
Abstract
Social capital is positively associated with adult health and well-being. We know little, however, about the impact of social capital for women, especially those from developing nations. Knowledge of this relationship is important not only for women but also for social workers engaged with this population. This study examines the impact of social capital on the health and well-being of 6,099 women in Indonesia. Results indicate that education and trust positively correlate with health and well-being. The findings are relevant for social workers at a direct practice and programmatic level to offer services designed for improved health and well-being.
A well-documented and positive relationship exists between social capital and adult self-reported health and well-being (Almedom, 2005). Yet, studies examining this link for women (Adkins, 2005), especially those residing in lower resource countries (Yip et al., 2007) such as Indonesia, are lacking. Women living in poverty experience poorer health and well-being than their male counterparts, but the effects of social capital may help to mitigate this disparity. The authors will discuss feminist theorists’ concerns related to social capital, in addition to examining the potential benefits of this resource for the health and well-being of women in poorer nations, in order to better inform social workers serving this population.
Review of the Literature
Bourdieu (1986) explains that social capital, which can be conceptualized as community engagement, trust, and reciprocity, is “the aggregate of the actual or potential resources which are linked to…membership in a group” (p. 51). Social capital provides potential benefits, such as larger social support systems (Dominguez & Watkins, 2003), interpersonal cooperation, and community cohesiveness (Putnam, 2000). Additionally, specific forms of social capital (e.g., membership in voluntary organizations, trust of others, and social participation) can positively impact health (Almedom, 2005; Yip et al., 2007) and well-being (Biddle, 2012). Although research specific to Indonesia is limited, one study found that membership in community-based organizations correlated with improved mental health (Miller, Scheffler, Lam, Rosenberg, & Rupp, 2006). Yet, social capital is not equally accessible by all and is often unavailable to marginalized groups who may need it most (Lin, 1999), including women (Adkins, 2005).
Social Capital and Gender
Feminist theorists have provided a critique of social capital, raising several relevant concerns, including the relationship with gender analysis (Gidengil & O’Neill, 2006; Schuller, 2007), power relations (Adkins, 2005; Alfred, 2009), and the over-engagement of women in social capital programs and mobilization (Molyneux, 2002). Social capital is seen as reinforcing masculine values and being built on traditional gender-labor division (Adkins, 2005), which tends to place women in caretaker positions both in the family and the community. Women are also often in lower positions of power than men, which impacts whom they connect with. Individuals draw benefits only from those networks in which they can participate, so individuals with less power and influence rarely connect with those who have high power and influence (Bourdieu, 1986). As such, female’s networks often provide noneconomic resources and rely on women’s time and nonmonetized labor exchange (Adkins, 2005). Thus, women may be separated from the very “networks with critical information that can enhance women’s development and career and life transitions,” (Alfred, 2009, p. 9; Lin, 1999). Furthering the discrepancy is that gender inequality can even be exacerbated, since at the same time that women are not engaging in the same networks as men with greater power and resources, men are simultaneously benefiting from them.
Another concern is that programs aimed at employing women’s social capital for development fail to address the underlying social, cultural, and family structures that create gender inequality to begin with. As opposed to advocating for real social change, women are asked to neglect other activities in order to volunteer and engage in community programs that will aid in capital accumulation. As Van Staveren (2002, p. 2) explains, “social capital appears to be a notion that tries to address a serious gap in economics, a gap that is also sharply criticized by feminist economics.” Yet, the responsibility to address the gap through programs focused on social capital places the responsibility solely on women. Thus, Molyneux (2002) and Rankin (2002) point out that social capital should not be the targeted approach to addressing poverty when the key concerns lie with the inequality and lack of power on a larger (societal) scale.
Although concerns exist for social capital and women, community engagement/participation is shown to offer women some benefits (Anucha, Dlamini, Yan, & Smylie, 2006). A contributing factor may be that excluded groups, such as women, develop closer networks and forms of social capital than nonexcluded groups (Franklin & Thomson, 2005), and greater isolation tends to yield stronger connections (Gaventa, 1982). Thus, women in societies that exclude them from positions of power, such as Indonesia, may develop stronger bonds and better accumulate social capital than those in other locales. The authors suggest that utilizing this social capital for positive gain is one step in the larger picture of improving women’s well-being.
