
Abstract
It is estimated that U.S. Latinas have a higher risk of developing postpartum depression (PPD) than the general population, with even higher risk among immigrant Latinas. We conducted three focus groups with immigrants from Mexico and Central America (19) inquiring about cultural messages regarding PPD. Groups were conducted in Spanish, and thematic analysis was used to uncover themes. Themes are presented within three categories: views of PPD, cultural messages and beliefs that prevent treatment seeking, and suggestions to promote treatment seeking. Community and family-led efforts to decrease stigma and normalize PPD are suggested.
Although motherhood confers high status among Latinas, some experience labile and negative emotions following childbirth. In fact, the risk of developing postpartum depression (PPD) is higher among Latinas, affecting 37% versus 10–15% of women in the general population (Lara-Cinisomo & Wisner, 2013). According to the Pew Research Center, Hispanics comprise approximately 17% of the total U.S. population and the number of Hispanics is expected to more than double in the next 40 years (Stepler & Brown, 2017). The foreign-born Latino population has increased by more than 20 times in the last 50 years, and the U.S. born population has only increased by sixfold (Stepler & Brown, 2017). This population growth is noteworthy, as research has increasingly demonstrated that disparities exist across ethnicities with social factors, such as support and economic status, influencing health outcomes (Braveman & Gottlieb, 2014). Women of color experience worse maternal and child health outcomes across several indicators compared to White women (Bryant, Worjoloh, Caughey, & Washington, 2010). As the U.S. Latino population has a younger median age than other racial and ethnic groups and a higher birth rate (2.53 children per woman compared to 1.71 for White women; Passel, Livingston, & Cohn, 2012), it is imperative to study Latina maternal mental health. Research on perinatal (during and after pregnancy) depression among Latinas is fairly new and prevalence rates in the literature range from 12% to 59% perhaps attributable to different measurements and different cutoff points (Blackmore & Chaudron, 2014). In a study of 60 Latina immigrants screened with two PPD instruments, Shellman, Beckstrand, Callister, Luthy, and Freeborn (2014) found that 36 (60%) of the women experienced PPD, with 19 (54%) of the 36 depressed women experiencing suicidal ideation. Culture has been recognized as having an important influence on health care, with beliefs, language, and practices affecting health-care-seeking behaviors (Bussey-Jones & Genao, 2003). Yet, research on PPD has largely overlooked the role of culture. This study aims to expand our understanding of cultural beliefs and meaning making of PPD as told by a group of Latina immigrants.
Literature Review
Latinas’ greater risk of PPD compared with their non-Latina counterparts may be related to issues of acculturative stress, lower socioeconomic status, younger age at birth, reduced partner support, geographic isolation, language barriers, possible illegal immigration status, lower education level, and inferior access to mental health services and resources (Lara, Le, Letechipia, & Hochhausen, 2009; Lara-Cinisomo & Wisner, 2013; Paris, 2008; Vega, Rodriguez, & Ang, 2010). Even if PPD is identified, Latinas may attribute the symptoms to stress or family strain and decline treatment because of stigma, cultural beliefs about motherhood, limited English proficiency, childcare issues, or occupational conflicts (Passel et al., 2012).
Latinas experience inequities in social determinants of income and education, known correlates of mental health functioning. Twenty-three percent of Latino families are living in poverty and 40% of Latina-headed households live below the poverty level (Stepler & Brown, 2017). Latinas also face risk of inconsistent access to health care. In 2011, 37% of Latinas were uninsured compared to just 14% of white women. The situation is even bleaker for immigrant women. Lack of access to health care for oneself and one’s family leads to chronic health conditions that steal time from both work and school, often meaning losing a job, or failing in school due to health-related absences (Gändara, 2017). Differences in what mothers perceive as “depression” and what providers ask to screen for depression may contribute to difficulties engaging Latinas for mental health screening and treatment. Chaudron et al. (2005) found that although 50 of 218 Latina postpartum mothers surveyed reported high levels of depressive symptoms, only half of them articulated a need for help. Chaudron and colleague’s findings indicate that although a mother may be experiencing symptoms on a standardized assessment, she may not think it is severe enough or worthy enough of reaching out for help. Oates et al. (2004) assessed the rate of PPD in 15 centers in 11 different countries and found that mothers commonly experienced “morbid unhappiness” following childbirth but did not recognize this PPD to be an illness requiring intervention from health-care professionals.
