
Abstract
Intravenous crystalloid solutions are among the most common medical interventions applied and have supplanted colloid-based solutions as the standard of care for volume resuscitation in most settings. Despite their widespread use, debate has existed over the optimal composition of these solutions and their differential effects on patient outcomes. In this review, we will describe the pre-clinical studies that identified physiological differences when ‘balanced crystalloids’ and ‘normal saline’ are administered, the experimental studies that confirmed these differences in humans, the observational studies that indicated the level of concern, and the subsequent clinical trials that provide evidence to guide therapy in current practice.
Keywords
Introduction
Intravenous crystalloid solutions are among the most common medical interventions, with millions of liters administered annually in the United States.1–3 Their conventional origins trace back to the nineteenth century, when O'Shaughnessy identified “stagnation of the venous system” as a key physiologic disturbance in patients with cholera and proposed that “salts of highly oxygenated constitution” would offer therapeutic benefit.4,5 That hypothesis was tested by Thomas Latta in 1831, who documented clinical improvement of a young girl with cholera after administering intravenous salt solutions, noting “the pulse… returned to the wrist…her extremities were warm.” 6
The term “normal” saline likely emerged in the late 1890s, when Hamburger's freezing point experiments led him to conclude that 0.9% sodium chloride was isotonic to blood. 7 Challenges to whether sodium chloride alone represented adequate physiologic replacement included seminal observations by Sydney Ringer and others, such as the finding that calcium added to a sodium chloride solution better supported perfusion and cardiac function. Building on these insights, Alexis Hartmann argued that ‘it may be necessary to give parenterally fluids that are quite similar to normal intercellular fluid’, advocating for the use of both electrolytes and buffers to restoring volume losses during illness. 8 Herein, we examine the composition of commonly used crystalloid solutions, summarize preclinical studies highlighting physiologic differences between ‘normal’ saline (NS) and ‘balanced’ crystalloids (BC), observational data that raised concerns about specific fluid types, and recent large trials that have shaped current clinical practice.
The Composition of Common Crystalloid Solutions
Table 1 presents the composition of the most prescribed crystalloid solutions, including (NS) and so-called ‘balanced’ solutions including Lactated Ringer's (LR), and Plamsalyte (PL). The differences in osmolarity, sodium chloride content, and the presence or absence of buffers raised questions about the relative benefits and harms of the different fluids, especially when infused in large amounts. In the case of NS, these concerns focused on metabolic acidosis and supraphysiologic chloride concentrations. Concerns with BC have included relative hypotonicity, accumulation of lactate and acetate, and accumulation of potassium in vulnerable populations.
Composition of Commonly Used Crystalloid Solutions.

Concerns Raised by Experimental Studies
Potential Hemodynamic Effects on the Kidney
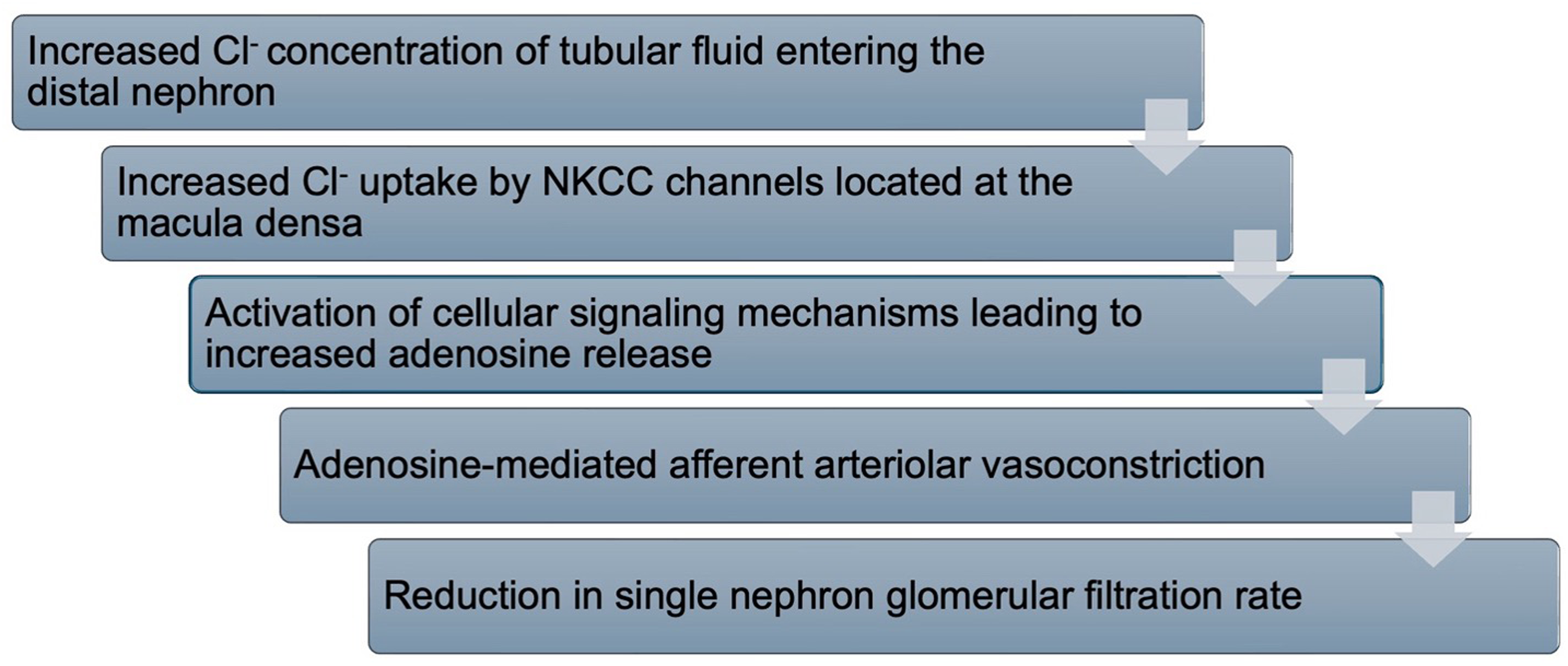
Renal blood flow and glomerular filtration are linked through the sympathetic nervous system, baroreceptors within arterioles, and delivery of chloride to the macula densa, a specialized region of the distal nephron that detects sodium and chloride concentrations.11–13 The macula densa releases adenosine in response to chloride delivery to the distal nephron, which acts on G-protein-coupled purine receptors to inhibit adenylate cyclase and cyclic AMP production, causing vasoconstriction of the afferent arteriole. 14 Vasoconstriction, in turn, decreases glomerular blood flow and glomerular filtration. This mechanism, known as tubuloglomerular feedback (TGF) (Figure 1), was examined through micro-puncture experiments demonstrating that infusions of various concentrations of saline into isolated segments of the distal nephron reduced the single-nephron filtration rate. 15 Work done by Schnermann in the 1970s suggested that chloride concentration, rather than osmolarity, was the major regulator of TGF. 16
