
Abstract
Background
The pathophysiology of CS is complex and is associated with increased inflammation and impaired vascular tone. Corticosteroids are recommended in septic shock and have been proposed as a potential treatment for other types of shock.
Objectives
We sought to evaluate the clinical outcomes associated with early corticosteroid use in patients with cardiogenic shock (CS).
Methods
Using a nationally representative database including over 1000 hospitals, we identified adults ≥18 years of age admitted from 2015–2023 with a diagnosis of CS. Patients with adrenal insufficiency, chronic rheumatologic conditions, COVID-19 infection and acute COPD exacerbation were excluded. Using inverse probability treatment weighting (IPTW), we assessed for the association of receiving early corticosteroids (within the first 2 days of admission) versus no early corticosteroids and in-hospital mortality.
Results
Of the 167,721 identified patients with CS, the mean (SD) age was 65.5 (±15.2) years and 35.0% were women. A total of 13.2% received any corticosteroid within the first 2 days of admission. The most common corticosteroid was hydrocortisone (73.9%). Mortality for those receiving and not receiving early corticosteroids was 48.8% and 29.6% (p < 0.001), respectively. After IPTW, early corticosteroid use remained associated with a 3.1% (95% confidence interval [CI]: 2.4% to 3.8%, p < 0.001) higher mortality. Among patients with CS and concomitant sepsis, 27.6% received early corticosteroids, which was similarly associated with a higher mortality (weighted mean 5.8% [95% CI: 4.6% to 7.0%, p < 0.001]).
Conclusions
Approximately 1 in 7 patients with CS received corticosteroids early during their admission, which was associated with higher in-hospital mortality.
Introduction
Cardiogenic shock, traditionally defined as a state of inadequate tissue perfusion from low cardiac output, is a complicated syndrome with a high mortality and very few interventions shown to improve outcomes. 1 Recently, different cardiogenic shock phenotypes have been recognized, highlighting cardiogenic shock as a heterogenous syndrome with widely variable hemodynamic and metabolic profiles.2–4 In particular, the pathophysiology of mixed septic and cardiogenic shock (termed mixed shock throughout), reported as the second most common type of shock admitted to the cardiac intensive care unit (CICU), 5 may be even more complicated and varied depending on the predominant driver of shock. 6
The use of biomarkers and molecular profiling has allowed for the recognition of a prominent systemic inflammatory response in cardiogenic shock which has been associated with endothelial dysfunction, shock severity, and higher risk of mortality.7–9 In patients with sepsis, also characterized by a systemic inflammatory process and host immune dysregulation, 10 immunomodulatory therapies such as corticosteroids have been used to blunt this inflammatory process and treat relative adrenal insufficiency. Although studies are conflicting regarding appropriate dosing and mortality benefit,10–13 recent societal guidelines recommend corticosteroids for patients with septic shock, 14 but given the limited data, no recommendations are available for patients with mixed shock. Given evidence of an inflammatory response, others have hypothesized that corticosteroids may be beneficial in patients with cardiogenic shock, prompting a randomized controlled trial in this population, 15 but to date, there are no prospective studies evaluating corticosteroids in cardiogenic shock.
To better define the scope and pressing need randomized controlled trials in this area, we utilized a large nationwide database to evaluate the clinical outcomes associated with early corticosteroid use in patients with mixed or cardiogenic shock.
Methods
Data Source and Study Population
We utilized the Vizient® Clinical Data Base, which includes over 1000 hospitals from 49 US states. Over 97% of academic medical centers and their affiliated hospitals in the US are included in the database, which includes administrative, financial, laboratory, and pharmacy related inpatient information time stamped to the day after admission. The database was queried for all adults aged ≥18 years admitted between October 1, 2015, and June 30, 2023, with a diagnosis of cardiogenic shock. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code R57.0 has a been found to have a high specificity (>95%) and positive predictive value (>90%) for cardiogenic shock. 16 The pooled specificity and positive predictive value of ICD-10 coding for sepsis has been found to be 98% and 72%, respectively, with a low sensitivity. 17 We defined those with both cardiogenic shock and sepsis present on admission as mixed shock.
To ensure precise timing of first corticosteroid administration from admission, patients transferred from outside institutions or unknown admission source were excluded (Figure 1). Similarly, patients transferred to another hospital during the index hospitalization or with unknown discharge status were excluded. We also excluded subjects with a separate indication for steroids, including patients with a diagnosis of rheumatologic disease, history of adrenal insufficiency, coronavirus disease-2019 infection, acute chronic obstructive pulmonary disease exacerbation, acute asthma exacerbation, contrast allergy, and anaphylaxis. Early corticosteroid use was defined as exposure to any corticosteroid within the first two days of admission, including hydrocortisone, prednisone, methylprednisolone, or dexamethasone. All data obtained from Vizient were deidentified and exempt from the Yale University Institutional Review Board review. Data from the Vizient Clinical Data Base used with the permission of Vizient, Inc, all rights reserved.

Consort diagram. Abbreviations: AECOPD, acute exacerbation of chronic obstructive pulmonary disease.