Social service providers have reported that, in the Latina community, gender roles and stigma may prevent self-advocacy in terms of seeking diagnosis of and treatment for PPD (Lara et al., 2009; Paris, 2008; Vega et al., 2010). Feeling shame or embarrassment to talk to mental health professionals or feeling judged and ridiculed by family stigmatize the process of admission of symptoms and help-seeking behaviors for Latina immigrants (Nadeem et al., 2008; Vega et al., 2010).
The National Alliance for Mental Illness (NAMI, 2016) reports that Latino/as have been identified as a high-risk group for major depression and generalized anxiety order, but engagement into treatment may be difficult since Latino/a immigrants are more likely to seek counseling from primary care or from church rather than mental health providers and many hold cultural beliefs that prevent help seeking. According to NAMI, depression is often stigmatized and seen as weakness and is likely to be communicated through somatic symptoms in Latino communities. Additionally, reporting of depressive or anxious symptoms may be viewed as “complaining” about motherhood in a culture that believes mothers happily adjust to new roles (Blackmore & Chaudron, 2014).
Feminist Theory and PPD
From a feminist perspective, medicalization of pregnancy, childbirth, and postpartum as illness do not acknowledge the social interactions inherent to the experience of becoming a mother (Beck, 2002). Through a feminist lens, motherhood is affected by sociopolitical and cultural elements that must be understood from the mother’s perceptions and experiences (Beck, 2002). Further, feminist theory recognizes the limits of binary thinking, instead of seeking to appreciate complexities (Ferguson, 2017). Intersectionality, in particular, recognizes emergent subjectivities and their interaction including, race, gender, class, and other social divisions (Ferguson, 2017). For a Latina immigrant, the interplay of living as a person of color, an immigrant, and a woman are aspects influencing the experience of PPD that strongly impact help-seeking behaviors. Additional qualities like being low income or having limited English proficiency add further complexity to the interlocking oppressions these women face.
Purpose the Study
Using a descriptive qualitative design (Sandelowski, 2000), the purpose of this study was to gain understanding of how the context and culture within which Latina immigrants mothers exist have informed their perception of PPD and help-seeking behaviors.
Method
Recruitment
Recruitment occurred through flyers in Spanish posted at a family service agency serving mothers with low socioeconomic status. Women interested in joining a focus group informed their family health case worker who then informed our research team. Case workers at the agency briefly informed the women of the content of groups and asked the women to sign up for 1 of 3 possible dates to participate. All clients of the agency had been screened, per usual standard of care, with the Edinburgh Postnatal Depression Scale, which has established validity and reliability in both Spanish and English versions (Garcia-Esteve, Ascaso, Ojuel, & Navarro, 2003). Mothers did not have to be depressed to be eligible for participation. However, based on verbal reports, we estimated that three quarters of participants had experienced some form of PPD. Inclusion criteria included age 18 years or older, Latina ethnicity, live birth within the past 18 months, documentation of PPD screening, and willingness to participate in a focus group on PPD. Based on verbal reports, most participants had been in the United States for at least 1 year. Spanish- and English-speaking participants were included. Institutional review board approval was granted from the university Committee for the Protection of Human Subjects.
Sample
Among the 19 participants, 16 were from Mexico, 1 was from Honduras, 1 was from Nicaragua, and 1 was from El Salvador. Most participants were married (84%), had a prior positive PPD screen (84%), and were an average age of 28 years old with an average household income of less than US$ 23,000 (see Table 1). Fifty-eight percent of the women had less than high school education. Forty-seven percent of the women were first-time mothers.
