
Abstract
Objective
Elevation of Troponin I (TnI) in spontaneous subarachnoid hemorrhage (SAH) patients is a well-known phenomenon and associated with cardiopulmonary complications and poor outcome. The present study was conducted to investigate the association of the TnI value on admission, and the occurrence of cerebral vasospam in SAH patients.
Patients and Methods
A total of 142 patients with SAH, who were admitted to the neurosurgical intensive care unit (ICU) between December 2014 and January 2021 were evaluated. Blood samples were drawn on admission to determine TnI value. Each patient's demographic, radiological and medical data on admission, the modified Ranking Scale score at discharge as well as continuous measurements of transcranial Doppler sonography were analyzed. A maximum mean flow velocity (MMFV) > 120 cm/sec was defined as any vasospasm. These were stratified into severe vasospasms, which were defined as at least two measurements of MMFVs > 200 cm/sec or an increase of MMFV > 50 cm/sec/24 h over two consecutive days or a new neurological deterioration and mild vasospasm defined as MMFVs > 120 cm/sec in absence of severe vasospasm criteria. The total study population was dichotomized into patients with an initially elevated TnI (>0.05 µg/L) and without elevated TnI (≤0.05 μg/L).
Results
A total of 52 patients (36.6%) had an elevated TnI level upon admission, which was significantly associated with lower GCS score (p < 0.001), higher WFNS score (p < 0.001) and higher Fisher grade (p = 0.01) on admission. In this context a higher rate of ischemic brain lesions (p = 0.02), a higher modified Rankin Scale score (p > 0.001) and increased mortality (p = 0.02) at discharge were observed in this group. In addition, TnI was identified as an independent predictor for the occurrence of any vasospasm and severe vasospasm.
Conclusion
An initially elevated TnI level is an independent predictor for the occurrence of any and severe vasospasm in patients with SAH.
Introduction
Cerebral vasospasm is known as one of the major factors for poor outcome and mortality after spontaneous subarachnoid hemorrhage (SAH).1–4 Especially, within the first 14 to 21 days after SAH, cerebral vasospasm can cause delayed cerebral ischemia (DCI) and vasospastic-related ischemic brain lesions in up to 30% of all SAH patients.5–11 Early identification and treatment of cerebral vasospasm is a cornerstone in intensive care unit (ICU) treatment of SAH patients.12,13 In daily practice, Transcranial Doppler sonography (TCD) is frequently performed to detect cerebral vasospasm. TCD is a non-invasive method for indirect measurement of the presence of cerebral vasospasms, which are caused by intracranial arterial vasoconstriction.1,3,7 Several studies define a maximum mean flow velocity (MMFV) > 120 cm/s as vasospasm.1,3,8,14,15 Nevertheless, TCD can only detect the presence of vasospasm, but not identify patients with an increased risk for the occurrence cerebral vasospasm. Therefore, the use of serum biomarkers upon admission could be helpful for an early identification of SAH patients with a high risk for cerebral vasospasm. These patients may benefit from an early more invasive cardiopulmonary and/or cerebral monitoring and intensive blood pressure management.
Elevation of the cardiac enzyme Troponin I (TnI) is a well-known phenomenon in up to 20-40% of all SAH patients, although the pathophysiological pathway is not completely understood.15–19 Several studies reported about the association between elevated TnI level and higher Hunt-Hess grade, higher WFNS grade, lower GCS score, poor outcome as well as cardiopulmonary complications in SAH patients.16–20 However., the association of elevated TnI and the occurrence of TCD-defined cerebral vasospasm is only scarcely described.18,20,21
Therefore, we investigated the value of TnI to predict the occurrence of TCD-defined cerebral vasospasm among neurosurgical patients with SAH.
Material and Methods
Study Design and Patients
The current study analysed all patients with SAH who were treated from December 2014 to January 2021 at our neurosurgical intensive care unit (ICU) for at least 24 h. TnI was determined from the blood sample upon admission. The study protocol was approved by the Ethics Committee of Justus-Liebig-University, Giessen, Germany (No. 81/21). Patients with SAH due to head trauma or brain tumors, acute cardiac and/or pulmonary decompensation, and patients aged less than 18 years were excluded. The diagnosis of SAH was made by computed tomography (CT) scan or lumbar puncture in case the CT scan was negative for SAH.
