
Abstract
The grieving process after perinatal loss has unique properties. This qualitative study examines one aspect of the grieving process: continuing bonds experienced by the mothers. We offer an interpretative phenomenological analysis of interviews with 15 Italian mothers. Three main relevant themes emerged: “continuing bonds between externalized and internalized presence,” “a difficult guilt to manage,” and “relationships are crucial support systems.” The first one illustrates the ongoing connections to the deceased on the part of mothers and siblings, the second one explores a fixation on finding the cause of the death and related feelings of guilt, while the third one describes the mothers’ process of elaboration of the event, especially with the support of the husband and the community. The findings highlight unique qualities of continuing bonds after perinatal loss and factors that might influence mother’s griefwork, while also suggesting that psychodrama and art therapy could be useful in the management of this kind of loss.
Keywords
Intimate and social relationships are widely considered to be an important factor in grief since they provide a fundamental source of support for the bereaved and help prevent complicated mourning (see Neimeyer, 2013). Indeed, as indicated by Maccarini (2019), the morphogenesis of any social transition implies the ability to share meanings through communication and the search for symbols.
Where this sense-making does not occur, inevitably the transformation derived from a crisis undergoes a process of disintegration instead of development (Maccarini, 2019). This holds true for families who experience the death of a family member, for example, where the inability to make sense of a painful experience makes mutual understanding and resilience difficult. This is why in such cases social workers and psychologists can collaborate to support families by preventing the social isolation of mourners (Foster & Davidson, 2003) and intervening when the bereavement is pathological (see Schut et al., 2001).
Perinatal grief, which follows losses that occur before or right after birth (Blood & Cacciatore, 2013), may have some devastating repercussions for the whole family (Martinčeková & Klatt, 2016). The grieving process can last 2 years or longer, to the point where, to resolve strong feelings of guilt, rage, and anxiety, a psychotherapeutic intervention is necessary (Doka & Martin, 2014). This happens because the nature of this often unexpected and sudden death deprives parents of the affective development of their family and parenthood identity (Moore et al., 2011). As a result, perinatal grief can have distressing physical and psychological consequences (Hughes et al., 2004).
After perinatal loss, that is, the death of a baby in the mother’s uterus or right after birth, mothers often suffer from depression and/or post-traumatic stress disorder, which are associated with a high risk of further health problems (Huberty et al., 2016). Additionally, 50%–80% of these women conceive other children after this loss (Huberty et al., 2016). These pregnancies might be affected by distress, with alternate feelings of hope and fear of a new stillbirth (specifically, the child’s death in the utero after 20 weeks of pregnancy) or of the child’s death right after birth (Hunter et al., 2017). Such feelings might influence the mother’s relationships with subsequent children (Lee et al., 2016).
Perinatal grief is profoundly related to a cultural obstacle that creates significant difficulties in the management of this distressing event. Disenfranchised grief (Doka, 2002) is a term used to describe the kinds of mourning that are culturally denied. Examples include those who suffer from the death of a pet, or a lover, or relative suffering from a sexually transmitted disease, or suicide, or murder. Such individuals are left to their grief and are stigmatized by grief that cannot be publicly expressed (Testoni & De Cataldo, 2017). In the case of perinatal death, society tends to minimize the suffering of this grief, interfering with the parents’ ability to freely express their emotions (Blood & Cacciatore, 2013; Moore et al., 2011). This is manifested through objectifying language (Scott, 2011), for example, by referring to the dead child from the mere biological point of view, not recognizing them as a person, which causes the repression of the mourners’ emotions. Consequently, mourners experience negative effects on their griefwork (Klass, 1993) and are deprived of adequate social support. Social supports are especially important for mothers to access their internal representations of the deceased (Rubin, 1985) and face the new state of things (Field, 2006). The social censorship leaves mourners in the seclusion of their inner phantoms, tormented by their sorrow and by the memory of the loss, in search of understanding and consolation. Furthermore, we should not underestimate how the typical social and cultural background of Western societies distances men from the emotional relationship with their children as well as, in some way, from the possible suffering caused by perinatal death (see Meaney et al., 2017).
In the Italian context, grief for perinatal loss is considered taboo (Bulleri & De Marco, 2013; Harris, 2010). In fact, even relatives and couples who suffer from perinatal loss tend to consider this event as a taboo. The problem is related to traditional patriarchal and sexist culture, which latently supports many prejudices toward childlessness and infertility, stigmatizing both men and women, although in different ways. Men who experience perinatal loss are stereotypically considered as impotent, whereas women suffer from a heavy sense of incompleteness because of the reproductive social mandate (Lombardi, 2015; Ottaviano, 2015; Testoni, 2012).