Mechanism of Tubuloglomerular Feedback.
Building on this hypothesis, Wilcox et al tested the effects of different infused solutions of hypertonic sodium chloride, sodium bicarbonate, sodium acetate, dextrose, ammonium chloride, or ammonium acetate on renal blood flow (RBF) of denervated dog kidneys. He observed that RBF declined below pre-infusion rates with the chloride-containing solutions after an initial period of vasodilation. Wilcox thus concluded that chloride acts as the signal for changes in afferent arteriolar vascular tone rather than the solution's osmolarity, leading to potential concerns about the effects of excess chloride on renal blood flow during acute illness. 17
Hyperchloremia and Metabolic Acidosis
Infusion of sodium chloride solutions can also alter plasma pH. In 1969, Rosenbaum found that changes in plasma bicarbonate concentrations during infusion of various hypertonic solutions into anesthetized dogs were not related to transcellular shifts but were the result of dilution of the intravascular space. 18 Similarly, when characterized by strong-ion difference (SID), NS (SID = 0) tends to reduce the SID of plasma, while BC has a higher SID.19,20 Regardless of the framework, the tendency to develop acidosis and hyperchloremia has been consistently reproduced in both preclinical and clinical studies (see below). 21 Experimental data from animal models demonstrate that acidosis can impair cardiac contractility and vascular tone.22,23 Similar effects on cardiac contractility have been described in observational studies of humans. 24
Inflammation and Worsening of AKI
In a rat model of sepsis, animals receiving NS had significantly more hyperchloremia and higher levels of interleukin-6, indicating increased inflammation compared to those receiving PL. Additionally, 100% of the rats in the NS group developed acute kidney injury (AKI), compared to 76% in the PL group. Moreover, 83% of the rats that received NS developed RIFLE stage I (injury) or F (failure) of AKI, while only 26% of the PL group progressed to these stages. Lastly, the NS group had histologic evidence of worse tubular injury, with more pronounced brush border loss, vacuolization, and dilation of the tubular lumen compared to animals receiving PL. The authors postulated that injury is mediated by multiple mechanisms including: increased chloride delivery and activation of TGF in an already under-perfused kidney and inflammatory cytokine gene expression stimulated by acidosis. 25 These results from animal models of AKI further supported the hypothesis that NS may be harmful compared to BC.
Early Experimental and Observational Studies in Humans
Human studies have confirmed a tendency toward hyperchloremia and acidemia with the use of NS compared to BC (Table 2). In a randomized crossover study of 12 patients using MRI arteriography to compare changes in renal cortical perfusion and renal blood flow, a measurable reduction in mean renal artery flow velocity and cortical tissue perfusion was observed after NS infusion, compared to baseline, which was not observed after PL 148 infusion. There were no differences in the urine neutrophil gelatinase-associated lipocalin (NGAL) concentrations, a biomarker of tubular injury, between the groups. While no adverse clinical events occurred in these healthy individuals, the differences elevated concern about the potential for NS to cause harm during acute illness. 26
Small Experimental Studies Examining Differences in Metabolic Parameters Between Balanced Crystalloids and Normal Saline.
