
Abstract
This is a qualitative study of postpartum women recipients of a home-visitation social support program. Recipients of the program have been identified by a health care professional as at risk for moderate postpartum mood disorder. Relational–cultural theory and social support theories provided a conceptual framework. Results indicated (a) new mothers feel isolated and guilt at not feeling happier and (b) that a relational component this study termed “permission to be authentic” appeared to be important. New mothers experience motherhood in a profoundly different context than mothers of other times. These findings may improve the training of providers and program development for postpartum women.
This study examines a relation-based home visitation program for new mothers who have been identified by a health care professional as being at risk for postpartum depression. Its approach is different from a home visiting nurse or counseling intervention in that it uses volunteer paraprofessionals to provide relations-based, social support to the new mother. This study sought to understand the new mothers’ experiences of this intervention, and if helpful, why it was deemed helpful by the new mothers.
There is an ongoing need for health and mental health professionals to provide quality services to postpartum women. Nearly 28% of women who give birth may develop postpartum depression (Ballard, Davis, & Cullen, 1994; Le Strat, Dubertret, & Le Foll, 2011; O’Hara, 2009). Numerous studies document that the postpartum period is marked by great personal changes for the mother and is a time when the mother might feel isolated, angry, or depressed, as well as be at an increased risk for more severe psychological distress (Brockington, 2004; Chich-Hsiu, Chia-Ju, Stocker, &Ching-Yun, 2011; Epperson, 2002; Fouquier, 2011; Graham, Lobel, & Stein Deluca, 2002; Halbreich, 2005; O’Hara, 2009; Taylor, 1996). According to research, providing services for mothers at risk for postpartum depression is important to (a) decrease potentially severe consequences of postpartum depression for the new mother; (b) enhance a healthy responsiveness between a mother and her child; (c) enhance child development by increasing the mother’s ability to parent effectively; and (d) enhance the maternal life course— that is, woman’s experiences as a mother (Gomby, Culross, & Behrman, 1999; Olds et al., 2002). Yet not everyone agrees on which services are most helpful (Olds et al., 2002; Stemp, Turner, & Noth, 1986).
Motherhood
The postpartum experience has been studied as a phenomenon embedded within social forces, structures, and roles, and positioned within a historical context (Taylor, 1996; Williams, 2000). The entry into motherhood, marked by the postpartum year, has also been examined as a change in social status and role (Hart, 1976; Maushart, 1999; Stern, 1995). For example, Stern (1995, p. 5) points out that “[A] woman develops a mindset fundamentally different from the one she held before, and enters a realm of experience not known to non-mothers.”. This change in status brings with it a change in roles, affiliations, and expectations within societal institutions and social relationships (e.g., within the family, within the work setting, and in terms of membership in such community organizations as school and church groups). Maushart (1999) has described this status change as one where the woman is an “exile in motherhood” while she transitions into the new role and develops the social network associated with her new status. Maushart also posits that the isolation is due to the physical demands of caring for an infant 24 hr a day.
Historians and sociologists have written about the change in social role and status for women that occurred in the last half of the 20th century (Coontz, 1992; Garey, 1995; Kerber, 1988; Taylor, 1996; Williams, 2000). Many studies have examined the impact this change has had on women’s economic status, childrearing practices, the family structure, work/family balance, and gender roles (Crittenden, 2001; Folbre, 2001; Friedman & Greenhaus, 2000; Hochschild, 1989, 2000; Willams, 2000). The literature paints a picture of motherhood as a social role that has changed, as the economic and social conditions of women have changed. With these changes are also changes in how motherhood is perceived and its role and function in the family. Whereas within the United States caring for children, which was once a multigenerational endeavor of extended family living under one roof, has become a solitary task. For new mothers in previous generations, there was an expectation of support for becoming a mother from the other women in the family, primarily their own mothers. According to the 2000 census, only 8% of young children in the United States lived in a household that included parents and grandparents (Hernandez, 2004). Women who are becoming mothers now are from a generation where most of their own mothers worked in the paid labor force while raising their children (Hattery, 2000; Hernandez, 2004). New mothers in the 21st century experience the transition to motherhood in a profoundly different context than did mothers of any other time in this country (Garey, 1995; Glenn, 1994; Hattery, 2000). The women of this study did not have their own mothers available to support, guide, and assist in the transition to motherhood.
