
Abstract
Introduction
Bronchiolitis is a viral respiratory illness that affects children under one year of age, and its diagnosis is based on history data and clinical evaluation. The natural history of this condition lasts approximately 10-15 days; moreover, most patients do not require hospital care and can be managed at home. However, a small proportion requires hospital admission and, often, early assessment of patients in the emergency department (ED) does not allow a reliable prognosis. 1 Under these premises, over the past 15 years, lung ultrasound (LUS) has demonstrated its usefulness in risk stratification of patients presenting the pediatric ED. In particular, its role has been validated in estimating the risk of being admitted to the hospital or high-intensity care units, receiving supplemental oxygen, or non-invasive ventilation.2–9 However, not all studies reached the same positive and encouraging results, due to the heterogeneity of the patients included, the variability of LUS scores used and the evaluated outcomes. 10 Our aim is to evaluate the predictive value of point-of-care lung ultrasound performed in a Pediatric ED in patients with bronchiolitis; especially for hospitalization, need for oxygen therapy and non-invasive ventilation.
Patients and Methods
A total of 109 patients were enrolled during a 5-month observation period in the ED of Gaslini Children's Hospital (November 2023 - March 2024, pre-Nirsevimab era in Italy), which is a second level pediatric emergency department with more than 35.000 patients/year. This was a monocentric, observational, prospective study and the inclusion criteria were as follows: 1) diagnosis of bronchiolitis, 2) age <1 year at the time of presentation, 3) presence of dyspnea (defined as labored breathing and/or increased respiratory rate) at the time of the visit and 4) a signed informed consent for study participation. Exclusion criteria were as follows: refusing to sign the informed consent, patients affected by a known cardiac or pulmonary disease, severe prematurity (<32 weeks of gestational age), or immunodeficiency. The observational nature of the study, despite the use of ultrasound in addition to the standard of care, is ensured by the irrelevance of the ultrasound results with respect to the patient's management. Enrollment included all the patients eligible for the study presented during regular work shift rotation of three participating physicians. The total number of patients is a convenience sample over a fixed time period. Each participating physician had completed postgraduate specific LUS courses, with at least 5 years of experience in ED point-of-care ultrasound and more than 500 exams performed per year. Patient's median age was 3-month-old and interquartile range (IQR) for age was 2-5 years. The male-to-female ratio was 1.14:1 and 25 patients (23%) were of non-European origin. For each patient, the following data were collected: age, sex, hours since initial symptoms, hours since the onset of dyspnea, clinical score (CS), lung ultrasound (LUS) score, presence of subpleural disventilated areas (SDA), oxygen saturation and pH value in the ED. Moreover, we collected: hospital admission, length of stay, need for and length of oxygen supplementation, need for and length of non-invasive ventilation ((NIV), such as high flow nasal cannula (HFNC) or continuous positive airway pressure (cPAP)), results of respiratory syncytial virus (RSV) test and need for mechanical ventilation. For study's purposes, SDA was defined as a hypoechoic area contiguous to the pleural line, with irregular edges, a maximum depth of less than 25 mm from the pleural line, and no Doppler signals. All patients were treated according to a recently revised internal protocol for bronchiolitis based on international and national guidelines. 11 The CS and LUS score were assigned by three experienced emergency pediatricians participating in this study, using the Wang Bronchiolitis Severity Score and the modified 12-point Basile score, respectively (Figure 1). 5 All lung ultrasounds were performed during ED admission using a portable Mindray TE7 with a linear high-frequency probe and lung preset. Patients were scanned in the supine position for the anterolateral windows and in the prone position for the paravertebral/posterior fields. For the purposes of this study, all lung fields were scanned, with the probe in sagittal plane. The entire examination was considered to assign the final US score. RSV tests were performed using fluorescent immunoassay (SD Biosensor®). Patients’ characteristics are extensively reported in Supplementary Table 1 and compared to local epidemiology of the same period in Supplementary Table 2.
