
Abstract
This phenomenological study captured the unique perspectives and insight of how 10 black women experience and define leadership in their HIV/AIDS community work. Black feminist epistemology provided the framework for understanding how these women experienced leadership at the intersection of race/gender/power while working on behalf of marginalized and stigmatized community members. Salient themes that emerged from the analysis include leadership is situational and contextual, leadership is inclusive and collective, intent is more important than label, leadership is transformative, leadership is scrutinized, and power is centered in mothering relationships. Their leadership builds on the efforts of the liberation and racial uplift work of the 19th-century Black Women’s Club Movement and emerged as black feminist leadership to address the contemporary social injustice of HIV/AIDS.
Black 1 women continue to be the group with the reported highest rate of newly diagnosed HIV/AIDS cases (Centers for Disease Control and Prevention, 2010). While black women have been engaged as leaders in localized community efforts to address the HIV/AIDS epidemic for the past 30 years, their efforts have been largely unrecognized by mainstream society (McLane-Davison, 2013; Sutton et al., 2009). Within the context of traditional western leadership theories, black women’s community work is not considered a form of leadership (Gilkes, 1980, 2001). Western definitions of leadership are too often legitimized and accepted without regard to the historical and contemporary context of race and gender (Abdullah, 2007; Bell, 2006). Black women have a history of being intrinsically involved in the welfare of their communities as leaders, organizers, and activists (Bell, 2006; Berger, 2004; Carlton-LaNey, 2001; Gilkes, 2001; Martin & Martin, 1985; McDonald, 1997; Simien, 2004). However, their contributions to mobilizing the community, political activism, volunteerism, and leadership are underrepresented in the literature on leadership (Carlton-LaNey, 2001; Gilkes, 2001; Hall, Garrett-Akinsanya, & Hucles, 2007; Simien, 2004). Black women’s leadership is often overlooked because it differs from traditional forms of leadership, and often takes the forms of community mothers (Gilkes, 2001), other mothers (Gilkes, 2001), activist mothering (McDonald, 1997; Rodriguez, 1996), community workers (Carlton-LaNey, 2001), race women (Carlton-LaNey, 1999; Gaetane, 2006), bridge leaders (Tate, 2003), and activist (Nance, 1996; Radford-Hill, 2000; Rodriguez, 1996), engaged in racial uplift (Gilkes, 1980; Slevin, 2005). Despite black women’s continued “caregiving of the race” since pre-emancipation, and particularly in times of political unrest, such as the Civil Rights Movement, their work continues to be limited in mainstream literature (Abdullah, 2007; Barrett, 1995; Collins, 2000; Randleman, 2007; Simien, 2004). Nonetheless, the contributions of black women to leadership are central, and imperative, to the fight against HIV/AIDS.
Researchers (Allen, 1997; Berger, 2004; Carlton-LaNey, 2001; Collins, 2000; Gilkes, 2001; Green & King, 2001; Radford-Hill, 2000; Slevin, 2005; Vakalahi & Peebles-Wilkins, 2010; Vakalahi, Starks, & Oritz-Hendricks, 2007) have concluded that black women developed a unique leadership style, in response to being marginalized and devalued as leaders, as well as in consideration of the intersection of race, gender, and class. While scholars indicate that there are leaders who operate from a black feminist perspective, black feminist leadership is a recent phenomenon defined in the literature by Hall, Garrett-Akinsanya, and Hucles (2007) and as the black feminist leadership model by Abdullah (2007). Thus, more contemporary black feminist scholars have begun to define and rearticulate black feminism as a viable leadership style, behavior, and practice among black women (Abdullah, 2007; Allen, 1997; Collins, 2007; Gentry, Elifson, & Sterk, 2005; Hall et al., 2007). The purpose of this study is to answer the overall research question of the nature of black women’s leadership in HIV/AIDS community work and to center black feminist leadership, not as a comparative, but in its own context. Salient themes that emerged from the analysis include leadership is situational and contextual, leadership is inclusive and collective, intent is more important than label, leadership is transformative, leadership is scrutinized, and power is centered in mothering relationships.