Methods
The baseline data, including sex, body mass index, age, Glasgow coma scale (GCS) scores and World Federation of Neurosurgical Societies (WFNS) scores, and duration of hospital stay, as well as TnI and additional serum biomarkers, comorbidities, premedication, radiological data including Fisher grade and localization of an aneurysm on admission were extracted from the patientś electronic medical records. In addition, treatment regime, the occurrence of TCD-defined vasospasm, DCI, ischemic brain lesions, inhospital mortality and the modified Rankin Scale score at discharge were evaluated in all patients.22–24
The initial TnI level in µg/dL (ADVIA Centaur XPT®, Siemens, Germany) was determined from the blood sample taken at the emergency department (ED) upon admission. At the ED of internal medicine and neurology, testing of TnI was routinely performed in all patients (conservative blood sample spectrum). Testing of TNI at the surgical ED, was only performed, if it was clinically indicated (eg, decompensated heart failure, angina pectoris, or ST segment elevation/depression in the electrocardiography [ECG]). All patients with raised TnI level upon admission underwent immediate ECG and echocardiography. Patients with cardiac wall motion abnormalities or electrocardiogram changes in combination with initial elevated TnI level, as indicator of a real cardiac decompensation, were transferred to the angiography and excluded from the study, if a coronary artery stenosis was found. Elevation of TnI level in the absence of suspicious ECG and/or echocardiography changes and/or angina pectoris and/or with a coronary stenosis were interpreted as brain triggered. Serial measurements of TnI were not done based on the lack of consequence. Furthermore, blood glucose levels in mg/dL (ADVIA Chemistry XPT®, Siemens, Munich, Germany), the white blood cell count in giga/L (XE 5000 Hematology Analyzer, Sysmex, Norderstedt, Germany), hemoglobin level in g/dL (XE 5000 Hematology Analyzer, Sysmex, Germany), hematocrit level in % (XE 5000 Hematology Analyzer, Sysmex, Germany), were assessed as additional serum biomarkers in all SAH patients.
Comorbidities comprised the presence of coronary artery diseases, chronic arterial hypertension, diabetes mellitus and history of stroke or traumatic brain injury. Additionally, the long-term intake of beta-blockers, diuretics, antidiabetics, antihypertensive, antidepressant and antiplatelet agents as well as vitamin K antagonists and new oral anticoagulants were defined as premedication. The Fisher grade was evaluated from the initial CT scan at admission. A digital cerebral angiography and/or CT angiography was carried out in all included patients to confirm and localize or exclude the evidence of an aneurysm. Ischemic brain lesions were defined as new hypodensities on CT scans. Patients with surgical and/or interventional related brain lesions were excluded from the analysis of secondary brain lesions. DCI was defined as the occurrence of a new neurologic focal deficit or deterioration of consciousness, which could not be explained by other causes than vasospasm. All data were reviewed by two independent neurosurgical consultants (M.B. and E.U.).
Transcranial Doppler Sonography and Vasospasm
TCD measurements were performed daily by one experienced medical technician from days 1 to 21 after ictus of SAH or to the end of the ICU treatment with a 2 MHz-range gated pulsed Doppler ultrasound Multi-Dop X ® digital (Compumedics, Singen, Germany). In case of absence of the medical technician, TCD measurement was done by an experienced neurosurgical consultant. A transtemporal approach was routinely used for all TCD measurements and recorded in centimeters per second (cm/s) in a TCD database. A maximum mean flow velocity (MMFV) > 120 cm/s on TCD was defined as any vasospasm in all SAH patients (TCD-defined vasospasm). These patients were stratified into patients with mild vasospasm and severe vasospasm. Severe vasospasm was defined as at least two measurements of MMFV > 200 cm/s or an increase in the MMFV > 50 cm/s/24 h over two consecutive days or the occurrence of a new neurological deficit. Mild vasospasm was defined as a MMFV > 120 cm/s and the absence of criteria for severe vasospasm. The vasospasm period was defined as the time-period from the first detected MMFV > 120 cm/s until it’s normalization.
General ICU Treatment
All patients were treated at the neurosurgical ICU. In general, all aneurysms were treated surgically or/and endovascularly within the first 24 h upon admission. An external ventricular drain or lumbar drain was placed in case of hydrocephalus. In addition, invasive blood measurement systems (Combitrans Monitoring Set Arteriell, B. Braun, Melsungen, Germany) and central venous catheters were implemented routinely (Arrow International, Inc., Reading, USA) in all patients. Endotracheal intubation and mechanical ventilation (Servo-I, Maquet, Rastatt, Germany) were initiated in patients with a GCS score lower than 9 or if the patient developed cardiopulmonary insufficiency. All patients received nimodipine intravenously (2 mg/h) for at least 14 days regardless of TCD velocities. The initial systolic blood pressure of each patient was maintained at <140 mm Hg. The systolic pressure was raised to 140-160 mm Hg after aneurysm occlusion or after 24 to 48 h in all patients with no evidence of an aneurysm in the cerebral angiography and/or CT. In general, hypertensive treatment for was initiated depending on the occurrence of vasospasm with a systolic blood pressure >10 mm Hg over MMFV until a maximum of 200 mm Hg. The target for mean hemoglobin values was >10 mg/dl and 30-34% for hematocrit. 25 The indication for interventional anti-vasospastic treatment (intra-arterial application of nimodipine) was a therapy refractory increase of MMFV >50 cm/s within 24 h and/or an MMFV >200 cm/s, in consideration of actual intracranial pressure and cardiopulmonary function.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) version 15.0 for Windows (Version 15.0; SPSS Inc., Chicago, IL, USA) was used for data analysis.