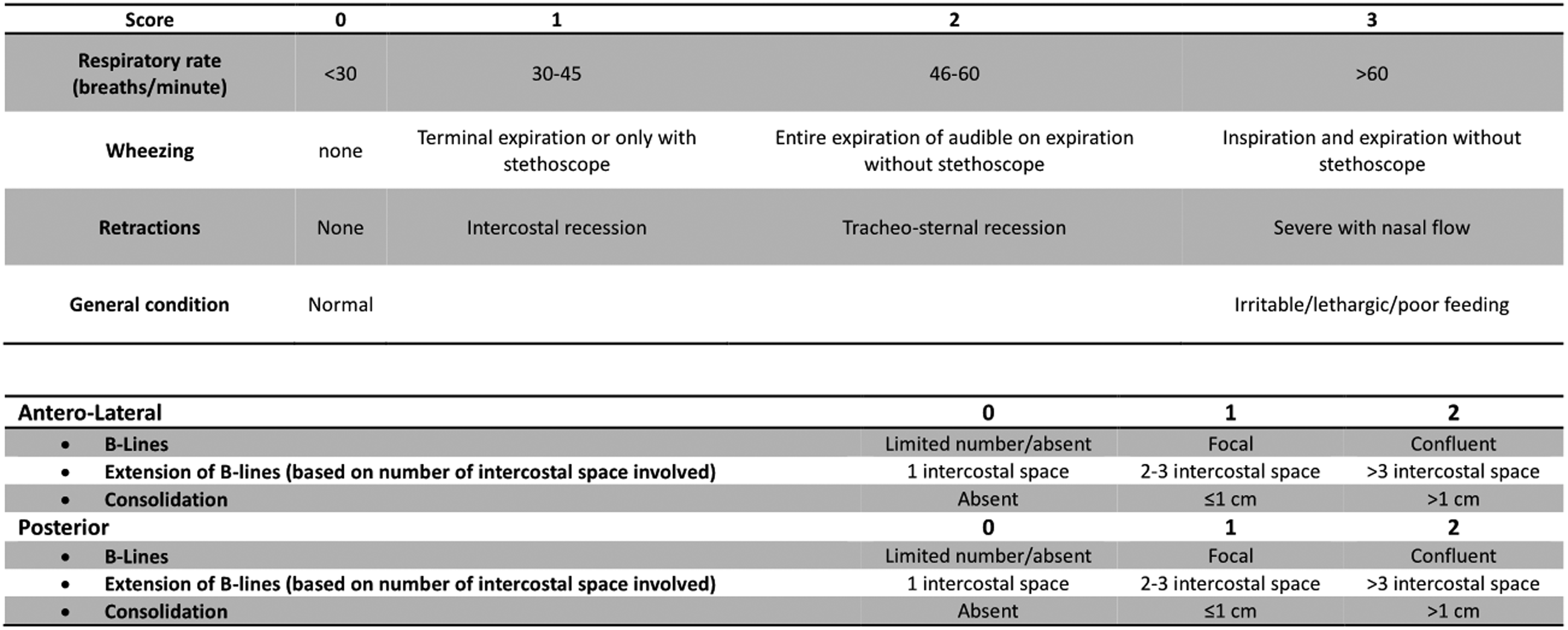
WANG Score (Upper Part) and Modified Basile LUS Score (Lower Part).
Descriptive statistics of the study patients were first performed and reported. Categorical variables were described as absolute frequencies and percentages. Quantitative variables were described as median and interquartile range. Non-parametric tests (Mann-Whitney U test) were used to compare groups for continuous variables. The association between categorical variables was performed using the χ2 test (Chi-Square) or Fisher's exact test, depending on the absolute values. The correlation between quantitative variables was investigated using Spearman's correlation test, while multivariate linear regression analysis was used to estimate the influence of independent variables on a single dependent variable of interest. Logistic regression analysis was used to estimate the risk of an event according to the independent variables. All p-values were estimated using a 2-tailed test with statistical significance set at p < .05. SPSS software (SPSS Inc., Chicago, Illinois, USA) 27.0 was used for all statistical analyses.
This study was previously approved by the Territorial Ethic Committee (CET Liguria #0033837/23).