Social pressures and lack of training among health care professionals also negatively affect grievers (Mattalucci, 2015). According to the Law 194/1978, the voluntary interruption of pregnancy is allowed in the Italian legal system. However, the practice is widely condemned by health care professionals who often refuse to practice it in public hospitals (Lalli, 2016; Minerva, 2014). Furthermore, Italian parents cannot obtain the legal permission to bury their deceased children if the death happens before the 28th week of pregnancy since Italian law (DPR 285/1990) establishes that such fetuses can be buried only if the parents immediately request it formally to the local health care unit. Often, the health care professionals do not inform parents in time, and the failure to inform parents may have negative effects on grieving (Ravaldi & Vannacci, 2009). There is also a lack of proper training on this problem among health care operators, especially obstetricians, who expose parents to serious distress, which in turn worsens their relationship with the bereaved (Davidson, 2018a).
According to the main models of grief (see Bowlby & Parkes, 1970; Worden, 1991), the elaboration of grief is considered to be over once the object of love is internalized as a mental memory and the griever accepts the absence. Bowlby and Parkes (1970) point out the struggle implied in the process of elaboration of grief, determined by the need to face the initial reaction of denial of the loved one’s death by the bereaved and their spasmodic search for the deceased, with intense feelings of rage, guilt, and depression, until the person is able to interiorize the deceased loved one and reinvest in a new course of life. Worden (1991), on the other hand, does not consider the stages of mourning important and instead emphasizes the tasks a bereaved person must fulfill in order to properly elaborate the grief. Specifically, Worden describes the possibility that the bereaved can work on more than a process at the same time, in a fluid way of proceeding. The tasks to be accomplished by mourners are acceptance of the loss, elaboration of the sorrow, readjustment to their environment in the new condition, and the relocation of the deceased in their own cognitive and emotional universe.
However, more recent theories concerning grief tend to reject the idea of “stages” or “tasks” to overcome in order to elaborate the loss and focus more on the concept of grief as the complex process of restoring meaning to one’s life after the loss, in a way that is highly personal and unique for each individual (Neimeyer, 2001). In this perspective, what matters the most is the ability to modify the relationship with the deceased in order to adapt it to the new context of loss, while completely severing the bond with them is not necessary.
Both the classic models and the more recent ones however assume that, for a proper mourning process to take place, the bereaved person must acknowledge the loss and the fact that the loved one will not return in the present life as a physical person, although they can still be part of the bereaved existence in a symbolic and integrated way, through memories, thoughts, and spirituality. However, when the perceived presence of the departed persists, with no distinction between the world of the living and the world of the dead, grief remains unresolved (Field, 2006).
Continuing bonds (CBs) is a concept referring to ongoing relationships or attachments that a bereaved individual experiences to the deceased (Klass & Walter, 2001). Despite CBs increasingly being viewed as a normal early phase of the grieving process, some researchers suggest that CBs are not universally adaptive (Field, 2006). Even though in some instances CBs are comforting to the bereaved, in others they can create distortions in relationships. This failure in the process of separation expresses itself in maladaptive CBs (Klass, 2006). Maladaptive CBs might include, for example, the sensation of perceiving the physical presence of the departed (Keen et al., 2013).
However, as previously mentioned, other studies concerning CBs point out how these manifestations could also simply be part of a healthy grieving process, in which maintaining an intense symbolic bond with the deceased can help the bereaved adapt to the loss (Neimeyer, 2001). Indeed, recent studies concerning CBs suggest that their role cannot be defined beforehand and that their either positive or negative influence over the bereaved might be mediated by the person’s capability to make sense of the loss and integrate it in their everyday life, with strong CBs linked to complicated grief only when the person is unable to restore meaning (Neimeyer et al., 2006).
Therefore, it appears evident how literature on CBs highlights the extreme complexity of the phenomenon and presents two opposite interpretations: the first considers them a symptom of unresolved mourning and the second, a method that can help to manage loss and resolve mourning (Hall, 2014). However, no solid conclusions can be made because of conflicting empirical findings (Field, 2006). It is likely that both are correct since during the early phases of grief, the search for physical proximity might be considered natural because of the conflict between remembering and forsaking the departed (Fuchs, 2018). In such cases, CBs can serve as a “transitional element” in the grieving process (Klass, 1993). At the same time, a positive grieving process will move toward a reorganization rather than the abandonment of the bond, through the internalization of the deceased as an extension of the self, maintaining a psychological rather than physical proximity (see Field, 2006; Testoni, 2016).
