
Abstract
Background and Objectives
Early recognition and response are paramount in the treatment of neurologic emergencies. Due to its complexity, neurocritical care continues to provoke unease for practitioners and trainees. Simulation provides a realistic opportunity for learners to detect an acutely deteriorating neurologic patient and make rapid-fire treatment decisions. A multidisciplinary simulation-based learning environment may improve trainee confidence when caring for the neurocritical care patient population.
Methods
Nine simulation lab sessions were performed with a multidisciplinary team including medical students, residents, critical care medicine fellows, advanced practice providers (APP), critical care pharmacy residents, and neuroscience unit nurses. High fidelity manikins capable of reproducing acute neurologic and physiologic emergencies were used. After the simulation, participants completed a survey utilizing Likert scale responses regarding simulation logistics, faculty competence, and pre- and post-simulation confidence levels managing specific acute neurologic emergencies and performing neurocritical care procedural skills.
Results
Nine simulation lab sessions were conducted, and thirty-eight surveys were completed. Mean learner confidence levels in managing patients improved from pre- to post-simulation in patients with coma [3.18 ± 0.51 versus 4.32 ± 0.25 (P < .001)], status epilepticus [3.23 ± 0.55 versus 4.36 ± 0.29 (P < .001)], acute ischemic stroke [3.75 ± 0.59 versus 4.63 ± 0.43 (P < .001)], intracerebral hemorrhage [3.25 ± 0.74 versus 4.63 ± 0.43 (P < .001)], intracranial hypertension [3.25 ± 0.74 versus 4.63 ± 0.43 (P < .001)], respiratory failure [3.5 ± 0.77 versus 4.63 ± 0.43 (P = .0016)], and procedures such as central lines [2.2 ± 0.56 versus 3.8 ± 0.56 (P = .003)], intubations [2.25 ± 0.39 versus 3.63 ± 0.62 (P < .001)], and bronchoscopies [2 ± 0 versus 3.2 ± 0.56 (P = .004). Consistently, learners strongly agreed that faculty were knowledgeable, well-informed, and thorough. Learners commented that the simulation experiences were realistic and allowed them to identify areas for improvement.
Discussion
Simulation training can be an effective method to improve neurocritical care education by increasing clinician confidence in managing neurologic emergencies and procedures while providing opportunities for multidisciplinary collaboration. Further evaluation of the effectiveness of simulation education in this patient care setting is warranted.
Keywords
Introduction
Both the American Academy of Neurology and Neurocritical Care Society consider management of acute and critical neurological emergencies to be a learning objective or core curriculum subject.1–3 Historically, neurocritical care has been imparted through concentrated didactic lectures and direct patient exposure, lacking intentional reinforcement of concepts and cases, under supervision. This approach leaves learners with insufficient skills to confidently make high-stakes, real-time clinical decisions in neurological emergencies. 4 Contemporary learners encounter a rapid surge in scientific knowledge, reduced learning opportunities stemming from duty or work hour limitations, swift patient turnover, and an escalated burden of comprehensive documentation within electronic medical records (EMR) 5 which create new challenges in education. Additionally, exposure to neurocritical care exhibits considerable variability, both within the United States and worldwide. Learners often discover that despite spending time in the neurocritical care unit (NCCU) under the guidance of trained neurointensivists, their educational experience remains insufficient6–8 resulting in “neurophobia.”9,10
Simulation education using manikin technology demonstrates value in addressing some of these knowledge gaps. Simulation can foster the development of problem solving, multidisciplinary collaboration, resource allocation optimization, professionalism, teamwork, and communication. 11 Through adequate debriefing and feedback, the benefits of simulation are compounded, when facilitated by a skilled debriefer.10,12 The key features of successful feedback consist of acknowledging the presence of and addressing the cause of discrepancies between learner performance and expected learner actions. 10 Demonstrated to be comparable to patient interactions, this approach offers additional advantages, including prompt feedback and the facilitation of teaching time-sensitive neurocritical care procedures such as central lines, endotracheal intubations, bronchoscopies, external ventricular drains (EVDs), and lumbar punctures (LP).5,13–20 This notion is supported by a study exploring simulation training for LP, showing greater post-simulation proficiency in comparison to bedside training. 14 One year following LP training, residents retained improvements compared to their original pretest score, supporting the long-term benefits of simulation training. 15
As healthcare increasingly embraces multidisciplinary care teams, medical education continues to isolate learners based on provider type outside of the clinical setting. These learners mainly engage with neurocritical care educational content through lectures and independent study, which are less efficient approaches for adult learners compared to simulation.10,21,22 The 2016 NEURON Study demonstrated a demand from neurology residents for education improvements and procedural skill training in neurocritical care. 6 Though an increasing number of institutions implement simulation education, these simulations often encompass individuals or a group of a single learner type, such as residents, medical students or nurses.5,16,23 This type of educational experience does not accurately reflect real-life scenarios faced by a mixed group of frontline providers and may create learning silos; therefore, a multidisciplinary approach is superior.24,25 Additionally, simulation-based, interdisciplinary education alone can improve attitudes toward colleagues in other disciplines, enhancing teamwork and communication skills of learners that will make up future healthcare teams.26,27
The primary aim of this study was to increase confidence of a multidisciplinary cohort of learners in managing acute neurological emergencies. In pursuit of this objective, our intention was to foster learner curiosity regarding topics of interest and prompt self-reflection on their abilities.