Rearticulating Black Women’s Leadership
A Long History of Activism
During the progressive era (1891–1918), the Black Women’s Club Movement (BWCM) was built on the self-help traditions of Africans in America, while expanding the social welfare of the black church (Martin & Martin, 1985; Sanders, 1995; Smith, 1995; Townes, 1995). These educated women were at the forefront of social issues and the improvement of their communities’ economic, social, and political conditions (Carlton-LaNey, 1999). According to Smith (1995), Black women built the infrastructure of their communities through their religious and secular associations, including church women’s groups, female auxiliaries, and women’s clubs. Clubwork was midway between the work of personal charity and professional social work and, as such, influenced the direction of social welfare work during the Progressive Era. Black clubwomen … were at the center of social welfare work for African Americans. (p. 17)
The BWCM agenda included the commitment to address social justice issues. From 1890 to 1950, a period of legalized segregation in the United States, many blacks saw their struggle for improved health conditions as part of a political agenda for civil and human rights. Although it was difficult for a group with little influence on government to affect public social policy, they attempted to make the health needs of blacks a legitimate political concern for the United States (Nance, 1996; Smith, 1995). Black female community leaders “formed the backbone of the Black Health Movement and were central to the founding and maintenance of African American public health projects” (Smith, 1995, p. 1). They implemented health reform measures at the local level, which translated health policy into health programs for the black community. Black women served as conduits in the community because of their position in the community. Smith (1995) reports “women were the primary targets of African-American public health work because of their influence on the physical and moral health of their families” (p. 1).
Black Feminist Leadership
Many historical examples of black women’s leadership are narrative documentations of politicized activities of a few women such as Ida. B. Wells, Harriet Tubman, Sorojuner Truth, Mary McLeod Bethune, Mary Church Terrell, Fannie Lou Hammer, and Ella Baker who focused on community building (Abdullah, 2007; Barrett, 1995; Carlton-LaNey, 2001; Nance, 1996). These women, although singled out for their individual contributions, acted in conjunction with their gendered and racial peers to bring about social change. The diverse literature, for example, autobiographies, case studies, and so on, and other qualitative research methodologies, reveal common themes around education, family values, the influence of church, commitment to community survival, cooperative work with and the support of black men, social networks, and shared leadership as among the characteristics of black women, which speaks to a unique leadership model. Excluded from participating in traditional political processes such as voting and holding office, black women initiated their own informal and formal means of developing leadership and owning a political voice (McDonald, 1997; Nance, 1996; Rodriguez, 1996; Rosser-Mims, 2005; Tate, 2003). Black women who engaged in the early efforts of HIV/AIDS community work built upon and adapted models of leadership similar to their foremothers of the BWCM and Civil Rights Era, but also in response to being “left out” of initial community organizing efforts and health campaigns that focused primarily on gay white men (Berger, 2004; Cohen, 1999; Sutton et al., 2009).
A definition of black female community leadership (Allen, 1997) suggested that “the struggle for group survival whereby group collective experience, and group socio-emotional support … the instrumental aspects of developing and maintaining internal female networks for institution building, merge to form collective action for cultural maintenance and Black community empowerment” (p. 47). The definition is also evident in the social and historical experiences of black women in America, relative to leadership. Allen (1997) emphasized the importance of “identifying the processes, content, and form of Black female leadership in contemporary America” as a means of “rebuilding the Black community” (p. 3). Over a decade later, the response to this statement has not been fully realized.
The rearticulation of black women’s leadership is both necessary and viable to community building. Missing from traditional models of leadership are the activities and experiences of black women and their continued work for community betterment. Leadership research and the existing literature fails to capture the ways in which black women have self-defined and emerged as the intellectual voice of the community during times of societal unrest.
