
Abstract
Using a reflective lifeworld and feminist perspective, this study aims to provide a deeper understanding of the temporal existential experiences of women who are living with gynecological cancer. The study was conducted via qualitative interviews of 10 Portuguese cancer survivors, using a phenomenological-hermeneutical approach. A main metaphorical meaning “Outside looking in” was identified. This essential meaning had three constituents: personal experience, biographical disruption, and refiguring the lifeworld. Those who are in contact with survivors in both professional and natural helping venues should give attention to the temporal dimension of cancer survival in order to meet the survivor’s impressions and utterances.
Introduction
Recovering from gynecological cancer can be a difficult experience. Each gynecological cancer experience will be personal and unique in terms of type of cancer, treatment effects, and support as well as the temporal understanding of it and meanings ascribed to it (Lockwood, 2009). As a result, researchers are increasingly considering and investigating the psychosocial issues faced daily by cancer survivors (Aziz, 2007; Beesley et al., 2008; Hodgkinson et al., 2007). Despite ongoing fear and misunderstanding of cancer as a fatal disease, substantial investments in cancer research have resulted in better outcomes for individuals diagnosed with cancer, with significant success in terms of improved survival rates (Hewitt, Greenfield, & Stovall, 2006).
There is a large body of literature suggesting that the presence of social interaction, particularly emotional encouragement and understanding, during times of stress is important in adjustment (Hewitt et al., 2006). In sharing stories, women offer each other mutual support, a forum for exploring issues of the body, psyche, relationships, and community that are relevant to them, and a sense that their knowledge and experience are resources for others. Thus, there is a female ethics of responsibility that emphasizes connectedness and empathy over individual survival (Lockwood, 2009).
Although previous research has identified psychosocial complexity of cancer and illness experiences, few studies have focused on the temporal lived experience of cancer survival. The aim of this article was to understand the temporal ordering of time as experienced by the survivors of trauma related to the diagnoses and treatment of an often fatal disease. The overarching research question that guided the current study was: how do gynecological cancer survivors understand their past, present, and future after cancer diagnosis and treatment?
We invited Portuguese female cancer survivors to talk about their lives (lived experiences) after cancer treatment. Mediterranean traditional values such as importance of family (familismo), respect for others, courage, self-sacrifice, and strong religious faith may deeply influence the ways in which Portuguese female cancer survivors make meaning of their cancer experience.
Given the increasing number of survivors, health professionals are likely to be in contact with women and families impacted by gynecological cancer. As humanistic, developmentally based practitioners, health care workers are well-positioned to listen to the women’s stories (Collie & Long, 2005), help them name their own meanings, and facilitate their healing by co-constructing a new life narrative and developing personal agency. This research was intended to help expand knowledge of survivor needs and thus be able to treat them in a more holistic way.
Background
Cancer Survivorship
Defined as a lifelong, dynamic process, survivorship begins when women have completed medical treatment for gynecological cancer yet live with the memories of their treatment and the possibility of a cancer reoccurrence (Pelusi, 1997). Although survivorship is considered the most important outcome of a gynecological cancer experience, it is understudied and thus the least understood aspect of the disease (Kaiser, 2008). Researching how gynecological cancer survivors actively construct their lives and the meaning of cancer is of particular interest to better understand the process of adjustment following the disease.
Survivorship suggests first and foremost a temporal relation. It looks back to the endurance of a past trauma and forward to a future that is willed into being by overcoming adversity. Cancer survivorship is a statement in the present perfect (of having survived) that speaks to a desire for the future known to be uncertain (when does remission become survival?). To survive is, by way of its etymology, to live above, beyond, or beside something; it refers to a “living longer than” that revises previous expectations of time. The temporality of cancer survivorship is always provisional and contingent, requiring adaptation and improvisation (Berlant, 2011; Bryson & Stacey, 2013). Time becomes newly relational, undoing the neat sequential flow of past, present, and future. Time may seem like air, we cannot see it; nevertheless, it is still a condition of our existence. In everyday life, there is a tendency to overlook basic aspects of our existence such as time. Serious illness changes this attitude. Our time is neither solely the time of the clock, nor of the soul, or the circadian rhythm but also a matter of significant social importance. It has economic value as well as personal value because of an awareness of the limited time in each day and in the human life span (Melucci, 1996).
Reflective Lifeworld: Temporality
An interpretative lifeworld perspective was employed as the theoretical lens for this study into women’s experience of cancer survival. Lifeworld research attempts to explore and understand the entirety of the phenomena of interest, grasping its meaning, analyzing, synthesizing, and then presenting the phenomena and their meaning as faithfully as possible (Dahlberg, Dahlberg, & Nyström, 2008).
Starting with the writings of Husserl, 1 a rich and influential phenomenological tradition exists, in which the lifeworld of human beings takes a central place (Toombs, 2001). Phenomenologically, there are four lifeworld existential elements: lived space—synonymous with spatiality; lived body—synonymous with corporeality; lived time—synonymous with temporality; and finally lived human relations—synonymous with relationality (Van Manen, 1997). This article focuses primarily on the lived time constituent of the lifeworld. Lived time, or temporality, is subjective time as opposed to clock time or objective time. It is a time that appears to speed up when we are enjoying ourselves or slow down when we are bored or anxious. Lived time is our temporal way of being in the world and includes temporal dimensions of past, present, and future that constitute a person’s life.
In this article, we have used Ricoeur’s (1988) interpretation of the context of three time dimensions. How we interpret the present is connected to how we have understood the past but also to how we view the future. To understand a person—in this case, the woman cancer survivor and her situation—the present and the situation in which we find ourselves is connected to the past, where our experiences are. We are also connected to the future that we imagine awaits us (Ricoeur, 1988). Toombs (1990), following Husserl, compared this to listening to a melody: I hear not only the present note that is now sounding but also retain in my present consciousness the previous note and anticipate a future note as the melody unfolds temporally.