Social Capital, Community Participation, and Gender in Indonesia
Indonesia is a lower middle-income country and the fourth most populous nation (World Bank, 2012a). Women in Indonesia are less educated than men, have lower rates of employment, and are less likely to hold leadership or make decisions within their households (International Fund for Agricultural Development [IFAD], n.d.). Further, Indonesia’s development agenda more strongly values male-dominated employment, so that women often have low-paying jobs (Arif, Syukri, Holmes, & Febriany, 2010), work in the informal sector without public benefits (Akhmadi, Budiyati, & Yumna, 2010), and experience higher expectations to perform household duties that prevent them from spending time on higher paying employment (KAPAL Perempuan, 2013). Nearly half of the population lives on less than US$2 per day (World Bank, 2012b). Poverty disproportionately impacts women (United Nations Development Program [UNDP], 2009) and is linked with emotional well-being (Yamaoka, 2008). As such, Indonesian women experience higher rates of sadness and anxiety than do men (Das, Do, Friedman, McKenzie, & Scott, 2007; Miller et al., 2006). These concerns may be compounded by the social structure in which they live. In response to the inequality and poverty and its impact for women, various government and nongovernment organizations have designed economic, health, and social empowerment programs for women and their families (Imelda, 2011; UNDP, 2009).
Two examples of such programs in Indonesia are Rotating Savings and Credit Associations (ROSCAs) and Pemberdayaan Kesejahteraan Keluarga (PKK or Family Welfare Organization). ROSCAs are an interdependent loan program in which members contribute a fixed amount of money to create a large group sum that is lent to one member at a time (Varadharajan, 2004). When the first borrower repays the sum, a second member then borrows the money for a set time and so forth. ROSCAs enable individuals without access to formal loans the ability to borrow money and also create a network built on membership, trust, and reciprocity. Thus, the potential benefits extend beyond financial gain and have been shown to improve women’s well-being in Kenya (Anderson & Baland, 2002).
PKK is a government-directed, but community-facilitated program designed to support mothers and pregnant women through a wide range of services, such as family planning and support groups (Imelda, 2011). Women form bonds and trust by gathering to discuss sensitive and often stigmatizing issues. This trust in one another has even been employed to expand awareness and develop other targeted health-prevention programs, such as HIV prevention, specifically for women (Imelda, 2011). In this way, women mobilize the resources from social networks to better address health needs within their communities.
Social capital is considered by many to be a mechanism for empowering women through increasing knowledge of resources, life skills, self-esteem, and community connections (Messias, De, & McLoughlin, 2005; Mok, Cheung, & Cheung, 2006). In many societies, although, women have been excluded from community participation (Lister, 1997), so that they lack influence in social or political affairs. When development-based community programs are aimed at women, they may offer opportunities for a more active voice in community affairs while also building on women’s roles as social and economic change agents in families and communities (UNDP, 2009).
Although programs promoting social capital among women are prevalent in Indonesia, data examining their impact is limited (Amar, 2010; Imelda, 2011). As the social structure often limits women’s access to power and formal resources, understanding the role of social capital is critical. This study aims to fill a gap in the research by analyzing the relationship between three forms of social capital (community participation, social trust, and social support) and the health and well-being of women in Indonesia. These findings can assist social workers to better serve women by tailoring programs to strengthen the most relevant forms of social capital.
Method
Data and Sample
This study utilized data from the Indonesian Family Life Survey, designed to provide information on a variety of topics, including social capital, health, and well-being at the individual and household levels. The data were collected between 2007 and 2008. Using stratified random sampling, the original sample consists of 45,000 individuals selected from 13 provinces. For this study, the inclusion criteria were being female, 15 years of age or older, and participation in at least one type of community organization. After taking into account the inclusion criteria and excluding missing cases, the resulting sample size was 6,099.
Measures
Dependent variables
There were three dependent variables in this study: health, mental health, and well-being. Health was assessed using a single question: “Generally how is your health?” Mental health in terms of depression was measured using a shortened version (10 of the original 20 items) of the Center for Epidemiological Studies Depression Scale. This scale is used to identify current depressive symptomatology related to major or clinical depression in adults and adolescents and has good to excellent reliability and validity (Radloff, 1977). Finally, subjective well-being was assessed by the question, “Taken all things together, how do you feel right now?” This single measure of happiness has been used in many studies, including the U.S. General Social Survey, to capture life satisfaction or overall well-being.