In this research, we examine the repercussions of CBs for mothers who experience perinatal grief. Few studies have focused on CBs after perinatal grief (Fenstermacher & Hupcey, 2013). In this research, we consider whether CBs help mothers after perinatal grief or not, and how. Indeed, this kind of mourning is quite different because the separation required is from an “internal” relationship with the fetus that has not entirely evolved. As such, these CBs may result in a difficulty which is expressed through specific psychological symptoms rather than constituting a useful strategy to cope with loss. This is very important since ignoring this issue can undermine our understanding of mourners’ suffering and proper intervention (Huberty et al., 2016). In this study, we use qualitative methods to examine the relationship between CBs and perinatal grief for Italian mothers who have suffered from this kind of loss. The final aim of our study is to identify social strategies that psychologists and social workers can use to support this specific form of mourning.
Participants
The study involved 15 Italian women, living in the northeast of the country. Participants experienced perinatal loss between the fifth and the ninth month of pregnancy, during a period of time between 1992 and 2018 (mean time since loss: 6.45 years; standard deviation: 7.29). Our choice to apply the precise inclusion criteria of the time of the loss not before the fifth month of pregnancy was so that our interviewees would all have experienced fetal movements (which start to occur during the fifth month of pregnancy). Such a specific choice was sustained by the objective to properly explore the mothers’ mental representation of their children, and therefore, fetal movements were considered very important in mothers’ perceptions of the presence of another separate person in their wombs.
Our participants’ age at the time of the loss was between 22 and 40 years old (mean age at loss: 31.6 years; standard deviation: 5.52). Nine women experienced loss during their first pregnancy, six already had one or more children, and eight had one or more children after the experience. Five of the women were Catholic, one had lost her faith following the perinatal loss, one was an atheist, and the others reported having an inner spirituality not linked to religion. At the time of the loss, all of our interviewees had a partner/husband; at the time of the interview, two had divorced.
We recruited participants from several sources. Four were contacted through a hospital in North Italy by the psychotherapist who supported them after their loss, three were referred by other participants, and seven were recruited through an internet support group, which is active through a blog and a Facebook page. Every participant was initially contacted by a psychotherapist at the hospital or the internet group they were part of. A follow-up email or cell phone message was sent to those who indicated their interest in the project. After their acceptance, all the research details were explained through a phone call, and an appointment was fixed in order to proceed with the interview.
Mourners were interviewed in a space of their choosing depending on what was more comfortable for them: Eight participants were interviewed through a Skype communication while they were at home because of the excessive distance and their impossibility to meet the researchers in person. As regard the remaining seven, six of them were interviewed at their home, while one met the researchers at the main researcher’s house.
Method
Each interview lasted approximately 90 min. We designed the interviews using a narrative perspective, where participants’ direct report of their experience was the starting point for our analysis of their perinatal loss. Our analysis used a qualitative–phenomenological approach, considered in the literature to be the most reliable method for investigating people’s biographies and their interpretation of life experiences (Testoni et al., 2017). Our study used interpretative phenomenological analysis (IPA), which has been utilized successfully with mourners (Testoni et al., 2019) and has been shown to be efficacious in the recognition of specific difficulties that require further research and intervention (Gill, 2014). IPA integrates the emic view of the participants with the interpretative etic view of the researchers (Testoni et al., 2019). IPA’s reference paradigm is the phenomenological one (Brocki & Wearden, 2006; Larkin et al., 2006; Smith & Osborn, 2008), with references to the hermeneutic and idiographic theory (Pietkiewicz & Smith, 2014). In order to get as close as possible to the participants’ perspective, the IPA follows two processes: People are asked to make sense of their experiences through a detailed narration guided by the researcher; the researcher then tries to make sense of the sense itself that emerges from the participants’ narrations (Smith & Osborn, 2008). Through this method, the researchers get as close as they can to the point of view of the person who experiences a certain phenomenon. The subsequent description is thus not anticipated by predetermined categories (Larkin et al., 2006). Rather, every discovery is a function of the relationship between interviewers and participants.
In order to be faithful to the phenomenon, the researchers’ attitude must be open without adopting predetermined assumptions or concepts. Indeed, this method can generate reflections to a much greater extent than the classic questionnaire technique (Testoni et al., 2018). Following the COnsolidated criteria for REporting Qualitative-research (CORE-Q) checklist (Tong et al., 2007), our analysis focused on the relationships between the representation of death and loss integrated with the exploration of participants’ experiences with others (partner, family, health care professionals and social network), and the presence of CBs (Zamperini et al., 2015).