Methods
Study Design and Participant Information
This prospective non-blinded study was performed at Cooper University Hospital's simulation center during June 2022-July 2023. This simulation center receives funding from Cooper University Hospital and the affiliated medical school, Cooper Medical School of Rowan University, and there was no cost associated with using the facility for this study. All participants consented to participate in the simulation activities and completed anonymous surveys following their session. All faculty leaders and participants participated voluntarily at no cost to them and received no monetary compensation for their involvement. A total of 38 learners participated in “BRAIN-SIM” simulation lab sessions. Our methodology, as depicted in Figure 1 involved self-directed theoretical learning, followed by active learning through simulation sessions, and concluded with reflection and knowledge consolidation during debriefing.
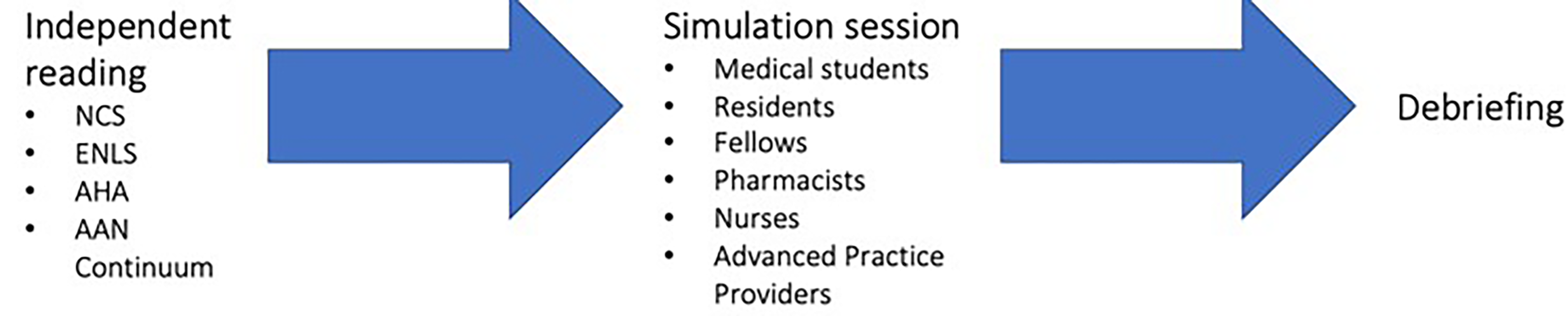
Structure of our multidisciplinary approach to simulation education in neurocritical care.
Participants received pertinent educational material curated from the Neurocritical Care Society, American Heart Association (AHA), Emergency Neurologic Life Support (ENLS), and American Academy of Neurology (AAN) Continuum: Lifelong Learning in Neurology one week before each session. Each simulation session consisted of two clinical scenarios. The group of multidisciplinary learners included a mixture of medical students, neurology residents, neurosurgery residents, advanced practice providers (APP), critical care pharmacy residents, critical care medicine fellows, and neuroscience unit nurses. There were no more than 6 participants per simulation. Teams were not provided instructions for establishing a leadership structure or delineation of individual provider roles.
Cases
A board certified neurointensivist designed all clinical neurocritical care cases for common acute neurological diagnoses including coma, status epilepticus (SE), acute ischemic stroke (AIS), intracerebral hemorrhage (ICH), intracranial hypertension, and cardiac arrest. The clinical cases progressively increased in complexity to replicate real-life scenarios encountered in neurocritical care, facilitating the acquisition, and application of diagnostic and treatment pathways related to neurological diseases (Figure 2). A separate simulation lab was conducted focusing on neurocritical care procedural competencies, including central lines, intubations, and bronchoscopies (Figure 2). For each case, learning objectives, action checklists, and event triggers were predetermined to minimize variability between training events.
