidence about challenges to reproductive health access to social workers working within the Ghana Heaith Service in hospitals and other health facilities. Social workers in this sector have a responsibility to train reproductive health service providers to be better equipped with cultural competency skills that would enable them to identify and address cultural factors that limit minority groups’, in particular female head porters’ access to reproductive health services. This would ensure accessibility to reproductive health services that are affordable and best suited to the needs of such minority populations. Also, based on the current findings, social workers in the GHS in partnership with organizations such as Marie Stopes International could embark on training exercises around the country to sensitize family planning service providers on best practices in order to eliminate barriers associated with poor service provision.
Limitations of the Study
Although the study provides insightful evidence on constraints to contraceptive use by migrant female head porters in Ghana, it is not without limitations. First, since gatekeepers were used to gain access to the study location, there is a possibility of sampling bias. Regardless, we adhered to best practices in qualitative sampling in order to minimize any biases. Again, the scope for this study is limited to only modern contraception, except for abortion, which was not explored due to its sensitive nature, particularly among the study population. The translation of interviews during transcription from Twi to English might have resulted in some data loss because of the difficulty in finding the exact meanings of some words and phrases in either language. While this study has offered a broad perspective on family planning constraints on migrant female head porters in Ghana, the findings have limited generalizability to a wider section of migrant women in Ghana.
Conclusions and Recommendations
According to UNFPA (2013), family planning contributes to sustainable development and promotes gender equality by making women more autonomous in decision making. Since access to appropriate family planning is essential for the well-being of women and communities, it is important that measures be taken to enhance its accessibility by migrant women and other minority groups. Given this observation, institutions, particularly the Ministry of Health, should take measures to address challenges and ensure universal access of services by underserved populations. Reproductive health issues, particularly family planning among migrants, must not be considered as only a matter of academic interest but should have implications for national policy in general. It is imperative for the government (Ministry of Health), policy makers, and other stakeholders such as Marie Stopes International, who have an interest in reproductive health, to work toward achieving universal access to sexual reproductive services and reproductive rights.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.