Description of Sample.
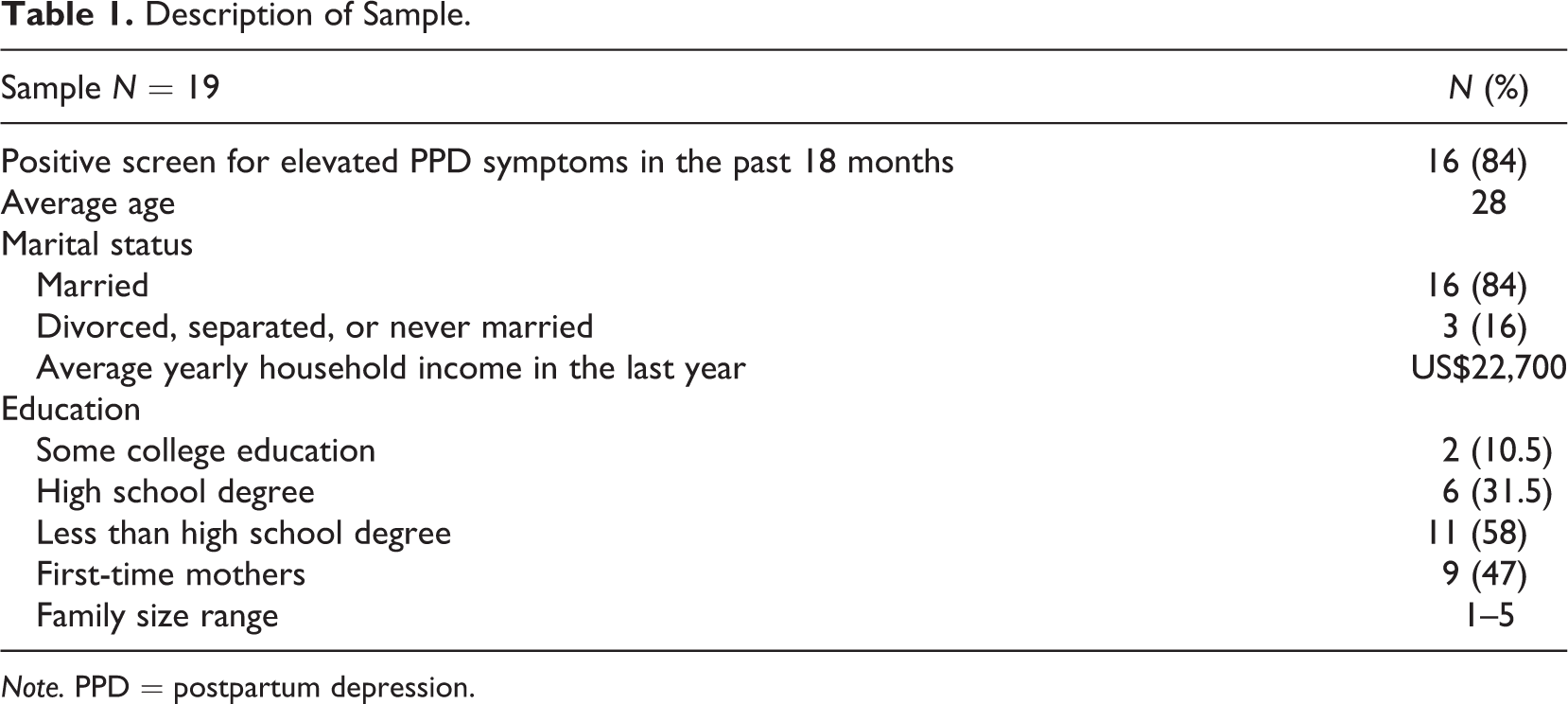
Note. PPD = postpartum depression.