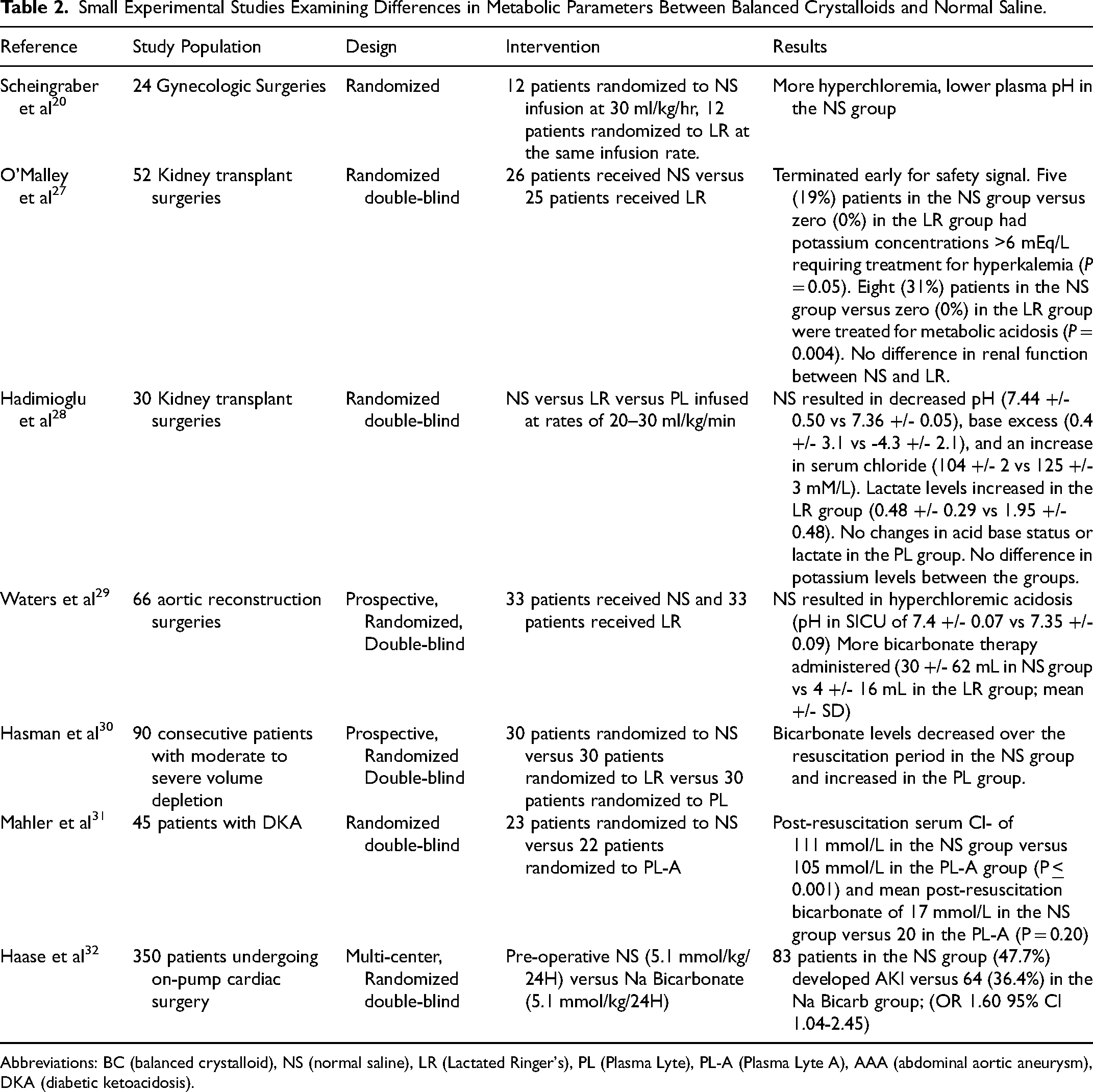
Abbreviations: BC (balanced crystalloid), NS (normal saline), LR (Lactated Ringer's), PL (Plasma Lyte), PL-A (Plasma Lyte A), AAA (abdominal aortic aneurysm), DKA (diabetic ketoacidosis).
Whether the use of different crystalloid solutions may translate to differences in clinical outcomes was initially investigated in several large observational studies (Table 3). Shaw et al performed a retrospective analysis of adult patients who underwent abdominal surgery. The investigators compared 30,994 patients who received only NS with 926 patients who received only BC on the day of surgery. 33 The investigators observed fewer infections, electrolyte disturbances, and a trend toward lower mortality and acute renal failure compared to NS. Another propensity-matched study of critically ill patients with systemic inflammatory response syndrome found that NS was associated with increased in-hospital mortality (3.27% vs 1.03%, P < 0.001), length of stay (4.87 vs 4.38 days, P = 0.016) and cardiac, infectious, and coagulopathy complications (all P values < 0.002). 34 Raghunathan et al evaluated the differences in mortality, acute renal failure, and length of stay between patients admitted to the ICU with sepsis who received either LR or NS. Out of 53,448 patients, only 6.4% were treated with BC. In the matched cohort, receipt of BC was associated with lower in-hospital mortality, but no differences were observed in acute renal failure or length of stay. 35
Observational Studies Evaluating the Differences Between Normal Saline and Balanced Crystalloids on Clinical Outcomes.