Social Support
In particular, social support during the postpartum period has been considered an important buffer against depression as well as a “buffer” that mediates the stress of transitioning into motherhood (Heinicke & Ponce, 1999; Nath, Borkowski, Whitman, & Schellenbach, 1991; Olds et al., 2002; Priel & Besser, 1999; Stemp et al., 1986). Social support is communication and behavior by someone close to the recipient that is intended to be helpful by conveying empathy and concern, and through the offering of information, advice, or concrete assistance with tasks (Rook, 1989; Thoits, 2011). However, studies have shown that not all social support is helpful and that sometimes the provision of social support can even have negative effects on the recipient (Coyne & Delongis, 1986; Kaplan & Toshima, 1990; McLeroy, DeVellis, DeVellis, Kaplan, & Toole, 1984; Schuster, Kessler, & Aseltine, 1990). For example, social support ineffectively provided can contribute to a longer recovery from a stroke (McLeroy et al., 1984) or to the recipient’s worsening physical health (Kaplan & Toshima, 1990). These studies suggest that social support itself is not necessarily positive, but that there are other factors that influence whether the support given provides positive or negative outcomes.
Stemp, Turner, and Noth’s (1986) study of 280 new mothers suggests that a relationship where the recipient feels cared for is a more accurate predictor of whether that social support will be effective than either of two other factors that are often examined: the number of social contacts or size of a new mother’s social network. Other studies (e.g., Burleson, Albrecht, & Sarason, 1994; Sarason & Sarason, 2001; Thoits, 2011; Weissman, 1987) have also found that the quality of the provider–recipient relationship is indicative of the effectiveness, or noneffectiveness, of the support to various populations.
Relational–Cultural theory
In addition to the factors mentioned previously, relational–cultural theory suggests that there are specific relational components that contribute to the social support relationship. Relational–cultural theory posits that there are essential elements (i.e., mutual empathy, authenticity, engagement) that create “growth-fostering” relationships, which are vital to women’s well-being (Jordan, 2000; Jordan, Kaplan, Miller, Stiver, & Surrey, 1991; Liang et al., 1998; Sormanti & Kayser, 2000; Spencer, Jordan & Sazama, 2004). One of these essential elements is authenticity, defined by relational–cultural theory as deliberate self-disclosure for the purpose of empathizing with and validating the other person, and honest reflection and sharing for the purpose of increasing trust and closeness (Miller, 1976; Miller et al., 1999; Miller & Stiver, 1997; Sloan, 2007). Authenticity has been shown to be an important component in the development of caring relationships (Erickson, 2005; Sloan, 2007; Thoits, 2011).
The literature from social support and relational–cultural theory inform the research questions of this study. Postpartum depression is serious and prevalent, requiring services that address the needs of new mothers. Social support has been identified as an effective form of support yet it remains unclear which forms of support are most effective and why. Relational–cultural theory adds an analysis of relational components that may offer a way to understand what is helpful in a relational social support intervention.
This study examines an intervention that is relation-based. Its focus is on the experiences of the new mother in becoming a mother. This is different from a public health intervention that might use a nurse to monitor the vitals of the newborn and the physical recovery of the mother. It also differs from a counseling intervention that might use psychotherapy approaches to help the mother explore her feelings. The purpose of this study was to better understand what the paraprofessional volunteers provide that is helpful, and why it is helpful.
Sample Recruitment and Selection
The program examined serves from 100 to 135 new mothers per year who are at moderate risk for postpartum mood disorders. The new mothers are usually referred by a health care professional that has identified factors that place them at moderate risk for increased stress or mood disorders during the postpartum period (e.g., limited resources, lack of emotional support). The program provides weekly in-home visits by volunteers to the new mother, with the goal of building a supportive relationship between the volunteer and the new mother to enhance the new mother’s self-esteem, provide her with community resources, and increase her social supports. Services are provided by paraprofessionals, “seasoned mother” volunteers who have older children of their own and are trained and attend weekly group supervision by a licensed clinical social worker. The services are available for the first year postpartum although some mothers receive services for the entire year, and others for considerably less. All services are voluntary and the length of provision within that year is primarily determined by the new mother. The services have no financial eligibility, as all services are free regardless of income or lack of income.