Procedure
The research team conducted three focus groups, a standard for reaching saturation when working with community groups (Krueger, 1994). Focus groups were led by a Mexican American female bilingual graduate student, with the principal investigator (PI) present. All groups were audio recorded with consent. At the beginning of the discussions, the facilitator would announce, “when we say culture we are referring to shared values and beliefs of a particular group that guides thinking and decisions.” This operationalization is based on Leininger and McFarland’s (2006) work that discusses the need to provide culturally congruent and competent care to multicultural populations. Because some participants were not fluent in English but all were fluent in Spanish, the groups were facilitated in Spanish. Group sessions lasted 1 hr each. These following questions were asked When I say PPD, what does it mean to you? What do other women, men, family, community—anyone that shares the same racial or ethnic group as you—say about PPD? What have people from your cultural group said about getting treatment for PPD? What do you think might help or stop moms from getting help for depression after childbirth?
Data Analysis
Recordings were transcribed in Spanish, translated to English, and checked for translation consistency. A six-phase process of thematic analysis (Boyatzis, 1998), as explained by Braun and Clarke (2006), was used to search for emergent themes regarding beliefs and experiences with PPD to understand the data and generate codes and overarching themes. Thematic analysis affords rigor but does not limit the researcher to a particular theoretical framework (Braun & Clarke, 2006). This methodology was chosen because of the exploratory nature of the research and the agency’s desire to know more about cultural beliefs surrounding PPD. For example, thematic analysis allows us to derive the meaning of PPD as Latina women in our sample understood it, both personally and within their cultures.
Transcripts were coded verbatim from English translated transcripts and distributed among the PI and three research assistants (two of whom are Latina). Using the approach recommended by Braun and Clarke (2006; see Table 1), we worked individually and as a group to understand the data. Phase 1 involves familiarizing self with the data. For Phase 2, that is, generating initial codes, researchers individually coded “interesting features” in systematic manner across entire dataset. The PI asked each research assistant to work from a table she had created to organize codes and corresponding quotes. We met after the completion of this phase to discuss codes and draft some initial themes. After transcripts were completed, we created an “aggregate codes” file. For Phase 4, that is, “reviewing themes” the research team worked individually and collaboratively to identify emerging themes. The research team returned to the original transcripts once more to match codes to the data and check for overlooked quotes (Braun & Clarke, 2006).
The team met bimonthly to discuss common themes and differing subthemes within the data. Much of the coding and initial phases of finding themes were done via e-mails with leadership from the PI, but we found the face-to-face team meetings to be the most productive. Phases 3–5, which involve searching for, reviewing for, and naming of themes, required intensive teamwork and respect for each researcher’s interpretation of the data. At the beginning of each meeting, we would revisit the overall story conveyed by the participants and strive to align themes under the broad context.
Trustworthiness in our data analysis was insured by keeping a clear audit trail with one table that tracked every decision made and another table that delineated quotes and themes that had been identified by members of the research team. Members of the research team (PI and three social work graduate students) each read transcripts and made notes of possible categories and recurring statements. With each phase of the thematic analysis, the team would meet in person to discuss. Using an audit trail, peer debriefing, and observer triangulation, we worked continually to increase trustworthiness (Lietz & Zayas, 2010).
Findings
All participants discussed experiences, examples, and knowledge from a bicultural perspective. They identified American culture versus traditional culture and referenced traditional beliefs and societal views of PPD. The findings, illustrated through examples of specific comments, are organized into three categories: (1) views of PPD, (2) shared cultural beliefs/practices that prevent treatment seeking, and (3) mothers’ suggestions to promote treatment seeking. Category 1, views of PPD, includes the themes of (a) PPD is an American problem, (b) women with PPD are considered impotent and useless, and (c) it passes. Category 2, cultural beliefs/practices that prevent treatment seeking, includes the themes of (a) mothers are expected to suffer; (b) acknowledging symptoms or seeking help creates stigma, shame, and loss of community; and (c) Latina immigrants fear accessing services. Category 3, mothers’ suggestions to promote treatment seeking, includes (a) spouses and family should be sought as supportive resources, witnesses, and advocates and (b) women need to overcome their fear of seeking services.