Results
Patient Characteristics
The median time to ED presentation since symptom and dyspnea onset was 72 h (IQR 48-96) and 6 h (IQR 6-24), respectively. The median Wang clinical score was 4 (IQR 2-5) while the median LUS score was 3 (IQR 1-5). 65 (59.6%) patients were ≤3-month-old at first visit; 71 (65%) patients were admitted and 43 of them (60%) required oxygen supply during hospitalization, while 23 (21.1%) required non-invasive ventilation (HFNC/cPAP). 11 (28.9%) patients among the 38 discharged at the first visit returned to the ED in the next seven days and nine of them were admitted; of these, two patients needed oxygen supply. Two out of 109 patients required intensive care (mechanical ventilation).
LUS Findings
We found a higher median LUS score in hospitalized rather than in discharged ones (4 vs 1 p < .001). Furthermore, comparing the need in oxygen supply and/or NIV among patients who were admitted in hospital, there was a greater median LUS score for those who required oxygen or NIV (4 vs 2 p < .001, 5 vs 3 p < .001 respectively) (Table 1). These results were also confirmed when comparing the presence/absence of subpleural disventilated areas (SDA) with the need of hospitalization, oxygen supplementation and/or NIV (Table 2) (p < .001, p < .001, and p < .04 respectively). In addition, the length of hospitalization and oxygen supply was greater for patients with SDA. Finally, patients classified “mild” according to Wang score (ie WANG score ≤4) had a lower LUS score and less SDA compared to moderate/severe patients (Table 2).
LUS Score.
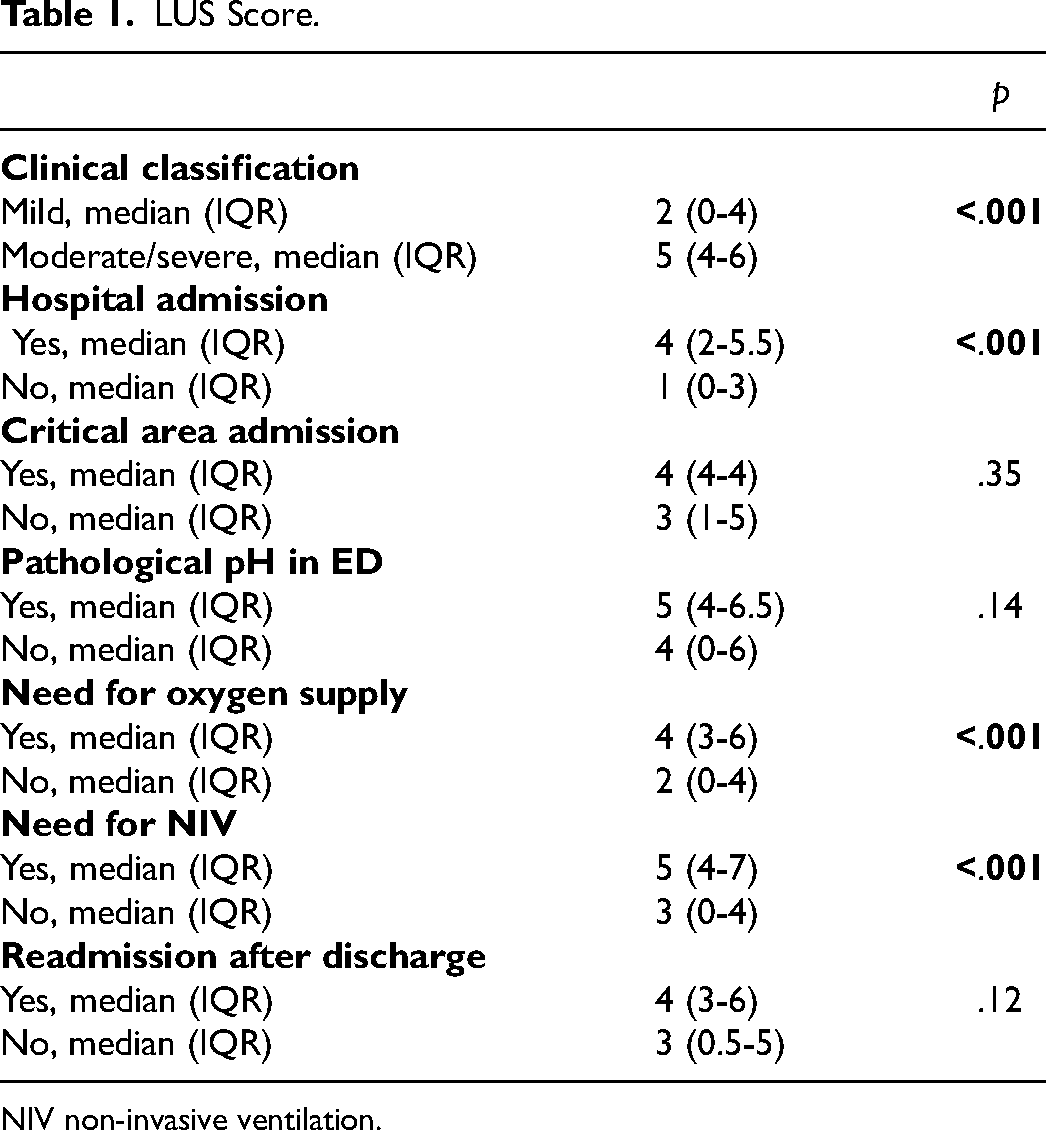
NIV non-invasive ventilation.
Supleural Disventilated Areas.
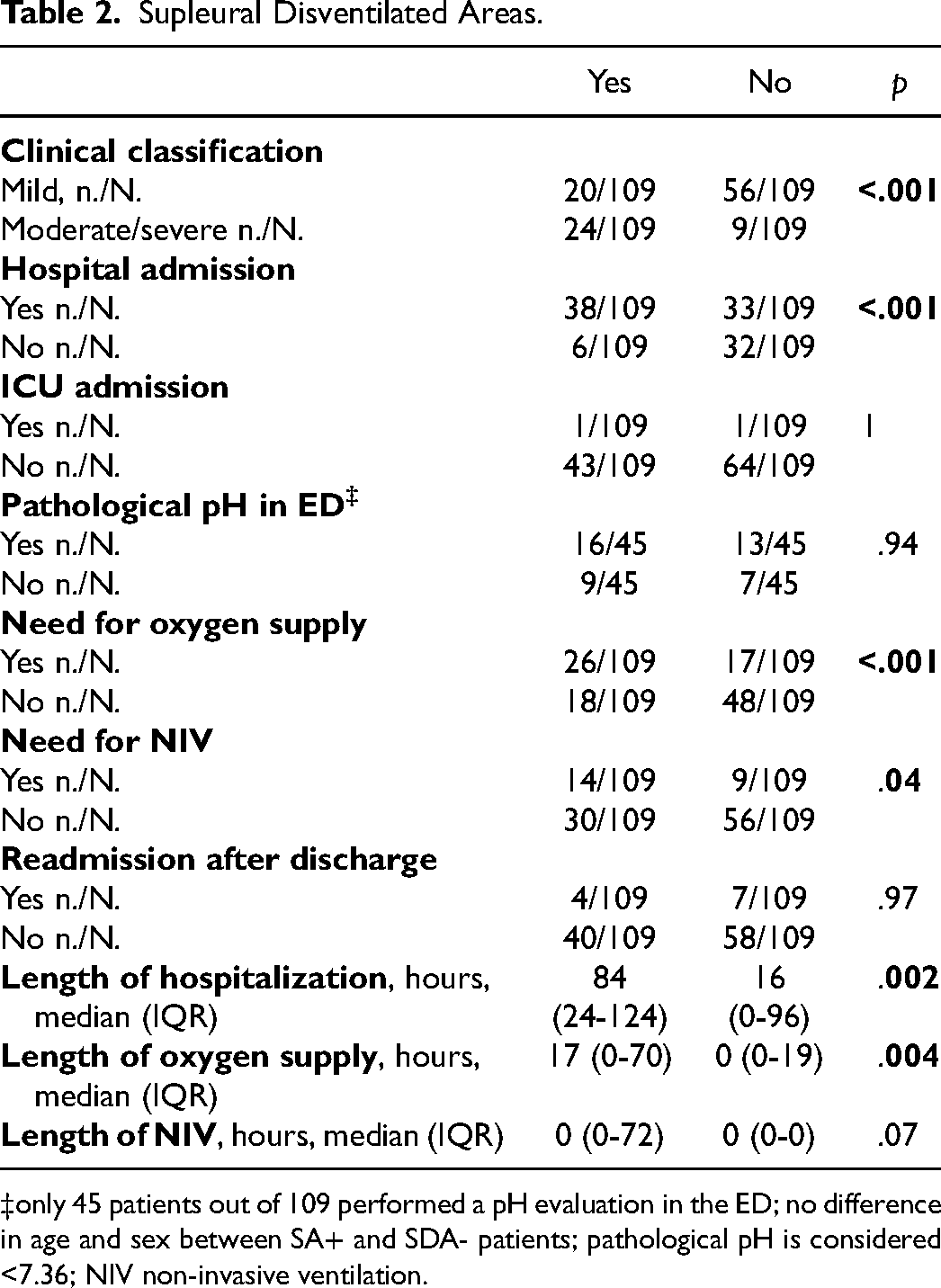
only 45 patients out of 109 performed a pH evaluation in the ED; no difference in age and sex between SA+ and SDA- patients; pathological pH is considered <7.36; NIV non-invasive ventilation.
Etiological Correlation