Feminist Perspective
Because all illness experiences are mediated by gender, a general feminist stance was taken, with conscious advocacy for the participants, meaning that analysis was purposefully and empathetically directed in the interests of women survivors (Aranda, 2006).
There is no unitary feminist perspective. Rather, literature shows diverse perspectives within feminism including liberal, essentialist, radical, Marxist, socialist, and postmodern feminism. Yet, distinctions among diverse feminist perspectives become blurred in contemporary feminism, which can be summarized by several principles that all feminist perspectives have in common. The principles are as follows: (a) it is important to center and make problematic women’s diverse situations and the institutions and frames that influence those situations; (b) all feminists refer the examination of that problematic theoretical, policy, or action framework in the interest of realizing social justice for women; (c) all feminist theory posits gender as a significant characteristic that interacts with other factors such as race and class to structure relationships between individuals; (d) with the exception of liberal feminism, most feminist theories reject the neutral objective observer for a social construction of scientific research based on the standpoint of the observer, which is influenced by gender, as well as other factors such as race and class; (e) most feminist theories reject dualism; (f) women’s experience is important; (g) the distance between observer and object of study is shortened; and (h) unicausal, hierarchical approaches are rejected (Aranda, 2006).
Overall, the incorporation of feminist principles into a phenomenological approach is valuable because such an approach aids in the recognition of how gender influences temporally experiences of illness and the meanings attributed to them.
Method and Design
To explore how participants experience the temporal dimension of life-threatening disease such a cancer, and how cancer influenced their daily life as survivors, a narrative approach based on Ricoeur’s phenomenological-hermeneutic understanding seemed appropriate. Narratives provide a channel to the internal personal world and reveal personality, identity, and development (Riessman, 2008). As time structure is an explicit aspect of the narrative, this approach is well suited to exploring the temporal dimensions of the informant’s experiences.
Participants
The Research Ethics Committee of the hospital involved reviewed and approved this research project. Informed consent was obtained from the participants after they had received written and oral information. We recruited a purposive sample of research participants from among women who received medical treatments at a hospital located in the middle part of Portugal. The study sample comprised 10 women who were selected based on the records of the oncology care facility of a Portuguese District Hospital (PDH).
Participants were chosen based on the following inclusion criteria: (1) adults able to self-report a cancer diagnosis and self-define survival; 2 (2) complete recovery from gynecological cancer (uterine, cervical, and ovarian cancer); (3) treatment for cancer completed for at least 6 months; (4) received follow-up outpatient care well at hospital; (5) a physical and mental condition that made interviewing possible. A potential participant was excluded if she was (1) receiving active medical treatment; (2) experiencing problems such as recurrence or metastatic disease; or (3) unwilling to share her personal story.
The 10 women were aged between 33 and 70 (mean 55 years) and their life situations varied. Most were married or lived in a relationship similar to marriage. They were diagnosed with various gynecological cancers in different stages. Four survivors had cervical cancer, four had endometrial cancer, and two had ovarian/fallopian tube cancer. The participants were Portuguese, came from the same community, and had a homogeneous cultural background.
Data Collection
The data used in the study were part of a larger qualitative project that explored the lived experiences of Portuguese gynecological cancer survivors. The women were first contacted by telephone, and the interviews were carried out in the informants’ private homes. Interviews took place between December 2011 and July 2012 and were tape-recorded and transcribed verbatim. The number of informants was not determined beforehand. Instead, data collection was concluded when the researchers determined the material was sufficient in its richness and variations of meanings, which is of greater importance to the quality and validity of qualitative results than the number of interviews (Dahlberg et al., 2008).
During the interviews, phenomena [the temporal lived experience of cancer survival] were explored from past, present, and future perspectives, allowing the researcher access to a range of temporal perceptions and memories (Ellis & Bochner, 2000). The participants’ attention was directed to (a) the phenomenon of cancer survival as it appeared in everyday life and (b) the meanings survivors ascribed to their lived time experience of cancer survival, as “areas of interest.” They were encouraged to describe these areas as experienced and incorporated into their respective everyday lives following the cancer. Some participants expressed their satisfaction at having the opportunity to relate their “whole story.” The interviews were carried out in Portuguese and later translated into English. They lasted 60 to 90 min, and the richness of the narratives reflected the complexity and uniqueness of the phenomenon.
Phenomenological interviews require an attitude that allows for the complexity and uniqueness of the informants’ lived experiences to be expressed. Such interviews also require the researcher to question his or her own prior understanding, to avoid assuming or presupposing something that was not expressed by the informants. The first author (C.L.), a nurse with 9 years of clinical nursing experience, conducted all interviews. All the authors have several years of experience as health researchers.
Data Analysis
We used QSR International’s (2008) NVIVO 8 computer software to organize, store, compare, and analyze the data obtained in the interviews. According to Ricoeur (1991), personal stories are not empirical data about reality; neither are they uninhibited fictitious statements. The stories bring real meaning to life and provide the potential to show empathy toward others. Through analysis and interpretation of the stories, it is possible to generate totality and bring about an understanding that exceeds the actual story. The analysis in this study was based on Ricoeur’s (2008) theory of interpretation, emphasizing the analysis of texts as a movement between understanding and explanation, a hermeneutic arch to bring forth a broader comprehensive understanding (Lindseth & Norberg, 2004).
Results
In this article, we examine temporality in participants’ accounts of illness. Through the focus on how the participant’s lives developed, the data presented a temporal structure. In the narratives, the women survivors explored their cancer problems by looking back to earlier events for answers to ground the present experience and forward toward future expectations, with awareness and understanding. Specifically, we seek to contextualize their illness experiences by identifying the disjuncture between illness and how they envisioned their current position in the life course, as well as their expectations for the future. Three themes were allocated to this lifeworld structure: personal experience (cancer legacy), biographical disruption, and refiguring the lifeworld.