Category 1: Views of PPD
In describing their views of PPD, the women considered how the problem of depression was identified and named in the United States but not in their native countries. The lack of public awareness combined with cultural variations in the care experienced after childbirth left many wondering if PPD existed. Through further discussion about what PPD is, the women articulated how damaging PPD was to their image as a mother. The women also believed that PPD would gradually diminish until there were no symptoms, in part because any experience of PPD they had was viewed as being relatively mild.
PPD Is an American problem
All participants believed PPD was not as prevalent in their native country because of traditional practices that support new mothers and prevent depression. One woman noted, In Mexico, you don’t hear about that [PPD] because our families, our friends, they all support you. They come and make you dinner, tell you not to get up, help you dress. But here [in the United States], no. Here your neighbors don’t even check on you. No one. Even if you have family here, no one checks on you. Here, you are on your own.
Specific cultural practices in their native countries, such as la cuarentena (40 days of child focused care and rest supported by family), were thought to prevent PPD. As one woman said, The 40 days [la cuarentena] help you heal and rest. But here in the U.S., that doesn’t exist. Here, when I had my baby, they gave me 30 days and I had to go back to work. And they told me if I asked for more time off, I’d lose my job. So in 1 month I had to be ready to leave my son. Yeah, that’s hard, but what else? I have to feed my kids.
Cultural practices are described as providing much needed social support that helps Latina mothers’ transition into their new role or situation (first child vs. additional child). Mothers also describe how isolating it can be to be in the United States and how policies limit the opportunity to fully participate in cultural norms like la cuarentena. Further, in their native countries, PPD was not discussed, so even though it might occur among mothers, it was not discussed as a clinical issue. One woman stated, When I came to this country and I had my first baby, that was the first time I heard about this illness. My mom, my sisters-in-law, my cousins—we never talked about it. But when I felt those symptoms after I had my baby here, then I learned about it [PPD]. I had never heard about it until I lived it.
Mothers agreed that, in their native countries, PPD occurs, but the culture does not acknowledge it. One Mexican immigrant reported, Here it has a name—postpartum depression. You might feel bad after you have a baby in your own country, but you don’t know this bad feeling has a name. You might feel bad after you have a baby here, but here it has a name and it’s “normal.”
Women with PPD are considered impotent and useless
Another essential view of PPD described by the women was how experiencing PPD was associated with feelings of inadequacy and powerlessness, which led to feelings of uselessness. One young mother described it as “loss of energy or, like, decay.” Another mother said, You’re impotent. You’re not able to do anything—you’re not even able to help your partner. Well, for me, my husband didn’t have work and I felt stuck and I blamed the baby. I knew it wasn’t the baby’s fault, but that’s what most hit me [begins to cry]. I kept resenting the baby and I was blaming it because I couldn’t work or do anything, you know? That was the worst feeling—impotence. When I had my baby, my brother didn’t live too close to me. It was just me and my husband and I had two kids, I had just had my newborn. And it hit me. I was even on medication because I felt so alone. My mom wasn’t close by and she used to come and help me with the kids. But with the newborn, she didn’t come. So I was alone—my husband worked all day. I was alone with [the baby] and I just felt so alone. Alone. I didn’t have anyone to talk to or help me. All day like that. I think that’s why I was depressed.
It passes
In the final emerging view of PPD, women agreed that the PPD symptoms would pass whether they focused on caring for their families instead of themselves. This belief had been instilled by mothers, sisters, aunts, and friends. Participants said that their feelings were either dismissed or described as a normal part of motherhood: They say “That’s normal, honey, it’s normal.” They say, “That’s the way it should be.” A participant described her process of waiting for PPD to pass: I wanted to kill my kid. But as quickly as those thoughts came, they left. I wouldn’t do those things. I’d think, “I’ll go to jail and what about the others?” So I’d put him in his cradle and I’d go to the kitchen and drink some cold water. And I’d go outside, and I’d hear him crying again and I’d get frustrated again, but I gave him something to eat. Then I hugged him and I started crying. He was, like, 2 months old. I held him and started crying, thinking, “Why would I want to hurt him?” But I didn’t even know why I wanted to do that. The thought just came. But just as quickly as the thought of doing something to him came, it left my mind.