Independent variables
The independent variable included the following three elements of social capital: community participation, social trust, and social support.
Community participation
This question assessed respondents’ participation in both formal and informal organizations, including community meetings in neighborhood associations, PKK (noted earlier), Community Health Post (a partially government-funded program run largely by female volunteers that provides health care for mothers and infants), ROSCAs (also noted earlier), and religious groups (community-run activities that provide religious teachings and are typically run by female volunteers in the community). Participants provided a “yes” or “no” response as to whether they had participated in each organization.
Social trust
Social trust was measured using six questions to assess respondents’ levels of trust in others and trust in the general community. Examples of trust questions include “How safe do you consider this village?” and “In most parts of the village, is it safe for you to walk alone at night?” The questions reflect respondent’s social trust in people in general and in the neighborhood and community. Responses were provided on a 4-point Likert-type scale with 4 indicating higher trust. These answers were reverse coded for analysis.
Social supports
Questions on social supports included four types of social supports: assistance/aids (e.g., foods, money, child care) received by respondents in the past 12 months from extended family members and assistance/aids received from friends and/or neighbors. The social support questions also asked respondents about membership in two government welfare programs: Unconditional Cash Transfer (UCT) and Rice for the Poor (a food security program). The UCT is a government program to help individuals who are poor by providing a direct cash transfer program given in four installments over 1 year. The Rice for the Poor program is a government program to provide rice for those who are poor.
Demographic variables
Several demographic variables were included: per capita expenditure, education (years), age (years), marital status (married or not married), having children under 15 years of age at home, living in Java (home to the capital of Indonesia and 60% of Indonesian residents), being head of the household or spouse of the household head, and being Muslim.
Analyses
The purpose of the analysis was to assess whether social capital, in terms of community participation, trust, and social supports, impacted the health and well-being of Indonesian women. Bivariate correlation and two regression models (ordinary least square regression and logistic regression) were used for this analysis. Frequencies and means were run for all variables.
Findings of Descriptive and Regression Analysis
Descriptive Analysis
Sample Characteristics of Demographic Variables.
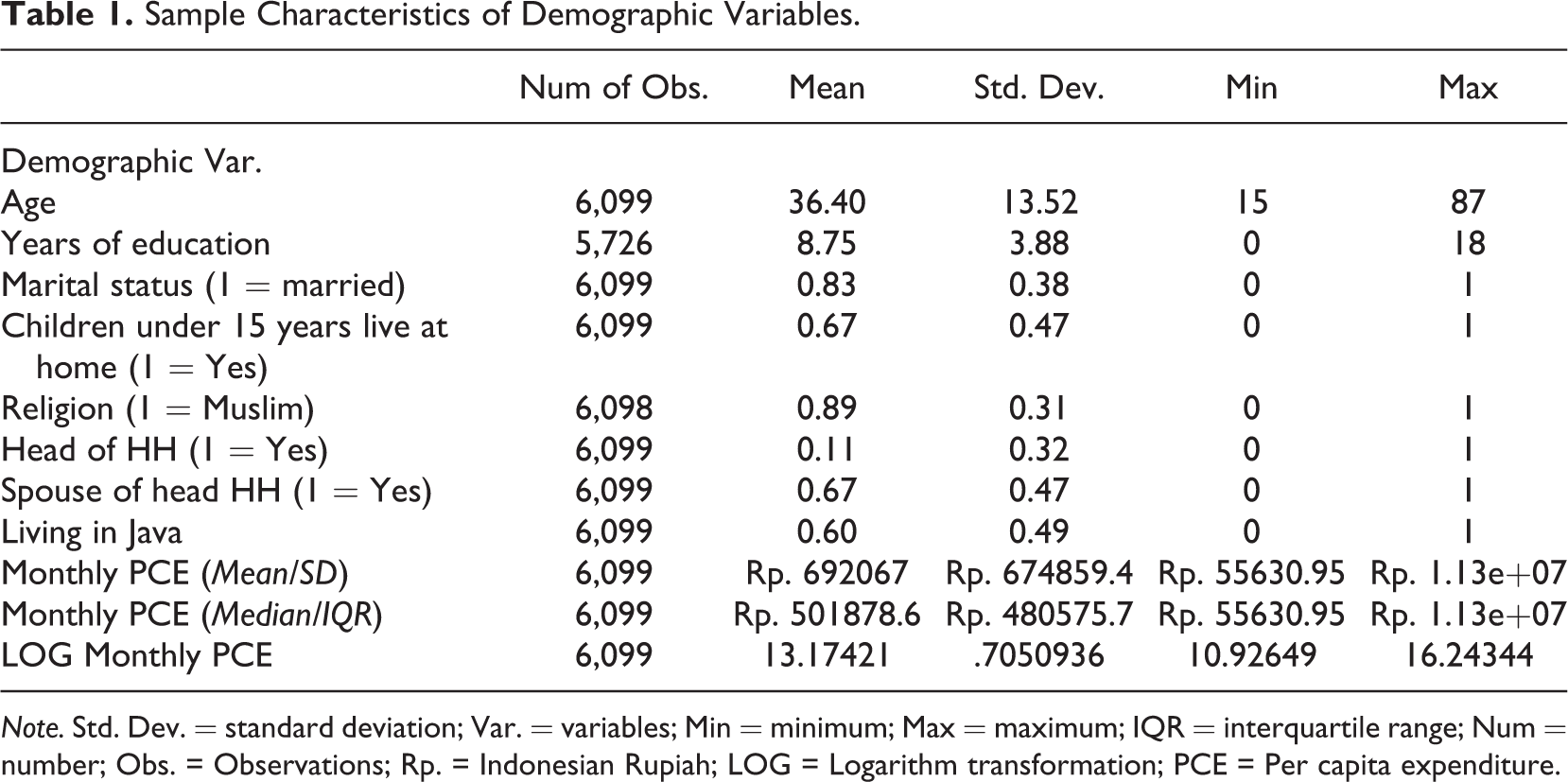
Note. Std. Dev. = standard deviation; Var. = variables; Min = minimum; Max = maximum; IQR = interquartile range; Num = number; Obs. = Observations; Rp. = Indonesian Rupiah; LOG = Logarithm transformation; PCE = Per capita expenditure.