The program has a small staff of paid licensed social work clinicians who supervise the volunteer paraprofessionals who conduct the home visits. The volunteers are “seasoned” mothers, women who have older children than those of the new mothers. Interested volunteers contact the agency with a desire to commit at least 1 year of service. They are accepted to be volunteers after an interview with the director to determine their open-mindedness to others and time availability. They receive 8 hr of training by the agency on issues such as active listening techniques and the role of the volunteer. These volunteers might not hold any advanced degrees or have any professional training in human services.
The program provides an intervention that is relationship-based. The thrust of the intervention is the relationship that the volunteer cultivates with the new mother; the goal is to develop a caring relationship with the new mother for the purpose of increasing the mother’s confidence and self-esteem. To that end, the volunteer offers various types of support in a non-judging interaction. A non-judging and caring relationship has been seen by researchers to be a necessary part of a successful relationship-based intervention (Heinicke & Ponce, 1999; Weissbourd, 2000).
Of this potential pool of participants, the recruitment targeted mothers who had finished the program within the prior 3 years to ensure that the participants would be women whose experiences with, and memories of, the program were still fresh in their minds. The final sample consisted of 29 new mothers and 20 volunteers.
Method
The interviews were conducted at a private location convenient for the participants, usually their home or office. Each participant completed a demographic form that identified items such as age, years of education, and marital status. Each interview lasted less than an hour (except one, which lasted 90 min), was audiotaped for later transcription, and followed a semistructured format. The structure of the individual interviews consisted of open-ended questions to prompt the participant to reflect and elaborate on the questions posed. The following are examples of questions for the new mothers’ interviews: “What was helpful about your volunteer? Did your volunteer know what you needed? Can you describe a time, or times, when your volunteer showed you that she truly understood what you were experiencing? In what ways was she able to communicate that understanding to you? How did it make you feel?
The questions to the volunteers were related to their perception of what they provided: What kinds of support do you think you provide the new mom? How does supervision provided by the agency affect your process of giving to the new mom? Is there a kind of support that is easier or more difficult for you to provide just by nature of who you are?
Grounded theory was chosen as the method of analysis. The purpose of the study was to understand the subjective experiences of the new mothers. Semistructured, in-depth interviews were the data collection method to solicit the new mother’s experiences. Using grounded theory for analysis of the interviews fits the purpose of letting the new mothers’ stories dictate the findings (Glaser & Strauss, 1967). Using a grounded theory approach involved a specific set of procedures for coding. These procedures began with an immersion into the data for the purpose of becoming familiar with the material in context before line-by-line coding. This process entailed repeatedly listening to the audiotape of the interviews, and repeatedly reading the transcripts of the interviews and field notes. The process continued with analyzing the data in parts, often proceeding line-by-line in order to sort, code, compare codes, cluster codes, condense clusters into categories, and compare categories. The coding started with an open coding procedure, an examination of the collected data that produce numerous initials in vivo codes (Kirk & Miller, 1986) that are verbatim excerpts (e.g., “I feel so lonely”) that reflect the range of phenomena (Creswell, 1998). Codes were sorted for common experiences and then clustered into categories (e.g., the new mother feeling isolated, the new mother not feeling as happy as she expected, the new mother feeling quilt at not being happier, the new mother experiencing a genuine response from the volunteer, ways the volunteer conveyed she understood the new mother). In axial coding, the data and initial codes were examined for possible central phenomena (e.g., Isolation involving many factors: isolation as a full-time mother, being removed from familiar adult work environments, not sharing her feelings with others for fear of being judged), with close attention paid to the properties of the phenomena (Kirk & Miller, 1986). The categories were examined through the lenses of social support literature and to the relational–cultural theory; both provided a lexicon to frame the properties represented by the category labels. The coding process was deemed complete when analyzing the data produced no new codes or categories that weren’t already accounted for by the existing codes, categories, and stories (Drisko, 1997; Glaser & Strauss, 1967). At the end of this coding process, “stories” emerged. The stories led to the development of the theory that “permission to be authentic” was an important experience within this sample. For confirmability to guard against bias or omissions in analysis (Drisko, 1997), data were triangulated through comparison of the various types of data collected: interviews, observations, review of the agency’s written material, and codes. In addition, findings were reviewed with paid staff who worked for the program but were not part of the study itself—two of the lead staff and the supervisors of the volunteers—to check if findings were congruent with their experiences. At the end of this coding process, a list of nearly 70 in vivo codes was generated. The codes were examined for common phenomena and grouped into categories. These categories were then compared and condensed when it made existing categories more accurate. In the final analysis, there were a limited number of themes that best captured the subjective experiences of the new mothers as recipients of this intervention. The most prominent theme relating to the quality and uniqueness of this intervention, permission to be authentic, is discussed later.