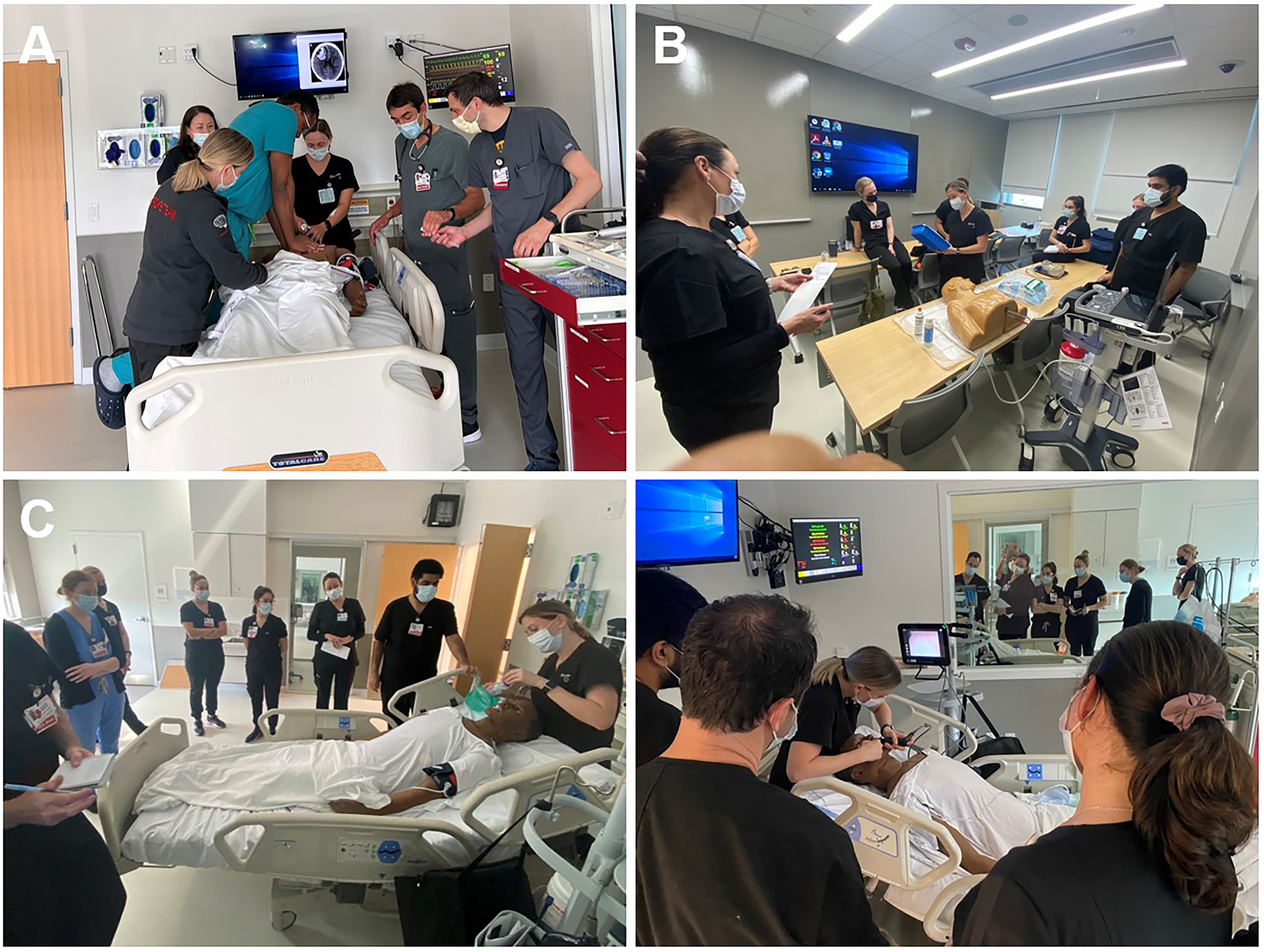
Learners engaging with the simulation experience. A. Care team responding to a cardiac arrest after failing to recognize intracranial hypertension secondary to thrombolytic-related ICH. B. Neurocritical care APP facilitator explaining the equipment and procedural skills involved in central line placement. C. Neurocritical care APP facilitator demonstrating preoxygenation techniques and video guided laryngoscopy.
SimMan 3G Simulation manikins portrayed the patient in cases. The manikins portrayed various relevant exam findings and symptoms including pulse, pupillary responses, tonic-clonic seizures, and changes in respirations. Requested information regarding available patient history or exam findings incompatible with manikin features was conveyed to participants from instructors via microphone, and a monitor displayed key diagnostic studies when requested by learners. Additionally, continuous pulse, respiratory rate, and pulse oximetry were present on a monitor throughout the case with blood pressure readings provided on a cycled rate or as requested by participants. The manikins reported real time CPR quality assessments to the study team leading the simulation.
A pre-brief session lasting approximately 5 min was held to illustrate the purpose of the simulation, objectives, and debriefing process.