The total study population was dichotomized into patients with a TnI value >0.05 μg/L (TnI positive) and those with a TnI value ≤0.05 μg/L (TnI negative) for analysis of the association between TnI level and vasospasm. Parameters with normal distributions are expressed as mean ± standard deviation and the median and interquartile range (IQR) were used for non-normal distributed parameters. The univariate analysis was performed using Mann–Whitney U-Test or the Student's t test and the Chi-square test to identify differences between both groups. A p-value of <0.05 was defined as the level of significance. Furthermore, a binary logistic analysis with a forward stepwise method was used to identify independent predictors for the occurrence of any vasospasm, mild vasospasm and severe vasospasm.
Results
Main Characteristics
The entire study population comprised 142 patients (91 women and 51 men) with a mean age of 58.6 ± 12.5 years (range: 28-85 years). Upon admission, the median WFNS score was 3 (IQR:1-5) and the median GCS score 13 (IQR:3-15). The median length of inpatient treatment was 31 days (IQR:20-45). Chronic arterial hypertension (49.3%) and antihypertensive drugs (31%) were the most common comorbidity and premedication. The median Fisher grade upon admission was 4 (IQR:1-4). Anterior communicating artery (25.9%) was the most common localization of cerebral aneurysm, followed by middle cerebral artery (25%). Moreover, 26 patients (18.3%) had no aneurysm. Clipping was performed in 43 (37.4%) patients, and endovascular treatment in 66 (57.4%) patients. The median mRS at discharge was 3 (IQR:0-5) and 14 patients (9.9%) died during the hospital stay (Table 1).
Baseline data and univariate analysis.
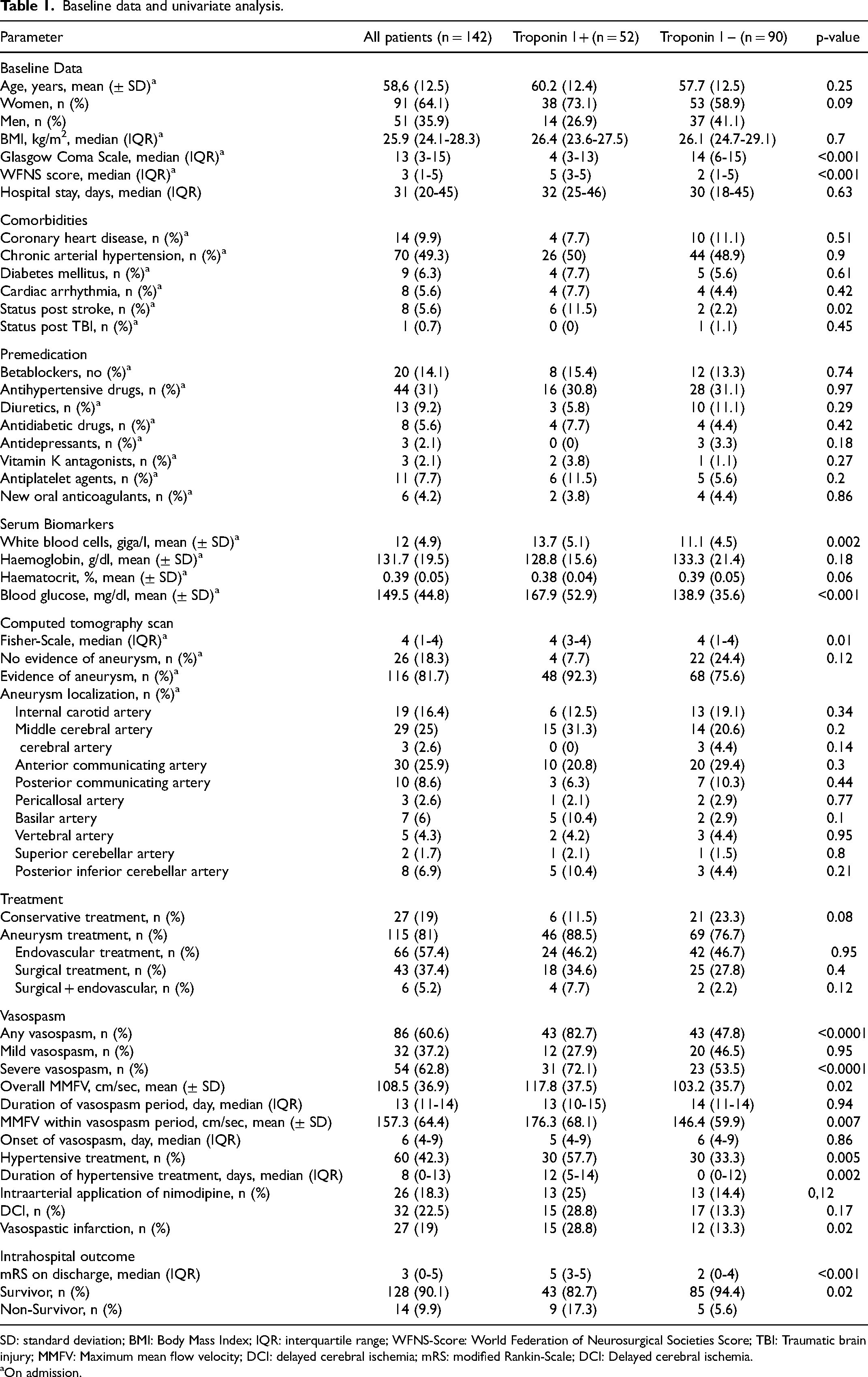
SD: standard deviation; BMI: Body Mass Index; IQR: interquartile range; WFNS-Score: World Federation of Neurosurgical Societies Score; TBI: Traumatic brain injury; MMFV: Maximum mean flow velocity; DCI: delayed cerebral ischemia; mRS: modified Rankin-Scale; DCI: Delayed cerebral ischemia.
On admission.
Troponin I
52 patients (36.6%) had an elevated TnI level upon admission. There was no significant difference with respect to age (p = 0.25), sex (p = 0.09, BMI (p = 0.7), length of hospital stay (p = 0.63), premedication and comorbidities, except history of stroke (p = 0.02), evidence and localization of a cerebral aneurysm, treatment regime, mild vasospasm (p = 0.67), duration of vasospasm (0.94), onset of vasospasm (p = 0.86), DCI (p = 