Findings
Volunteers
Twenty volunteers participated in the study. All the volunteers had worked with at least one new mother. Ten of these volunteers had coincidentally provided services to 10 of the new mothers who participated in this study; this information was provided when a new mother stated in the interviews the name of her volunteer.
Half of the sample of volunteers had adult children. The volunteers were almost equally divided in terms of having children living at home: 9 (45%) had no children living at home and 11 (55%) had one to four children living at home. The majority of those with children living at home (8, or 40%) had two children living with them.
Half of the volunteers had paying jobs in addition to their volunteer work and half were not currently employed. Only two (10%) had previously worked in the human service sector.
Fourteen (70%) of the volunteers stated that they rarely or never attended religious services, four (20%) attended religious services monthly, and two (10%) attended such services weekly.
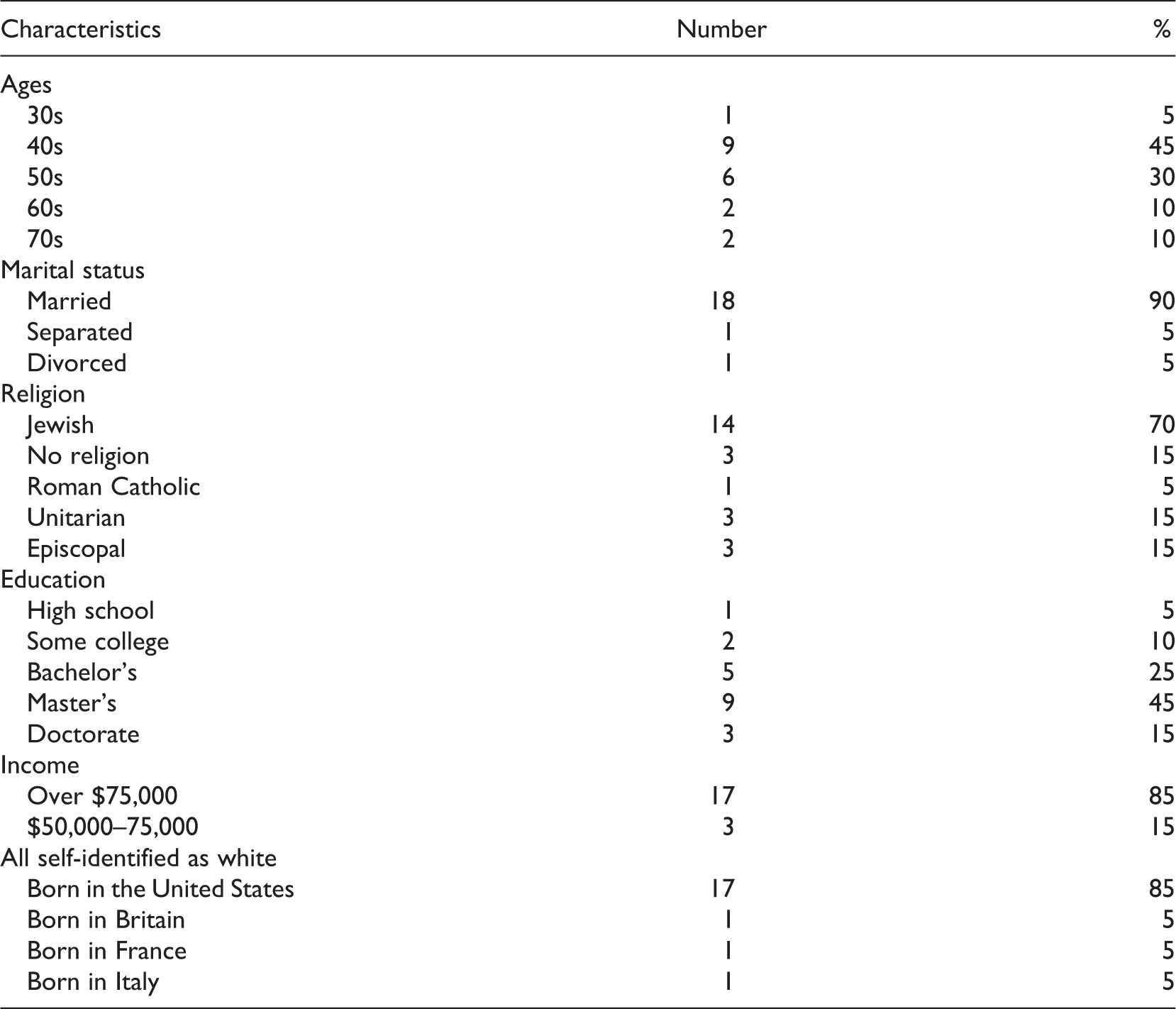
The length of time a volunteer had been with the agency at the time of this study ranged from 1 to 17 years, with a mean length of 4 (SD = 4.8) years. Six participants (30%) had volunteered with this agency for 2 years, five (25%) for 1 year, four (20%) for 1.5 years, and the remaining five volunteers in the