Furthermore, patients with a positive nasal RSV test required more frequently and longer oxygen supplementation (p < .001 and p = .01, respectively), required more frequently NIV (p < .05) and longer hospitalization (p = .01). No difference was reported for the median LUS score, hospital admission, pathological pH in ED, ICU admission, readmission after discharge and duration of NIV (Table 3).
RSV Antigen Test ‡ .
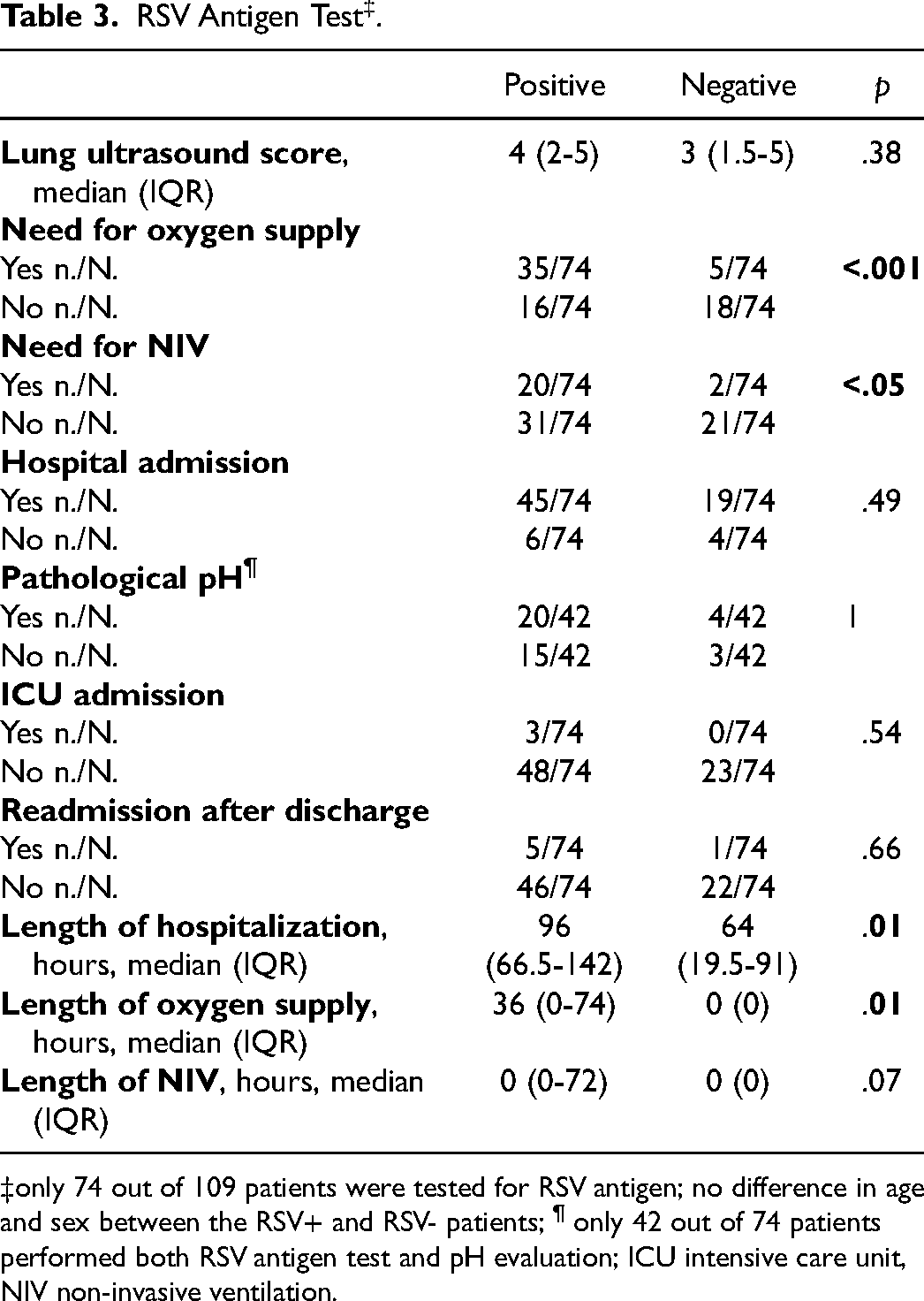
only 74 out of 109 patients were tested for RSV antigen; no difference in age and sex between the RSV+ and RSV- patients; ¶ only 42 out of 74 patients performed both RSV antigen test and pH evaluation; ICU intensive care unit, NIV non-invasive ventilation.
Accuracy of LUS Score
Focusing on the LUS score, the area under the receiver operating characteristic curve (AUC ROC) was calculated for hospital admission, need for oxygen supply and need for NIV. Setting a threshold at 3.5 of LUS score, a sensitivity and specificity of 66% and 84% were obtained for hospital admission (AUC 0.781, CI 95% 0.686-0.877). Moreover, 74% and 68% were sensitivity and specificity for oxygen supplementation (AUC 0.750, CI 95% 0.657-0.843) with a negative predictive value of 80%. Finally, the sensitivity and specificity for NIV were 86% and 61% respectively (AUC 0.798, CI 95% 0.704-0.891) with a negative predictive value of 93%. These data are graphically depicted in Figure 2a to c.

ROC curve for
Predictive Value of LUS Score
To explore the covariance of the LUS score with the main clinical outcomes of interest (length of hospitalization, oxygen supply and NIV), a correlation study using Spearman's test was conducted, without finding any statistically significant results (rs 0.08 p = .49; rs −0.061 p = .7; rs 0.13 p = .56). Similarly, multivariate linear analysis of the aforementioned variables did not show any statistical significance (data not shown).