Case 1: Status Epilepticus/Coma
In this case, learners responded to a patient in the emergency department (ED) presenting with acute coma because of initial non-convulsive SE, evolving to convulsive SE. High-fidelity manikins capable of reproducing convulsive seizures were used. The case describes a middle-aged man who is found unresponsive on the street by emergency medical services (EMS). He then becomes transiently responsive and combative, followed again by unresponsiveness to noxious stimuli during transportation. Learners are first responders in the ED evaluating the patient. Upon completion of initial assessment and learner tasks, the patient demonstrates convulsive movements, concerning for convulsive SE. This prompts learners to perform rapid sequence intubation and quickly identify and treat SE. The educational goals of this case are for learners to recognize coma, examine a comatose patient, consider possible etiologies including SE and initiate prompt evidence-based treatment plans including checking blood glucose, considering thiamine and naloxone treatment, managing an airway appropriately, providing abortive seizure treatment, and recognizing the need for electroencephalogram (EEG) monitoring.
Case 2: Brain Code, Acute Ischemic Stroke
In this case, learners responded to a patient in the ED presenting with acute left-sided weakness. Learners are first responders, evaluating the patient. Upon successful initial assessment including neuroimaging and administration of a thrombolytic, the patient deteriorates neurologically due to a thrombolytic-related ICH. Depending on learner management choices, the patient either improves or an alternate pathway ensues. In the alternate pathway, neurological decline occurs sooner due to intracranial hypertension and herniation. If intracranial hypertension is not promptly recognized and managed, the patient progresses to cardiac arrest. High-fidelity manikins capable of reproducing pupillary changes were used in this case. In all clinical scenarios, the patient develops acute respiratory failure. The educational goals for this case are to recognize and initiate prompt evidence-based treatment plans for AIS, ICH, intracranial hypertension, impending respiratory failure and cardiac arrest.
Case 3: Procedural Skills
In this case, applicable learners first observed, then practiced procedural training for central line placement, endotracheal intubation, and bronchoscopy. Educational goals consisted of understanding the equipment and procedural kits, describing basic steps of setting up and performing procedures, recognizing common procedural risks and complications, troubleshooting these issues, and recognizing when to call for help.
Assessment of Learners and Simulation Utility
An assessment was created by the study team to assess two categories of simulation training. The first category sought to elicit the participant's perception of their own confidence, and the latter inquired about simulation logistics. Before participating in each simulation activity, learners completed a pre-activity assessment of confidence level with managing a specific acute neurological entity or performing a specific procedure. The learners scored themselves on a 5-point Likert scale. After the feedback session, learners completed the same assessment survey (Supplementary Files 1-3). Regarding the simulation logistics, the assessment solicited a 5-point Likert scale rating regarding the performance of the faculty leaders, the ability of the case to meet the predefined learning objectives, relevance of the case, and timeliness of training exercise. Finally, there was space for additional open-ended comments on the survey (Supplementary Files 1-3).
Debriefing
Debriefing sessions were held for 15 min immediately after completion of the simulation and before post-simulation self-assessments were completed. We utilized a multidisciplinary co-debriefer model, composed of an attending neurointensivist, neurocritical care pharmacist, and neurocritical care APP to deliver debriefing sessions, utilizing the TeamSTEPPS approach created by the Agency for Healthcare Research and Quality.28,29 All cases and debriefing met a minimum faculty to learner ratio of 1:3 fluctuating based on availability of the debrief leaders. The debrief focused on providing a psychologically safe environment, encouraging the use of effective, closed-loop communication. The facilitators established a shared mental model by encouraging a team member to provide a case summary following learner reflections on the simulation, and identification of areas of strength and improvement, while addressing key learning objectives and providing clinical pearls related to the simulation. Key learning objectives included clearly understood roles and associated responsibilities, how and when to ask for and offer assistance, and strategies to keep all team members informed about the care plan. During this period, facts, concepts, principles, and emotional experiences were discussed using open-ended questions as necessary, as well as reflections on how decisions and behaviors uncovered during the simulation related to real-life situations.
Sample Size
Convenience sampling was used to determine the sample size for this study in lieu of a pre-study sample size calculation. Participants included the members of the NCCU clinical team for the day of the study.
Bias
This study minimized bias through participant selection, standardization of simulation cases, participant feedback, and survey collection. Participants were not recruited outside of those who worked or rotated in the NCCU, minimizing selection bias. Standardized simulation cases ensured a consistent difficulty for participants and was coupled with uniform preparation materials and case introduction. For participant feedback, standardized debriefing methodology was utilized. All participants completed the anonymous survey at the end of the simulation minimizing non-responder bias, and time elapsed after the experience was uniform to limit recall bias.
Statistical Analysis
Statistical Analysis was performed using Microsoft Excel version 2306. A paired, two-tailed t-test was performed to compare pre- and post-simulation self-assessment scores. Data is reported as mean ± 95% confidence interval and accompanying p values.
Results
Confidence in Managing Coma and Status Epilepticus
Four coma and status epilepticus case-based simulation lab sessions were completed resulting in twenty-two surveys. From these surveys, the mean pre-simulation confidence level was 3.18 and 3.23 for coma and status epilepticus management, respectively. Mean learner confidence levels in managing neurocritical patients improved by just under 1 point on the Likert scale from pre- to post-simulation with coma [3.18 ± 0.51 versus 4.32 ± 0.25 (P < .001)] and status epilepticus [3.23 ± 0.55 versus 4.36 ± 0.29 (P < .001)] (Figure 3).