Theme 1: Personal Experience (Cancer Legacy)
The first theme that emerged is that of the cancer legacy—a legacy characterized by a reconciliation of suffering and despair with personal growth and transformation. This theme is about ascribing meaning to life events that seem incomprehensible and beyond one’s control.
This theme may be described as one that encompasses an intense personal awareness of the finitude of life, a gratitude, empathy, and connectedness to others. In the excerpts following, participants relate the legacy of the cancer journey as one that has brought new values, self-understanding, strength, and a strong awareness of the sensitivities and plights of others who inhabit their social reality. The cancer journey is one of discovering the fragility of life and the importance of loved ones. The finitude of life cannot be ignored. A time without a future becomes possible.
For some participants, experiences from childhood adversity and positive parental role modeling provided a present connection that was supportive and enhanced the experience of survival; additionally there was an opportunity for learning and healing. One woman (P5) recalled survival lessons gained in younger life: When I was 16 years old, that time [political oppression], I worked in the countryside, hard work…little bit of food, and at night time, we didn’t have electricity. I used oil light…Difficult times …
P8 drew inspiration from her father for the strength and courage to face her gynecological cancer: I always think that’s life (referring to cancer), I don’t know, maybe it’s from my father. My father took everything so easily. Women internalized the lessons learned from their past lived experiences, observations of their parents to support their internalized psychological mind-set. As long as they remained positive and strong, they would more likely be shielded against premature death. From a feminist perspective, women often feel a social duty to hide signs of illness, repress feelings of anger or grief, and embrace an optimistic attitude (Broom, 2001).
Furthermore, family of origin was often the site of genetic and lived experience of cancer. Many participants had the experience of losing a family member to cancer, and several had knowledge of genetic predisposition. This shared hereditary/ancestral cancer experience had the capacity to affect past, present, and future generations.
P2 spoke about his sister as a cancer survivor and the death of her mother from cancer, although neither situation appeared to negatively influence her outlook. “My sister has had two different cancers…my mother died of breast cancer [crying softly] I think when you hear that someone in your family whom you love has cancer, it makes you change forever. Obviously even though she (sister) knows [strong intonation] that I loved her, when I say it, it is nice to hear it from someone that you love.”
P4 also experienced the death of an aunt with breast cancer and her brother was living with prostate cancer, yet these experiences did not negatively influence her attitude or outlook. “I don’t think about it, I have the cancer yes, but what can I do, it is there. I am having treatment for it. I don’t know, I think that is the best way to look at it, what can you do? You cannot brood and worry and worry, it won’t help.”
There is a greater likelihood that past events and memories, both positive and negative, could influence a cancer experience. In the past, cancer and death from cancer were not discussed by the medical profession or in society as openly as today. Therefore, the women who witnessed a cancer experience many years ago could be more likely misinformed. They may have experienced death of family members from cancer, yet overwhelmingly they maintained positive outlooks during their own experiences.
The cancer legacy, the gift of the illness, is a movement that alters how women come to view themselves, others, and the finitude of life. This theme refers fundamentally, as Levinas (1981) would have suggested, to the very visibility of others. The legacy of the illness is finding meaning in the very realization that, while their parents’ lives have been spared, others are mourning. The gift of illness is about invoking the faces of all others “in their infinite alterity” (Derrida, 2001, p. 11) for whom escaping despair and suffering is not possible. The cancer legacy is the ability to see the face of the “other.” Overall, past family of origin issues appeared significant to the way participants constructed their present survival experience in terms of a temporal connection to their past self. “We learn from the other” (Waldenfels, 2002, p. 68). This is the lived experience of time in relations with the other, writes Levinas (1987, p. 39) “Time is not the achievement of an isolated and lone subject, but that it is the very relationship of the subject with the Other.”
Theme 2: Biographical Disruption
In this theme, we describe the various ways that participants experienced cancer as disruptive to their identities as women or their expectations for this time of life. We have divided this theme into two subthemes that are feeling “off time” and realizing mortality. As a whole, this theme highlights how participants experienced illness with respect to their position in the life course and how illness was felt to be inconsistent with other aspects of their lives. While many of the women faced issues that have been identified in the existing literature on illness experiences, we seek to demonstrate that participants also experienced and made sense of illness in unique ways because of their life stage.
Feeling “Off Time”
The threat that illness posed to “normality” was evident in the stories of several of the women, who recognized that being ill made them different from many of their peers. Specifically, illness introduced limitations or setbacks into their lives that led them to be different from their peers. In addition, illness was perceived by many of the participants as throwing them “off time” with respect to their life course trajectory, demonstrating their awareness of common characteristics associated with adulthood. Thus, illness resulted in experiences that were viewed as being typical of individuals older than themselves, as well as younger than themselves on occasion. Further, some of the women described being unable to relate to others affected by the same illness because of the different timing of illness in the life course. The examples that we highlight with respect to this subtheme contribute to the notion that illness was disruptive to the women’s perceived position in the life course.
First, several comments were made by participants with respect to their feelings of abnormality and the desire to be like other people of their age. For example, P2 and P4 referred to feelings of oddity, commenting, respectively: It’s like ‘Okay! I just kind of want to be normal for once.’ And Why couldn’t I be normal? I really went into shock, like this cannot be happening to me, this happens to other people. After diagnosis, my life as a large wave rolling in, after that other [waves] problems appeared…It was a huge tsunami, I have to deal with so many things.