Variables of Interest
Demographics included age, sex, race, ethnicity, insurance status and income quartile by home zip code. Hospital characteristics included region (Midwest, Northeast, Southwest), number of beds (<125, 125-300, 301-500, >500), and Association of American Medical Colleges (AAMC) teaching hospital status. Comorbidities present on admission included a history of coronary artery disease, prior percutaneous coronary intervention (PCI), prior coronary artery bypass grafting (CABG), acute myocardial infarction (AMI), congestive heart failure (HF), peripheral vascular disease, cerebrovascular disease, chronic obstructive lung disease, chronic liver disease, chronic kidney disease, end-stage renal disease, history of left ventricular assist device (LVAD), heart transplantation, diabetes, cancer and tobacco use. Additional identified diagnoses, coded as present on admission, included out of hospital cardiac arrest and acute renal failure. We calculated shock stage per Society for Cardiovascular Angiography and Interventions (SCAI) classification using previously utilized methods from the Critical Care Cardiology Trials Network (CCCTN). 18
The database includes timed procedures and medications reported as the day since admission. We identified critical care interventions performed within the first two days of admission, including use of pulmonary artery catheter (PAC), use of any mechanical circulatory support (MCS) device, intra-aortic balloon pump, Impella, extracorporeal membrane oxygenation, durable LVAD, left heart catheterization (LHC), PCI, CABG, and heart transplantation. Noncardiac interventions included thoracentesis, bronchoscopy, renal replacement therapy, non-invasive and invasive mechanical ventilation use within the first two days. Supplementary Table 1 lists the ICD-10-CM codes used to identify procedures and diagnoses.
Outcomes
Our primary outcome was in-hospital mortality. Secondary outcomes included total hospital costs, and hospital and ICU length of stays.
Statistical Analysis
Baseline characteristics were compared between patients receiving an early corticosteroid (within the first two days of admission) and those that did not. Continuous variables were described as means and standard deviation and categorical variables were described as frequencies and percentage. T-tests were used to compare continuous variables and chi-squared tests for categorical variables. Using inverse probability of treatment weighting (IPTW), we assessed for the association between early corticosteroid utilization and in-hospital mortality. To reduce extreme weights, we used weight stabilization and truncation at the first and 99th percentiles. 19 In order to ensure covariate balance, we assessed weighted standardized differences with a target difference <0.10. Covariates used in the multivariable models included demographics (age, sex, race and ethnicity, primary payer, and income quartile), comorbidities (smoking, coronary artery disease, dyslipidemia, history of acute MI, prior PCI, prior CABG, diabetes, congestive HF, peripheral vascular disease, cerebrovascular disease, prior heart transplant, prior LVAD, chronic kidney disease, end-stage renal disease, chronic obstructive lung disease, chronic liver disease, cancer, dementia, Acquired Immunodeficiency Syndrome), Charlson Comorbidity Index, 20 key diagnoses present on admission (out-of-hospital cardiac arrest, acute renal failure, and sepsis), maximum admission (on day 1) SCAI shock stage, hospital/admission characteristics (bed size, region, AAMC-teaching status, and admission timing), and key therapies within the first two days of admission (vasoactive medications, number of vasopressors on day 1, MCS, LHC, PAC, and invasive mechanical ventilation). To evaluate hospital and ICU length of stay, we used Poisson regression expressed as an incidence rate ratio (IRR). Adjusted total hospital costs were assessed using a gamma regression model.
In addition, we performed several subgroup and sensitivity analyses. First, to differentiate patients with potential mixed shock, we repeated analyses for patients with and without a diagnosis of sepsis on admission. Second, we stratified by key admission diagnoses, specifically those with a primary admission diagnosis of AMI or HF. Third, to evaluate for differences in outcomes relative to markers of acuity, we repeated analyses among only patients receiving MCS within the first two days of admission, only patients receiving vasoactive medications within the first two days of admission, only patients with an admission lactate ≥5 mmol/L, and again with a model also including baseline creatinine, lactate, and white blood cell count. Fourth, we repeated analyses in patients presenting with and without cardiac arrest. Fifth, we stratified analyses by the maximum SCAI shock stage C through E on admission.
Next, we conducted falsification testing, which is a method to test for residual confounding in observational studies, where non-significant results suggest that findings are less likely driven by residual confounding. 21 We a priori selected pneumonia and a composite of deep venous thrombosis, cellulitis, osteomyelitis, and diarrhea as our falsification endpoints. Finally, we also performed interaction testing to assess for differences in steroid type and in-hospital mortality as well as early corticosteroid use and vasoactive agent. All analyses were performed on STATA 16.0 (Stata Corp, College Station, TX) with statistical significance considered at a two-tailed P < 0.05.
Results
Patient Characteristics
A total of 167,721 patients with a diagnosis of CS were identified (Figure 2), 22,140 (13.2%) of which received corticosteroids within the first two days of admission. A total of 38,456 (22.9%) of patients had mixed shock, including 10,607 (27.6%) of which that received early corticosteroids (Central Illustration). The most common corticosteroid was hydrocortisone, used in 16,358 (73.9%) of patients, followed by dexamethasone and prednisone, used in 3285 (14.8%) and 3160 (14.3%), respectively. The least commonly used corticosteroid was methylprednisolone, used in 235 patients (1.1%).

Central Illustration.
The demographic and clinical characteristics stratified by early corticosteroid use are presented in Table 1. Patients who received early corticosteroids were slightly younger (64.5 vs 65.6 years) and more likely to be female (38.9% vs 34.4%) when compared to those who did not receive early corticosteroids (both, p < 0.001). Patients receiving early corticosteroids were also more likely to have acute renal failure, out-of-hospital cardiac arrest, and more severe SCAI shock classification on admission (all, p < 0.001). Demographic and clinical characteristics stratified by patients with and without mixed shock are detailed in Supplemental Table 2.
Baseline Demographic and Clinical Characteristics Stratified by Early Corticosteroids use.