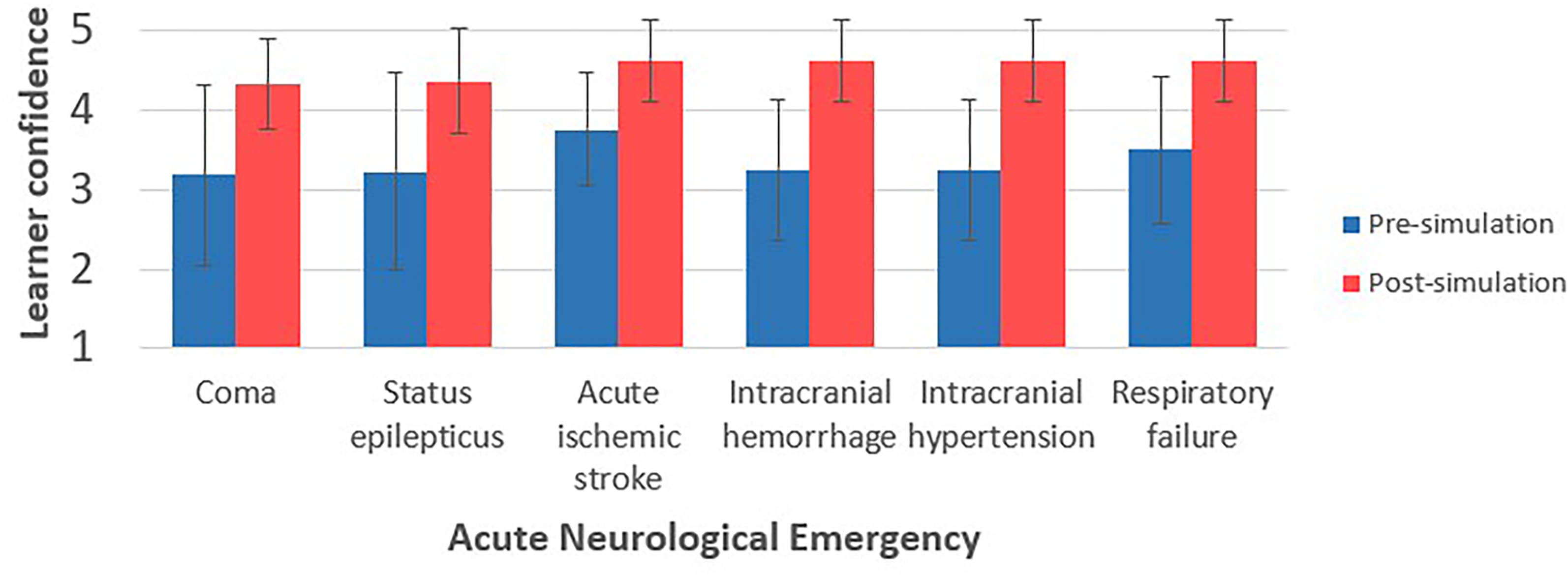
Learner confidence before and after case-based simulation sessions. Learner reported scores range from 1 (lowest) to 5 (highest). Error bars represent standard deviation.
Confidence in Managing Acute Ischemic Stroke and Brain Code
Three acute ischemic stroke and brain code case-based simulation lab sessions were completed resulting in eight surveys. From these surveys, the mean pre-simulation for acute ischemic stroke, intracranial cranial arterial hemorrhage, intracranial hypertension, and respiratory failure were 3.75, 3.25, 3.25, and 3.5, respectively (Figure 3). Mean learner confidence levels in managing neurocritical patients improved by 0.88 to 1.38 points on the Likert scale from pre- to post-simulation with acute ischemic stroke [3.75 ± 0.59 versus 4.63 ± 0.43 (P < .001)], intracerebral hemorrhage [3.25 ± 0.74 versus 4.63 ± 0.43 (P < .001)], intracranial hypertension [3.25 ± 0.74 versus 4.63 ± 0.43 (P < .001)], and respiratory failure [3.5 ± 0.77 versus 4.63 ± 0.43(P = .0016)] (Figure 3).
Confidence in Performing Advanced Procedures
Two skill-based simulation lab sessions were performed, and eight surveys were completed. The mean pre-simulation confidence in setting up and performing central lines, intubations, and bronchoscopies ranged from 2-2.2 on a scale of 1 to 5, with 1 indicating the least confidence and 5 representing the highest confidence (Figure 4). After the simulation, mean learner confidence levels in executing relevant neurocritical procedures improved by at least 1 point on the Likert scale from pre- to post- simulation including central lines [2.2 ± 0.56 versus 3.8 ± 0.56 (P = .003)], intubations [2.25 ± 0.39 versus 3.63 ± 0.62 (P < .001)], and bronchoscopies [2 ± 0 versus 3.2 ± 0.56 (P = .004)] (Figure 4).