Black women’s self-defined leadership (Abdullah, 2007) centers black women’s leadership development in African traditions and as a response to political unrest in the community. Moreover, black women’s leadership emphasizes a communal model developed from grassroots efforts (Abdullah, 2007). This model of leadership is in direct contrast to popular models of leadership in educational, political, and business structures that prefer top-down leadership. Abdullah (2007) expanded the concept of self-defined leadership to include four characteristics of black feminist leadership: (1) infinite connection of theory and practice, (2) proactive and not simply reactive, (3) adopts a group-centered approach based on shared leadership responsibility to “own” the movement, and (4) utilizes fluid forms of activism (p. 329). Another definition of black feminist leadership has been defined by those with based on the intersection of race and gender, leadership by example to encourage and create conditions of success (Hall et al., 2007, p. 283).
Black women’s community leadership, black women’s self-defined leadership, black feminist leadership, and black feminist leadership models are conceptualizations of leadership, which will be used to guide the discussion regarding black women leaders’ community work within the fight against HIV/AIDS.
Theoretical Framework
Framing this study was the work of Patricia Hill Collins one of the most consistent voices in the development of black feminist thought (BFT). Collins (2000) contends that the definition of black feminism is entangled in a complicated “nexus of relationships among biological classification, the social construction of race and gender as categories of analysis, the material conditions accompanying these changing social constructions, and black women’s consciousness about these themes” (p. 21). Hill posits a definition of BFT that specializes in knowledge created by African American women and clarifies a standpoint of and for black women. BFT contends that knowledge exists in daily common knowledge shared by group members and is specialized and provided by expert group members that express the groups standpoint (p. 750).
Deconstructing the sexist and racist views of black women, while allowing them to rearticulate their views, offers African American women an opportunity to define themselves on their own terms. Collins (2000) asserts that BFT seeks to uplift black women from a social justice lens based on intersecting oppressions. The eradication of the intersecting oppressions leads to black women empowerment and BFT promotes the transcendence of social justice to address their needs (p. 22).
Method
Research Design
This qualitative study utilized elements of phenomenological inquiry (Creswell, 2007; Vaz, 1997) and black feminist epistemology (Banks-Wallace, 1998, 2000; Collins, 2000; Hamilton-Howard, 2003; Taylor, 1999) to explore the phenomenon of black women’s leadership in HIV/AIDS work. Black feminist epistemology scholars advocate for research that provides a service to black women, rather than simply a discussion about black women (Abdullah, 2007; Banks-Wallace, 2000; Few, Stephens, & Rouse-Arnett, 2003; Green-Powell, 1997; Rosser-Mims, 2005; Taylor, 1998). Thus, this research explored the nature of black women’s leadership in HIV/AIDS community work in relation to their experiences with leadership, community mobilization, the intersection of race and gender, and how their leadership in HIV/AIDS contributes to contemporary leadership models approach effectively captured the unique perspectives and insight on how black women experience and define leadership in their HIV/AIDS community work.
Data Collection
Upon obtaining approval from the institutional review board, participants (see Table 1) were identified and recruited via e-mail and phone, through their involvement in HIV/AIDS community work. Those who agreed to participate were sent a written letter describing the study, requesting written consent to participate, and asked to complete a demographic questionnaire. In order to participate, participants were required to sign and submit the consent form. Prior to the individual interviews, document reviews were conducted including the review of each participant’s résumé, a participant’s agency’s website, and information on the World Wide Web/Google. Two-hour individual interviews using a semistructured interview guide based on existing literature was conducted with each participant. Key participants were asked to identify additional perspective participant who were also sent an e-mail with a letter (attached) inviting them to participate. Oral and written consent was obtained to audio record each interview. Two research assistants also took field notes that clarified the interview data.
Participant Profiles.
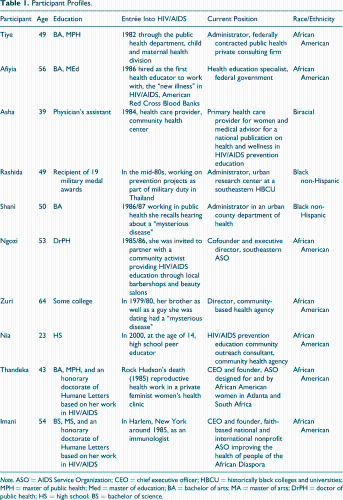
Note. ASO = AIDS Service Organization; CEO = chief executive officer; HBCU = historically black colleges and universities; MPH = master of public health; Med = master of education; BA = bachelor of arts; MA = master of arts; DrPH = doctor of public health; HS = high school; BS = bachelor of science.