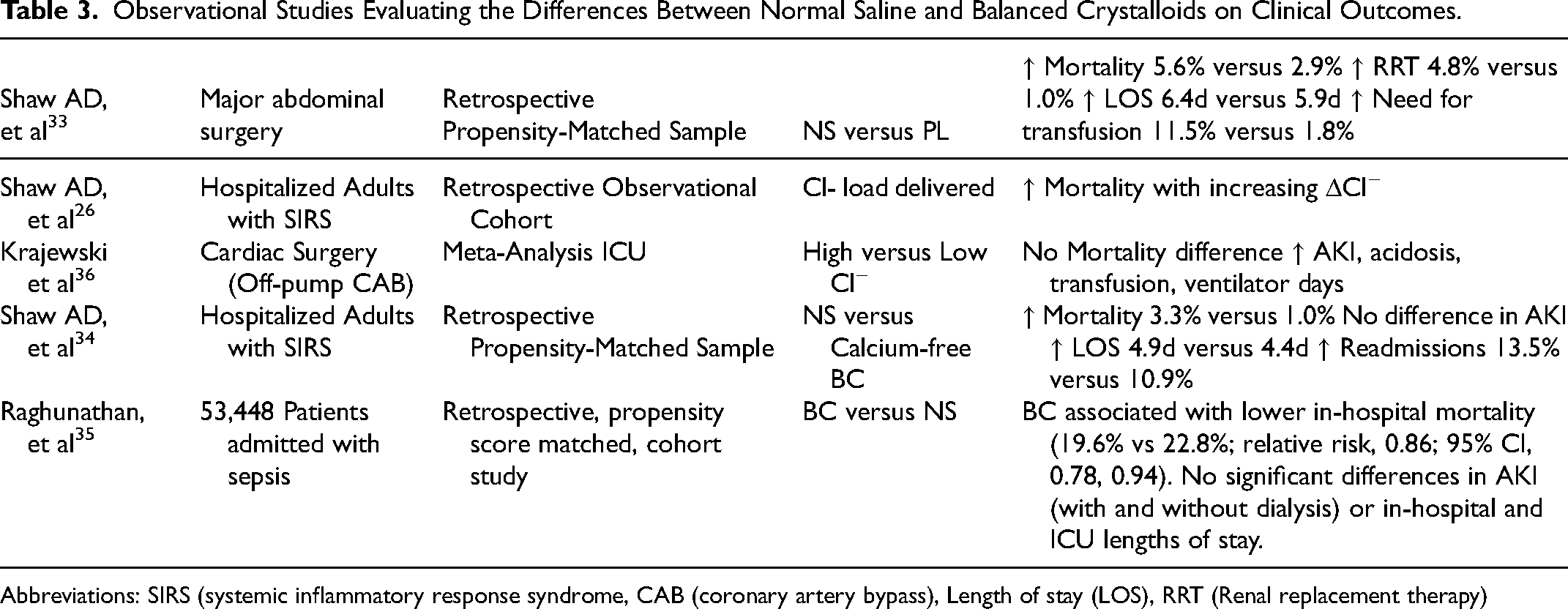
Abbreviations: SIRS (systemic inflammatory response syndrome, CAB (coronary artery bypass), Length of stay (LOS), RRT (Renal replacement therapy)
While these large studies applied rigorous methodologies to address potential confounding by indication, they may not fully account for unique patient or provider characteristics that may explain these differences. Furthermore, the small number of patients who received BC raised potential concerns surrounding generalizability. However, the consistency of the findings and biological evidence indicated by experimental studies ultimately prompted further formal testing.
Clinical Trials
Yunos Study
In 2012, Yunos et al performed a prospective, open-label, sequential period study of 760 consecutive patients admitted to the ICU comparing a chloride-liberal to a chloride-restricted fluid resuscitation strategy (Table 4). 37 The chloride-restrictive strategy was associated with a lower increase in serum creatinine level during ICU stay of 14.8 μmol/L (95% CI, 9.8-19.9 μmol/L) during the intervention period versus 22.6 μmol/L (95% CI, 17.5-27.7 μmol/L) during the control period (P = .03; adjusted P = .007). The incidences of Injury and Failure classes of RIFLE-defined AKI, including renal replacement therapy (RRT), were also more common in the chloride-rich period. Limitations of the study include the non-randomized design, lack of blinding, and potential for secular changes in behavior or provider practices. Further, the bundled nature of the intervention precluded the ability to identify a specific fluid that may have conferred the most benefit.
Notable Trials Comparing Balanced Crystalloids to Normal Saline.