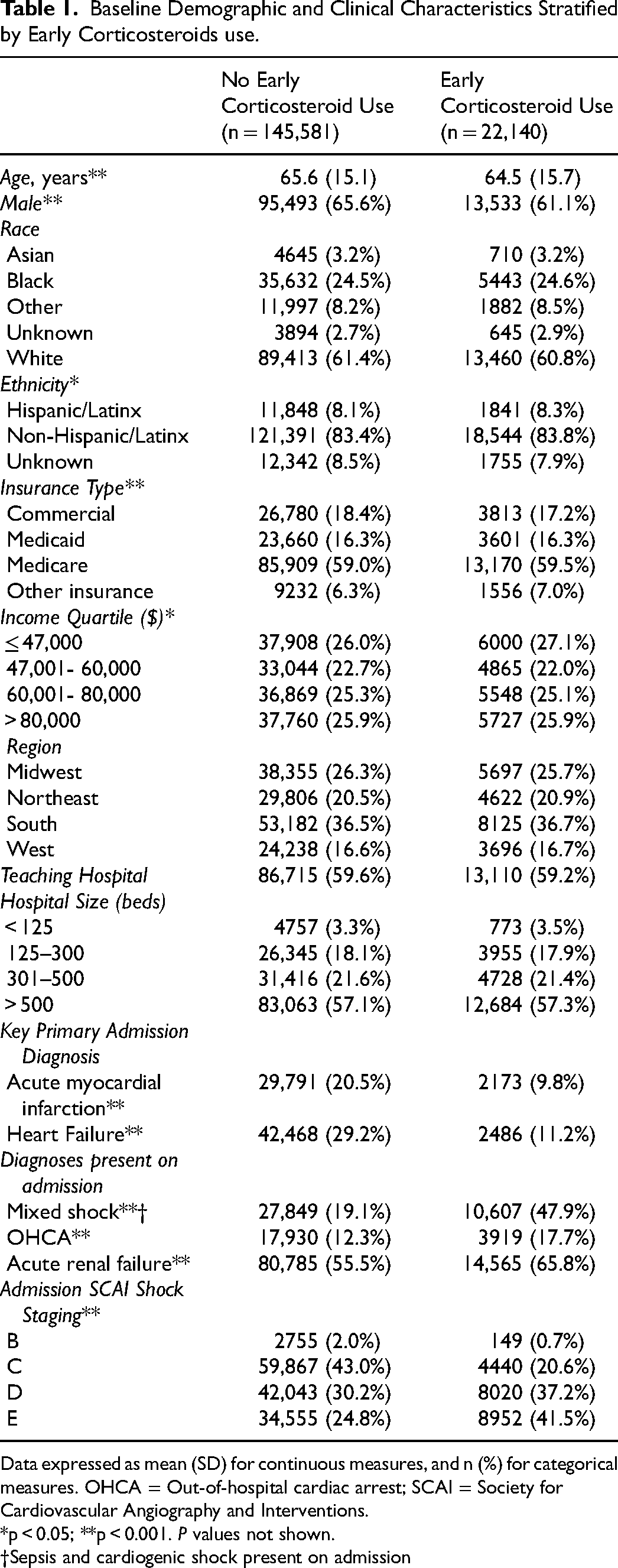
Data expressed as mean (SD) for continuous measures, and n (%) for categorical measures. OHCA = Out-of-hospital cardiac arrest; SCAI = Society for Cardiovascular Angiography and Interventions.
*p < 0.05; **p < 0.001. P values not shown.
†Sepsis and cardiogenic shock present on admission
Overall, the early corticosteroid group had a higher comorbidity burden (mean Charlson comorbidity index 4.4 vs 4.3, p < 0.001) and more chronic medical diseases, such as chronic kidney, liver, and pulmonary disease (all, p < 0.001) (Table 2). In contrast, those receiving early corticosteroids were less likely to have several cardiovascular comorbidities, including history of coronary artery disease, prior PCI, prior MI, HF, and peripheral vascular disease (all, p < 0.001). The early corticosteroid group was less likely to have atrial fibrillation (45.6% vs 46.9%, p < 0.001) and ventricular tachycardia (3.2% vs 3.5%, p = 0.008) compared to those not receiving early corticosteroids.
Baseline Comorbidities Stratified by Early Corticosteroids use.
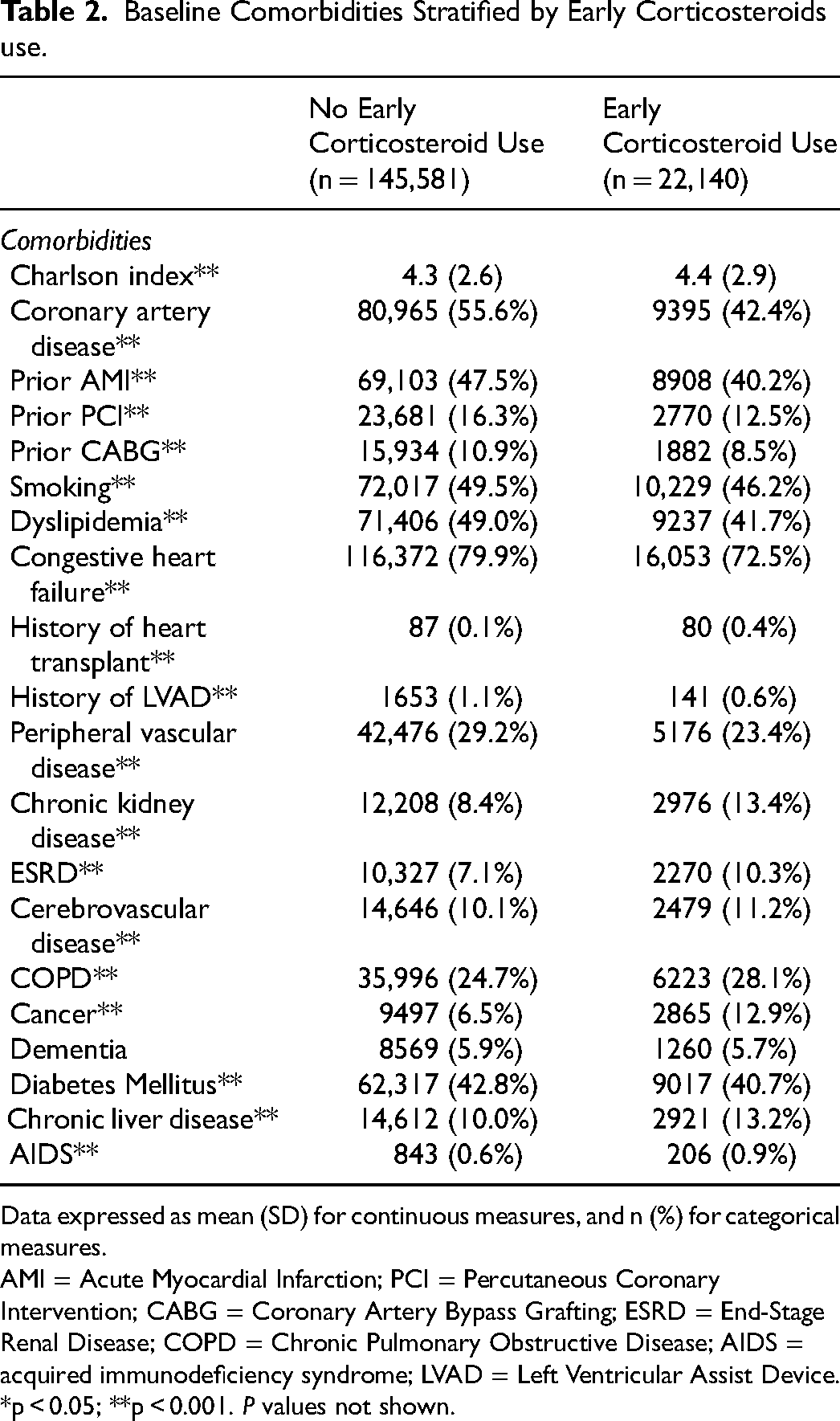
Data expressed as mean (SD) for continuous measures, and n (%) for categorical measures.