Data Analysis
The phenomenological data analysis procedures described by Creswell (2007) provided the structure for analyzing the data. Each taped interview was transcribed immediately following the session. As needed, follow-up phone calls to the participants were made for clarification if there were any concerns about the audible content of the tape. Data were triangulated with the research field notes, résumés, and transcribed oral interviews to ensure that the responses from the participants were appropriately aligned with each question. An initial preparation of the data began with listings of significant statements generated from reviewing the field notes and immersion in the transcribed text.
The transcripts were read and reread to create codes and to generate themes. Significant statements were grouped into larger units of information, called, “meaning units” or themes. A description of “what” the study participants experienced with the phenomenon, also known as a “textural description,” was added. A description of “how” the experience happened, also known as the “structural description,” was documented. Finally, a written composite description of the phenomenon incorporating both the textural and the structural description was generated. This integrative description or passage is the “essence” of the experience and represents the culminating aspect of a phenomenological study.
Interrater and Interobserver Reliability
Reliability was achieved through the use of an independent researcher and research assistants in coding and mind mapping, field notes, and analytic memo review. Mind maps (Gunter & Nelson-Crespo, 2002) were created independently by the researcher and research assistants and compared to establish similar observations of the codes. This technique provided a visual brainstorming method to understand the relationships between the words. Additionally, an objective researcher not connected to the study was asked to review the transcripts for codes and to arrive at the final codes that were used to develop the phase of meaning units.
Limitations
The small sampling size (10) may jeopardize the ability to generalize this study. However, generalization is not the focus or goal of qualitative studies (Creswell, 2007). Although the sampling size was small, their professional and educational paths are reflective of both national and international experiences. None of the women self-identified as HIV/AIDS positive in this sample. In lieu of the rising rates of HIV/AIDS among black women in the United States and across the Diaspora, this voice is missing. However, the researcher did not feel that this undermined the experiences of the women who worked with and on behalf of HIV/AIDS-infected black women.
All of the women self-reported in the study. Direct observations and confirmation from others who work with these leaders on a daily basis may have provided insight as to how they cope with the underlying stressors of race and gender in their environments, as well as how leadership is experienced by these women. Although initially participants consented to the use of their names in the final document, after about the fourth interview, the researcher noticed that the participants seemed to be guarded with their answers. Intimate details around their experiences as black women were seen as sensitive subjects and some of the women seemed to answer questions to please the researcher. They made comments like, “is that what you wanted?”; “I’m not sure if I’m answering your question right”; “well off the record”; or “you’re going to have to turn that thing (the tape recorder) off.” However, the women openly welcomed the researcher into their home or their place of work. Beforehand or afterward, they gave the researcher tours, introduced the researcher to colleagues, and/or gave the researcher extra items such as agency newsletters and reports. Thus, there was a balance between trust with their personal story and distrust of how persons may interpret their story.
Findings
Findings showed that black women in HIV/AIDS leadership were engaged in various aspects of the struggle including direct services, such as community outreach, health care providers, public health officials, and as executive directors of their own agencies. There was a strong connection between their professional and private lives. Their work involved uplifting other black women to develop the internal and external resources to address social injustices, but especially combatting HIV/AIDS. Each participant expressed commitment to the value of creating positive and nurturing relationships as a part of their leadership style. Their leadership experiences described a host of qualities that were based on the collective understanding of being both black and female.