sample had volunteered with this agency for 6, 10, 12, 13, and 17 years, respectively. Six (30%) of these participants had volunteered in some capacity—in other agencies—for 20 or more years, six (30%) had volunteered for 10–13 years, and eight (40%) had volunteered for fewer than 10 years throughout their lives.
New Mothers
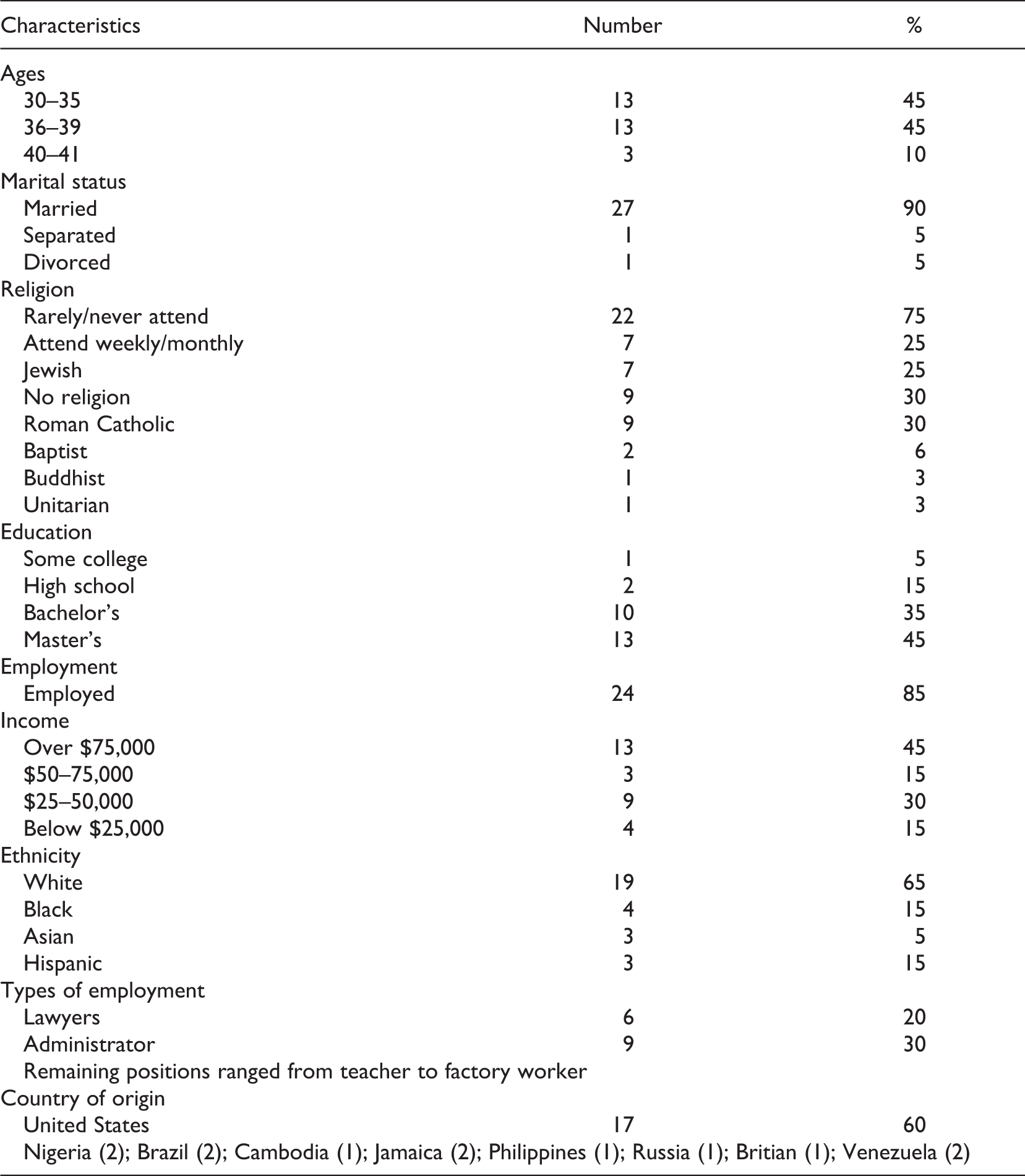
Twenty-nine new mothers were interviewed. In this study, the term “new mother” reflects the participant’s postpartum status and not to mean that she is a first-time mother, as is evident in that not all the mothers were first-time mothers.
The new mothers were asked if they felt their mothers were available for support, and if not, the reason for unavailability. Most of the new mothers acknowledged that they did not have a mother who was as available to them as they wanted. This lack of maternal availability was due to a number of circumstances: death, geographic accessibility, or the new mother’s perception of her own mother’s inability to provide the desired emotional support.
Twenty-four (85%) of the new mothers were married and living with their spouses; the remaining five were single (2), separated, or divorced (2). Most (22, or 75%) of the new mothers had one child. Four other new mothers (15%) had one previous child in addition to the baby whose birth had brought them to the attention of the agency, and three new mothers (10%) had a total of three children living at home.
New mothers in this sample had received services from the Visiting Moms Program between 2004 and 2007. Twelve (40%) of the new mothers had received services for 9 or more months postpartum, the longest service period among the new mothers studied. One (5%) had received services for 8 months postpartum, one (5%) for 7 months postpartum, and 15 (50%) new mothers had received services for 6 or fewer months.
Permission to Be Authentic
Examining the experiences of the new mothers through the lens of relational–cultural theory reveals that their relationships with the volunteers were valuable to them in an important way: permission to be authentic. Permission to be authentic included elements such as non-judging responses, empathic responses, appropriate self-disclosure by the volunteer, and feeling that the volunteer cared about the new mother (as demonstrated by the volunteers maintaining the relationship).The concept builds on the relational–cultural concept of authenticity (Jordan, 2000; Jordan et al., 1991; Miller, 1976; Miller et al., 1999; Sloan, 2007) and captures a component of the volunteers’ exchanges with the new mother that is characterized by appropriate self-disclosure, self-reflection, and the use of self as a tool of intervention to help the new mother accept her actual experiences.
