
Abstract
Little is known about the lives and hardships of socially marginalized and economically destitute women in rural Central China living with human immunodeficiency virus (HIV), who acquired the virus through commercial blood and plasma donations in the mid-1990s. Women living with HIV and acquired immune deficiency syndrome (AIDS) experience significant economic hardships and social exclusion in a male dominated, traditional, rural Chinese society, including the loss of labor power, financial burdens, and HIV-related stigma. This qualitative study examined strategies used by these marginalized women to cope with these hardships. Thematic analysis was used to analyze data from 15 interviews from women in Fuyang City, Anhui. Findings reveal that women undertook a variety of coping strategies: migrating to smaller towns, reducing labor intensity, reallocating labor within households, supplementing incomes by taking on additional jobs, borrowing money from relatives, reducing food consumption, lowering standards of living, withdrawing children from school, strategically disclosing HIV status and background information to employers, as well as avoiding weddings or funerals. This study identifies policy implications that can be used by social workers to mitigate the deleterious social and economic impacts of HIV and AIDS on the lives of women in vulnerable rural households in central China.
Keywords
Human Immunodeficiency Virus (HIV) Among Former Commercial Plasma Donors in China
The HIV epidemic among former commercial plasma donors and their families began in China in the early 1990s, when China’s integration into the world economy brought with it a large external demand for domestic plasma products, which were used by transnational pharmaceutical companies to produce other blood products such as albumin, intravenous immunoglobulin, and anti-inhibitors (Chen, 2014). In China, the transnational pharmaceutical companies and transnational blood and plasma trade fuelled the transmission of HIV. The market for blood plasma prevailed in rural areas in China where poor farmworkers were offered cash compensations for blood plasma donations (Chen, 2014; Volkow & del Rio, 2005). The transnational pharmaceutical companies and public health officials in central rural China offered poor farmworkers lucrative deals to donate their blood and plasma (Gittings, 2001; He & Detels, 2005; Kaufman & Jing, 2002; Volkow & Del Rio, 2005). Given the extreme economic hardships that poor communities were facing in China, farmworkers saw this as an opportunity to supplement their incomes (Gittings, 2001; Kaufman & Jing, 2002).
As some of the paid blood donation stations were operated by local/provincial health officials (Kaufman & Jing, 2002), besides significant income increase for poor individuals in rural areas and booming profit for pharmaceutical companies, the plasma economy became a lucrative source of income for government officials (Kaufman & Jing, 2002). Due to unsafe collection and reinfusion processes, the donors’ blood and plasma products came in contact with blood-borne viruses such as HIV (Gittings, 2001; Kaufman & Jing, 2002; Sullivan et al., 2010; Wu, Rou, & Detels, 2001). Poor farmworkers were unaware of this, and by continuing to sell their blood and plasma products, many rural residents acquired HIV (Chen, 2014; Kaufman & Jing, 2002; Volkow & Del Rio, 2005).
Multiple advocates have campaigned to try to force the government to care for sick villagers who had become infected while donating blood plasma for cash during the 1990s (Kaufman & Jing, 2002). Many publications (both in China and abroad) at that time published front-page stories about the widespread epidemic in rural Central China, detailing the human tragedies of dying parents, poverty-stricken and stigmatized families and children, the increasing number of AIDS orphans, and the provincial government’s cover-up of the epidemic and refusal of care or assistance to the victims (Kaufman & Jing, 2002). Unfortunately, while this public health tragedy among poor rural farmworkers and their families came to the world’s attention in late 1990s (Kaufman & Jing, 2002), the Chinese government only acknowledged this issue in 2004 because by then the HIV epidemic among this Chinese population became so significant that it demanded radical public health policy rethinking (Copeman, 2009). In 2004, China also launched programs for rural and poor urban residents, providing free treatment, free drugs to HIV-infected pregnant women, free voluntary HIV screening tests, and free education for orphans of people living with HIV/AIDS (Zhang, Pierre, & Zhang, 2011).
Economic and Social Exclusion Experienced by Women Who Acquired HIV Through Paid Blood and Plasma Collections
Previous research (Zhang & Souleymanov, 2017) revealed that the well-being of people living with HIV and AIDS who acquired virus through paid blood and plasma collections was immensely affected by loss of income, and other financial difficulties, as well as social exclusion due to HIV/AIDS-related stigma, which remained a significant issue in a workplace, funerals, and weddings. Importantly, women living with HIV experienced an additional layer of economic and social injustices and hardships in male-dominated rural Chinese communities, particularly in areas of employment and participation in social events (Zhang & Souleymanov, 2017). These findings necessitate a unique investigation in the experiences of women, in particular women’s coping strategies to mitigate these hardships.