AMI = Acute Myocardial Infarction; PCI = Percutaneous Coronary Intervention; CABG = Coronary Artery Bypass Grafting; ESRD = End-Stage Renal Disease; COPD = Chronic Pulmonary Obstructive Disease; AIDS = acquired immunodeficiency syndrome; LVAD = Left Ventricular Assist Device.
*p < 0.05; **p < 0.001. P values not shown.
Laboratory Values and Critical Care Therapies
Patients who received corticosteroids within the first two days had higher initial and peak lactate and creatinine values at the time of presentation (both, p < 0.001) (Table 3). They also had a higher initial white blood cell count (13.0 vs 11.4 x1000/µL, p < 0.001) compared to patients not receiving early corticosteroids.
Admission Laboratory Values Stratified by Early Corticosteroids use.
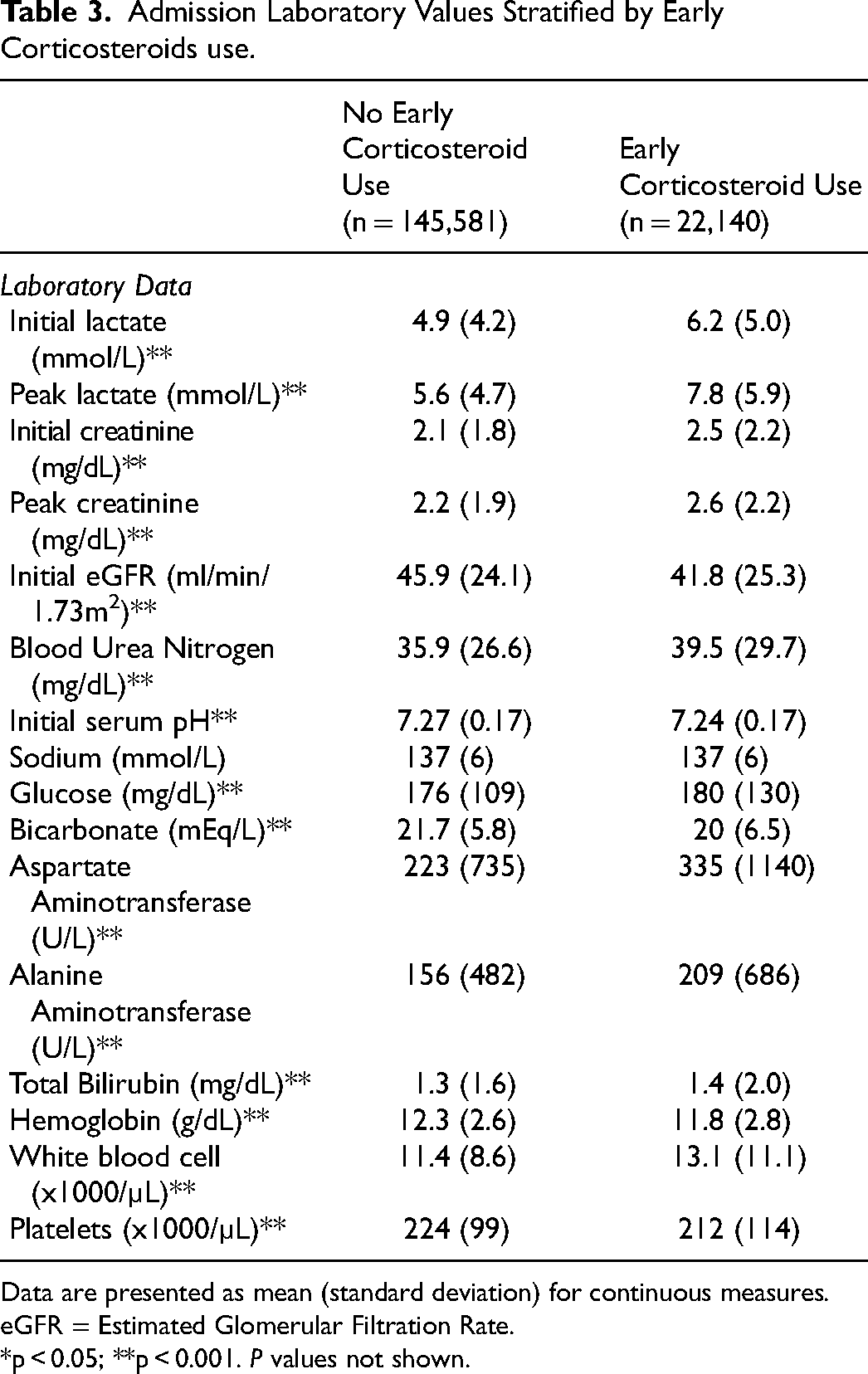
Data are presented as mean (standard deviation) for continuous measures.
eGFR = Estimated Glomerular Filtration Rate.