The main research question that guided our study was: “What kind of relationship is there between the phenomenon of CBs and the support the bereaved mother feels she received, at different levels and contexts, both at the moment of the loss and afterwards?” In order to identify the phenomenon of CBs, the image that the mother had of her child was explored during the interview, together with her fantasies concerning where the child might be now (a more intimate and spiritual dimension or, on the contrary, a concrete and physical one), as well as the kind of connection she felt with her lost child. Similarly, in order to explore the type of social support that participants received, they were asked to describe their experiences, the problems they had with others, and how their grief changed over time. We used a semistructured format to ensure a smooth and logical flow of conversation, deriving transition questions from our interviewees’ narration of their experiences. All the interviews were conducted in Italian, the participants’ native language, and they were audio-recorded and transcribed verbatim, still in Italian, for analysis. The written texts obtained from the interviews were translated in English after the data analysis, during the elaboration of the first draft of the present article by the authors who were very careful to maintain the linguistic style and precise terms the participants had used in the original language (Italian).
The interviews were conducted by the first author, with two additional researchers involved at the data analysis stage. Using an IPA analysis allowed the researcher to identify relevant thematic categories (Larkin et al., 2006; Testoni et al., 2018). The first round of analysis was conducted by the lead researcher who had interviewed the mothers, followed by subsequent rounds of analysis with the other two researchers. This process allowed a deeper understanding of the participants’ points of view to emerge. The researchers used Atlas.ti, a program that is particularly suited for qualitative analysis.
The study followed the APA Ethical Principles of Psychologists, the Code of Conduct, and the principles of the Declaration of Helsinki. Furthermore, it was approved by the ethics committee of the University of Padova. Participants were informed about the study’s aims and procedures and were assured that participation was voluntary. The confidentiality of their responses was guaranteed by the fact that the researchers stored all the information and data inside encrypted files accessible only to them. Informed consent was obtained from all participants. All participants’ names were changed in this article to protect their identity.
Results
From the data analysis, three main areas of thematic prevalence emerged: “continuing bonds between externalized and internalized presence,” “a difficult guilt to manage,” and “relationships are crucial support systems.”
CBs Between Externalized and Internalized Presence
The theme of CBs was cited in all the narratives, although there were important differences across the sample. Nine participants described beliefs, at least to some extent, about the possibility of the deceased existing externally as an omniscient presence above them. To these mothers, the child was concretely part of the family, appearing in different forms. Five mothers were convinced that the deceased was present in the representations or in the games of the living siblings. The mothers believed that the deceased manifested presence in different ways through symbolic elements such as in the form of small objects like butterflies or hearts. This is what happened to Barbara, a married, unemployed woman who lost her daughter in 2016 during her seventh month of pregnancy. She described how she saw her deceased daughter, even after insisting no photograph be taken. After 2½ years, she had still maintained an external relationship with the child who was buried in a grave where Barbara often went. As Barbara explained: I know she is here, I feel her in the little things. Even a silly thing, for example a little heart that is formed in the foam. I believe it is her, here. Sometimes I see a butterfly that lands near me, and I believe it is her. Anyway, she is always with us, she is a constant presence in our family. We visit her very often, so we constantly feel her presence. We mention her a lot and we know she is only a little further, somewhere else. She is not physically here, but she is with us anyway, in everything we do. It’s beautiful because my son always says: “Mum, I need to go home because I have to play with Judy and Ethan.” Ethan is the dead brother. I think it is their own way of coping with this […], their way to say: “You are with us, you are here just like we want,” their way not to believe he is dead. This is beautiful because they don’t forget him. I will never have him here with me, but I know he is here with me every day in a different way: he is a constant presence for me and for his brother who was born sometime after him. We feel that he is with both of us every day. The first months after the loss my son saw her before going to bed, in the dark…he said he saw his sister. This happened lots of times. At first all this seemed strange to me, then it became almost normal and still, sometimes, when it happens, I’m not surprised. All this helps me and my son cope with this painful loss.
Six mothers described the external presence of the deceased not as constant or pervasive but as somehow exceptional. One such mother was Silvia, a divorced and retired woman who lost her second child at the age of 39, during her fifth month of pregnancy. Silvia believed that her deceased child lived in another dimension, a sort of heaven “among the noblest souls, especially because he was so little, where else should he be otherwise? I think we are still in contact, through these two dimensions which somehow are intertwined.”
These experiences describe external CBs, while other narrations showed a particular form of internalization, not exactly comparable to the recognition of a mentalized memory. Such an experience was narrated by Laura, a married woman who lost her first child during her ninth month of pregnancy, when she was 22 years old. Laura took a photo of her deceased daughter and buried her in a grave. When she was asked whether there still was an internal dialogue between her and her child, she concisely explained, “I do not speak to her, but she knows everything and is always with me. There is no need to say anything and I do not have anything to say to her actually, you know? We are still together.”