Although the definition and the role of leadership were used interchangeably, the women described the role of leadership as one of the service and nonpositional, so there was not necessarily a top-down approach as described in more traditional forms of leadership. They described the role of leadership as less authoritative and more supportive, empowering, motivating, and visionary. “I consider myself to be a servant leader, inspiring, motivating, and helping to empower people. I don’t think that leadership is doing to or for people but rather working with people (Zuri).” While Thandeka saw the role of leadership as “service through demonstrating and working a vision that you have chosen to share with others,” Ngozi infused power as a component of her leadership, which included empowerment; “I use my power to motivate people who think they’re powerless to feel more powerful. I try to use my power to reduce stigma among people that traditionally have been oppressed so that the broader community sees them differently.” Hence, leadership was simultaneously a role, definition, and action. The themes about the nature of black feminist leadership in HIV/AIDS community work are described in more detail subsequently.
Leadership Is Situational and Contextual
The participating women described leadership as situational and contextual and in part as a living entity that is utilized by the group and for the group to achieve an outcome. Their leadership in working with black women in the community was a reciprocal relationship that is interdependent and based on a commitment to pull together to do collective work on behalf of the communal survival.
Tiye, a program manager, with 27 years of experience in the field of HIV/AIDS prevention, captured the essence of leadership as an inclusive approach that includes shared responsibility toward a common goal. I think leadership is the ability to listen to all sides, work with people, and facilitate a common ground. To help the group develop a process and move it forward. It’s understanding that no man is an island and you can’t do it all by yourself. Everybody brings to the table talent or skills and experience and background. As a leader you place yourself as someone who can facilitate a process. I think leadership is one who acknowledges responsibility to influence others and to guide and direct both persons and maybe the way a policy or things are governed to create change. I hope someone in leadership acknowledges their position to influence and to create change and to cause a shift to occur both in people and the environment. And then with the acknowledgment of that influence has the responsibility that they can guide and advise and help stir people to do or help people change the way they do things into a better way.
Leadership Is Inclusive and Collective
The definition of leadership as described by these women leaders was based on their integration of both their definition of leadership and their role as leaders. Thandeka, a CEO of a national and international AIDS Service Organization (ASO) working with women and girls of African descent, with 23 years of experience in the HIV/AIDS field saw the role of leadership as, Service through demonstrating and working a vision that you have chosen to share with others. It is the willingness to be in front; the willingness to be at the side of those in the front; it is being the backdrop so others can be in front. Leadership is taking responsibility of your ideas thoughts and action. It is also about creating space for others recognizing and others to be recognized.
Black women’s leadership was also described as analogous of an extended family with a collective experience and voice focused on a common goal. Thandeka described this linked fate as a fictive kinship to one another that recognizes differences and diversities, but respects the finality that there is a common bond to our lives. Kinship-the leadership I experience with for, around, Black women is a common bond. The horizontal diversity is the least and most common denominator for Black women and says we can change whatever we need. We will get it done better when we recognize all of our strengths.
Intent Is More Important Than Label
Asha prefaced her response based on her work as a health provider for HIV-positive women. As she processed her answer out loud, she arrived at a term more to her liking, “human rights leader.” I’m sure it can be called Black feminist leadership but that’s something that someone needs to try and get a further understanding of. I mean how important or how dedicated I am to women, to women’s health, to Black women’s health, to the health of women of color, to equal opportunity and rights, to healthcare access, and an opportunity to access information that leads to health and wellness for not just women but our teens and our young women and our adolescents and our women and children who we really need to be spending more time educating. But—so this can be a definition, but I don’t like to be put into a box or to put titles on. Yes! I would call this Black feminist leadership, because I think there is a basic differentiation from a non-theoretical standpoint, from a lived experience, how I see it, how I feel it, perspective. Feminism, while it’s not for everybody, by its very definition has a limited focus on what equality entails and leaves room for different identities to define equality in different ways. Most people think of feminism as broken down strictly along misogyny, along gender discrimination, along inequality among sexes. I think Black feminist theory takes equality from a woman’s standpoint to another level of recognizing the intersecting complications of race/class/gender/power/sexuality as a whole in terms of addressing equality. I think that multiple oppressions become more clearly defined by people who live the experience of being Black and female.