*p < 0.05; **p < 0.001. P values not shown.
Vasoactive medication utilization and critical care therapies are shown in Table 4 and Supplemental Table 3. The early corticosteroid group was more likely to receive any vasoactive medication within the first two days (90.1% vs 75.0%, p < 0.001), including norepinephrine, vasopressin, epinephrine and dobutamine but were less likely to receive milrinone (all, p < 0.001). In interaction testing, we found a significant association between early corticosteroid use and vasopressin (p < 0.001), epinephrine (p = 0.002), and dobutamine (p = 0.03). There was not a significant association with the remaining vasoactive medications.
In-Hospital Medications Stratified by Early Corticosteroids use.
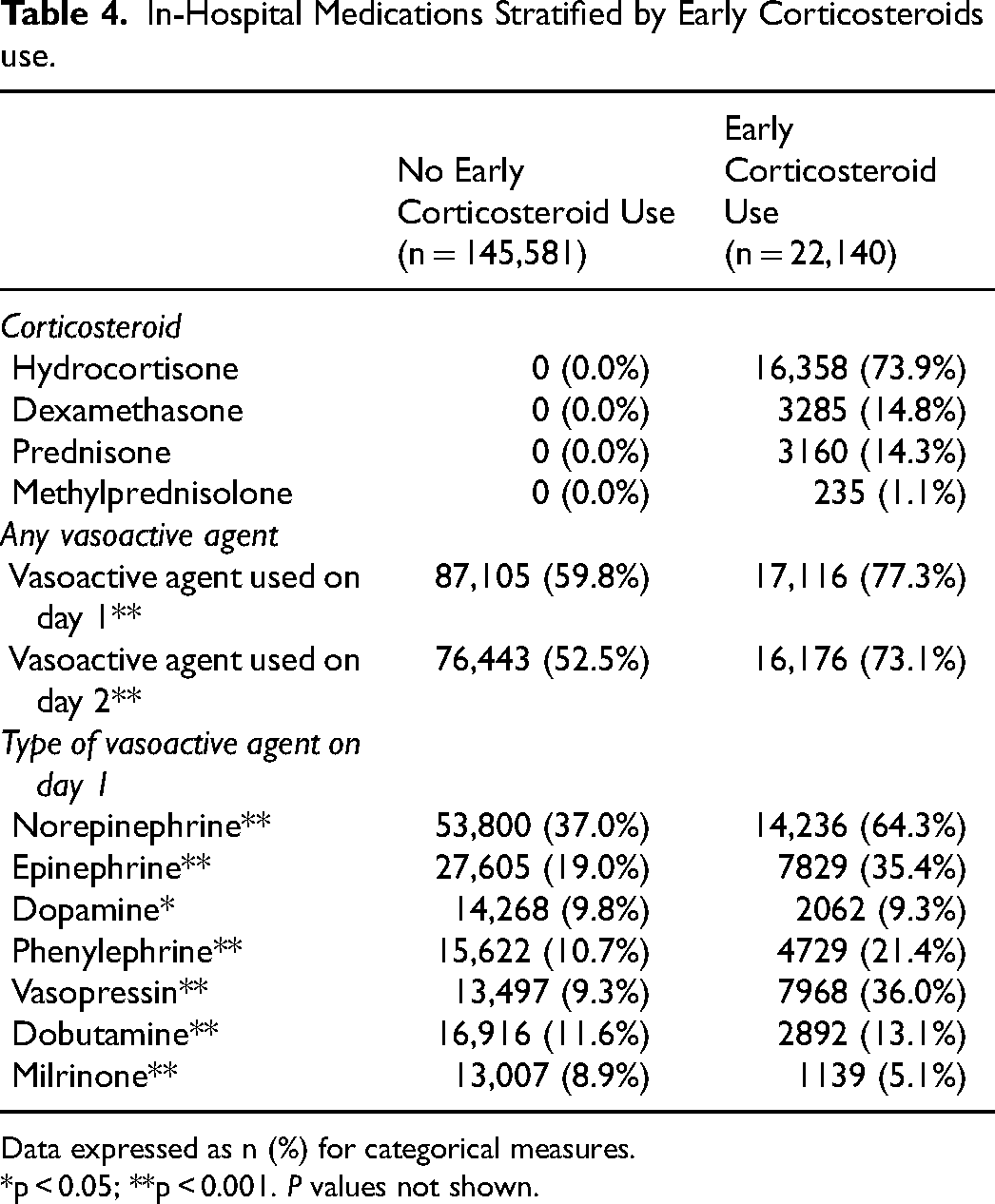
Data expressed as n (%) for categorical measures.
*p < 0.05; **p < 0.001. P values not shown.
Patients who received early corticosteroids were less likely to undergo left heart catheterization, PAC placement, PCI and temporary pacemaker within the first two days of admission (Figure 3). Early corticosteroids use was also associated with a lower use of MCS. Those who received early steroids were also more likely to undergo noncardiac therapies, including thoracentesis, bronchoscopy, renal replacement therapy, non-invasive and mechanical ventilation within two days of admission (all, p < 0.001).