Descriptive findings on health indicated that the majority of respondents reported having good health (75%) with 10% reporting excellent health. A total of 4.4% indicated having mild depressive symptoms. Finally, women’s average well-being score was 2.98 (SD = 0.38), suggesting very little variability in the distribution.
Descriptive Results of Health, Well-Being, and Social Capital Variables.
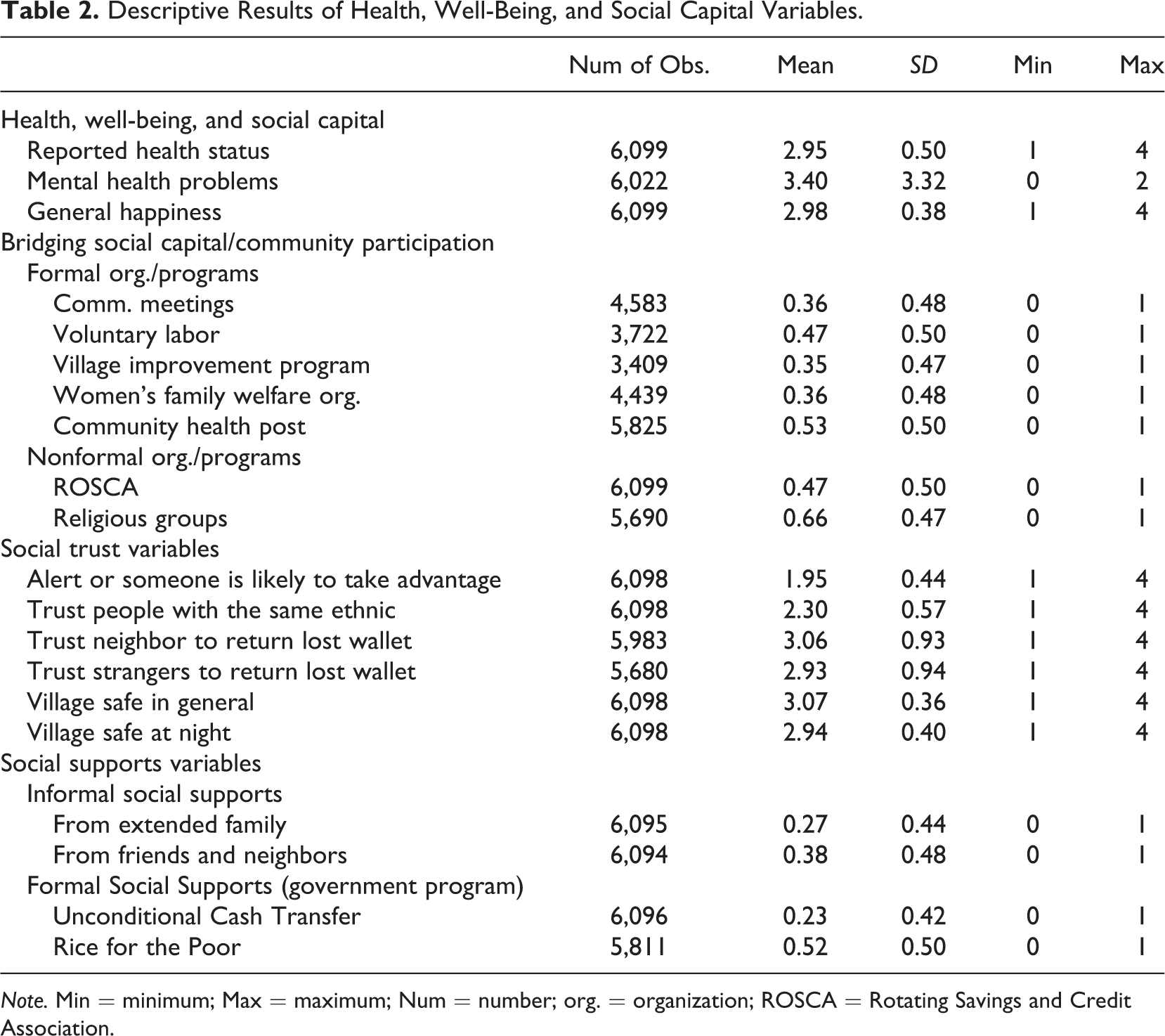
Note. Min = minimum; Max = maximum; Num = number; org. = organization; ROSCA = Rotating Savings and Credit Association.
Determinants of Health, Mental Health, and Well-Being
The following sections report findings of these analyses of how social capital influenced health and well-being, taking into account the effect of demographic factors.
Self-reported health status
Predictors of Health, Mental Health, and Subjective Well-Being (Happiness).
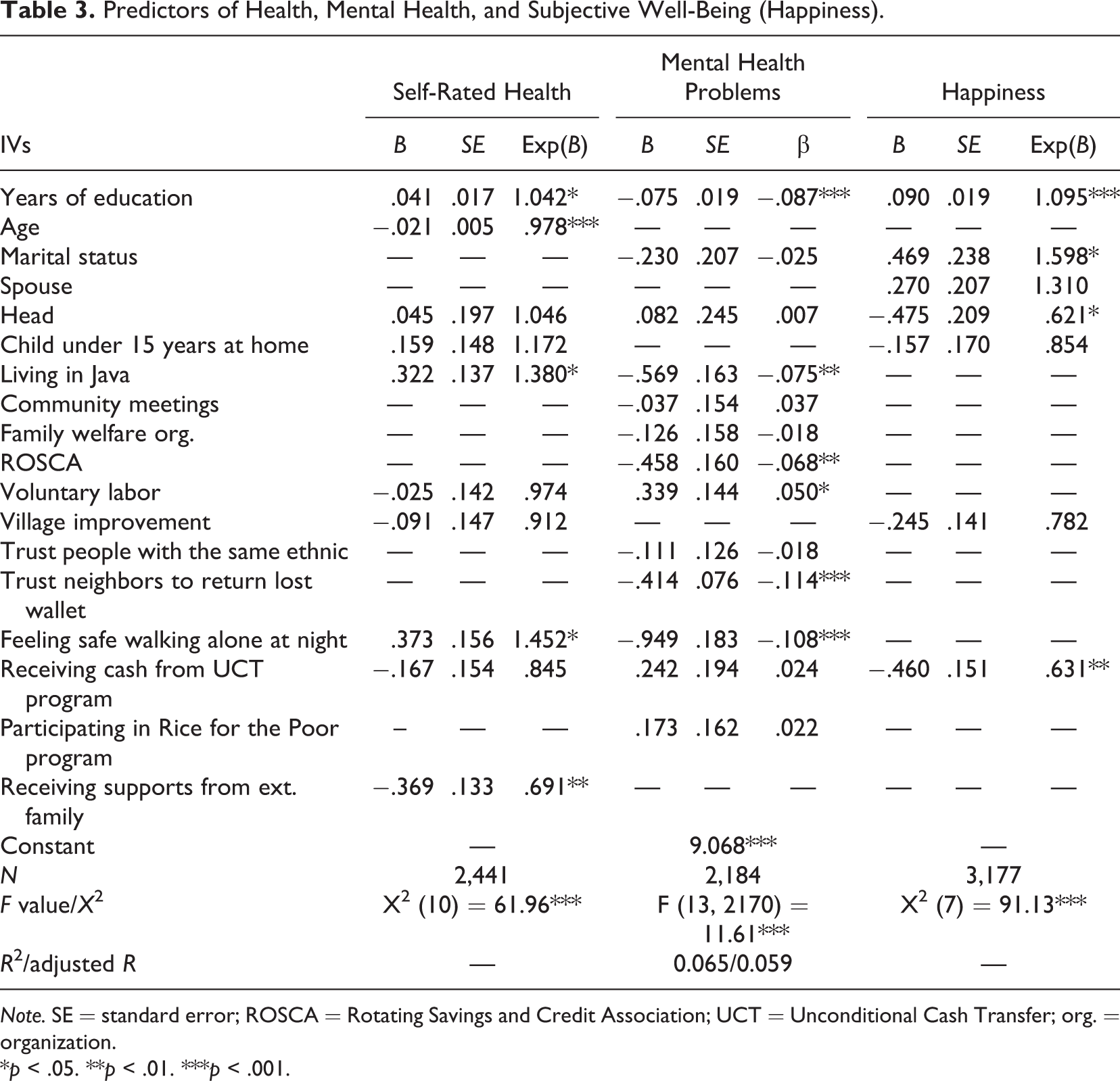
Note. SE = standard error; ROSCA = Rotating Savings and Credit Association; UCT = Unconditional Cash Transfer; org. = organization.
*p < .05. **p < .01. ***p < .001.
Mental health
The regression model predicting occurrence of mental health problems showed that an overall relationship exists, F(13, 2184) = 11.61, p < .001. Additionally, six independent variables had an individual relationship with mental health: education, living in Java, participating in ROSCAs, feeling safe walking alone at night, trust in neighbors to return a lost wallet, and participating in voluntary labor.