Leadership Is Transformative
Asha described her leadership style as transformational in terms of health care for HIV/AIDS positive women. In her opinion, persons in leadership possess, A powerful, powerful, strength that they would need to be sensitive and yet transform pain to power among the women that they’re influencing, not just pain but fear to faith. I mean they have to be these transformers and excellent researchers like librarians they have to be full of resources because unfortunately there’s not one stop shop for women, community women that are infected. I came from the segregated South where the focus has always been on saving the people. I sat at the table with my grandparents, aunts, uncles, mom and dad where the discussion was always centered at saving Black people. Right now the issue just happens to be saving Black people from HIV/AIDS. We have got to save the race! This is our time so that our children’s children will be able to save the community for the next generation.
Leadership Is Scrutinized
Leadership experiences of black women differed from their male and white counterparts based on numerous factors. Leadership is scrutinized and validated based on gender and race both internally and externally to the black community. The women discussed issues of institutional racism, historical racism and sexism, internal (within the black community), conflict, and the overarching pressure of constantly having to legitimize their presence as a leader.
Tiye started out describing how she wanted to believe that all leaders are created equal, but confessed that her experience as a leader as one of constant struggle, offense, defense, and comparison of skills and talents that never seem to quite measure up. I’d like to say leaders are leaders. I think what happens when you start looking at Blacks specifically, or people in color in general, and you try to compare them to the majority community, the white community, they always want to make us jump higher and run faster in order to prove that we are equal. I think our fight as leaders in the Black community and as women is a lot harder, because, the expectation is there is a ‘present foot on neck syndrome.’ There’s always a need to over compensate, be smarter, be louder, be more articulate, write better, present better, look better and unfortunately as Black women we’re also judged by our appearance. We are pitted against our male counterparts and in some circles it’s easier for the sisters than for the brothers, in some cases it’s harder. When women are being aggressive or a little bit more animated and into her culture and her femininity then they want to call you the “B word” and say that you’re angry.
Power Is Centered in “Mothering” Relationships
Power was defined by these black women in leadership as the ability to influence people’s thoughts and actions, attitudes and beliefs about something and involved influence, control, or the ability to persuade something or somebody to “move.” For them, their power was centered in relationships, particularly, in mothering characteristics that extended past their biological roles. Mothering meant teaching prevention education, guiding and referring them toward appropriate health services, nurturing relationships, utilizing scarce resources, or/and advocacy on the part of their consumer base.
Thandeka believed that black women were necessary to the survivability of the community and thus had the greatest opportunity to effect change through their positions of visibility in the community. She discussed how black women, as mothers, have always had the solutions and are resourceful, and therefore, they can use these skills to also resolve concerns regarding sexuality and HIV/AIDS. In our communities and especially our urban communities there are a disproportionate number of female headed households with no male partners. Our schools, are where our children are disproportionately taught and administrated by Black women. Our churches are worked, coordinated, the ministry work, and congregations are mainly represented by Black women. In the workplace women of color do the majority of the back breaking work which is the hardest of the organization. Just by the fact that every aspect of daily living and building communities is dependent on the resources of those communities mainly being the women, more so women of color, and Black women, then by in large we have the greatest opportunity and power to create change in all those spaces. Black mothers have always known what to do!
Discussion
This study examined the nature and characteristics of black feminist leadership in HIV/AIDS community work. Black feminist epistemology (Collins, 2007) provides the filter through which black women experience leadership at the intersection of race/gender/power. As a result of these lived experiences, we gained a better understanding of power imbalances, power centers, hidden agendas (Taylor, 1999), and unspoken barriers and hurdles in working with marginalized and stigmatized communities of African ancestry. Their leadership was a tangible product of their passion to fight for the liberation of their community against the devastation of HIV/AIDS and its accompanying demarcation in parallel issues of oppression, stigma, and discrimination.
For black women in leadership, their lived experiences at the intersection of multiple oppressions (Collins, 2000) indicate that they have a means of knowing how to address the issues that impact the black community’s quality of life and mortality. Their early leadership experiences were shaped by their family values, community and church involvement, and being in communal relationship with others. As pioneers in the HIV/AIDS fight, the women spoke about being the “first,” or the “one and only” in a room full of others who were there to address the new disease called AIDS. As leaders already working in the community, they admitted in the early days they didn’t know what to do, but they knew something had to be done to help save the people. For the majority of the women, returning to school and earning additional degrees, while simultaneously participating in community and public health trainings, provided additional opportunities for them to address the issue of HIV/AIDS in their communities. Their collective commitment to each other as community leaders was emphasized, as they talked about being side by side with other committed sisters, who provided a reciprocal peer mentorship and a safe space for them to strategize, take risk, vent, and celebrate.