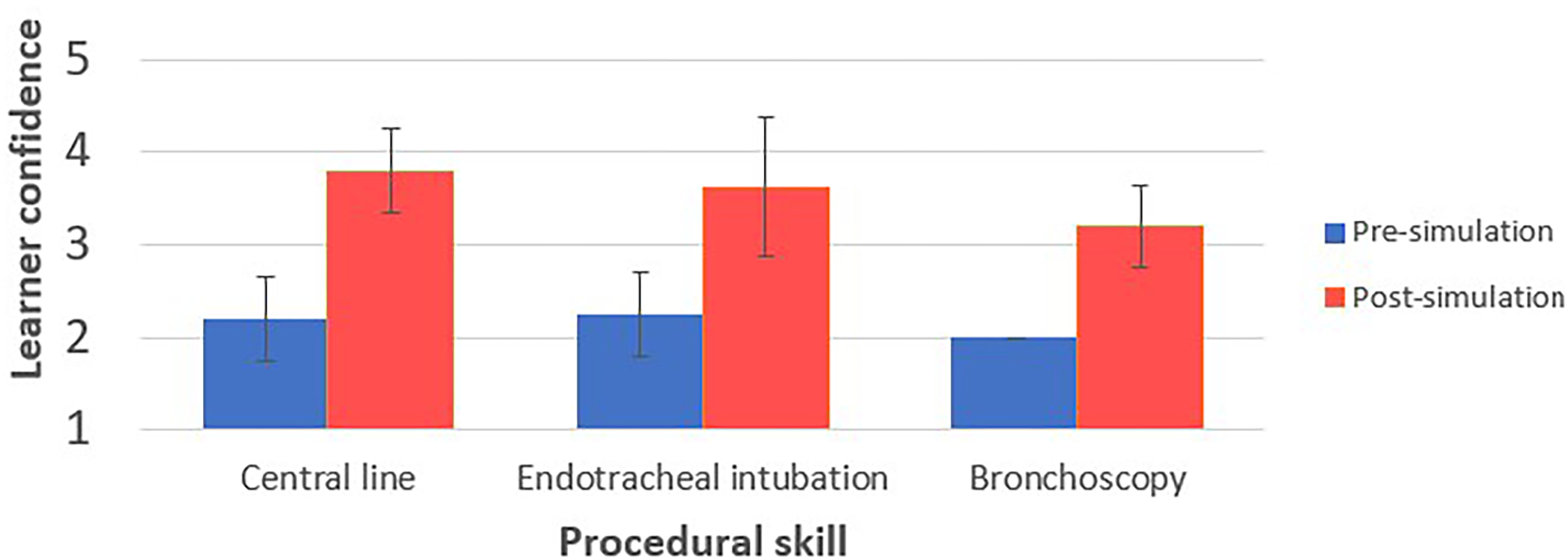
Learner confidence before and after procedural skill simulation sessions. Learner reported scores range from 1 (lowest) to 5 (highest). Error bars represent standard deviation.
Learner Feedback
Both open-ended and Likert scale post-simulation feedback was collected anonymously. All learners agreed that faculty were knowledgeable, and sessions were well-informed and thorough. Moreover, all learners agreed the course objectives were met and the time-allotted for the case and debrief were appropriate. All participants, except for one which was neutral (3), agreed that the case was relevant to their current practice.
Learners commented that they learned from their team and found the multidisciplinary simulation experiences to be realistic and relevant to real-world patient encounters. They unanimously found the cases to be of appropriate difficulty and complexity for their educational level and were able to identify areas for improvement.