P4 used a wave allegory (ecological metaphor) to illuminate her experience of living with cancer. The cancer diagnosis can be described as a large wave rolling in, hitting women as a shock, leaving them feeling uncertain about the future. Initially, getting cancer was experienced as an existential threat; a threat to life itself—and to their being in the world. After the first shock, the waters calmed down and gave them time for reflection. Then new waves appeared and in different ways stirred up the water again, for example, treatment side effects, problems with sexuality, a new awareness of the physical body, a feeling of being left alone, practical, and physical obstacles to living “normally,” distress in the marital relationship, and encounters with friends and health care providers (Hodgkinson et al., 2007). These new experiences, and the manner of relating to them, must be understood in light of the individual and the first large frightening cancer wave.
On the other hand, some participants experienced their diagnoses as “off time,” because of the other events happening at the time and perceptions that the illness affecting them was typical of older individuals. For example, P3 experienced her initial diagnosis of cervical cancer at age 47 as unexpected and highly disruptive to her promising career.
Similarly, P4 experienced her diagnosis as highly disruptive to her role as a wife and mother of two children. Several other participants also talked about the disruption caused by illness to educational and employment aspirations. These examples demonstrate how the timing of illness was perceived as inconsistent with their other social roles and contributed to the belief that it was “off time,” even though many women [their age] are affected by serious illness like cancer.
In addition, the side effects of treatment caused some women to feel as if their body was going through things more common to older women. Primarily, both P4 and P9 experienced menopausal symptoms due to their gynecological cancer treatment. P4 summed up her feelings regarding this experience: It’s like living in my mother’s body because suddenly you’ve got, um, you know, hot flashes, um, you know, more peach fuzz on your face, like just, you know, the things that happen to an older woman but they’re happening to you at the wrong time.
P4 emphasized how she viewed this experience with respect to her position in the life course, as she perceived menopause to be an experience more consistent with someone of her mother’s age than her own.
P9 expressed a similar sentiment regarding the possibility of chemically induced menopause as a treatment for endometriosis. She sarcastically exclaimed: It’s like ‘Whoa! Okay, yeah, menopause in my 40s. Cool, like, that’s awesome.’ In saying this, P9 also highlighted the view that menopause was inconsistent with the typical bodily experiences of adulthood. These comments regarding the possibility of entering menopause during this life stage highlight an important issue: The physical implications of serious illness can contribute to an inconsistency between how people feel and their perceived position in the life course. In particular, this inconsistency emerges because the physical experience of illness is typically unknown to others of their age (Lee, 2001).
P5 and P7 felt that they could no longer enjoy a night out with their friends in the same way as they had in the past because of fatigue and/or mobility issues. P7 communicated how this restriction led her to feel different from others of her age: Even if I did want to go out to the bar, I know that I wouldn’t stay very long because I’d feel sick and it’s just, it’s exhausting for me…I just feel a little bit left out sometimes. As a result, P7 experienced her illness as disruptive to her social life and ability to be like other people.
P2 also articulated how having gynecological cancer during her 30s had put her “off time” by talking about her and her husband in comparison to other couples. Stating that she sometimes feels left behind, the comments of P2 provide evidence of how being ill has shifted her and her husband off a perceived normal life course trajectory. Specifically, she noted that not having children made them different than other couples of their age, as well as unique to other couples going through a cancer experience who are typically older and may already have children and/or grandchildren.
Here, she acknowledged that older individuals who are facing a life-threatening illness such as cancer are in a different position than younger individuals who have yet to fulfill many developmental tasks and goals for their lives, such as raising a family. Further, P2 emphasized her belief that it is unjust to be facing the possibility of a shortened life course because she has several goals that she would like to accomplish.
The previous paragraphs highlight participants’ experiences of feeling different in comparison to others. Their stories suggest that illness caused the majority of women to feel “off time” with respect to their perceived position in the life course. Being ill during adulthood led participants to feel either younger or older than other individuals affected by illness, as well as different from their peers. Such a sentiment is also evident in existing research on adults with serious illnesses who report being overwhelmed by the time-consuming nature of illness (Badlan, 2006) or feeling misunderstood by others of their age who do not have concerns of such magnitude (Odo & Potter, 2009). This subtheme highlights issues related to the social construction of the life course and how sociocultural expectations can be problematic for adults experiencing serious illness.
Realizing Mortality
The experience of a life-threatening illness raised significant questions related to mortality and longevity for some of the participants. Specifically, realizations of mortality resulting from illness often introduced anxiety and threatened some participant’s expectations for the future. In addition, these participants considered how the possibility of dying from illness would affect their loved ones. Underlying participants’ comments are sociocultural ideals associated with health and illness, the life course, and death. In acknowledging such social constructions, the women’s stories expose the struggle they face because of the possibility of dying from illness and, further, dying an “abnormal” death, as most people in industrialized societies have expectations of growing old (Kellehear, 2007).
Primarily, some participants recognized the life-threatening nature of the illness by which they were affected. At this moment, P10 feels harshly confronted with death. The breaking point in the story is P10’s insight into her own mortality: “In this period I somehow reached the conclusion that there is nothing worse that could happen than that I could die.”
P8 described a similar awareness of the possibility of death when talking about a friend who had died from leukemia. She said as follows: [People with leukemia] have a constant reminder that we can die, sooner or later, so, [this woman] was a good friend. I met her [in Coimbra, Portugal]. She was treated for leukemia and she died just in October and I just learned this in January…it reminds me that death is always possible and is always [hanging over] my head.
P8 highlighted her realization that she could also die from her illness as her friend recently had. The comments of P8 call attention to the heightened awareness of mortality that results from a cancer diagnosis, as her well-being and future are constantly in question. Existing research on individuals with cancer has also identified the increased awareness of mortality that results from such an experience that requires the ongoing negotiation of uncertainty (Mckenzie & Crouch, 2004).
Despite her acute awareness of the uncertain future that she faced, P8 suggested that optimism was the most significant way for her to cope with the heightened possibility of death. Thus, her comments reflect social discourse that suggests that optimism and good humor are central to the appropriate management of cancer and ill health more generally (Mckenzie & Crouch, 2004; Werner, Isaksen, & Malterud, 2004).