Category 2: Cultural Messages and Beliefs That Prevent Treatment Seeking
The overall message perceived by the participants is that within the Latino culture, the experience of PPD is not validated. From implied stereotypes of the ideal mother, and role expectations to be the nurturer for children and husband, women felt they did not have permission to have depression symptoms or admit the need for help. Needing help with childcare, housework, or with emotions meant being weak. Fear of being judged by elders who claim to never have bouts of depression and fear of deportation were powerful deterrents to admitting symptoms or seeking help.
Mothers are expected to suffer
Cultural expectations regarding being a mother included pressure to be the ultimate caretaker of one’s child and husband and, sometimes, other relatives. Meeting others’ expectations meant cooking, cleaning, and caring for others without complaint. Displaying signs of depression and asking for help were taboo. One mother shared, Another thing, I think, that keeps us, as a culture, from seeking help is the gender roles they give us back in our countries. Women must be strong. I tell myself, “I can do this. I should be able to do it. I need to be strong and do it alone, for my kids and for my family.” I don’t want my husband thinking he has someone useless for a wife. I must be strong for my family. But all this pressure can make us feel worse. Sometimes we need to realize we’re human and can’t always be strong. I had to get up and cook chicken soup for my husband as soon as I got home from the hospital. So I was crying. I was exhausted. I wanted to rest. But the two girls [her children], they were saying they were hungry, too. And the newborn was okay; he was sleeping. But I felt horrible.
Acknowledging symptoms or seeking help creates stigma, shame, and loss of community
Another cultural belief that prevented women from getting treatment originated from the lack of exposure to other Latina women dealing with PPD, particularly those closest to them. Participants reported never having witnessed their female relatives struggle with PPD and felt ashamed that they needed help. This quote captures the bicultural perspective and consequential tension: Sometimes I see my aunts and they had, like, four kids and were in worse situations than me and did well. How can I even approach them with my problems or with this attitude if my life has been easier than theirs? I have only two kids. I can’t ask for help. They’d say, “Look how many kids I had. I did it. You can do it. You have only two kids. You’re in the United States!” No, I can’t ask for help.
Latina immigrants fear accessing services
In addition to the cultural views limiting help-seeking behaviors, Latina women recognized that their immigrant status could be a costly threat. Participants agreed that not seeking treatment was related to a fear of deportation, discrimination related to immigrant status, and lack of Spanish-speaking providers. One woman explained, More than anything, we’re scared to seek help at hospitals because we’re immigrants. For us, it’s not just about opportunity and access. We’re scared. I talked to my sister-in-law, and she said, “Be careful because there are a lot of problems. Sometimes they fool you just to take your kids.” And there are a lot of myths, and it scares people.
Category 3: Mothers’ Suggestions to Promote Treatment Seeking
In the final category of themes, women spoke about potential pathways for supporting Latina women experiencing PPD. Women identified family and professionals as critical observers helping to screen for problems. Women also believed that help-seeking would be more palatable if those around them had a better understanding of PPD and the benefits of treatment. Women recognized that overcoming individual fears could greatly change their outcomes.
Spouses and family should be sought as supportive resources, witnesses, and advocates
When asked what would encourage them to seek treatment, the participants stressed family and community support. Mothers suggested educating the entire family to help with lessening stigma and encourage early identification of PPD. One mother suggested needing others to intervene: It’s easier for people who are around you to notice when you’ve reached that breaking point. I think that at times we moms think, “It’ll pass, it’ll pass,” but then it gets worse the longer you wait. In that case, you need a social worker or your husband to realize what’s going on and help you get out of it. Sometimes when we’re in our own little world of depression, we’re just not aware of what’s happening.