Discussion
Self-reported learner confidence consistently increased in the post-simulation survey. This supports the theory that simulation-based education in neurocritical care with a team-based approach is advantageous for multidisciplinary learners. Data regarding the procedural training for ultrasound guided lumbar punctures is excluded from our analysis because of a small sample size of three participants. We used the pillars of observation, action and reflection, described by Lewin, John Dewey and Kolb in developing our simulation structure. 30
Historically, educational approaches in simulation education have often tailored materials to specific learner backgrounds and proficiency levels.10,13,16–18,23,31,32 However, in our study, we took a different approach by employing simulation education to instruct learners with diverse training backgrounds and proficiency levels. Participants in our study consistently recognized the value of this approach, appreciating camaraderie and teamwork within the multidisciplinary team. They observed mutual learning among peers, a departure from pre-established hierarchies, and noted that this approach closely mirrored real-life scenarios. Such an approach aligns with John Dewey's Theory that teaching is most impactful when it is centered around real-world problems, and applicable to practical scenarios. 30 We used an interprofessional group of co-debriefers to maintain relatability to clinical practice and engagement with the multidisciplinary group of learners. 33
Our primary goal was to provide insight and validation for a multidisciplinary approach to medical education in neurocritical care. As medicine becomes more specialized, exposing learners to emergencies in sub-specialties, especially those encountered infrequently, becomes increasingly challenging.7,13 Simulation proved effective in addressing this knowledge gap, offering exposure to both common conditions and rare scenarios while refining management skills in situations where urgent interventions are crucial.24,25 The multidisciplinary approach also encouraged learners from varying educational backgrounds to share their expertise, collaborate and learn from one another. While at times, learners remained in their traditional role such as referring to the pharmacist for medication recommendations. There were also many instances of role switching, especially in groups where not every discipline was represented. This included but was not limited to medical students deciding on medications and residents taking a primary role in resuscitation efforts like chest compressions. The non-hierarchical and role-switching simulation experience familiarized participants with decision making and responsibilities inherent to their colleague's professional roles, which potentially could improve the implementation of flattened hierarchies in critical care settings though that outcome was not explored in this study.
Our secondary goal was to observe the benefits of multiple cases in one study. While the referenced studies out of Northwestern University demonstrated the efficacy of LP training using simulation,14,15 they did not explore the benefits of simulation in other procedures or management of neurocritical emergencies. The benefits of simulation training have been demonstrated in acute stroke codes.23,25 We expanded on this work by exploring the benefits of simulation in an acute stroke case and a status epilepticus case. Moreover, the importance of APP simulation education in neurocritical care compared to residents has been explored, 23 but unlike our study, does not elucidate the benefits of APP simulation when working alongside residents and other learners.
In addition to bolstering confidence in managing neuro-emergencies, our hope was to spark interest among learners in pursuing careers that involve such cases. In addition, engaging in simulation education offers a psychological benefit for learners, enabling learners to make errors and learn from them without the fear of causing harm to an actual patient. 9 This approach also helps them improve speed of decision-making in critical situations.10,34
While we observed a notable change in pre-simulation and post-simulation learner confidence, this study may be improved by objective evaluation of learners over time and with repeated simulations. This may provide valuable insights into the long-term benefits of simulation-based education. However, the utility of self-confidence as a measure should not be understated. As outlined in the Social Cognitive Theory, cognitive factors, behavioral factors, and environmental factors influence each other.35,36 In this framework, a high sense of self-confidence can lead to observed improvements in cognitive performance and increased resilience.35,36 A study evaluating self-confidence in surgical trainees found that trainees with higher self-reported confidence correlated positively with receiving higher score on the global rating scale of surgical skill by their attendings. 37 Furthermore, the increased resilience may support participants’ interest and motivation in careers in neurocritical care despite the previously outlined sentiment of neurophobia among trainees in the field.
The current literature on this topic ranges from single center studies to meta-analyses which all greatly benefit the neurocritical care community's fund of knowledge regarding simulation education impact on AIS and SE management.38–43 Four studies over the past decade studying door to needle (DTN) time in AIS have shown the benefits of simulation education.38,39,41,43 One meta-analysis and one quality improvement project conclude a decrease in DTN time as a result of both changes in hospital protocols and simulation education but do not reliably control for one variable versus the other, whereas this study only evaluates the effects of simulation education.38,39 A study evaluating an AIS simulation curriculum for first year neurology residents demonstrates decreased hospital-wide DTN times compared to historical controls and reflects real-life situations by requiring the residents to respond to a beeper activation instead of starting on-scene. While this study offers valuable insights, it does not sufficiently describe the results for the nursing participants it references in the methodology. 41 Additionally, a strength of our study not seen in similar AIS simulation research is the response to ICH after thrombolytic administration and a multidisciplinary response to potential adverse effects of thrombolytics. While two studies exploring SE management offer promising objective measurements for learners, neither matches our study's multidisciplinary approach.40,42 The robust objective measurements for learners could lend itself as a guide for a future study evaluating a multidisciplinary team on role specific competencies.
As multidisciplinary learners, the metrics and assessments used to evaluate participants vary by professional role, which poses an obstacle for objective measurement. However, given the current voluntary participation design, patient outcomes would not be an appropriate measure as simulation exposure by participant and confounders such as consultants or teams consisting of neurocritical care providers who did not participate in simulation events would be too prevalent. The most practical solution in future research is to implement a pre and post-test regarding pertinent course content that is relevant to all disciplines or repeat simulation cases with a standardized checklist of provider objective and evaluate for improvement in performance between attempts. Another avenue to assess patient-based outcomes would be to randomize simulation involvement of neurocritical care providers and track patient outcomes for those providers, which may also increase our number of participants. Though it would remain difficult to appropriately attribute outcomes to providers’ simulation experience given the length of stay and number of providers involved in the care of neuro-critically ill patients.