P5 and P1 also discussed the confrontation of their mortality that resulted from illness. For example, P5 considered the possibility that death could result from her cancer, which motivated her to pursue further medical testing to ensure that she was cancer-free. Furthermore, recognizing the life-threatening nature of cancer, P5 indicated that she spends more time with her children and focuses on enjoying life. Thus, the illness experience prompted some of the women to develop a different perspective toward their lives and the people in them, a transformation that resonates with what has been reported in existing literature on illness experiences (Kleinman, 1988).
Although positive growth could result from the realization of mortality, this occurrence led some participants to experience “biographical disruption” because it required the adjustment of how they envisioned their future. In particular, P2 and P9 recognized that their lives could potentially be shorter than they had previously expected. P9 captured this experience by commenting that: You think ‘When I am 70…but maybe I won’t be 70 at all’…That’s difficult because you don’t know, your life- is it long or short? It’s very uncertain.
Here, P9 highlighted the uncertainty of her future and the recognition that her illness might cut her life shorter than expected. In doing so, P9 demonstrated how she has had to reexamine her expectations for the life course as a result of illness and the realization of her mortality. Additionally, she has had to reconstruct her identity to account for the possibility that her life may not follow the typical, albeit socially constructed, life course in which individuals in industrialized societies live into their 60s, 70s, 80s, and even 90s.
Similar to P9, P2 discussed how having cancer has led her to realize the possibility that her life course may not be as long as she previously thought. She stated [showed a photograph of her matrimonial]: What going through the cancer journey has done is forced me to confront some of those things or to say to myself, you know…A part of what’s in this photo is the store that we purchased which was one of the scariest things I have ever done, and I’ve been having anxiety attacks ever since, um, but it’s been good. Thus, P2 also experienced the realization of her mortality as a need to revise how she envisioned her life course. In addition, she suggested that the potential for a shortened life meant that there was a greater urgency for her to realize her goals and dreams, a sentiment that was echoed by P9. Thus, the realization of mortality led these participants to reflect on how they spent their time, focusing on quality of life as often occurs with individuals affected by cancer (Rasmussen & Elverdam, 2007).
The previous quotations demonstrate participants’ cognizance of the threat that illness posed or continues to pose to their well-being and longevity. Additionally, their comments show the potential for their lives to be pushed off a perceived “normal” life course because of illness and the possibility of dying earlier than expected. Thus, the realization of mortality was experienced as a threat to the fulfillment of their envisioned life course, as well as an existential threat.
While some participants spoke of the realization of mortality in relation to their well-being and imagined future, a few also discussed their mortality in respect to the significant impact that their possible death could have on loved ones. For example, P5 focused on the emotional burden that her ill health placed on her parents. Her comments broach the idea that death is thought to normally occur at a specific time in life (old age) and that death is “premature” when children die before their parents (Exley & Letherby, 2001).
Additionally, P10 expressed concern for her husband in the event that she succumbed to cancer, highlighting her fear that her death would bring about great emotional difficulty for her husband. Thus, some of the women frequently viewed illness in respect to its relational impact, in addition to, or instead of, recognizing the threat that illness posed to their personal well-being. Focus on the relational impact of illness may be common for women affected by illness because of the portrayal of women as caregivers in Western discourses of feminism (Lafrance & Stoppard, 2006). As a whole, this subtheme highlights how illness prompted many of the women to realize their mortality and the fragility of life. Thus, this subtheme provides a basis for the following examination of how participants renegotiated their expectations for the future in light of illness.
Theme 3: Refiguring the Lifeworld
Recent research has suggested that female cancer survivors tend to fluctuate between being focused on their loss and being in a future-oriented state (Hodgkinson et al., 2007). The women in our study described this struggle between the present (inflected by the past) and the future (with new possibilities), from a position where they are able to look back and reflect on experiences. All women believed that their illness trajectory had made them stronger and that they had gained new strength to face the challenges of life.
P1 explained: “Generally, more will have to happen before I will be shocked […] I have survived, now I just can’t imagine what could happen that will get me down […].” P1 is now facing the lifeworld from a different and more self-assured platform. Although each participant had unique and different ways of seeking meaning, with time, they all found meaning through confronting and then embracing life’s basic conditions.
We understood this process by drawing on Ricoeur’s (1988, 1991, 2008) work on narrative, particularly his notion of “narrative refiguration.” Ricoeur describes a fundamental human need to reconfigure the episodes of our lives together into a coherent narrative. It is through this narrative that we construct our identities. This narrative is, in part, the product of a human attempt to reconcile the irreconcilable, to bridge the gap between the vast, essentially infinite, quality of cosmic time and the limited, finite, nature of phenomenological time (time as lived). The human desire to leave traces on the cosmos results in the production of histories, both sociocultural (through the array of stories that we are thrown into) and personal, as we attempt to make meaning out of often seemingly disparate and conflicting moments in our lives. A crisis, such as the losses or potential losses resulting from the illness experience, ruptures any sense of narrative continuity. This rupture of continuity was clearly experienced by the participants. Following the rupture, the future as planned is no longer possible and there is a danger of becoming stuck in only present and past concerns. However, these women did find ways of moving beyond such quagmire, not by forgetting or by “moving-on” but instead by finding ways to integrate their loss into their life stories. Although this is not an easy task, it was clearly an essential one as it once again opens up future possibilities within the consciousness.