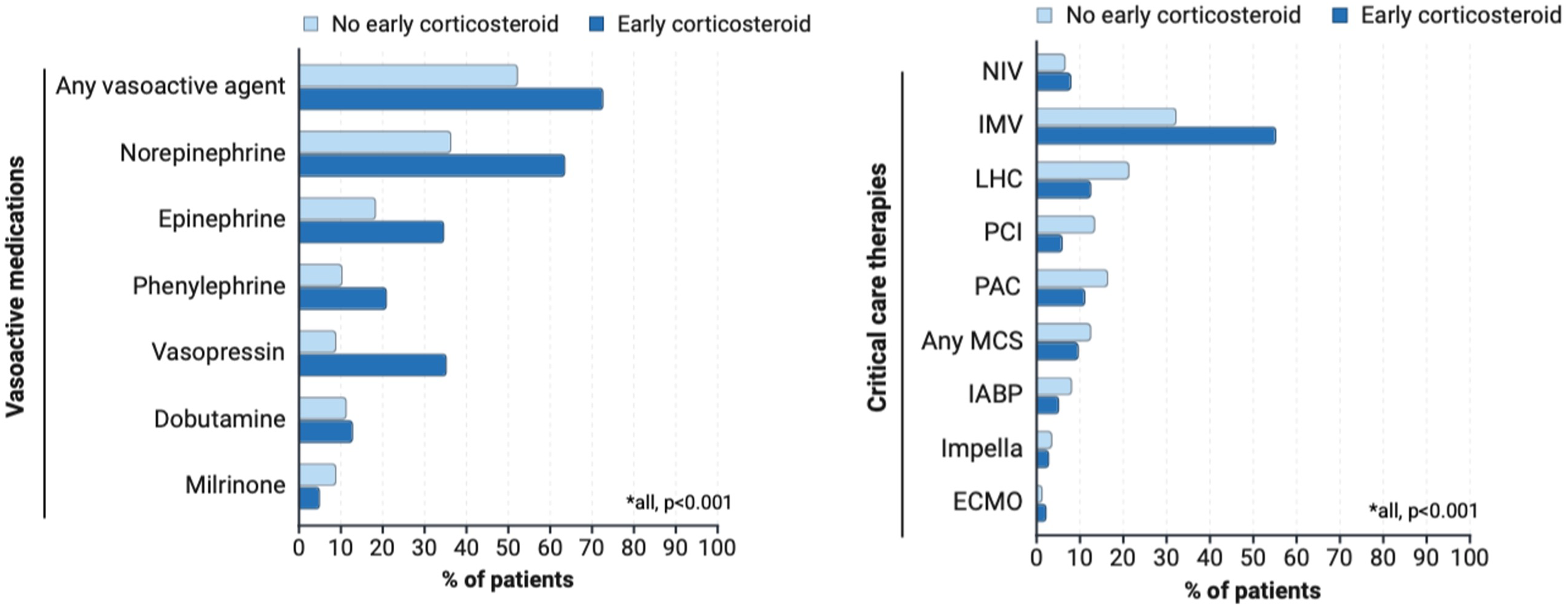
Medications, procedures, and therapies stratified by early corticosteroids. Abbreviations: MC, mechanical circulatory support; IABP, intra-aortic balloon pump; ECMO, extracorporeal membrane oxygenation; LVAD, left ventricular assist device; LHC, left heart catheterization; PAC, pulmonary artery catheterization; PCI, percutaneous coronary intervention. CABG, coronary artery bypass graft; RRT= renal replacement therapy; NIV, non-invasive ventilation; IMV, invasive mechanical ventilation.
Mortality
The unadjusted in-hospital mortality was 48.8% versus 29.6% (p < 0.001) in the group who received early corticosteroids compared the group that did not. Mortality was higher among the early corticosteroid group when stratified by the number of vasoactive medications, except for those receiving 5 vasoactive medications, and when stratified by maximum SCAI shock stage on day 1 of admission (Figure 4A and B).
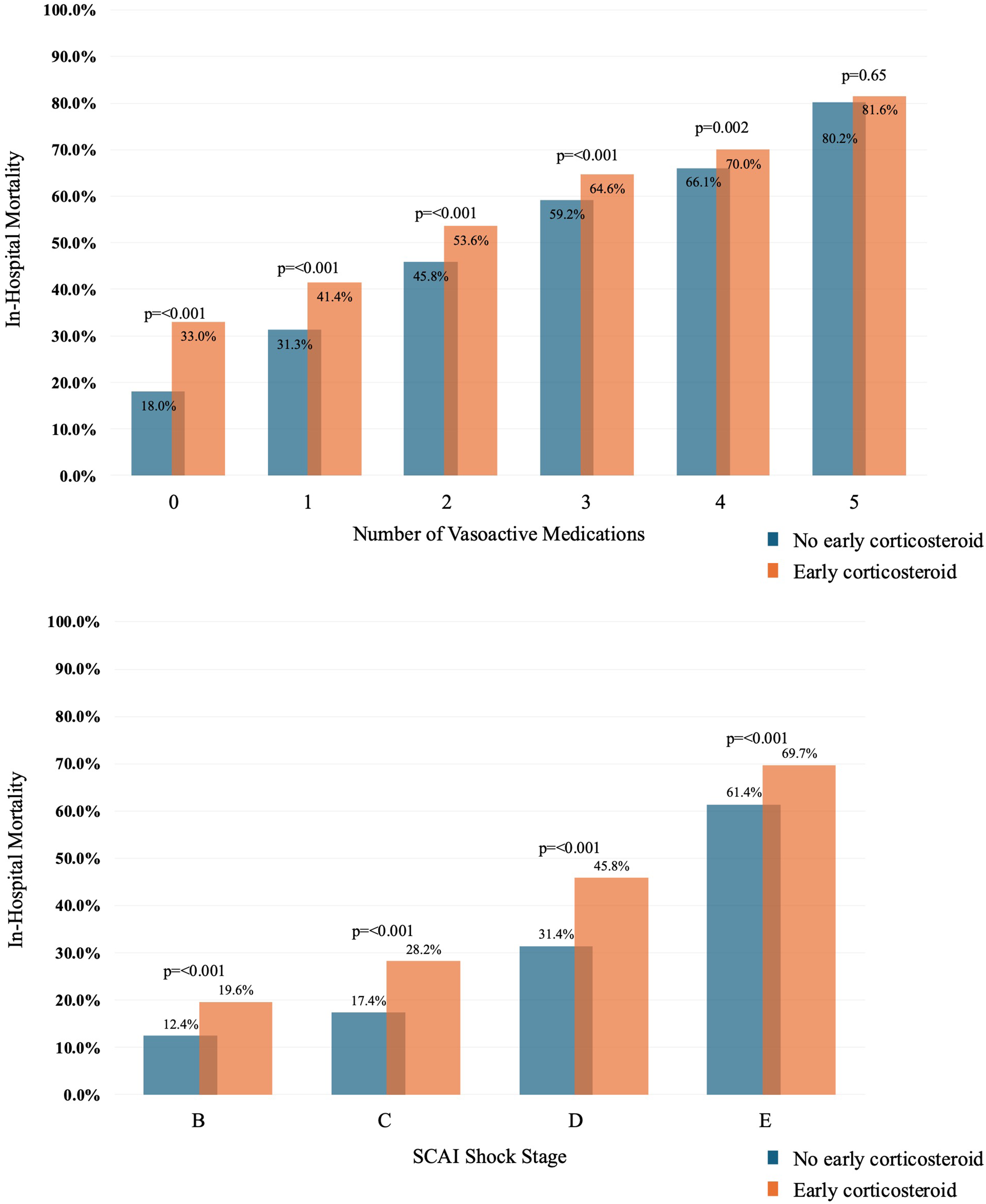
Maximum number of vasoactive medications (A) and SCAI shock stage (B) on the first day of admission. Abbreviations: SCA, society for cardiovascular angiography and interventions.
After IPTW with well-balanced standardized mean differences (<0.10) (Supplemental Table 4), early corticosteroid use was associated with a 3.1% increase in weighted mean mortality (95% confidence interval [CI]: 2.4% to 3.8%, p < 0.001). Interaction testing between corticosteroid type and in-hospital mortality was statistically significant (p < 0.001). After multivariable adjustment, compared to no early corticosteroids, we found significant differences in in-hospital mortality stratified by corticosteroids type (Supplemental Figure 1).
In subgroup analysis among patients with and without mixed shock on admission, early corticosteroid use was associated with a 5.8% (95% CI: 4.6% to 7.0%, p < 0.001) and 2.3% (95% CI: 1.5% to 3.2%, p < 0.001) increase weighted mean in-hospital mortality, respectively. Next, when stratified by primary admission diagnosis, early corticosteroid use remained associated with a higher in-hospital mortality in patients presenting with a primary diagnosis of acute MI (weighted mean difference 2.5%; 95% CI: 0.4% to 4.7%, p = 0.02) or HF (weighted mean difference 2.1%; 95% CI: 0.6% to 3.6% p = 0.007). Results were similar when stratified by only those that received MCS within the first two days of admission (weighted mean difference 2.9%; 95% CI: 0.7% to 5.1%, p = 0.01), only those receiving vasoactive medications (weighted mean difference 3.4%; 95% CI: 2.6% to 4.2%, p < 0.001), admission