Indeed, stigmatizing attitudes and behaviors toward people living with HIV remains a problem in China (Sullivan et al., 2010), and people living with HIV typically face social exclusion and discrimination within health-care and employment settings, as well as from their families (Cao, Sullivan, Xu, Wu, & China CIPRA Project 2 Team, 2006). However, existing studies on former commercial plasma donors in China (Chen, 2014; Dou et al., 2010; Ji, Detels, Wu, & Yin, 2006; Qian et al., 2006; Wu et al., 2001; Xu et al., 2006) often render the experiences of women invisible. For example, existing quantitative studies on former commercial plasma donors in China investigate various aspects associated with this type of HIV transmission: factors associated with mortality and survival of donors (Dou et al., 2010), prevalence of HIV infection among former donors (Wu et al., 2001), coinfection of HIV and hepatitis C among these donors (Chen, 2014; Qian et al., 2006), ways HIV can spread from former donors to nondonors (Ji et al., 2006), and HIV antiretroviral therapy use practices among donors (Xu et al., 2006).
What can be observed from existing literature is that: (1) Most studies of HIV-infected former blood and plasma donors that have been published investigated primarily the clinical and epidemiological aspects of donors’ lives, (2) No study has previously focused exclusively on HIV-infected women who were former blood and plasma donors, and (3) The existing research continues to address the lived experiences of former blood and plasma donors from a deficit paradigm (that focuses only on problems) and overlooks opportunities for understanding the role of coping in the lives of this marginalized and stigmatized population.
Instead, a research focus on coping strategies views former blood and plasma donors as people with the freedom to affect their own fates (having subjective agency and resilience) and more specifically positions the subjectivities of women living with HIV as people who are working hard to cope with structural oppression or adapt to changing circumstances of their lives. This study aims to complement these existing research gaps (a focus on women’s lived realities and coping strategies).
Scholarship documented that women living with HIV employ coping strategies to address stigma in their lives (Logie, James, Tharao, & Loutfy, 2013; Shannon et al., 2008). Some scholars also suggested that women living with HIV in China are in greater need of social support and coping strategies (Li, Lin, Liang, & Ji, 2016) and that coping strategies to address stressors that arise from HIV might be different in China than other countries, all of which warrants a unique investigation (Zhang et al., 2014). Currently, there are no qualitative investigations of the coping strategies of socially marginalized and economically destitute women who live in rural areas of Central China and who acquired HIV through former commercial blood and plasma donations in the mid-1990s. Typically, these studies are rare because it is difficult to collect data from stigmatized populations of plasma donors (Chen, 2014).
Gender Beliefs in China and Structural Violence Against Women
The issues affecting women living with HIV and AIDS also have to be conceptualized within the context of gender beliefs in China. Research suggests that in rural areas of China, women may be particularly vulnerable to being ostracized because of the traditional gender beliefs and attitudes that judge them as inferior to men (Thornton & Lin, 1994; Yang, 1996). Importantly, one distinct feature of the traditional Chinese family is the paramount importance of family lineage (Chu & Yu, 2010). The traditional Chinese family has long been characterized as patriarchal, patrimonial, and patrilineal, putting women at a severe social disadvantage relative to men (Thornton & Lin, 1994). Some scholars for instance suggest that families tend to sacrifice older daughters’ educations to benefit the educational outcomes of younger sons (Chu, Xie, & Yu, 2007). In rural China, research highlights that married sons are given more opportunities provide larger amounts of financial support than married daughters to elderly parents in rural China (Yang, 1996).
However, there are also good indications that a substantial fraction of Chinese population (however primarily people with higher income and with higher level of education) no longer subscribes to the traditional Chinese value of maintaining family lineage (Wu & Xie, 2013). Nevertheless, women remain disadvantaged relative to men in terms of labor income in China, as the gender gap in earnings has increased over time (Hauser & Xie, 2005). Research conducted in China estimates women’s earnings to be 70% of those of men (Li & Xie, 2013). Scholars also report large gender gaps in household work in contemporary China, with the lion’s share falling on the shoulders of the wife rather than the husband, with women being responsible both for caring for children and the household (Yu & Xie, 2011). Thus, in addition to already being disadvantaged in terms of labor income, the traditional division of labor in the Chinese household may impede the realization of women’s full potential in the labor market.