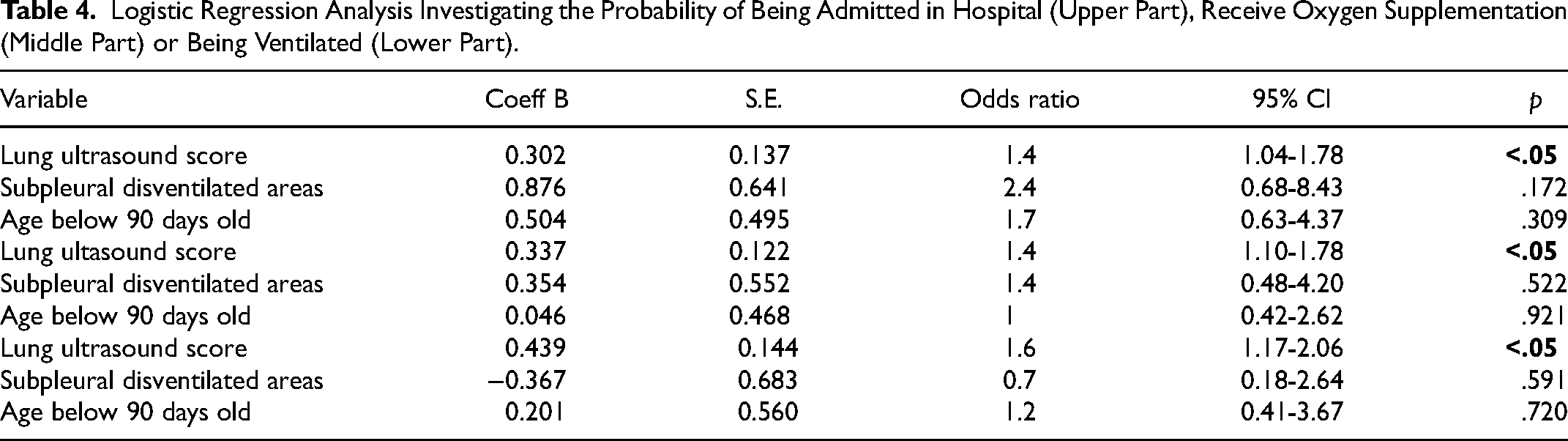
Finally, a logistic regression analysis was performed to explore the probability of being admitted in hospital, receive oxygen supplementation or being ventilated non-invasively. A statistically significance increase in the aforementioned specific risk (OR 1.4, 95%CI 1.04-1.78, p < .05; OR 1.4, 95%CI 1.10-1.78, p < .05; OR 1.6, 95%CI 1.17-2.06, p < .05 respectively) was found for each one-point increase of the independent variable LUS score. No significance was reached using SDA and age less than 90 days old as independent variables (Table 4).
Logistic Regression Analysis Investigating the Probability of Being Admitted in Hospital (Upper Part), Receive Oxygen Supplementation (Middle Part) or Being Ventilated (Lower Part).
Discussion
The aim of this study was to evaluate what clinically relevant information can be obtained from lung ultrasound in patients with bronchiolitis in the ED. Summarizing the relevant results, a higher median LUS score was obtained for both hospitalized patients and those requiring oxygen supplementation or non-invasive ventilation. Even patients who were readmitted to the ED after a previous discharge had a higher median LUS score (assessed at the first visit). In addition, the need for oxygen supplementation and non-invasive ventilation was more common among patients with a positive test for RSV, as expected. Furthermore, the median length of hospitalization and oxygen therapy was longer among these patients, with a nearly significant result also for the duration of non-invasive ventilation. A higher number of SDA was observed in hospitalized patients requiring oxygen or non-invasive ventilation. Moreover, the presence of SDA was correlated with a longer median length of hospital stay and oxygen therapy (with a nearly significant result also for NIV patients). Using a threshold value of 3.5, the LUS score was found to be moderately accurate as a test to assess the need for hospitalization, oxygen therapy, and non-invasive ventilation, notably considering the high negative predictive values for oxygen supply and NIV (80% and 93% respectively). Finally, a higher ultrasound score was associated with an increased likelihood of hospitalization: each 1-point increase in the LUS score contributed to a 1.4-fold increase in the risk of hospitalization and oxygen supplementation, while a 1.6-fold increase in the risk for non-invasive ventilation was reported for each additional point of LUS score.