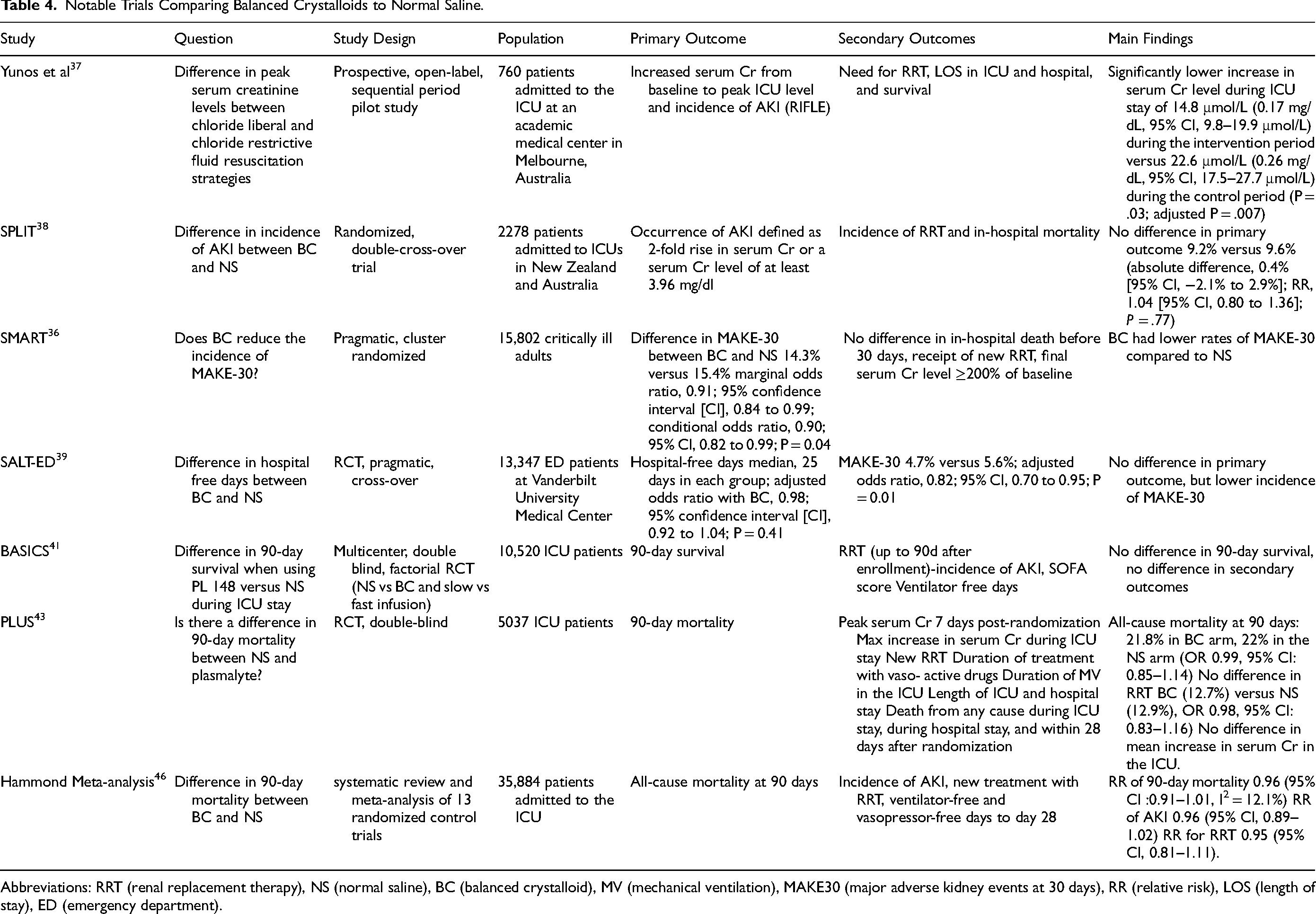
Abbreviations: RRT (renal replacement therapy), NS (normal saline), BC (balanced crystalloid), MV (mechanical ventilation), MAKE30 (major adverse kidney events at 30 days), RR (relative risk), LOS (length of stay), ED (emergency department).
SPLIT
In 2015, Young et al performed the Effect of Buffered Crystalloid Solution Vs. Saline on Acute Kidney Injury Among Patients in the Intensive Care Unit Trial (SPLIT), a randomized, double-blind, crossover trial of 2278 patients conducted in 4 ICUs in New Zealand. 38 The units were assigned to either PL 148 or NS for alternating 7-week treatment blocks. The primary outcome was the occurrence of AKI, defined by the RIFLE classification. Secondary outcomes included the incidence of RRT and in-hospital mortality.
Approximately 70% of the patients were surgical with each group receiving a median of 2 liters of fluid following enrollment. No difference was observed between the two groups for the primary outcome 9.2% (NS arm) versus 9.6% (PL) (absolute difference, 0.4% [95% CI, −2.1% to 2.9%]; RR, 1.04 [95% CI, 0.80 to 1.36]; P = .77), nor the need for RRT, ICU days, hospital days, mechanical ventilation duration, or readmission to ICU. Mortality was observed in 7.6% of the PL group and 8.6% of the NS group (p = 0.4).