Other participants described the sensation of the presence of the children inside them, as if they had never been born. An example of this was Giovanna, a divorced woman who lost her child when she was 33 years old, at the fifth month of pregnancy. Isolated from her family, she bore her loss alone. While talking about where she imagined her child, she said, “If he is somewhere, he is inside me, I don’t know how to say it, he is not somewhere outside. Somehow he wasn’t completely born.”
A Difficult Guilt to Manage
Another meaningful theme that emerged was the guilt the mothers experienced toward their lost child. Feelings of guilt appeared to have many implications for the theme of CB. Indeed, guilt spontaneously emerged in all the narratives as a painful thought that was mentioned even by those who did not actually feel guilty. Feelings of guilt were depicted as expressions of repentance and contrition for not having done something important. Melissa, who lost the fetus before arriving at the hospital, described this feeling as follows: I touched her, I kissed her, but I didn’t hold her…I just didn’t feel like doing it. And this is one of the reasons why I repent, because I didn’t think about it! Because I didn’t hold her! And I kept asking myself: “Why didn’t I hold her?” She was my daughter, so why didn’t I hold her?
In some cases, guilt was worsened by friends’ accusations and social stigma. As Barbara perfectly described: I was unlucky enough to see some friends of mine with whom I was sharing the experience of pregnancy who completely left when I lost my child; they didn’t want me there when they gave birth, they didn’t call me, because they thought I brought bad luck. Such a silly thing, yes…well, fine! You need to get used to it, you become a label. After the stillbirth, I was the dead child’s mother…you have to know that people label this fact. […] You are not able to do your natural duty. A ritual, if we may call it this. But I think it is more linked to the fact that I lost the sense of reality because I talk to my baby…yes…the majority of time I ask him for forgiveness.
Chiara’s story was similar. A married and retired woman who lost her second child just few days before the birth when she was 28 years old, she did not see the child because it was not recommended by the obstetricians. However, the baby was buried, and there is a grave where Chiara sometimes prays. She reported the fact that she was still suffering from perinatal loss because “it is much too difficult to process this experience.” The main emotions she felt were guilt and shame: I lived this grief in silence, no one helped me, even in my family no one talked about it. These events are underestimated and for us mothers it is almost considered a shame. You are abnormal, you’ve done something wrong and you don’t know what it is. I felt a lot of rage before my daughter’s autopsy, but now I am serene, because I think: “It’s not our fault, we did everything we had to” and: “Fine, next time it’ll be better.” I think that I am not responsible for what happened. I am not responsible for all this. All I can do is try to have some children, and I’ve been lucky after all, because I managed to have all the children I desired. Their fate didn’t depend on me […]. I contemplate my whole life path, and everything is balanced, I accept it like this…It’s fine….
Relationships Are Crucial Support Systems
A third aspect that emerged from the narratives concerned the role of postmortem photography. In general, neither the pictures nor the funeral appeared to have a crucial influence on the participants’ CBs since they could emerge both when the mother had taken pictures and had had a funeral and when she had not.
Gloria, a married, employed woman who lost her first daughter during her ninth month of pregnancy when she was 28 years old saw her daughter and held her in her arms. She said, My partner had taken some pictures, he gave them to me as a present for our first Christmas without her and I have them hanging in our room, so she is there, I always see her. She is always in front of me and I cannot avoid seeing them and feeling her presence. For my husband it is more difficult to talk about this, but we manage to talk. We wanted to process this together. Perhaps I talk more about it, sometimes I bring it up[…]. It has never been our main topic of conversation, but for me it was important, especially after the stillbirth, I needed “to let it out” and, unfortunately for him, I did it with him. No one is responsible, it simply happened…so now we go on because no one is bringing her back anyway. Fixating on it is not worth it, so you must go on, you don’t forget but you must go on. I am not always at the cemetery. We had the funeral, we cremated her, and gave her a proper burial. We visit her every 15–20 days, just for 5 minutes […] it is not something too burdensome. We took what happened and we considered it a bump in the road; the more children we try to have, the more likely it is for us to get caught up in these tragedies, it is part of life[…]. So, we had enough strength to say: Let’s not let this get us down, let’s go on, but with hope, because we want to live in hope, not in sorrow.