Women must overcome their fear of seeking services
Several women knew about the availability of services but felt that they needed to be encouraged to use these services. One woman said, “When I was pregnant, there was so much information at the clinic and here [at the agency] about help that’s available. But I didn’t look for help because of fear I’d be labeled as sick.”
Stories of being labeled “crazy” or of having children taken away were pervasive. The participants discussed helping other mothers reduce such fears. Everyone wants to hear from other women who look like them, share their culture, and can relate to their struggles. The participants discussed promoting education about PPD and the availability of services. One woman remarked, A lot of women are scared to come here [to the agency]. For example, I had a friend and I’d tell her, “Let’s go to the workshops and talk to them,” and she’d say, “I don’t like doing that. I don’t want to go there.” I’d tell her that it helped me a lot. You come out saying, “I’m learning something new.” With my first daughter, I didn’t know these things and I didn’t take as good care of her because I didn’t know. When I got pregnant again, I came here and learned things. I thought, “Well, it serves me better, I want to go. They’re helping me learn things and do things for my little kids.” So I came and I kept coming, even when I got pregnant again. So I’d tell my friend, “Let’s go. It benefits us.”
Discussion
This study contributes to existing literature on PPD by sharing the perceptions of culture and PPD as told by Latina immigrants. Participants in this study reported their own experiences or other women’s experiences with PPD as immobilizing sadness, loneliness, and confusion. Women who experienced depression after childbirth had an overwhelming sense of responsibility for everyone in the family but themselves. Their PPD symptoms ranged from subtle (e.g., feeling overwhelmed) to severe (e.g., exhaustion, uncontrollable crying, and increased anxiety). This is to be expected, given that research shows PPD can present in a variety of ways including sadness, anger, irritability, and a feeling of being overwhelmed (Beck & Indman, 2005).
Focus group participants shared that their families and communities conveyed beliefs, through actions and words, that new mothers should be able to handle the added responsibilities after childbirth but that they somehow fell short. Most participants were geographically isolated from other family members. They lacked tangible assistance, were culturally isolated, and were too ashamed, scared, or embarrassed to ask for help. This finding is pertinent to Davila, McFall, and Cheng’s (2009) work that found separation from one’s native culture is a risk factor for Latina immigrant mothers, especially those who are isolated from family.
The participants thought that PPD must be a Western phenomenon because here in the United States it has a name. In their native countries, sadness following childbirth, if it existed at all, was to be endured silently. Although it was not explicitly stated, the discussion that “here it has a name” may be speaking to a group belief that in the United States, we medicalize “normal” aspects of birth. There is research to substantiate that PPD is in fact a global phenomenon with prevalence rates in the low teens up to 60% (Halbreich & Karkun, 2006; Lara-Cinisomo & Wisner, 2013). In our focus groups, women mentioned cultural practices such as increased family and community help that may prevent persistent depression versus less societal and familial support during their time in the United States.
Cultural expectations of motherhood seemed to influence the participants’ perceptions of PPD and its symptoms. They discussed feeling impotent and useless as mothers. This is similar to what the research says about motherhood in Latino culture. Motherhood is revered. The concept of marianismo promotes the image of a self-sacrificing, pious woman who, as a mother, is blessed with moral superiority (Stevens, 1973). Acknowledgment of PPD symptoms or seeking treatment for it is in direct contrast to these cultural beliefs. These beliefs were communicated through traditional Latino gender roles, cultural resistance regarding mental illness, and lack of information or empathy from elder Latinas.
Limitations
Because of the community setting, the study was limited to single-site recruitment. The sample is comprised of women who agreed to be in the family services program. They may reflect populations who are more likely to engage services rather than more difficult to reach women who do not engage. The study was also limited by our inability to only include mothers with prior PPD experience. The agency staff, where participants were recruited, asked us to include all interested women who had been screened for PPD (whether or not they had history of PPD) in an effort to increase participation and decrease possible stigma associated with joining. This type of limitation is typical of community-based research where it is important to be deferential to the agency who is an expert on their clientele even when it differs from the ideal sampling situation.