Due to an inability to conceptualize such structural violence as a determinant of HIV transmission among women, HIV interventions are failing marginalized communities of women (Lane et al., 2004). The concept of structural violence (Farmer, 2004; Farmer, Nizeye, Stulac, & Keshavjee, 2006) may help render the experiences of female participants who acquired HIV through plasma donations more visible. Structural violence describes social, economic, political, legal, religious, and cultural structures that stop individuals, groups, or societies from reaching their full potential (Galtung, 1969) and highlights the differential access to economic resources, political power, education, health care, or even legal standing (Farmer, 2004).
Utilizing feminist theory (Enloe, 1993), this study conceptualized the experiences of women within the domain of patriarchy-based structural violence (Brock-Utne, 1989; Ebert, 1996), as a way of describing social arrangements, injustice, and oppression that put poor and socially marginalized women living with HIV in harm’s way. Thus, when examined from a patriarchy-based structural violence perspective, it is clear that women who acquired HIV from former commercial plasma donations were already encountering multiple forms of economic and social exclusion. The mere fact that women acquired HIV in the first place through commercial blood and plasma donations because poverty and social exclusion were the primary and determining condition of their lives highlights the effects of this structural violence. Understanding these findings through the lens of patriarchy-based structural violence can also help to position the socioeconomic struggles of women in China who acquired HIV from former commercial plasma donorships within global socioeconomic and political contexts.
Social workers are ideally suited to recognize the psychosocial complexities that HIV entails for women (Parrish, Burry, & Pabst, 2003). Social workers have to be prepared to address the social and economic problems associated with HIV/AIDS in rural regions of China, such as poverty, lack of employment, social exclusion, and stigma. Conceptualizing women’s narratives in this study as patriarchal structural violence against them provides social workers with nuanced tools to conduct a fine-tuned, systemic analysis of power and privilege in interpreting how women living with HIV experience socioeconomic hardships and suffering. Utilizing the structural violence framework, this qualitative study examines the coping strategies of socially marginalized and economically destitute women who live in rural areas of Central China and who acquired HIV through former commercial blood and plasma donations in the mid-1990s.
Method
Study Sites and Population
This study was conducted in the Jingjiu Technological Development Zone in Fuyang City, Anhui province. Individuals who received community health services targeted for HIV/AIDS were provided with information about the study by the staff at local community health service station. The interviews were collected as part of the larger study, which aimed to examine the economic and social impacts of HIV and AIDS on rural Chinese households and examine the coping strategies employed by people in these households to deal with these impacts. In total 30 respondents (15 men and 15 women) took part in this study. This particular analysis focused exclusively on the lived experiences of 15 HIV-positive women who were former commercial plasma donors.
Procedure
All interviews were conducted at the health station between December 2013 and January 2014. All study participants living with HIV who were receiving community health services for various health issues associated with HIV and AIDS were provided with the study information by the health station’s staff. Those participants who expressed interest and wished to participate in this study were then invited to take part in the study by contacting research staff in a private room at the health station. Participants were provided with the basic information about the potential interview. Oral consent was obtained from those who agreed to participate in the interview. Study participants were not nervous and expressed their opinions in a relaxed manner. Participants were also reminded at multiple times during the interview that they could withdraw from the interview any time without penalty.
The interviews elicited narratives on the social and economic impacts of HIV and AIDS and coping with HIV-related financial burdens, labor power loss, stigma, discrimination, and social exclusion. Participants were asked: (1) What impacts (economic, physical, psychological, social) did HIV/AIDS have on your household? (2) How did you deal and cope with these issues/impacts? and (3) What kind of resources and supports did you capitalize upon to cope with these issues/impacts?
Two interviewers conducted the face-to-face interviews in Mandarin, which lasted approximately 1 hr. Participants were compensated RMB 50 for their time (equivalent to US$8, an average day’s wage in this area). This study was approved by the review board of the School of Social Development and Public Policy, Beijing Normal University.
Study Participants
Fifteen women living with HIV in the Central Rural China were interviewed. Detailed information is presented in Table 1.
Sociodemographic Characteristics of Women Living With HIV.