When this social support was absent, however, the suffering became unbearable. As Giada described: I tried more than once, even if not immediately after the loss, to talk to my husband. I told him that I needed to escape for a while[…]. And I told him that I needed a distraction, I needed to express my pain…this pain that, in fact, I cannot express. The pain is yours, right? It stays inside you and you cannot express it. The healthcare professionals were very attentive too, because they let my partner stay there with me. They gave me a room with two beds, and they told me I could have him there, so he was always with me during labour[…] we faced this together and this brought us closer, and we are getting married next year. I also have other people who support me anyway: my mum, my dad, and my sister; I think I couldn’t possibly have better support. And I also have my friends. Regarding the hospital, they were exceptional, they managed it wonderfully. Especially the young ones. I believe they really knew how to deal with the situation. The oldest ones were a little less prepared to manage it[…] while on the contrary the younger [ones] were more attentive, and maybe they were even more prepared on the subject. I got along really well with my obstetrician who was my age and was absolutely adorable. The psychotherapist was a lifesaver for me. She helped me a lot at the moment of the loss and I am very grateful because it is very difficult to talk about it in those moments. There are so many things at stake…it is overwhelming. I spoke with the psychotherapist twice. The first one alone, the second with my partner, and he too said that she was a very competent professional and that it was useful for him too. He didn’t want to come at first, but in the end he did, and he later told me that it had been important for him.
Figure 1 summarizes the three areas of thematic prevalence that emerged from the data analysis, displaying the main connections and subthemes related to them. It focuses in particular on the third one: “relationships are crucial support systems.” The figure exhibits the positive effects that a valid social network had on the participants’ recovery and well-being. It also highlights the negative consequences that lack of social support, together with an unresolved sense of guilt, can have on bereaved mothers in terms of prolonged grief and CBs.
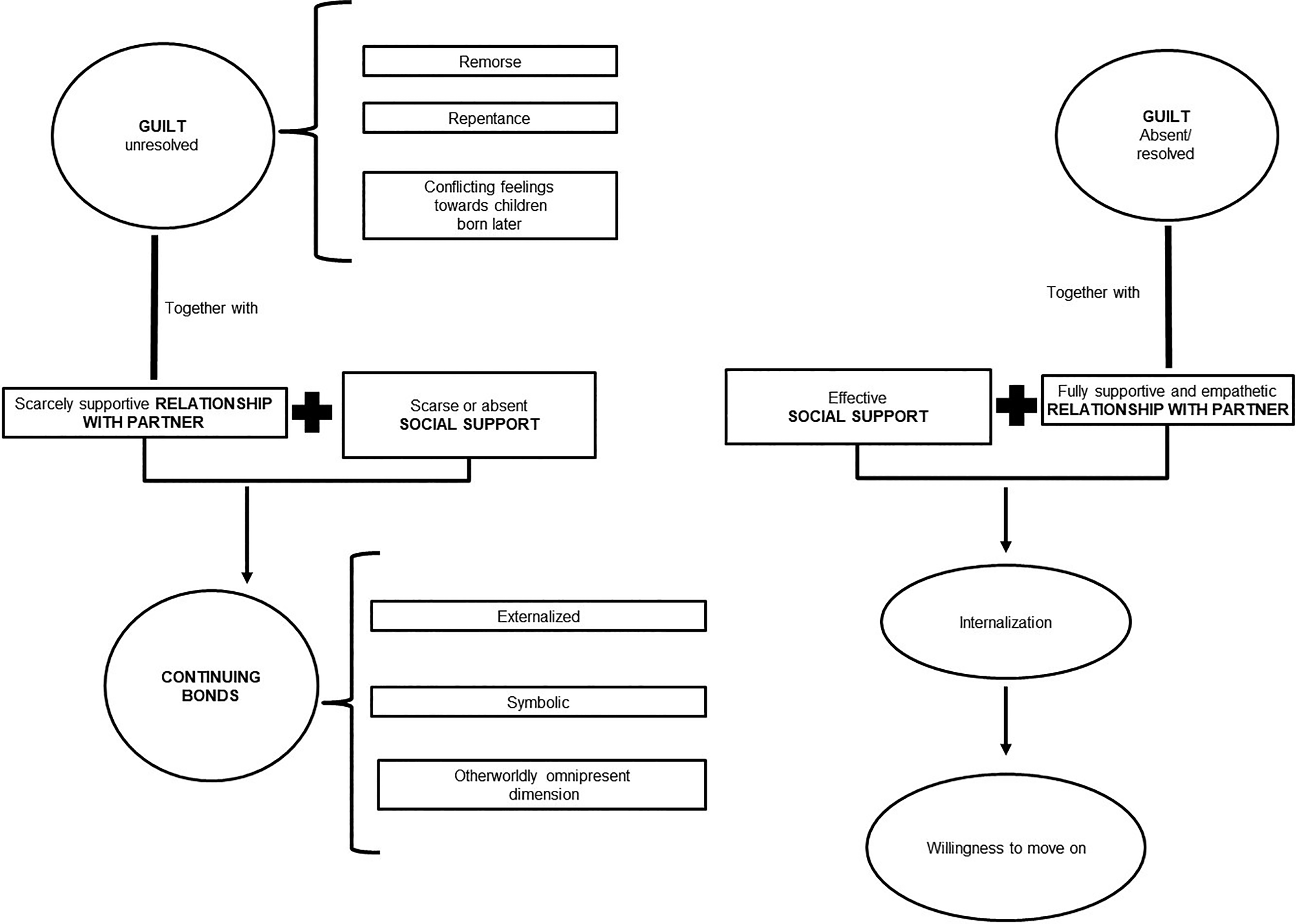
The role of close relationships and social support.