Given the duration of illness that P2 experience when we interviewed her, she was able to most articulately communicate the disruptions to her expectations for adulthood that illness had brought about. P2 captured the rupture between what she expected her 30s to be like and what they had turned out to be by saying: I feel like [my husband and I have] fallen behind, and maybe that’s ridiculous, but when I entered my 30s I remember sort of what my unwritten list of goals were, you know, by the time I’m 40 these are the things that I’m hoping we’ve accomplished, you know ‘I wanna have the mortgage paid off, we will have kids…’
She explained how she and her husband had failed to accomplish some of the things that couples often do in their 30s because they had put life on pause for her illness. Her comments highlight her awareness of the life events typically associated with young adulthood, such as establishing a career, gaining financial stability, having children, and setting up a home. As mentioned previously, P2 experienced her diagnosis as particularly disruptive to her career. P4 also discussed many of the same issues, noting that her cancer diagnosis led to setbacks in the obtainment of a full-time job and buying a home with her partner, which had financial ramifications. Thus, P2 and P4 continued to negotiate their current situations with respect to their expectations for this time in their lives.
One expectation that some participants talked about at length was having children. Describing her 30s, P2 recalled: There’s this big gap in which I’ve learned a lot and grown a lot and met a ton of people, but have not done some of the things that people normally do in their 30s and, at this point, we may never because of [the cancer], um, and one of the most important parts of that is planning a family, which you can’t do while you are going through this process because your body won’t do it, when it’s so full of chemicals that you couldn’t responsibly do that and you can’t come off the medications until a certain time frame when they’re hoping that you’ll be okay.
P2 comments highlight how her expectations were threatened by the possibility that their ability to have children was compromised by illness or its treatment. Other participants, including P4 and P9, also shared similar thoughts regarding possible complications imposed by illness with respect to fertility and pregnancy. Thus, illness greatly threatened their assumption of the motherhood role, a role that is closely tied to femininity (Exley & Letherby, 2001). Women perceive fertility as pivotal to being female and the inability to have children indicates that they are old before their time and less attractive (Walton, Reeve, Brown, & Farquhar, 2010). While concerns about fertility and pregnancy with respect to illness have been well documented in women affected by cancer (Odo & Potter, 2009), further research is needed to ascertain the extent to which women affected by other types of serious illness experience this set of issues.
Participants also talked about their education and employment goals and how being ill had affected them. In some cases, illness forced participants to take time off from university or hindered their ability to secure desired employment as was the case for P3 and P4, respectively.
P3 indicated how she had somewhat relaxed her expectations for herself since becoming ill: It’s just a matter of making adjustments, um, you know? At first I thought ‘Oh maybe I’ll do a nursing degree.’ and then I realized that I don’t need to push myself, or force myself into getting those grades that I know would be achievable if I wasn’t sick. But I can only do what I can do right now and I don’t want to put my life on hold any longer…however I want to conclude my degree. This quotation demonstrates the tension between prior expectations of P3 and her revised outlook due to illness; specifically, P3 continued to have hope for the achievement of her goals and dreams but also put less pressure on herself. Charmaz (1991, p. 21) reported such an occurrence as common among the chronically ill, finding that “illness and disability force lower expectations of self—at least for a while.” However, despite confronting the likelihood that certain goals may go unachieved, P3 and P4 continued to strive for certain goals or achieve them in partial ways. Thus, having to take time off from university or trying to negotiate academic or work responsibilities while being ill may pose problems for women and necessitate that they renegotiate expectations for this life stage.
Finally, while many of the changes that participants talked about with respect to their expectations were relatively negative, a few participants discussed new expectations for the future in positive terms. P7, for instance, described feeling a greater purpose in life following her recovery from depression. Specifically, she indicated that she may pursue education and employment related to alternative therapies. P3 had also initiated a new career path since her cancer diagnosis. While she had considered entering the nursing profession previously, she believed that experiencing cancer affirmed her decision to pursue a nursing degree and endowed her with invaluable life experience that could help her to empathize with patients. Thus, these participants’ experiences demonstrate the transformative aspect of illness for some individuals (Kleinman, 1988). This theme illustrates how many participants’ past visions of their future were threatened by illness, forcing them to renegotiate their expectations, and acknowledge that previously held dreams may be delayed or go unfulfilled.
All the participants spoke of having learned a number of things as a result of their experience of loss. This has resulted in them having greater strength and appreciation for life itself. They express great appreciation for close family and believe that people need to learn to live their lives to the fullest. They are less focused on the minutiae of life and the loss has strengthened their relationships with significant others. These women are better able to prioritize what is important to them based on their own values and not on societal expectations. Finally, they described how the loss has resulted in increased self-awareness, a more positive attitude, strength, and gratitude. In general, the participants stated that they have become more inclusive, tolerant, caring, sensitive, outgoing, and generous to others. These accounts support Tedeschi and Calhoun’s (2004) findings regarding posttraumatic growth. The way in which the participants have dealt with their losses also testifies to the strength of these women as they have been able to face the adversities of life, regardless of their difficulty, with the courage to be.
Knowing the Time (Existential: Lived Time)
Conceptually integrating the synthesized themes, a main metaphorical theme was identified addressing the interdependency between past, present, and future for cancer survival. Outside looking in is a symbolic representation of the temporal essence of the female cancer survivors’ lived experiences and of their being throughout their lives up to the time of the study. The overarching theme personifies a process of self-discovery through resolute looking inward. Outside looking in captures their lives as being temporal, active (participatory), and dynamic (changing) in the contexts of the past, present, and the future. Interpretation of the cancer survivor’s philosophical and practical perspective of life is revealed through the structure of meaning (see Figure 1), wherein the enveloping circle, with a continuous line, represents the external environment, a bounded system that indiscriminately influenced the cancer survivors. Their past, present (at the time of the study), and the future worlds are superimposed on the external environment. These worlds are encircled with broken lines symbolizing the dynamic evolution that occurred within these worlds. The broken line acknowledges that influence from societal values, beliefs, and prejudices might have had direct or indirect influence on the cancer survivors and their worlds. The circle representing the cancer survivors’ (then) present world is larger than circles representing the past and future worlds, because this world was most meaningful. Thus, the emergent themes are represented within this context. The smaller circles within the worlds of past, present, and future represent a transformational phenomenon that occurred between the women and their respective narrative.