Limitations of this study included that each group received a median of one liter of PL prior to enrollment, potentially reducing physiological separation. The focus on feasibility also resulted in no sample size calculations being performed, limiting definitive conclusions on efficacy. Despite the latter, the study established the feasibility of a cluster-randomized, double-crossover design that informed the development of a larger future efficacy study (See PLUS below) and highlighted the importance of fluid administration before enrollment.
SMART and SALT-ED
In 2018, two large, single-center, pragmatic trials were published examining the impact of BC versus NS in critically ill and noncritically ill patients. 39 The SMART study was a pragmatic, multiple-crossover cluster-randomized trial involving 15,802 critically ill adults at a tertiary care hospital admitted to one of five ICUs randomly assigned to use either NS or a BC (LR or PL) on an alternating monthly basis. Participants were enrolled at ICU admission and randomization was coordinated with emergency and operating rooms to minimize receipt of non-randomized fluids. The primary outcome was major adverse kidney event (MAKE30), defined as death, new RRT or an increase in serum creatinine ≥ 200% of baseline within 30 days. 40
The median of 1000 mL (IQR 0-3210 mL) and 1020 mL (IQR 0-3500 mL) of fluid was given for the BC and NS arms, respectively, with only a small number of patients in each group receiving non-study fluids. Plasma chloride concentrations >110 mmol/L and plasma bicarbonate concentrations <20 mmol/L occurred less commonly in the BC than NS groups (24.5% vs 35.6%, P < 0.001) (35.2% vs 42.1%, P < 0.001), respectively. In the BC group, 14.3% experienced a MAKE30 event compared to 15.4% in the NS group (marginal odds ratio, 0.91; 95% confidence interval [CI], 0.84 to 0.99; conditional odds ratio, 0.90; 95% CI, 0.82 to 0.99; P = 0.04). The individual components of MAKE-30 trended toward benefit for BC with the largest differences observed in the mortality (10.3% vs 11.1%, P = 0.06). Stage 2 or greater AKI occurred in 10.7% of the BC arm and 11.5% in the NS arm (p = 0.09).
Simultaneously, the Balanced Crystalloids Versus Saline in Noncritically Ill Adults (SALT-ED) trial enrolled 13,347 patients admitted to non-ICU wards from the emergency department at the same institution. The median volume of crystalloid administered was 1079 mL (IQR 1000-2000mL), with 88.3% of patients receiving only the assigned crystalloid in the emergency room. No difference in the primary outcome of hospital-free days (median 25 days in each group; adjusted OR with BC, 0.98; 95% CI, 0.92 to 1.04; P = 0.41) was observed. Similar to SMART, there was a lower incidence of MAKE 30 (4.7% vs 5.6%, p = 0.01). Patients with a creatinine level greater than 1.5 mg/dL or a chloride concentration > 110 mg/dL appeared to have the most significant benefit. While single-center and non-blinded, these two studies were among the first to demonstrate a modest but rigorous difference in meaningful clinical outcomes such as MAKE30.
BASICS
A subsequent double-blind, two-by-two factorial, multicenter, randomized controlled trial titled Effect of Intravenous Fluid Treatment with a Balanced Solution versus 0.9% Saline Solution on Mortality in Critically Ill Patient (BaSICS) was performed. 41 Two interventions were tested: the type of fluid (NS vs PL) and the speed of infusion (slow 333 ml/hr vs fast 999 ml/hr) in a population of 10,520 critically ill patients enriched for at least one risk factor for AKI (age >65, hypotension, sepsis, mechanical ventilation, early signs of kidney or liver dysfunction).
The volume of fluid administered was greater than in earlier studies (median 2.9 L (SD 2.4 L)). Approximately 18% of patients in the PL arm received at least 1 liter of NS in the 24 h before enrollment. In comparison, 32% of patients in the NS arm received at least 1 liter of PL and approximately 60% of patients received some non-protocolized fluid before enrollment. There was no difference in the primary outcome when stratifying by infusion rate. There was also no difference in the primary outcome of 90-day mortality (26.4% PL vs 27.2% NS, p = 0.47). However, patients with traumatic brain injury (TBI) who received PL experienced higher 90-day mortality compared to NS, 31.3% versus 21.1% (HR, 1.48; 95% CI, 1.03-2.12) in subgroup analysis.
Given the potential effects of pre-enrollment fluid contamination, the authors performed a post hoc analysis using hierarchical Bayesian modeling to examine the impact of the intervention. The analysis was conditioned on the type of pre-enrollment fluid received (PL, NS, mixed, or none). 42 Among patients randomized to the PL arm, mortality rates were 16% among those who received only PL prior to enrollment and 20% among those who received only NS during the pre-enrollment period, translating to a 92% probability of improved mortality, with observed benefit greatest among those with planned admissions and sepsis. Conversely, in those who received NS in the pre-enrollment period, there was only a 39% probability that BC was beneficial. While post-hoc, these observations provided further evidence for a benefit from BC, particularly in patients with sepsis.