These new mothers reported that, in instances when the volunteer shared the experiences she had had when her own child was an infant, it invited the new mother to reveal her “less than ideal” experiences. In the following quotation, a new mother described feeling more self-accepting of her own situation following the self-disclosure by the volunteer: She was able to say it like it is, to be honest. Also she told me some stories about things that had happened to her when her children were young which were traumatic in ways that it made her think differently of herself as a mother. She had this same thing I had, this ideal vision of being this perfect mom, and you know she would have a really bad day. She said, “You know, I really felt like I let them down. But then again of course I was frustrated. Of course I had a bad day.” She was really able to get the point across that it was okay to be a person.
Many of the new mothers stated that they appreciated that the volunteer was a mother of older children. They stated that knowing the volunteer had survived this period of motherhood helped them to trust the volunteer’s assurances, and to feel understood, as the following new mother described: “First of all I could see someone who had lived through it and was okay, and knowing that I was probably going to be okay.”
The new mothers reported feeling relieved that their experiences were not just their own, but part of a process that other new mothers had gone through. In the following quotation, the new mother describes it succinctly: The fact that there is sort of the myth that you have this baby and everything is, you are like floating on a cloud with birds chirping in your ears all day … she [the volunteer] gave me permission to admit that it is not like that.
The new mothers’ isolation and guilt were lessened by being able to share their authentic feelings. The permission, or invitation, to share these feelings was conveyed through (a) the non-judging responses of the volunteer; (b) the empathic response of the volunteer; (c) the self-disclosure by the volunteer; and (d) the feeling that the volunteer cared about the new mother as demonstrated by the volunteer’s maintaining of the relationship.
In the following quotation, the new mother describes the tension she experienced as a woman trying to reconcile her idealized mother image to the mother she now saw herself as. In the relationship with her volunteer, the new mother was given permission to be accepting of her own behavior and experience as a new mother, even if that experience was far from what she expected or hoped. What she [the volunteer] was able to do was to make me feel like I hadn’t failed because I had this depression. I had sort of thought that, if you were a mother, you had to be perfect. And she let me know that nobody is perfect and especially not mothers, and that in some ways, it is great not to be perfect, because if you are perfect then your kids are under all this pressure to pretend to be perfect too. The best thing you can do is be good enough. She really took a lot of that feeling of guilt away.
Throughout the interviews, the new mothers expressed appreciation for the volunteers’ non-judging reactions to their “disorganized house,” “un-showered state,” or “negative comments about being a new mom.” Most of the new mothers, like the one quoted below, noted that the non-judging reactions made them feel safe to express their “true” feelings. Especially when she first started seeing me, I was a complete wreck, and I was in tears all the time. I was real emotional. She saw it all. She was strong and didn’t seem upset or horrified that I was upset or judgmental—like “put it together”—none of that. She was really empathetic. I felt that “This is going to get better. This isn’t forever, and I’m going to feel better.” And here is this person sitting here who isn’t running screaming from the room; and it was nice to have somebody to be honest with about how unhappy I was.
The qualities in the relationship that enhanced the perceived social support described by the new mothers were often the qualities that, when lacking, resulted in the new mother feeling less helped by the volunteer. The new mothers referred directly to the presence or absence of elements that could be seen as falling under the rubric of “permission to be authentic,” such as non-judging responses, empathic responses, appropriate self-disclosure by the volunteer, and feeling that the volunteer cared about the new mother (as demonstrated by the volunteers maintaining the relationship).
Six of the 29 new mothers made direct comments that described an absence of “permission to be authentic,” such as the following: I’m not sure she [volunteer] got it. I mean, she was comforting, but there were some things about my experience I would never tell her. I just don’t think she would understand …. I already have family who doesn’t understand my feelings. I didn’t need this woman [the volunteer] to also look at me like I should never have had a child …which is what I was fearing.
Sometimes the lack of authenticity appeared when the volunteer seemed unaware of the experiences of the new mother, as reflected in this new mother quote: “It seemed like she [volunteer] loved infants more than I do …. I would sometimes stay quiet and smile instead of telling her how trapped I felt.”
When the helping relationship was going well, the new mothers perceived that the volunteers provided them with permission to be authentic about the full range of feelings they were experiencing as a part of the transition to motherhood. Those new mothers who did not report receiving this permission appeared less satisfied with the social support received.