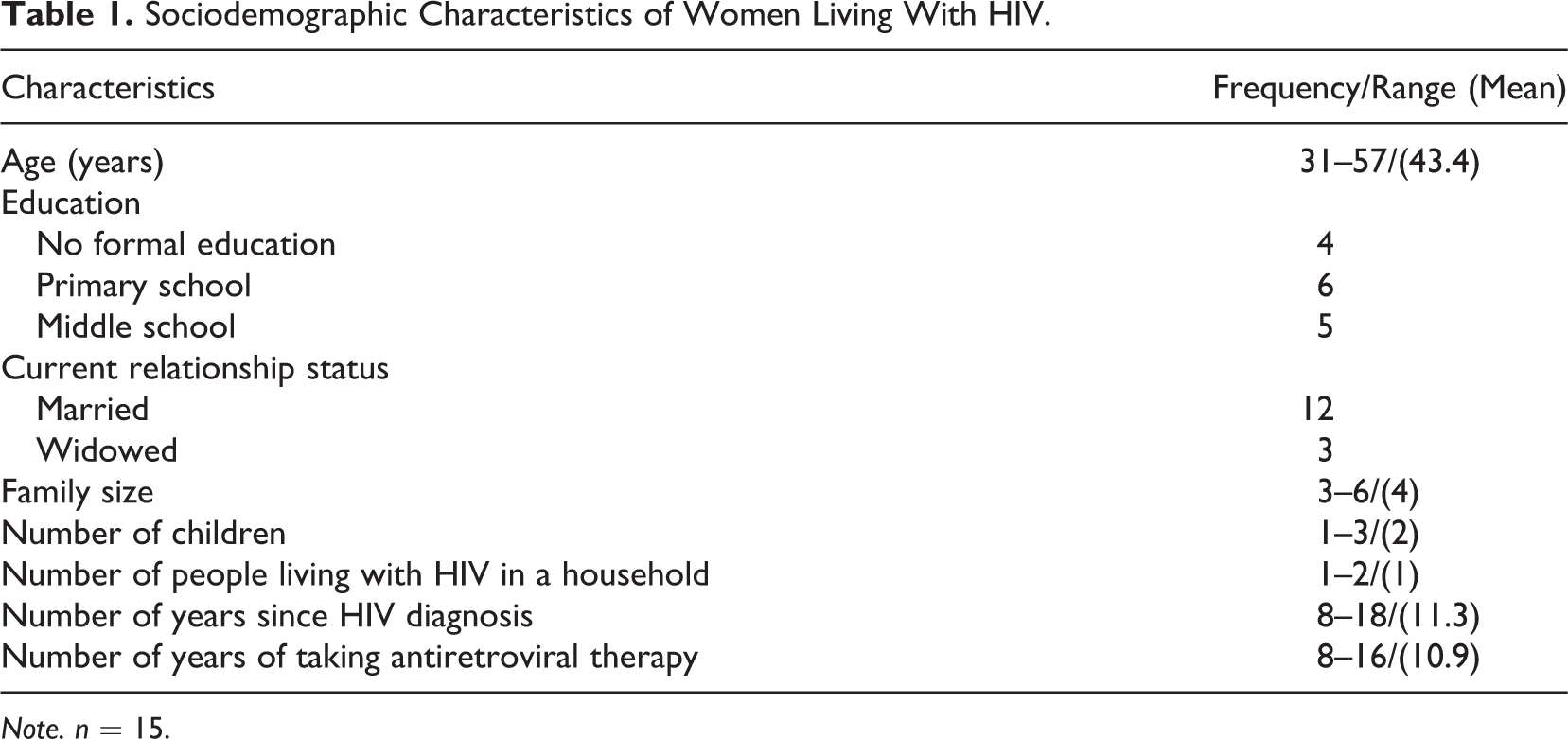
Note. n = 15.
Data Analysis
The interviewers transcribed the recorded interviews. The interview recordings were destroyed after transcription process. The electronic transcripts were kept on a computer within an encrypted drive and with a password that was only made available to research staff. Any identifying information in transcripts was removed in order to assure confidentiality of study participants (pseudonyms were used). After transcription, the transcripts were translated from each participant’s dialect (participants spoke different dialects of Mandarin) into Standard Mandarin. The research questions guiding this analysis were: What were the coping strategies of economically and socially marginalized women who acquired HIV from commercial plasma donorships in rural Central China? What resources and supports did women who acquire HIV from former commercial plasma donorships in rural China capitalized upon to maintain their social and economic well-being?
The data were analyzed using thematic analysis methodology (Guest, 2012). Following inductive analysis, the first step included drawing inferences from the data. This strategy was closely grounded in the study’s objective to examine the social and economic impacts of HIV and AIDS on these women and their families including labor participation, economic hardships, and the coping mechanisms they employed to deal with financial burdens, loss of labor power, and social exclusion. The second step included comparing all data and grouping similar concepts (e.g., financial challenges, disclosure of HIV status) and differentiating those concepts from one another. Based on this approach, the third step included identifying themes, which could describe and summarize the findings under each category. To achieve data trustworthiness, three coders independently coded data, and the coding was later compared for agreements and discrepancies in coding. The debriefing process was employed, in which the coders met regularly to discuss the data analysis process, compare notes, resolve any discrepancies, and recode data in instances of significant disagreement.