Implications for Social Work
This study speaks to several implications that are at the heart of the social work profession. First, it introduces black feminist epistemology as a vital framework that encompasses the major values of social work such as social justice, importance of human relationships, integrity, and competence (Vakalahi & Peebles-Wilkins, 2010; Vakalahi et al., 2007) and provides a context by which professionals can develop culturally competent means of working with a community at the micro, mezzo, and macro system level. Second, it emphasizes a commitment to mutual aid, self-determination, and collective work and responsibility as described in the National Association of Black Social Workers Code of Ethics (Reid-Merritt, 2010).
Third, within the context of black feminist epistemology, black women have been considered “race leaders” (Carlton-LaNey, 1999) of the community. They have a historical legacy of tackling social justice issues such as poverty and health disparities in the face of race and gender discrimination. Much of our current curriculum in social welfare history and leadership omits the legacy of black pioneers and historical social service mutual aid societies (Carlton-LaNey, 2001; Martin & Martin, 1985). The inclusion of these rich models of leadership could contain significant insight for addressing many of the current urban social problems.
Fourth, their community activism and use of culture, gender, and race, as agency of change offer a renewed strategy for working in communities that have been overwhelmed with multiple social problems. Utilizing grassroot strategies and social networks helped these women to have a more significant impact on addressing issues when government resources were limited. Black women leaders activated their mothering power to build relationships and gather funding, knowledge, and other vital resources. For them, their extended mothering countered the discrimination, stigma, and neglect for human life that was often a part of HIV- and AIDS-positive diagnosis. There is a push toward clinical and licensure in social work education that will help better prepare professionals to deliver direct care services. However, clinical skills appear to dwarf the curriculum of community organizing and activism, some of the founding skills and principles of the profession. Black feminist leadership with HIV/AIDS community work provides examples of leadership with marginalized communities and populations, indicating that community emergence and relationship building can have a profound impact.
Fifth, leadership is experienced within the context of position and title, but mostly by action and relationship to others. Black women’s leadership is dynamic, compassionate, relational, familiar, inclusive, visionary, and transformative. The collaborative nature of their leadership meant that power was also fluid. Leadership involved being a part of a supportive cast with a shared vision that produced change. As a result, these women experience remarkable success in their roles as leaders with persons impacted by HIV and AIDS. Their willingness to act in conjunction with those infected with HIV and AIDS, along with invested stakeholders, created an atmosphere of trust and cooperation that helped them to expand their influence. Much of the social work literature and curriculum borrows from traditional models of western leadership, which are steeped in patriarchal forms of power that exclude and are hierarchal. As our society becomes more culturally diverse and globally focused, other forms of leadership, including black feminist leadership can serve as valuable models.
Finally, black women’s leadership in HIV/AIDS builds on the efforts of the liberation and uplift work of the Black Clubwomen of the 19th century, as well as the black communal leadership of the Civil Rights Era, to address the social injustices of HIV/AIDS. The integration of theoretical frameworks that are inclusive and affirming to black women’s lived experiences may be a renewed opportunity to significantly improve the life of those infected with HIV/AIDS, while simultaneously adding to their self-determination. Examining the historical content of indigenous leadership, such as black feminist leadership, can provide a blueprint for the development of future leaders in the HIV/AIDS fight and social services.
Footnotes
Acknowledgment
This author is grateful for the women who graciously shared their journeys of leadership through the pioneering days of HIV/AIDS community work. Their voice, although often edited and sometimes muted, is significant to the continuous fight against this pandemic. This research serves as a documentation that their work was and will always be phenomenal.
Author’s Note
This article has not been published elsewhere and has not been submitted simultaneously for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.