Reflecting on the strengths and weaknesses of this study, there is an opportunity to further bolster the procedural skill findings in this study. Previously published work evaluated central line insertion skills learned and practiced through simulation by measuring resident procedural success in the clinical setting. 19 Additionally, a meta-analysis of bronchoscopy simulation called for additional high-quality research correlating simulated bronchoscopy training with patient outcomes and clinical performance. 20 These studies demonstrate a need for further research in procedural skills training through simulation and in subsequent studies the presented simulation curriculum can be modified to better measure clinical outcomes.
Limitations of this study include small sample size, exclusive implementation at a single institution, and the use of expensive, high-fidelity manikins, which hinder generalizability. These challenges are common in simulation education, particularly in neurocritical care. A large multi-center study would provide more comprehensive insights into the benefits and optimization of simulation education for residents, APP's, fellows, medical students, and other healthcare providers. Because this study implements a convenience sampling approach, no formal sample size calculations were conducted prior to the study. As a result, our true sample size may not include the optimal number of patients to power the study. While our participants likely benefited from training with high-fidelity manikins, these simulation tools may be prohibitively expensive for other departments looking to implement simulation training. The SimMan 3G Simulation manikin used in the cases has an estimated cost of $115 000 with a $7000 per year warranty and simulation manikins for specific procedures such as central line and bronchoscopy training cost an estimated $1000-4,000, which may pose a significant financial burden to groups looking to replicate these cases. We encourage hospital systems, schools, and departments interested in pursuing high-fidelity simulation to pursue grant funding through one of many avenues including the U.S. Department of Education Modeling and Simulation Program and the Nursing Education, Practice, Quality, and Retention (NEPQR)’ s Simulation Education Training program.44,45 The value of multidisciplinary simulation training often extends into the team dynamic and understanding roles, 26 which participants can acquire with less advanced simulation technology.
The design of this study sought to reduce bias and promote clinically applicable conclusions. One way in which this was achieved was through participant recruitment of the clinical team in the NCCU on the day of simulation. By imitating the multidisciplinary team structure in a typical NCCU, the results of this study help reflect the practice environment familiar to most providers and learners. 46 Additionally, this strategy minimized selection bias by not recruiting participants with a specific interest in simulation participation, as volunteers may answer surveys more favorably. Finally, the pre-post study design eliciting only participant perception of confidence is subjective and can vary by individual.
In addition to the specific outcomes highlighted in this study, our research aims to make a significant contribution to the expanding body of evidence supporting simulation education in neurocritical care. This overarching goal emphasizes our commitment to advancing educational practices, ultimately aiming to bolster the proficiency and confidence of healthcare professionals in effectively managing neurocritical conditions.
Conclusion
In conclusion, multidisciplinary simulation training using clinical cases and advanced procedures can effectively address crucial neurocritical care learning gaps for learners of various disciplines. The observed increase in self-reported confidence among participants provides objective evidence of the benefits derived from this approach. Future large prospective studies should continue to evaluate the most efficient and practical way to incorporate this training into neurocritical care training programs.
Supplemental Material
sj-doc-1-jic-10.1177_08850666251327156 - Supplemental material for BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach
Supplemental material, sj-doc-1-jic-10.1177_08850666251327156 for BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach by Brett DerGarabedian, Lauren Lacovara, Justin Delic and Swarna Rajagopalan in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-2-jic-10.1177_08850666251327156 - Supplemental material for BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach
Supplemental material, sj-docx-2-jic-10.1177_08850666251327156 for BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach by Brett DerGarabedian, Lauren Lacovara, Justin Delic and Swarna Rajagopalan in Journal of Intensive Care Medicine
Supplemental Material
sj-docx-3-jic-10.1177_08850666251327156 - Supplemental material for BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach
Supplemental material, sj-docx-3-jic-10.1177_08850666251327156 for BRAIN-SIM: Leveraging Simulation for Neurocritical Care Education with an Innovative Multidisciplinary Approach by Brett DerGarabedian, Lauren Lacovara, Justin Delic and Swarna Rajagopalan in Journal of Intensive Care Medicine
Footnotes
Author Contributions
Brett DerGarabedian: Data curation, formal analysis, visualization, writing – original draft. Lauren Lacovara: Conceptualization, data curation, investigation, methodology, methodology, resources, writing – review & editing. Justin Delic: Conceptualization, investigation, methodology, resources, writing – review & editing. Swarna Rajagopalan: Conceptualization, investigation, methodology, project administration, resources, supervision, writing – review & editing.
Consent to Participate
Informed consent was obtained verbally from all individual participants in the study.
Consent for Publication
Not applicable
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Anonymized data will be shared by request from any qualified investigator.
Ethical Considerations
The study qualified for an exemption per the Cooper University Hospital Institutional Review Board. The analyzed data set did not include data on participant demographics except for level of training and clinical role.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.