Findings
The findings representative of the coping strategies among women living with HIV are organized into two themes: (1) coping strategies aimed at mitigating the financial impacts associated with HIV/AIDS and (2) coping strategies aimed at mitigating the impacts related to social exclusion, stigma, and discrimination within families and employment environments.
Theme 1: Coping With Financial Burdens and Labor Power Loss
The first theme presents finding with regard to the financial hardships. The most direct impact of HIV on households was the loss of labor power. In response to loss of labor power, women living with HIV and their family members undertook a series of strategies to cope with it. These coping strategies are presented below.
Internal remigration of families
After diagnosis, women and their family members remigrated back to hometowns from larger cities where they worked due to HIV-related deteriorating health. As a result, the family income was reduced because wages are lower in a smaller towns compared with incomes in larger cities in China: Before I was diagnosed with HIV, my husband and I worked in Hangzhou city. We earned some money. After diagnosis, we returned to our hometown because of our health conditions. I stayed at home and didn’t work. My husband worked as a bricklayer in our town. The highest monthly income was 1,000 Yuan. The lowest was a few hundred. Compared to work in the city, our income dropped significantly. In the last 2 years, I could not do any heavy work due to my deteriorating health (Xueqin, 34 years).
Reducing labor intensity
Three women also reported how they had to resort to less demanding work and eventually could not do any work at all because of their health conditions. The following quote exemplifies this situation: I drove city guests on a battery tricycle. At the beginning, I could drive people all day and night. After traffic regulation in 2008, I could only do this at night…The disease has a great influence on my physical strength. I want to earn money to afford my children’s tuition…I began to sell fruit. After one year, my health condition became even worse and I could not sell fruit anymore. (Huazhen, 49 years).
Labor reallocations within households
In order to cope with the loss of labor power and diminished capacity to work due to HIV, women also had to rely on their children to help them financially. The following quotes from two women shows how a 50-year-old woman dropped out of the workforce to take care of her grandchildren while her sons became the primary breadwinners: My two children are earning money so I don’t need to work. I stay at home and take care of my grandchildren. Both of my sons work out of town in the city; one works in Nanjing city, and the other in Shenzhen city, and they can make money now. They send me money twice a year. (Jizhen, 50 years) I can’t do farm work now. My husband went out to work. During the farming seasons, he wants to come back and help me to do farm work. I don’t let him come back and instead I asked my relatives for help. I asked my sister and brother’s wife for help. The machine can harvest the wheat but I still need someone to help with the corn (Guixia, 39 years).
Supplementing income and coping with labor loss due to family members’ death
Women living with HIV in this study adopted a variety of coping strategies to improve the economic conditions of their families. Four women discussed how they capitalizing on limited resources and existing social networks. The following quote exemplifies this situation: After my husband died of AIDS, I began to work as a bricklayer’s mate. The daily wage is 20–30 Yuan. When my health permitted I worked every day. Although I felt the pain in my waist and leg, there’s no other way but to work because I am the only breadwinner. The role of government subsidies is very limited and you can’t expect to cover the daily expenditure with them. Things are expensive now; the price of a barrel of cooking oil is 60–70 Yuan. In addition, our land was all occupied due to the construction of many factories. Besides the work as a bricklayer’s mate, I also did the work in the field by myself. I harvested 100 kilos of wheat this year. If I didn’t plant wheat, it’s too expensive for me to buy the flour (Zhixia, 42 years).
Borrowing money
Faced with the financial burdens due to HIV-related treatments, borrowing money from close relatives was one of the most common coping strategies for women in this study: The total medical expense after receiving treatments at the hospital was 140,000–150,000 Yuan. I had to pay that out of my own pocket and there were no reimbursements at that time. We borrowed from my relatives. My brothers and sisters didn’t mind lending me the money; they just wanted to help cure my illness. My elder brother lent me 30,000 Yuan and I got 40,000 Yuan [approximately 2 years income for farmworkers] from my younger brother (Jizhen, 50 years). We borrowed 20,000 Yuan from my sisters and brothers on my mother’s side when my husband was receiving treatment in the hospital. Eventually, he died of AIDS. There was no money to borrow from my husband’s family because my brother-in-law was also infected with HIV and he is very poor (Huaying, 48 years). My family had more than 10, 000 Yuan in medical debts. I raised chicken but eventually spent all my money. We borrowed more than 20,000 Yuan from my husband’s sister to buy chickens and poultry feed (Jing, 33 years).