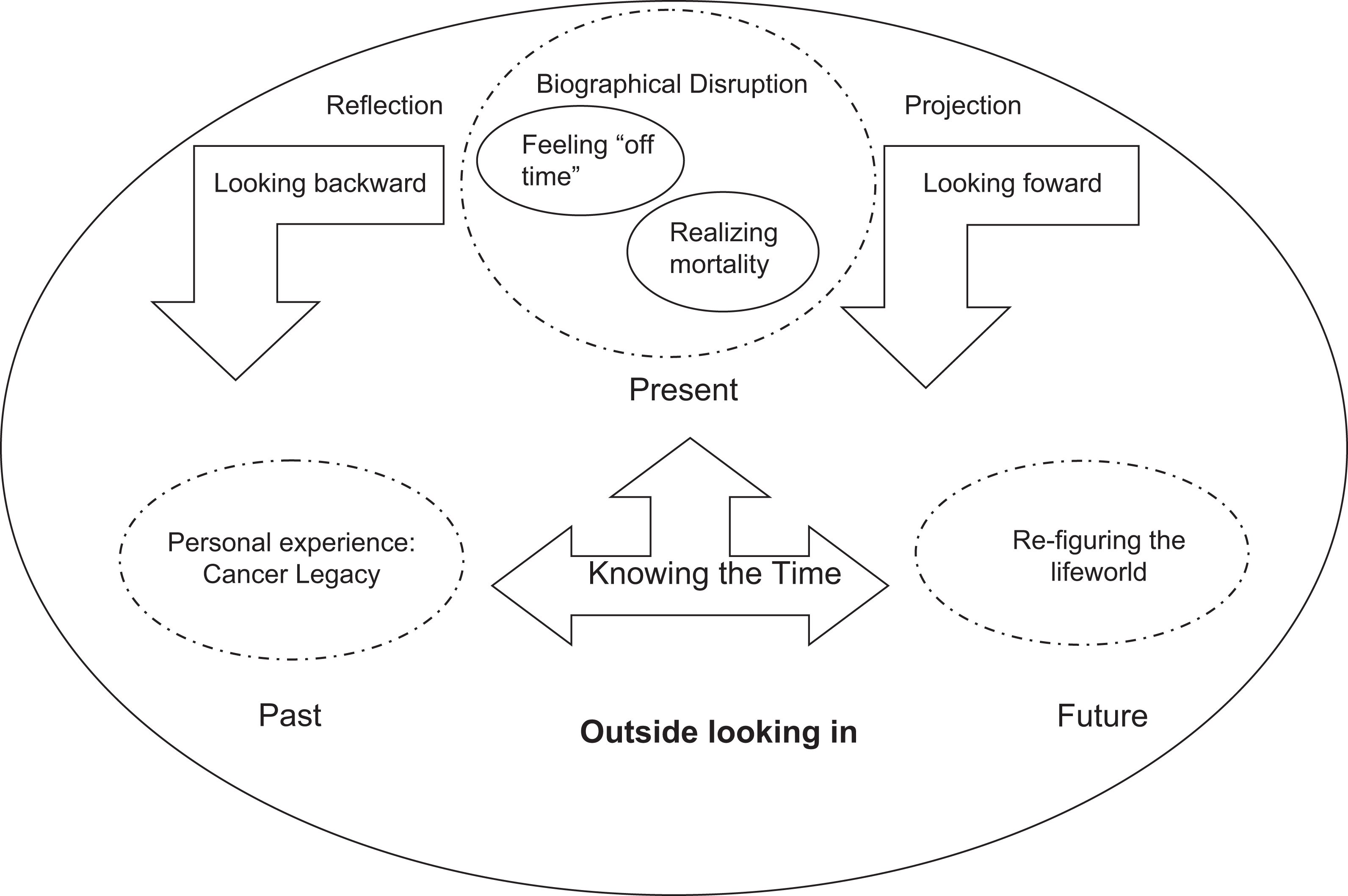
“Outside looking in” as a visual representation of the cancer survivor’s lived time experience.
Discussion
When a life-threatening disease is diagnosed, patients find their sense of time altered, for example, the passage of days or view of the future (Murray, 2000; Rasmussen & Elverdam, 2007; Toombs, 1990). Confrontation with death may result in a loss of the future, making the individual more conscious of the importance of living in and for the present moment. Therefore, time takes on another meaning, redefined as temporality. The experience of time is divided into the period before or after the diagnoses or into periods before the health problems occurred and finally the period when the individual has learned how to deal with everyday life situations. This can be reformulated as negotiating time, reflecting insufficient time and rationalizing time (Rasmussen & Elverdam, 2007).
Our participants communicated feelings of difference from others as a result of illness and the limitations that it imposed. Such feelings are similar to those reported by adult cancer survivors, for whom the illness experience magnified the sense of difference and isolation that they felt from their peers (Lee, 2001; Odo & Potter, 2009). Such feelings are significant in that they can contribute to a sense of alienation from others and “the breakdown of a commonly shared reality” (Good, 1994, p. 125). As such, feeling abnormal because of illness threatens one’s sense of belonging and comfort in social interactions, which may hinder seeking support and psychosocial adjustment to illness. Thus, feeling abnormal can lead women to view themselves as having departed from “normal development,” which may contribute to frustration, self-esteem, and/or identity issues; relationship troubles; and difficulty making sense of illness (Lee, 2001; Odo & Potter, 2009).