Several studies have been published in the past 10 years discussing the predictive role of LUS in bronchiolitis, most of them regarding ICU admission, length of hospital stay, need for respiratory support and correlation with clinical course.12–16 For the first outcome, an increased risk of ICU admission has been shown for higher LUS scores, but we did not obtain the same result in our study, probably because of the very small number of ICU-admitted patients. Regarding the length of hospital stay, this study demonstrated a longer hospital stay in patients who had SDA at the US examination performed in the ED compared to the rest of patients. However, it was not possible to establish a strong correlation between the LUS score and the length of hospital stay, presumably because the latter in patients with bronchiolitis with a very low median age depends not only on the patient's respiratory effort, but also on other relevant factors such as the feeding ability, family compliance and the availability of follow-up care. Focusing on the correlation between LUS score and clinical course, we found a worse LUS score in admitted versus discharged patients, as well as in moderate/severe versus mild cases, as reported in the literature.2,5 Moreover, the ability to predict admission is fairly good, although slightly worse than reported in literature (AUC ROC 0.78 vs 0.81). 17 This phenomenon, once again, could be related to the very young age of the patients. No US scan was repeated during the hospitalization; therefore, no data on the evolution of LUS were obtained in our patients. 12 Finally, as reported in the literature, 12 in our cohort, we demonstrated a higher median LUS score and a higher probability of SDA in patients who required oxygen supplementation or non-invasive ventilation during hospitalization In addition, patients with SDA had a longer duration of oxygen supplementation or non-invasive ventilation than other patients. Regarding the ability to predict the need for oxygen therapy or non-invasive ventilation by LUS scanning performed in the ED, the literature contains both data indicating excellent performance 5 and a much lower predictive ability. 10 Our study showed a fairly good AUC ROC of 0.75 with sensitivity and specificity of 74% and 68% for oxygen therapy, and an AUC ROC of 0.8 with sensitivity of 86% and specificity of 61% for non-invasive ventilation. Our results may have a poorer performance because more than half of the patients in our cohort (68 out of 109) had a very early onset of symptoms (dyspnea onset <18 h before ultrasound), with nearly all patients evaluated within one day of symptoms. This condition may have led to an underestimation of the LUS, as the patient may have been evaluated too early in the course of the disease. Nevertheless, a recent study by Thabet et al in patients with HFNC-dependent bronchiolitis found similar AUC, sensitivity and specificity values for the LUS score in predicting the clinical course of the disease. 18
Our study has several strengths. First, to our knowledge, this is the largest dataset of Italian patients ≤1 year of age diagnosed with bronchiolitis, and the median age of 3 months is of considerable importance because it reflects a group of patients with pure bronchiolitis, typical of the first 6 months of life. 19 Moreover, the selected sample is representative of the natural history of the disease: indeed, RSV+ cases have a worse prognosis as expected; moreover, the clinical course of our cohort was comparable to that of patients with bronchiolitis not enrolled within the same period (see Supplementary Table 2). Finally, a 7-day follow-up was recorded for all patients who were monitored for any new hospital admissions and potential subsequent hospitalizations.
Conversely, the three main weak points are related to the monocentric nature of the study with a convenience sample selected over a fixed period of time and the very small number of patients admitted to the ICU. Moreover, the lack of a concordance study among sonographers is another weakness.
In conclusion, LUS examination could be a useful tool in the challenging process of risk stratification for patients under one year of age affected by bronchiolitis and presenting to the ED, although further multicenter studies, with the use of a unique LUS score, are needed to attribute the correct value to the point-of-care ultrasound.
Supplemental Material
sj-docx-1-jic-10.1177_08850666251344465 - Supplemental material for Lung Ultrasound Score and Bronchiolitis: What can be Predicted in a Single Center Experience
Supplemental material, sj-docx-1-jic-10.1177_08850666251344465 for Lung Ultrasound Score and Bronchiolitis: What can be Predicted in a Single Center Experience by Matteo D’Alessandro, Tommaso Bellini, Marta Bustaffa, Benedetta Chianucci, Francesca Ridella, Daniele Franzone and Emanuela Piccotti in Journal of Intensive Care Medicine
Footnotes
List of Abbreviations
Acknowledgments
Not applicable.
Authors’ Contributions
MD conceptualization, investigation, formal analysis, writing original draft; TB investigation, review and editing; MB investigation, review and editing; BC conceptualization, data curation; FR data curation, formal analysis; DF data curation, formal analysis; EP supervision, validation, review and editing.
Availability of Data and Materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was previously approved by the Territorial Ethic Committee (CET Liguria #0033837/23).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.