Conclusions and Implications
Results of this study reveal that social workers may need to delve deeper and thoughtfully question Latina mothers of similar demographics. A cursory inquiry into how a mother is doing may not reveal a mother’s true experience or feelings since PPD may be highly stigmatized in her community. Based on our findings, early identification of depressive symptoms is hindered by beliefs that it is not serious, it will pass and depressed mothers are “impotent” or useless. Given the high risk of Latina mothers developing PPD during pregnancy (Davila, McFall, & Cheng, 2009), it is imperative that social workers who have contact with Latina immigrants who are pregnant or early motherhood conduct screenings that are culturally sensitive and will not further alienate or shame mothers.
Fear was a pervasive obstacle for mothers in terms of acknowledging having symptoms of PPD. They were afraid of being labeled as “crazy,” or being judged as an incapable mother. These fears exacerbated their feelings of isolation, depression, stress, and a sense of inadequacy. Lessening fear by normalizing the experience of PPD and bringing in families may be critical for social workers to consider when working with postpartum Latinas in the United States. The women were also afraid of deportation. As one woman said so eloquently, “For us, it’s not just about opportunity and access. We’re scared.” The political climate of immigration and demand for deportation has worsened since these focus groups were conducted. In focus groups, among immigrant women of color, relocation, and undocumented immigration status were discussed as stigmas that compounded their negative feelings (Lazear, Pires, Isaacs, Chaulk, & Huang, 2008). In our focus groups, fear of deportation was mentioned as a reason for not admitting symptoms or seeking treatment. Social workers must build rapport and earn trust to create a safe space for a mother who is an immigrant to admit she may be suffering.
Participants in this study desired a community approach to increasing awareness about PPD—with the goals of decreasing the stigma, encouraging family support, particularly from their husbands, and getting treatment for those who need it. Including the family when discussing potential mood changes with new mothers seems critical for this group of Latina immigrants, and this finding may transfer to other populations of Latinas who share similar beliefs. Asking a patient about her family beliefs may feel less invasive than asking specifically about her mood right away. It would be worthwhile to hold more focus groups with Latina immigrants to explore what factors contribute to PPD once they reside in the United States that the women did not experience in native country.
More research regarding how cultural beliefs may affect symptom manifestation and self-reporting should be conducted and disseminated in social work journals in the hope of reaching frontline workers who encounter newly postpartum mothers. Halbreich and Karkun (2006) suggest that researchers attend to cultural norms regarding postnatal access to health care, religious customs, attitudes of pregnancy and motherhood, and stress when screening and reporting on PPD. More qualitative research is needed to inform culturally responsive methods of identification of PPD and engagement in support programs or therapy.
For Latinas with limited English proficiency, stigma, low health literacy, and unfamiliarity with depression symptoms and treatments may deter women from receiving care (U.S. Department of Health and Human Services, 2001). However, attending to cultural norms of confianza (trust and respect) and simpatia (warmth and support) is useful for improving engagement with clients when discussing mental health (Hansen & Cabassa, 2012). Training social workers to work with culturally diverse clients is critical. Currently, there is a shortage of bilingual medical and mental health professionals and lack of linguistic competency threatens effectiveness of communications about health issues even when health care is accessed (Substance Abuse and Mental Health Services Administration; SAMSHA, 2017).
In an update to its 2009 screening recommendations for depression in adults, the U.S. Preventive Services Task Force now advocates universal screening for pregnant and postpartum mothers (Siu et al., 2016). With a recommendation this sweeping, starting a conversation with a postpartum mother about her mood will likely become protocol. We encourage social workers to lead the way in building safe bridges to open communication about this mental health issue that affects so many women.
Footnotes
Acknowledgments
We acknowledge Neighborhood Centers Inc. for their assistance in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.