lactate ≥5 mmol/L (weighted mean difference 2.1%; 95% CI: 1.2% to 3.0%, p < 0.001), or in the additional model including baseline labs (weighted mean difference 4.1%; 95% CI: 3.2% to 5.1%, p < 0.001). When stratified by cardiac arrest on admission, early corticosteroid use was associated with a higher mortality for those without (weighted mean difference 3.3%; 95% CI: 2.6% to 4.2%, p < 0.001) but not with (weighted mean difference 1.0%; 95% CI: −0.9% to 3.0%, p = 0.29) cardiac arrest. Results were consistent across shock stages C through E (Supplemental Table 5 and 6).
In falsification analysis, we did not find a statistically significant association between patients receiving early corticosteroids and pneumonia or the composite endpoint after inverse probability of treatment weighting (Supplemental Table 7).
Secondary Outcomes
Total hospital cost was significantly higher in those who received early corticosteroids ($30,781 vs $28,242, p < 0.001), which persisted after multivariable adjustment (+$2418; 95% CI: $1292-$3,543, p < 0.001). Early corticosteroid use was associated with a shorter median hospital length of stay (6 days vs 7 days, adjusted Incident Rate Ratio [IRR]: 0.99; 95% CI: 0.98-0.99, p < 0.001) and similar median ICU stay (3 days vs 3 days, adjusted IRR: 1.00; 95% CI: 0.99-1.01, p = 0.84). Among hospital survivors, ICU LOS adjusted (IRR: 1.03; 1.02-1.04, p < 0.001), total hospital LOS (IRR: 1.04; 1.03-1.04, p < 0.001), and total hospital costs (+$3231; 95% CI: $1562-$4,900, p < 0.001) were all higher in those receiving early corticosteroids.
Discussion
In this nationwide study investigating clinical outcomes for patients with cardiogenic shock receiving early corticosteroids, we present several key findings. First, we found that nearly 1 in 7 patients received early corticosteroids, including nearly 50% of patients with mixed shock. Second, patients receiving early corticosteroids presented with increased markers of acuity, more non-cardiac comorbidities, and more frequently underwent non-cardiac procedures and therapies. Third, early corticosteroid use was associated with higher in-hospital mortality when compared to patients who did not receive early corticosteroids, which persisted after multivariable adjustment and several sensitivity analyses. Taken together, these findings highlight that early corticosteroid use is relatively common, especially for those with mixed shock, and its use is associated with worse outcomes. These findings should not be interpreted as causative and are observational, hypothesis-generating results.