Discussion
This study examined the role of CBs in perinatal grief. Our analysis of the narratives of 15 Italian mothers identified three key themes: the significance of CBs, feelings of guilt, and the crucial role of intimate and social relationships for support.
Regarding the first area of thematic prevalence, literature on CBs after perinatal loss is quite scarce. In our study, we found that the forms in which the mothers imagined their children were different and, because of this, the bonds they maintained or did not maintain with them varied. For mothers who experienced externalized forms of CBs, the child’s presence was perceived physically through symbolic objects like little animals or hearts. This contrasted CBs where the deceased child’s presence was placed in an otherworldly, ubiquitous dimension as an all-pervading entity.
The literature indicates that the lack of conceptualization—associated with the absence of a body to mourn (Cacciatore et al., 2008)—makes it more difficult to organize a mental representation not only of the loss but also of the child’s identity for both parents (Golan & Leichtentritt, 2016). CBs can be the result. That is why perinatal grief photography has become an accepted practice and considerable literature recommends it as a standard of care, explaining how to take respectful and compassionate photographs of deceased infants (Alexander, 2001). As there are limited studies which support the effectiveness of this intervention and our research was not aimed to check its efficacy that remains beyond the scope of this research. However, the results suggested that photography was used to memorialize and maintain constantly present the dead children, transforming them into a constant presence for the couple (as happened with Gloria). Importantly, CBs were maintained by both those who took photographs of the deceased and those who did not. As such, this practice does not seem to play a crucial role in relation to the possible mourning outcomes.
On the other hand, the results indicated that with this kind of grief, the internalization of the deceased child does not guarantee the resolution of the bereavement and could be a problem (as for Laura, who took some photos, and Giovanna, who had to manage her grief alone). This stands in contrast with what both researchers who emphasize the positive role of CBs regarding the successful adaptation to bereavement say, and what researchers who highlight their negative role stress. In other words, when the connection becomes internal and does not involve the physical existence of the other, grief may be considered resolved.
This potentially contrasts other forms of mourning, where internalization implies a change of attachment to the deceased in order to reflect the physical separation (Bowlby & Parkes, 1970; Worden, 1991). In perinatal grief, it could be linked to the incompleteness of the pregnancy, as if in these cases the child had never left his or her place inside the mother.
Only in Carol’s case did the internalization results in a positive resolution of grief. However, this was due to a crucial aspect: the positive relationship with her husband and the elaboration of grief with him. The husband’s support, and the opportunity to talk about what happened without making it a taboo (as also seen in the narrations of Carol and Mary), turned out to be very important, allowing the mothers to overcome the sorrow and internalize the representation of their lost child in an efficacious way, moving toward the resolution of grief. The same also happened when the mothers were helped by a solid, understanding, and empathetic social network. Specifically, their feelings of guilt appeared to be better resolved and, at the same time, the child was not perceived as a constant and permanent presence. In fact, Paola, Carol, and Mary, whose guilt was resolved by the support they received, showed no forms of CBs with their lost children.
The decisive importance of a proper social and intimate support for the bereaved mothers after a perinatal loss has been confirmed by other studies (Davidson, 2018a; Neimeyer, 2013). Indeed, when the relationship with the husband or with the social network was not very supportive, the sorrow of the loss became unbearable, as has already been emphasized by other surveys (Blood & Cacciatore, 2014; Mattalucci, 2015). In these situations, CBs, both externalized and internalized, appeared to be quite unhealthy, because the dead children became omnipresent entities in the family environment, even involving the siblings, as with Valentina, Giada, and Melissa, who evidently profoundly influenced their living children with their CBs. These mothers reported how their deceased child was present also in their living children’s everyday life, and this was expressed in particular through their children’s drawings and games. The possible presence of CBs manifested by children who lost a sibling in a perinatal death has already been documented (Youngblut & Brooten, 2013), in particular the presence of externalized forms of CBs (through small objects, photographs, drawings). These four participants’ children appeared indeed to maintain strong CBs with their deceased brother or sister, a behavior that was exactly specular to the one narrated by their mothers, as they described in the interviews. Since the parents can indeed remain significantly connected to their lost child and openly manifest this to their other children, they can also shape the kind of bond their living children create and maintain with the deceased one.