PLUS
Finfer and colleagues conducted the Balanced Multi-electrolyte Solution versus Saline in Critically Ill Adults (PLUS) trial in 2022 in 53 ICUs in Australia and New Zealand, a randomized, double-blind trial that assigned critically ill patients to PL 148 or NS. 43 Due to the COVID-19 pandemic, only 5037 patients of 8800 planned participants were recruited. A median of 3.9 liters (IQR 2.0-6.7) and 3.7 liters (IQR 2.0-6.3) of study fluid was administered in the PL and NS arms, respectively. Before enrollment, patients in the PL arm received a median of 624 mL (IQR 28-1700mL) of NS, while patients in the NS arm received a median of 0 mL (IQR 0-80 mL) of BC. After enrollment, 63% of patients randomized to PL received at least 500 mL of NS, and 3.5% of patients randomized to NS received at least 500 mL of PL,though higher plasma chloride concentrations and lower pH were observed in the NS group. All-cause mortality at 90 days was 21.8% in the BC arm and 22% in the NS arm (OR 0.99, 95% CI: 0.85-1.14). There was no difference in new RRT (12.7% BC vs 12.9% NS, OR 0.98, 95% CI: 0.83-1.16) or mean increase in serum creatinine in the ICU.
Other Special Patient Populations
Diabetic ketoacidosis (DKA) and sepsis are clinical scenarios in which large volumes of intravenous crystalloid are given in order to restore hemodynamic stability and correct electrolyte and acid-base disturbances quickly. Therefore, the potential benefits and harms of commonly used crystalloids may be magnified when administered to patients suffering from these conditions. Several post hoc analyses have been performed to identify potential populations of interest where the benefit may be greater. For example, a subgroup of patients from the SALT-ED and SMART trials with DKA were analyzed for time to DKA resolution defined by plasma glucose less than 200 mg/dL and 2 of the following: plasma bicarbonate greater than or equal to 15 mEq/L, venous pH greater than 7.3, and anion gap less than or equal to 12 mEq/L. BC use was associated with faster DKA recovery, shorter insulin infusion duration, and less hypokalemia. 44 Brown and colleagues performed a subgroup analysis of 1641 patients from the SMART trial admitted with a diagnosis of sepsis. They found that patients receiving BC had a lower incidence of MAKE30, more vasopressor-free days, and required less dialysis than did those who received NS. 45
Combining the Data
Hammond and colleagues conducted a systematic review and meta-analysis of 13 randomized controlled trials (11 studies and two conference abstracts) comparing BC with NS in critically ill patients in 2022. 46 A Bayesian approach was leveraged to understand the average treatment effect size and its distribution. The primary outcome was all-cause mortality at 90 days. Secondary outcomes included the incidence of AKI, RRT, ventilator-free and vasopressor-free days up to day 28. From the six trials assessed as having the lowest risk of bias (34,340 participants), the risk ratio for mortality was 0.96 (95% CI :0.91-1.01, I2 = 12.1%), reflecting a treatment effect ranging from a 9% relative reduction to a 1% relative increase in death by 90 days. The latter translated into an 89.5% probability that BC is associated with lower 90-day mortality compared to NS, an effect graded as having a high certainty of evidence. The risk of developing AKI within the low-risk-for-bias studies was 0.96 (95% CI, 0.89-1.02), and the relative risk of needing RRT was 0.95 (95% CI, 0.81-1.11). The authors found no differences in ventilator-free days or vasopressor-free days. In subgroup analysis, the pooled estimates for the relative risk of mortality in patients were 0.93 (95% CI, 0.86 to 1.01; I2 = 22.3%) for sepsis and 1.26 (95% CI, 0.98 to 1.60; I2 = 20.2%) for TBI. Based on these findings, the authors concluded “a high probability that the average treatment effect of using BC is to reduce mortality.”
Potential Concerns of Hyperkalemia with Balanced Solutions
In addition to concerns about using BSs in specific patients (eg, TBI), another area of concern regarding their use has included the risk of hyperkalemia. As balanced solutions contain modest amounts of potassium, caution has been raised about their use in potentially vulnerable populations such as those with evidence of impaired kidney function. One retrospective study of patients with chronic kidney disease (CKD) presenting to the emergency room who received BC found no difference in serum potassium levels. 47 Another single-center retrospective trial of patients with eGFR of <30 ml/min admitted to general medical floors and the ICU, including those with ESKD who had received at least 500 ml of LR found no correlation between serum potassium levels and receiving LR. 48 A secondary analysis of the SMART study examining 187 patients who presented to the ICU with a plasma potassium concentration > 6.5 mmol/L and 1324 with AKI at baseline showed BS was not associated with a higher incidence of severe hyperkalemia (K ≥ 7.0 mmol/L) in patients who were hyperkalemic at baseline (adjusted OR 0.57 (95% CI (0.22-1.46, p = 0.24)) nor among those with AKI at baseline (adjusted OR 0.33 (95% 0.09-1.25, p = 0.10)). 49 Limitations of these studies include a lack of blinding, limited power, and failure to preserve randomization. However, these results were consistent with prior observational data and trial data in patients undergoing kidney transplantation. 50 The mechanism may be due to the relatively low amount of potassium in BS or a greater impact of the acid-base differences on potassium with NS. Regardless, while caution and close monitoring is warranted, these data provide some reassurance that hyperkalemia does not seem to be more common when studied using BC.