Discussion
This study examined a relation-based home visiting intervention that uses volunteer paraprofessionals. The findings suggest that in this intervention there is an element involved in the helping relationship that is beneficial to the recipients of the service. This element appears to be “the permission to be authentic.” The “permission to be authentic” was inferred from the new mothers’ reports of how the volunteers behaved. This “permission to be authentic” was expressed in various ways by the volunteers—through self-disclosure by the volunteer, through the normalizing of feelings, through validation of the new mother’s feelings and experiences, and through the non-judging responses of the volunteers. In whatever way it was communicated, the effects were positive for the new mother: She felt understood, less isolated in her experience, and had a greater belief that she would survive this stressful time.
There are many ways the volunteers could convey permission to be authentic; in those cases where permission was not communicated clearly, the perceived support was deemed less satisfying and effective than in those cases where it was communicated clearly.
The phrase “permission to be authentic” is derived from relational–cultural theory’s concept of authenticity and was coined in this study to describe a relational component that appears to be important for this population. The fact that the mothers perceived that the volunteers provided them with permission to be authentic in feeling and disclosing their experiences as new mothers is an important finding because (a) it provides an indication of specific interventions that are needed for this population; (b) it underscores the relational aspects of the new mother’s experience (the relationship the new mother has with herself, with the baby, and with those closest to her); (c) from a macroperspective it suggests a change from previous generations in social forces that have altered the postpartum experience for many modern-day American women; and (d) it reveals the subjective experiences of the new mothers as they are affected by these social changes.
The use of the relational–cultural theory’s concepts of authenticity and engagement was of particular help in this study in understanding the experiences of providers and recipients of social support. This study used the concept of authenticity in a manner somewhat different from that of previous research, which employed the term to mean a quality present in each of the individuals in a relationship. This study focuses on authenticity as the creation or result of a supportive relationship in which the recipient is allowed and encouraged to reveal isolating and shameful experiences (permission to be authentic). Thus, permission to be authentic is the provider’s deliberate use of self as an intervention targeted to populations who feel shame and isolation regarding their experiences. Permission to be authentic is a concept that reaffirms the importance and centrality of authenticity in understanding human relationships, but that also holds that a service recipient’s authenticity can be encouraged by a supportive “other” who provides permission. It entails (a) the new mothers’ needs to feel connected to their own experiences; (b) the importance of the interactions between the new mothers and the volunteers; (c) the impact of self-disclosure by the volunteers on the new mothers; (d) the volunteers’ desires to feel connected to the new mothers; and (e) how the supervision groups helped the volunteers to feel connected to the new mothers. Further, this permission is a crucial element in working with emotionally isolated and shamed populations.
Implications
This study’s findings have practice and theory implications. For practice implications, the findings suggest that new mothers may benefit from social support tailored to unexpected feelings that may arise for them as they transition into a new social role. The findings also suggest that paraprofessional volunteer training can be enhanced by using a relational based approach such as relational–cultural theory that emphases authenticity. This study suggests that “permission to be authentic” decreases shame and isolation for individuals. This intervention could be adapted as a low-cost, accessible skill for paraprofessionals and professionals who reach out to populations isolated through shame or guilt. This intervention also appears to enhance the delivery of social support and could be a useful adjunct to social support agencies. The agency in this study, upon reviewing the research findings, has used the concepts of authenticity in the volunteer group supervision meetings along with discussions of relational–cultural theory. Supervisors are encouraged to model for the volunteers the “permission to be authentic” by responding authentically. It is possible that permission to be authentic is a type of support that has hitherto been labeled as emotional support or validation. This distinction among types of support is important because it may expand our understanding of what makes social support effective, as well as possibly help agencies train providers to offer more precise forms of support to more closely fit the needs of recipients. The theoretical implication of this study is its expansion in the use of relational–cultural theory in research. By using the concept of authenticity as defined by the relational–cultural theory, as an intervention, provides researchers and providers with a perspective that may capture the relational, interactional, and intrapersonal aspects of social support. In turn, this perspective may provide greater insight into when social support is effective and when it is not.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.