In the participants’ narrations, the children’s CBs were described as positive, a way they had to feel closer to their lost brother or sister and to elaborate the loss. However, some researches in literature describe the risks that can arise from a strongly perceived presence of the deceased brother or sister since the living siblings could tend to compare themselves to the deceased one, experiencing feelings of inadequacy and distress (Sabbadini, 2008). Siblings’ grief is not generally considered, especially concerning perinatal loss (Davidson, 2018b). However, our findings suggest that this is an issue that should be considered carefully, especially by psychologists and social workers who offer support to the bereaved family.
In certain cases, the loneliness that was experienced by the participants culminated in real isolation. Isolation was accentuated by a lack of understanding from relatives and friends, in a way delegitimizing the mothers’ pain, as has already been described in other studies conducted in the Italian context (Bulleri & De Marco, 2013; Mattalucci, 2015).
Social stigma worsened the effects, so that the mother felt she was labeled as “the mother who lost the child” or “the one who brings bad luck,” making it even more difficult to cope with the loss. The intense impact of stigmatization toward women who cannot become mothers has been confirmed by other studies as well (Lombardi, 2015; Ottaviano, 2015).
Given our findings, we believe that an adequate intervention by social workers who operate in hospitals is important, especially in death and dying situations, as has already been evidenced (see Moon et al., 2019). In particular, however, we believe that not only can they make local services available to mourners to ensure appropriate psychosocial support, but they could also use techniques to support mothers to better manage their grief, possibly in group initiatives.
Conclusion
The study considered the relationship between perinatal bereavement and CBs, highlighting the crucial role played by both the mourner’s husbands/partners and by their social network in helping the mothers to begin a healthy mourning process. Supports made a significant difference since the participants who could not count on such a support faced isolation, stigmatization, extreme sorrow, and ultimately unresolved grief, with the strong presence of CBs.
Since some of the participants expressed the importance of receiving psychological support in the hospital, it is important to underline how this kind of intervention should be made available to all mothers, informing them that they could use this service in case of need. Psychodrama and art therapy could also be useful strategies to support mothers to better represent their lost children and meet them in the surplus reality (Orkibi et al., 2014; Orkibi et al., 2017a, 2017b; Testoni et al., 2019). These form of interventions appears to be very promising since they offer the opportunity to manage unresolved issues concerning one’s relationship with a deceased loved one, to decrease symptoms of depression and loneliness, and to help address perceived stigmas (Orkibi & Feniger-Schaal, 2019). Literature in this field shows the positive effect of artistic expressions in all the phases of mourning and how these activities may be managed by both psychologists and social workers (Kaplan, 2007; Tompson & Neimeyer, 2014; Wood et al., 2019).
Limits of the Study and Future Developments
The research has some limitations, in particular concerning the way the mothers have been contacted, since four of them were recruited by the psychotherapist who supported them after their loss, and this might have affected the mothers’ answers concerning the type of support they received. Another limitation is the fact that a different amount of time had passed since the loss for every participant, and this could have influenced their grieving process and the different kinds of support they received. Moreover, some interviews were conducted face-to-face, while others (because of the distance) were conducted via video call, therefore providing different degrees of intimacy between the interviewer and the participants and, in the second case, hindering the ability to grasp nonverbal cues from the mothers.
Considering the mothers’ need to express their grief and receive strong support, together with the necessity to mentally and psychologically reorganize the way they represent their deceased child, further research should focus on what kind of professional interventions could be particularly helpful for sustaining their mourning process, especially by social workers who are able to improve the social support. Finally, future research should investigate siblings’ and fathers’ reactions to perinatal loss since this kind of grief is still scarcely recognized by society, in order to develop a more adequate support system for them too.
Footnotes
Acknowledgments
We would like to thank Novella C. Buiani, perinatal psychologist who works in Udine (Italy) and Erika Zerbini, writer and facilitator for self-mutual help groups which operates in Genoa (Italy)—founders of the website luttoperinatale.life—who both try really hard to spread information and knowledge concerning perinatal grief and to map the Italian organizations that support grieving parents. We would also like to thank Doctor Rossella Ponchia, psychotherapist who works at the Obstetrics and Gynecology Service of the University Hospital of Padova (Italy).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.