The results showed women with more education and who lived in Java experienced fewer mental health problems. Java is home to 5 of Indonesia’s 32 provinces, has lower poverty rates (10.98%), and improved health care access, as compared to the other Indonesian islands (Biro Pusat Statistik, 2014; KAPAL Perempuan, 2013). Three social capital variables, including participating in ROSCAs, trusting neighbors, and feeling safe walking alone at night, corresponded with a decrease in mental health issues (accounted for a 0.46, 0.41, and a 0.95 decrease in mental health issues respectively on a scale of 0–30).
Subjective well-being (happiness)
Using logistic regression, an overall significant relationship was found between the set of independent variables and whether or not respondents were happy, χ2 (7, 3177) = 91.13, p < .001. Four independent variables had a significant individual relationship with subjective well-being: education, marital status, being head of the household, and receiving cash from the UCT program (see Table 3). Having more education and being married positively impacted subjective well-being. The odds of experiencing happiness were 60%, Exp(B) = 1.598, p < .001, higher for married than for nonmarried women.
In conclusion, three aspects of social capital (participating in ROSCAs, trusting neighbors, and feeling safe walking alone at night) corresponded with reduced mental health problems and feeling safe walking alone at night (which reflects trust in the community), was associated with increased odds of good health. No community participation or social trust variables significantly predicted subjective well-being.