Additionally, participants talked at various times about how illness hindered their ability to fulfill goals that are common to this life stage, including those related to social life, education, employment, and family. As such, participants’ experiences of feeling “off time” due to illness demonstrate their awareness of such characterizations of illness and the life course and the influence of these characterizations on how illness was experienced and understood. Therefore, many participants experienced feelings of oddity as a result of becoming ill during adulthood because it threatened their ability to feel and behave in the way that is typical of this life stage.
We describe some of the participants’ realizations of mortality that resulted from the illness experience. In addition to bringing about the recognition that illness threatened their existence, some of the women spoke of the threat that illness posed to their envisioned life course. Several participants acknowledged that illness could cause the life course to deviate from the expected and “typical” duration. Thus, some of the women recognized that a shorter life meant less time to accomplish their goals and aspirations. As a result, these participants came to view their lives differently, feeling a greater sense of urgency to achieve their goals and enjoy life.
Recognizing that their lives would be forever changed because of serious illness, women were involved in a process of renegotiating their expectations for the future. Disruptions in everyday life and short-term plans as a result of illness contributed to further disruptions in long-term plans or setbacks in the achievement of certain tasks or aspirations. As such, many of the participants were required to revise how they envisioned the future. However, this renegotiation of expectations was problematic because it involved trying to come to terms with uncertainty and losses or potential losses resulting from the illness experience.
Study Limitations
Our sample was limited to a small group of Portuguese women, who were relatively homogeneous with regard to socioeconomic status and was limited geographically. Also, as this was a qualitative study with a focus on individuals’ lived experiences, caution should be exercised in assuming the transferability of the findings to other groups or contexts. Thus, future research in this area should focus on women from more diverse backgrounds in order to determine similarities and differences across socioeconomic and ethnic backgrounds. This study was a retrospective study that invited the women to recall their experience throughout the survivorship. Thus, it was limited by researching after meaning or recall bias that is inherent in retrospective research study. In the future, longitudinal studies with long-term follow-up of the survivors from the diagnosis of the disease are recommended in order to understand how Portuguese women experience cancer over time and to verify the findings of this study. It is likely that the journeys of these survivors were still too recent for some of the cognitive reappraisals and meaning-making to be as pertinent as they might be later (Tedeschi & Calhoun, 2004). Since change can be a slow process, it would be helpful to reinterview these participants further along the survivorship trajectory. Survivorship also impacts the woman’s life partner, and research into the relational aspects and partner responses and needs would be beneficial.
Relevance to Clinical and Social Practice
Time is of crucial importance within survival care. Currently, the health worker is heavily influenced by clock time and conducted at a rapid pace, with emphasis on a hectic turnover or throughput of patients and ever increasing pressure to discharge early (Becker, 2010). The contradiction between the patient in need of a flexible rhythm, giving clock time little value, and a health care system dominated by a fixed clock time, is challenging both for patients and health workers. However, it is important to be aware that norms and values in a society are man-made and changeable. The health worker should seek to facilitate care not by looking at the clock but by observing and complying with a starting point in the women’s desire to transcend the sociocultural demands of the everyday world (Jones, 2010). Through this process of transcending, participants were constructing, and reconstructing, meaning of the cancer survival experience within the context of their temporal lived experience. While setting aside heretofore clinical and societal norms and not withstanding ordinary constraints within one’s work world, health care workers, nevertheless, have an obligation to enter into the lived world of the person through dialogue. It is only then that we can truly develop and deliver the essences of patient-centered care in a way that is visible, valued, and respected. True intimacy bridges the relationship, each emerging from the relationship forever transformed by the other through personal commitment and sharing. Adopting a flexible rhythm in care can provide an opportunity for the woman to open up, release energy, or share an important story saturated with meaning. In such situations, life is confirmed and women may experience being given more time and being seen by the heart. In turn, the health care worker intuitively utilizes this lived information, which is a fundamental shift in oncology practice, by providing what is needed, based upon each theme identified in this study.
We consider this research to be new and important knowledge because it emphasizes the need to understand women cancer survivors’ experiences on an emotional level as well as on a temporal level and highlights how these experiences are gendered. Being gendered as women informs the experiences of gynecological cancer patients to a great degree, and it is vital that we take gender seriously when developing better treatment policies and advocating for social transformation.
As the psychosocial adjustment of elderly survivors of cancer is an underresearched area in Portugal, there is a need to investigate the experience of illness trajectory in this group of clients, so that their physical and psychosocial needs in survivorship can be better met.
Implications for community development workers include supporting cancer survivors to understand the pedagogy of survival. That is, the survival lessons of suffering and compassion could be used as a mutually beneficial skill for community work. Group work facilitation of cancer support groups may benefit from understanding the temporal complexity of survival. Supporting the women to speak out about their experiences and feel acknowledged and validated for the meaningful contributions was congruent with feminist epistemological processes. Peer support offered by similar others in a group setting or through the telephone or Internet may help to lessen women’s feelings of abnormality and isolation that can result from the illness experience.
Conclusion
Cancer is a complex, dynamic illness, impacting the individual in a multitude of ways. Participants have eloquently explored the illness experience, with expressivity laden with personal meanings of self-importance. The findings from this study provided invaluable insights to aid oncology health workers and other psychosocial providers to assess these women’s needs, anticipate potential problems, facilitate their internal “positive and strong” frame of coping, as well as support the development of culturally appropriate psychosocial and supportive care services to maximize adaptation and recovery. The recognition that female cancer survivors may experience unique losses or potential losses from others affected by serious illness is also crucial to meet the needs of this population. In addition, participants’ experiences of cancer were contextualized by discourses of gender, as the women negotiated sociocultural constructions of identity and feminine social roles in their discussions of illness. By learning about the experiences of the participants of this study and the specific issues that they faced because of illness, health care and support providers may be better equipped to understand their clients and offer more sensitive and appropriate care and support.
Footnotes
Acknowledgments
We would like to thank the participants who have opened their hearts to share their worries and fears as well as their hopes and dreams.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.