Reducing food consumption and lowering the standards of living
In order to mitigate the economic pressures, lowering the standards of living and reducing food consumption was one of the common coping strategies of HIV-affected women with lower incomes: I haven’t bought any meat for nearly a year since the spring festival last year. I have no money, so I can’t eat [participant starts to cry]. I don’t have any vegetables for my family. I bought one large 50 kg bag of radish because it was cheap. I pickled some radish (Hongfang, 52 years). How can we eat? We don’t have enough money to make ends meet. I regularly bought pickles and cheap vegetables. I haven’t bought the meat for nearly a year. My children’s physical growth is affected. My son is very thin (Zhixia, 42 years).
Withdrawing children out of school
Due to economic hardships, children of donors had to drop out of schools, which was the common situation for two households. One woman commented: When my husband died of HIV, my eldest daughter dropped out of the fourth year of primary school because I could not afford the tuition. She really wanted to go to school and her academic performance was very good (Huazhen, 49 years). My three children were still at school when my husband passed away. My oldest daughter didn’t continue her study when she graduated from the middle school. I can’t support the whole family by myself. My daughter told me that she decided not to go to school. I didn’t say anything when she told me her decision. How can I afford the tuition for three children (Zhixia, 42 years)?
Theme 2: Coping With HIV-Related Stigma, Discrimination, and Social Exclusion
The second theme dealt with issues of HIV-related stigma, discrimination, and social exclusion. The women and their family members used a variety of coping strategies to reduce the effects of social exclusion due to HIV. These strategies are presented below.
Concealing HIV status from others due to HIV/AIDS-related stigma
Three women in the study talked about the stigmatizing effects of living with HIV. The following quote exemplifies how often women had to conceal their HIV status from other family members due to stigma, discrimination, and social exclusion: My daughter-in-law didn’t know that my husband and I were HIV-positive when my son and her were dating before they got married. She learned about my disease after the grandchildren were born. We didn’t dare to tell her the truth because we feared that she would not marry him. (Hongfang, 52 years). Only my husband knew I had the disease. My mother-in-law didn’t know about it. My mother-in-law discriminated against people living with HIV badly. She has a relative living with HIV and she didn’t let her eat in our home. Now they don’t even keep in touch. I told my husband that he could tell his mother that I had HIV. My husband said that there is no need to tell his mother (Jing, 33 years). I came back to home immediately after my diagnosis. My boss’s wife asked why I went home. I told her that my mother-in-law was sick. I didn’t tell her the truth because my wage of 2,000 Yuan was still in her hands. I was afraid she wouldn’t give me the money. I lied to her that my mother needed to be taken care of (Xueqin, 34 years).
Strategic HIV status disclosure
Two participants in this study also commented how they strategically disclosed information about their HIV status to others. For example: We’ve been hiding the information about my HIV from my daughter-in-law until they started planning the marriage. I told my son that it is the time to let his fiancée know that I was infected with HIV, and that if she didn’t want to get married, he could break up with her. When my son told her about me, she said she was not afraid of HIV and they got married eventually (Chunyun, 46 years). When my two daughters looked for partners, we didn’t hide information about the disease right from the beginning. We didn’t dare to hide it because we were afraid this would eventually lead to a marital breakdown in the future (Zhenmin, 49 years).
Concealing background information in order to avoid employment discrimination
Importantly, women chose to leave their homes to find employment in larger cities in order to avoid the stigma and discrimination in rural areas where everyone knows each other. As the quote below suggests, in order to avoid discrimination many women had to resort to a commonly used strategy of hiding information about their hometowns: Don’t work with people who know you well. If you work away from your hometown, nobody will know that you have this disease because the people around you don’t know you at all. The stranger the surrounding environment, the more secure it is. Some people with HIV who work in the city told me that their bosses inquired about their hometown. If they tell their boss that they are from Fuyang, the boss will know that this place was heavily hit by HIV and will assume that they have the disease. People living with HIV avoid telling the truth in order to avoid stigma and discrimination in employment. If some people want to see my ID, I will say no. When they ask me where is my hometown, I say i am from Taihe county, which is adjacent to my hometown, but it is a town with a lower HIV incidence. Simply put, I will not tell you where I am from (Xueqin, 34 years).