What Do Clinical Practice Guidelines Recommend?
The results of the meta-analysis above provided support to the 2021 edition of the Society of Critical Care Medicine's Surviving Sepsis Guidelines, which recommended using BC over NS for resuscitation in sepsis. 3 These recommendations were based largely on the results of the SPLIT and SMART studies, with the evidence graded as weak. More recently, the 2024 European Society of Intensive Care Medicine, incorporating more recent trials and the Hammond analysis, provided a conditional recommendation suggesting BC rather
than NS for volume expansion in critically ill adult patients and patients with sepsis (low certainty of evidence) and in patients with AKI (very low certainty of evidence). Exceptions to these recommendations included patients with TBI (for whom they recommend NS) and cirrhosis (for whom they recommend albumin). 51
Does the Type of Balanced Crystalloid Matter?
Previous studies have found an association between acetate concentrations used in hemodialysis solutions and an increased risk of hemodynamic instability and hypopnea, leading to their being less commonly used in hemodialysis solutions. 52 For fluid resuscitation in non-ESRD patients, this question has been investigated in animal and human studies without evidence to suggest that acetate is associated with an increased risk of hypotension in volumes and concentrations typically used for resuscitation. 53 A systematic review of 27 trials comparing acetate-buffered solutions to NS or lactate-buffered solutions found no incidence of metabolic alkalosis. 54 One study showed a difference in serum lactate levels between lactate versus acetate buffered solutions in patients undergoing reconstructive surgeries; however, there were no differences in electrolytes or pH. 55 Another review of trials comparing lactate to acetate-buffered solutions found no difference in mortality, acid-base abnormalities, hemodynamic parameters, renal function, coagulation, or markers of inflammation. 56 More recently, a single-center study of 2083 critically ill patients found no difference in serum bicarbonate concentrations between patients receiving Normsol-R and LR or statistically significant differences in the risk for dialysis or death at 30 days. 57
By What Mechanisms do Balance Crystalloids Help?
The modest benefit observed with the use of BC has raised questions about whether specific formulations confer greater benefit than others with primary interest on the type of buffer used. In the trials above and Hammond's analysis, the most consistent signal of benefit has been observed through small reductions in mortality rather than AKI. This is surprising, given the mechanistic data that primarily point to physiological effects on the kidney. The latter suggests the potential benefits observed may be through pathways independent of AKI, including the previously mentioned systemic effects of acidosis and inflammation. Future work to identify the mechanisms driving the benefits observed are needed better to support the biological plausibility of the trial findings and identify other potential therapies or solutions that may favorably impact the same pathways.
Summary and Conclusions
Administering crystalloid solutions is one of the most common decisions clinicians make in the hospital. Until recently, this decision was guided by strong opinions with little hard evidence to inform therapy. The recent evolution of the field has exemplified how a pressing therapeutic question can shape clinical practice through a progression of physiologic research, observational studies, and a series of robust clinical trials. The preponderance of that evidence now suggests that balanced crystalloids are more beneficial than normal saline in most critically ill patients (with the potential exceptions of patients with TBI). Uncovering this signal has required substantial resources and the pooling of data from some of the largest critical care trials conducted to date, indicating that the observed benefit is modest with a large number needed to treat. However, given the high frequency of use, the absence of demonstrated harm in most patients, and relative similar costs (ie, at least with LR), we agree with the current clinical practice guidelines favoring the use of BC in most patients with the evidence suggesting that broader implementation can translate into a significant reduction in the number of patients who experience poor outcomes. Ongoing research is needed to clarify the mechanisms of benefit, identify the most responsive patient populations and those who may be harmed, and determine optimal dosing strategies. In the meantime, fluid selection should be individualized to support each patient's perfusion and metabolic needs, and administered with the same care and precision given any other therapeutic intervention.
Footnotes
Author Contributions
TR, NW, JL, and EDS conceptualized the structure of review article.
TR, EDS, NW, JL, and EK performed the literature review.
TR and EDS wrote the first draft of the manuscript with significant input from all authors.
EDS provided supervision at all steps of the literature review and writing process.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EDS has received grant funding from the National Institutes of Health and Department of Veterans Affairs, paid to his institutions. He current receives royalties as an author for UptoDate, and has a current consulting agreement with Novartis, Inc. for service on a Data Safety Monitoring Board, and received an honorarium for an educational talk at the Dialysis Clinics Incorporated Medical Directors Meeting in 2025. He has previously received personal fees serving as Associate Editor for the Clinical Journal of the American Society of Nephrology through 1/24.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.