Our results align with two previous, smaller single-center retrospective studies.22,23 In 2023, Fan et al found that 16.4% of over 1500 patients with cardiogenic shock admitted to a tertiary university hospital received corticosteroids, and that corticosteroid use was associated with increased 90-day all-cause mortality. 22 Similarly, using the same institutional data, Haddad et al reported higher 90-day mortality and fewer ventilator-free days in patients with cardiogenic shock receiving systemic early corticosteroids (defined as within 24 h of admission). 23 Both studies detailed higher severity of illness scores in the corticosteroid group, similar to our findings. In addition to being a substantially larger study, our results are additive by being nationwide, multicenter and the addition of detailed analyses of the mixed shock patient population, an important patient population with limited data. 6
One important observation from our study is the high proportion of patients with cardiogenic shock that received systemic corticosteroids within the first two days of admission, even after exclusion of certain groups that could have received them for proven indications. Potential reasons behind this practice could be related to a clinical presentation of mixed or undifferentiated shock, lack of hemodynamic assessment or delay in shock phenotyping. Conversely, patients who did receive early corticosteroids were less likely to undergo invasive hemodynamic assessment with a PAC, despite presenting with more severe shock per SCAI staging, higher levels of lactate, and higher use of vasoactive medications. Early recognition, phenotyping and staging is critical in patients with cardiogenic shock and the implementation of hemodynamic tailored therapies may help clinicians make more informed decisions regarding the use of corticosteroids in this population. 24
Our findings highlight the needs for prospective data, especially in the mixed shock patient population which is more likely to receive corticosteroids. Mixed shock is a complicated syndrome with unique phenotypes, recently defined as cardiogenic-vasodilatory, vasodilatory-cardiogenic, and primary mixed shock, each with unique pathophysiology and treatment strategies. 25 Numerous randomized clinical trials have evaluated the use of corticosteroids in critically ill patients with sepsis, but patients with mixed or concomitant cardiogenic shock were often excluded and poorly represented in many general ICU studies.11,12,26 If patients with cardiac involvement as part of their shock syndrome are less likely to benefit from steroids, one potential mechanism for the higher mortality could be the known adverse effects of steroids, including metabolic derangements, hyperglycemia, neuromuscular weakness, and potential for increased infections. 27
Our study has several limitations, including a retrospective design utilizing an administrative database which relies on ICD-10 coding and claims data. Given the high specificity for cardiogenic and sepsis coding (>90% in both), it is likely we identified true cases of mixed and cardiogenic shock. However, the sensitivity is low, and it is very likely that we missed cases. Despite rigorous IPTW analysis with excellent covariate balance, consistency across multiple subgroup analyses, and neutral falsification endpoints, there is certainly residual confounding by indication insofar as corticosteroids are often used in clinical practice when a patient is severely ill with refractory shock. One unique aspect of the dataset is date-stamped procedures and medications, but we are unable to narrow the time beyond the day of admission. Furthermore, we lack data on medication dosages or whether medications were push versus continuous infusions, which is important for corticosteroid administration and vasopressor therapy. While we excluded patients with known indications for corticosteroids, we do not have home medications and therefore cannot identify patients chronically prescribed corticosteroids. Given the administrative dataset, we also do not have vital signs or invasive hemodynamic data, which is important clinically and to define the predominant type of shock (eg, primary vs secondary shock etiology). Finally, we do not know the reason why corticosteroids were given, but the predominant use of hydrocortisone suggests use of “stress dosing”.
In conclusion, in this large, multicenter study of patients with mixed and cardiogenic shock patients receiving early corticosteroids, we found that early corticosteroid use was relatively common and associated with higher in-hospital mortality. It is unclear if these associations represent a much sicker patient population where corticosteroids were utilized for refractory shock or a true association with worse outcomes. However, findings highlight the need for randomized prospective data to determine the role of corticosteroids in patients with mixed and cardiogenic shock.
Supplemental Material
sj-docx-1-jic-10.1177_08850666261437767 - Supplemental material for Early Corticosteroid use and Clinical Outcomes in Patients with Mixed and Cardiogenic Shock
Supplemental material, sj-docx-1-jic-10.1177_08850666261437767 for Early Corticosteroid use and Clinical Outcomes in Patients with Mixed and Cardiogenic Shock by Maria Gabriela Gastanadui, Hannah R. Murphy, Andi Shahu, Israel Safiriyu, Cory Heck, Maria Hysolli, Santiago Callegari, Sanjana Garimella, Tariq Ali, Jacob C. Jentzer, Ann Gage, Mark Jacobs, Jason N. Katz and P. Elliott Miller in Journal of Intensive Care Medicine
Supplemental Material
sj-jpg-2-jic-10.1177_08850666261437767 - Supplemental material for Early Corticosteroid use and Clinical Outcomes in Patients with Mixed and Cardiogenic Shock
Supplemental material, sj-jpg-2-jic-10.1177_08850666261437767 for Early Corticosteroid use and Clinical Outcomes in Patients with Mixed and Cardiogenic Shock by Maria Gabriela Gastanadui, Hannah R. Murphy, Andi Shahu, Israel Safiriyu, Cory Heck, Maria Hysolli, Santiago Callegari, Sanjana Garimella, Tariq Ali, Jacob C. Jentzer, Ann Gage, Mark Jacobs, Jason N. Katz and P. Elliott Miller in Journal of Intensive Care Medicine
Footnotes
Abbreviations
ORCID iDs
Ethical Considerations
All data obtained from Vizient were deidentified and exempt from the Yale University Institutional Review Board review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article are available in the article and in its online Supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.