Avoiding weddings and funerals
Three women living with HIV described how they adopted the strategy of avoiding funerals and weddings due to HIV-related stigma with the exception of attending funerals and weddings of very close family members. One participant commented: I didn’t dare to attend the weddings or funerals when I was diagnosed at first. I really worried that people around us had a bad view for me. I only attended weddings and funerals of my sisters and brothers. (Huazhen, 49 years). I really don’t want to attend the weddings or funerals if I don’t have to. Usually, my husband or my children who are HIV-negative will attend these activities. If they are not at home, then I will have to attend. You have to participate in these activities in rural areas. I truly, from the bottom of my heart, don’t want to go out into the world (Zhanlan, 57 years).
Discussion
In summary, this study suggests that in order to deal with the social and economic impacts of HIV and AIDS on vulnerable households in central rural China, women had to undertake a variety of coping strategies in order to mitigate issues surrounding loss of labor power, financial burdens, or HIV/AIDS-related stigma, social exclusion, and discrimination.
Patriarchy-based structural violence was often embedded in social structures that made up the lives of the women in this study, and normalized by institutions, such as families or marriages. The fact that women commented on the effects of HIV on their families, as well as the importance of maintaining relationships with close relatives to borrow money, attend funerals and marriages or navigating HIV disclosure to make sure their children were able to marry speaks of the importance of families and marriages as institutions that organize social life in rural Chinese communities (Fan, 2000).
The findings from this study highlight how HIV-affected families’ income was significantly reduced after migrating back to smaller towns. While the topic of internal remigration of families has received a significant empirical scrutiny since the 1990s Chinese census, which started tracking migration patterns (Liang & White, 1996), the paucity of data on urban-to-rural migration among women living with HIV in China is notable. While it is possible to interpret the migration of study participants to smaller towns as a coping mechanism to be able to shift to less demanding work, of importance here is the fact that it is primarily women who lacked employment opportunities when families remigrated back to smaller towns. Through the framework of structural violence (Farmer, 2004), the fact that women have no employment opportunities compared to their husbands highlights how cultures in rural areas perpetuate systems of discrimination and oppression against women by limiting their employment opportunities.
Importantly, while some women were able to shift to less demanding jobs, such as selling products, there were also participants who reported that they no longer could do any work at all because of deteriorating health conditions. Many women whose health has deteriorated significantly due to HIV also reported that they had to rely on their children, in particular their sons to help them financially, while women themselves had to drop out of the labor market. The commonality of this narrative shows that the opportunities to secure an income for women who were diagnosed with HIV were quite limited, and in most cases forced women to leave the workforce altogether to take care of their grandchildren.
Many women also had to deal with labor power loss due to the AIDS-related deaths of their husbands. These findings are consistent with other literature which suggests that due to the traditional roles ascribed to women in a male-dominated, patriarchal societies women often faced significant hardships after their husband’s deaths as the lone breadwinners for their families (Shisana, Rice, Zungu, & Zuma, 2010). The data from this study suggested that this situation was even more exacerbated for women in the context of continuing displacement of farmworkers due to urbanization, as well as the increasing food prices in China. Thus, overall, the findings indicate how the structural patriarchal violence is also linked to economic and labor systems in China, which structurally disadvantages women both before and after acquiring HIV. Before acquiring HIV, women were performing physically demanding and time-consuming jobs using battery tricycles. After acquiring HIV, women either lost their jobs or their work literally counted for nothing and they became even more financially destitute.
When faced with economic hardships, informal social networks based on kinship (family members, close relatives, sibling) were the main resources that marginalized women relied upon. This finding is not a surprise, given the salience of informal social networks in rural areas in China. However, it should be noted that borrowing money from relatives became a less common practice after the implementation of social assistance programs, the provision of free antiretroviral medications for people living with HIV in China (Li et al., 2016; State Council of the People’s Republic of China, 2006), and after the implementation of tuition subsidies for poor children in rural areas because students previously had to pay a small tuition fee after primary school (Zhang et al., 2011).
To cope with economic difficulties, many women spoke about switching to lower nutritional value foods, which deleteriously affected the health of their younger children, in particular their sons. Previous work highlights that structural violence against girls and women can be evident in food and health-care distributions, where girls and women receive less nutritional foods than their male counterparts in developing countries (Christie, Wagner, & Winter, 2001). In this sense, it is particularly peculiar that participants in this study shared their worries about their sons in relation to food consumption, not their daughters.
Women in this study also spoke about their daughters dropping out of school as a form of coping with the financial hardships. Scholars suggest that in the long term, not investing in their child’s education results in the lowered human, social, and economic capital for the household (Sivard, 1993). These findings are similar to other research suggesting that girls receive less education and young girls are kept at home to perform other forms of labor or to assist their mothers (Mazurana & McKay, 2001; Sivard, 1993; United Nations International Children’s Emergency Fund, 1994).