Discussion and Implications for Social Work
This study provides valuable information for social workers serving women in Indonesia. First, education emerged as a key variable for improving health and well-being. This finding is particularly notable, as women, individuals in rural regions, and those living in poverty all have lower levels of education (United Nations International Children’s Emergency Fund [UNICEF], n.d.). This also fits with the second finding that living in Java predicted better health than living outside of Java. Java is wealthier and more urban than other parts of Indonesia, with more substantial resources (e.g., health and education). Additionally, women in rural regions, such as outside of Java, may live in more traditional social systems that reinforce their roles in the home as opposed to gaining education and may also experience barriers (e.g., transportation) to accessing valuable resources not available in their home communities. Thus, these two outcomes suggest a need for targeted services that assess barriers and promote access to education, particularly for women and girls outside of Java.
In terms of social capital, trust (in the form of trusting a neighbor to return a wallet and feeling safe walking alone at night in one’s village) and participation in ROSCAs were each linked to better mental health status. Also, safety predicted better physical health (Jen, Sund, Johnston, & Jones, 2010). In more traditional, rural parts of Indonesia, women can be isolated to household work with limited opportunities to build trusting relationships outside the home (IFAD, n.d.). Lack of trust is linked with reduced community participation among women, increased anxiety (Middleton, 1998) and health problems (Hill, Ross, & Angel, 2005). Thus, low trust in neighbors reduces interactions with community members, not only lowering social capital but also further deterring trust-building activities and increasing isolation. In such situations, women may particularly lack a voice and power in the community or access to networks outside the family. Therefore, community-based programs designed for women can serve as a vital resource for increasing engagement and social capital, yielding opportunities to build trust in others (Almedom, 2005; Yip et al., 2007). Through participation and increasing trust, women’s subjective mental health status can improve.
These data are useful for social workers to tailor services in a manner that encourages community engagement, as well as feelings of trust and safety. Designing programs, such as ROSCAs, that allow women the space to not only connect and have a stronger voice but also to develop interdependence can serve women in terms of building greater levels of trust with one another. Additionally, Indonesian women may benefit from working with social workers to identify barriers to participating in such community-based programs, as well solutions to those barriers. Finally, safety emerged as an important dynamic for physical and mental health. Social workers can play a critical role in assessing what factors may either inhibit or contribute to higher feelings of safety in one’s village. Such an assessment can inform social workers of ways to support an important need that ties back to better health status.
Although social capital may have benefits for women and may be a useful resource for social workers to leverage in community-based programs, this discussion would be incomplete without a consideration of concerns expressed by feminist theorists related to social capital. Reliance solely on services to build women’s social capital not only ignores the underlying social structure that promotes inequality for women but also places the responsibility of well-being on women alone. The authors suggest that promoting social capital accumulation is a potential positive step for women but must be accompanied by larger scale advocacy for women’s rights at a social and familial level. Thus, while this article has a limited ability to address the concerns posited by feminist theorists, findings showed that women who were engaged in community organizations and had greater trust in their communities maintained better perceptions of their health status and fewer mental health conditions. With awareness that gender-specific concerns exist related to social capital, it still appears to be a resource that should not be altogether neglected.
Conclusion
Indonesian women experience poverty and gendered power discrepancies, while also living in a social structure that expects more household-confined work of them and often relegates them to informal types of employment with lower pay and without benefits. Not surprisingly, they experience mental health concerns to a greater degree than do Indonesian men. However, specific elements of social capital, including trust and safety within their communities, and participation in community-based programs may help to mitigate effects of the social structure to foster improved mental health status. Social workers can serve a key role in programmatic development and direct practice to aid in creating and linking women with programs that specifically promote trust, safety, and participation. Future research would build on this study well by examining variations in the impact of social capital for women of different ethnic backgrounds and by region. Additionally, future research should examine the detrimental factors related to social capital in order to determine both the pros and cons of programs aimed at using this resource to facilitate improved well-being for women. These findings should be considered with caution, because as noted by Harriss and De Renzio (1997), community-based programs for women may risk too strong of a reliance on social capital and too little responsibility for government and society to address core problems of gender inequality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.