Women in this study also talked about how often they had to conceal their HIV status from others due to stigma, discrimination, and social exclusion. These findings are consistent with previous work suggesting the effects of stigma and social exclusion on people living with HIV in China (Yanhai, Ran, Ran, & Arnade, 2009).
Given the importance of family as an institution (Fan, 2000), which primarily organizes life in rural areas in China, children’s marriage is regarded as an important endeavor linked to deep-rooted conceptions of procreation. Faced with the HIV stigma, hiding information about this illness from potential partners emerged as a coping strategy so that children from households affected by HIV can successfully marry their significant others. However, through the feminist lens one can elucidate that this strategy differentially affected daughters-in-law from whom the information about HIV was kept in complete secrecy, thus positioning this strategy itself within the discourse on patriarchy.
Conclusions and Social Work Implications
Social workers who pursue careers in HIV care and prevention have to attend to social factors like poverty, unemployment, and stigma in relation to patriarchy. Social workers are urged to use the framework of structural violence (Farmer, 2004) when working with marginalized communities in similar circumstances. The social work profession in China is uniquely positioned to lead efforts to address stigma, poverty, and unemployment as fundamental contributors to health inequalities for this stigmatized population of women living with HIV.
The ethical and social justice implications associated with the lives of HIV-positive women have to be understood in the burgeoning context of the globalization of markets. The provision of significant financial compensations to engage blood and plasma donations is not a phenomenon exclusive to China, it is a common practice in a global context, including such countries as India and Brazil (Kanbur, 2004; Volkow & del Rio, 2005). Although the HIV-infected former blood and plasma donation cohort in China is unique because it is likely the largest known HIV-infected cohort in the world related to commercial plasma donation (Dou et al., 2010), given that 52% of people living with HIV and AIDS in low- and middle-income countries are women (The Joint United Nations Programme on HIV/AIDS, 2013), the social and economic exclusion of women living with HIV is an important global concern. When viewed through a global lens, the hardships, lived realities, and the coping strategies of women who acquired HIV from former blood and plasma donations may be generalizable not only within the Chinese context but also to other parts of the world, thus offering a contribution to a global, social work response to structural violence against women.
Coping with the deleterious impacts of HIV and AIDS and improving the family livelihood is a challenge in rural areas with low economic development. Social workers who pursue their careers in HIV care should take these findings into account by creating interventions that can alleviate the economic destitution of women affected by HIV. Community-based interventions may prove to be the most effective in such circumstances (Chow et al., 2015). In addition, investments and tailoring financial supports and services are urgently needed for women affected by HIV including tax preferential policies, microloans, social assistance, or waiver policies. Previous studies documented that the financial and educational empowerment of women can also contribute to improved coping (Kotzé, Visser, Makin, Sikkema, & Forsyth, 2013). Such initiatives will increase the ability of women to generate income, which may consequently improve the overall situation of HIV-affected households.
Implications for Women and HIV/AIDS Care and Programming
The findings from this study serve as a basis for HIV program and policy initiatives focused on the improvement of the well-being of women living with HIV and AIDS and inform HIV care programs specifically designed for women in low- and middle-income countries. First, these findings underscore the need for HIV/AIDS care initiatives for women that address intersecting social and economic impacts of living with HIV/AIDS, as well as stigma, poverty, and unemployment. Health professionals and service providers working in HIV/AIDS care should also consider the role that economic and social exclusion play in the development of potential negative health outcomes for women living with HIV and AIDS. The findings enable service providers to work with women living with HIV and AIDS to develop strategies to mitigate the deleterious impacts on them when they encounter stigmatization, exclusion, and discrimination because of their HIV status, gender, or socioeconomic status. The results of this study can be used by service providers who work with women living with HIV to identify coping strategies and resources to deal with these negative social impacts.
In addition, these findings highlight the importance of continuing funding support for HIV/AIDS-based organizations and programs that aim to dismantle the social oppressions that impact the lives of women living with HIV and AIDS. Social workers in China should consider implementing improvements in HIV-related community-based care in rural areas and advocate for making HIV care more convenient and socially acceptable for women. Finally, on a structural level, advocacy for policies and protections against the discrimination of people living with HIV can reduce stigmatization, social exclusion, and potentially address barriers to employment at their source for this population of women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundamental Research Funds for the Central Universities (grant number: SKZZX2013052).