0.17) and necessity of intraarterial application of nimodipine (p = 0.12) between patients with and without initially elevated TnI level. In contrast, the group TnI positive had a lower GCS score (p < 0.001), higher WFNS score (p < 0.001), higher rate of status post stroke (p = 0.02), increased white blood cell count (p = 0.002), higher blood glucose level (p < 0.001), higher IQR of the Fisher grade (p = 0.01) upon admission as well as a higher mRS score (p < 0.001) and an increased mortality (p = 0.02) at discharge (Table 1).
TCD-Defined Vasospasm
Any vasospasm was identified in 86 patients (60.6.%), mild vasospasm in 32 patients (37.2%) and severe vasospasm in 54 (62.8%). TCD-related vasospasm occurred on median day 6 after the bleeding (IQR: 4-9) and the median duration of anti-vasospastic treatment was 8 days (IQR:0-13). Average MMFV 108.5 ± 36.9 cm/s and the average MMFV within the vasospasm period was 157.3 ± 64.4 cm/s. A hypertensive treatment was performed in 60 patients (42.3%) and 26 patients (18.3%) required an intraarterial application of nimodipine. DCI occurred in 32 patients (22.5%) and 27 patients (19%) suffered from an ischemic brain lesion. In the univariate analysis, elevated TnI level upon admission was significantly associated with the occurrence of any vasospasm (p < 0.001) and severe vasospasm (p < 0.001), however, not with mild vasospasm (p = 0.95). In addition, a higher average MMFV during inpatient treatment (p = 0.02), higher MMFV within vasospasm period (p = 0.007), necessity of hypertensive treatment (p = 0.005), duration of hypertensive treatment (p = 0.022) and occurrence of ischemic brain lesions (p = 0.02) were found in the TnI positive group in comparison to the TnI negative group (table 1).
The univariate and multivariate analysis for parameters to prognosticate any and severe TCD-defined vasospasm are summarized in Tables 2 and 3. The binary logistic analysis identified younger age (odds ratio [OR]: 0.92, confidence interval [CI]: 0.87-0.96, p < 0.001), higher Fisher grade (OR:2.31, CI:1.12-4.76, p = 0.02) and elevated TnI level (OR:5.55, CI:1.77-17.41, p = 0.003) upon admission as independent predictors for any TCD-defined vasospasm. Furthermore, younger age (OR:0.93, CI:0.89-0.98, p = 0.003), higher WFNS score (OR:2.01, CI: 1.1-3.97, p = 0.025) and elevated TnI (OR:3.3, CI: 1.1-9.95, p = 0.034) were independent predictors concerning the occurrence of severe vasospasm.
Univariate and Multivariate Analysis of Predicting any Vasospasm.
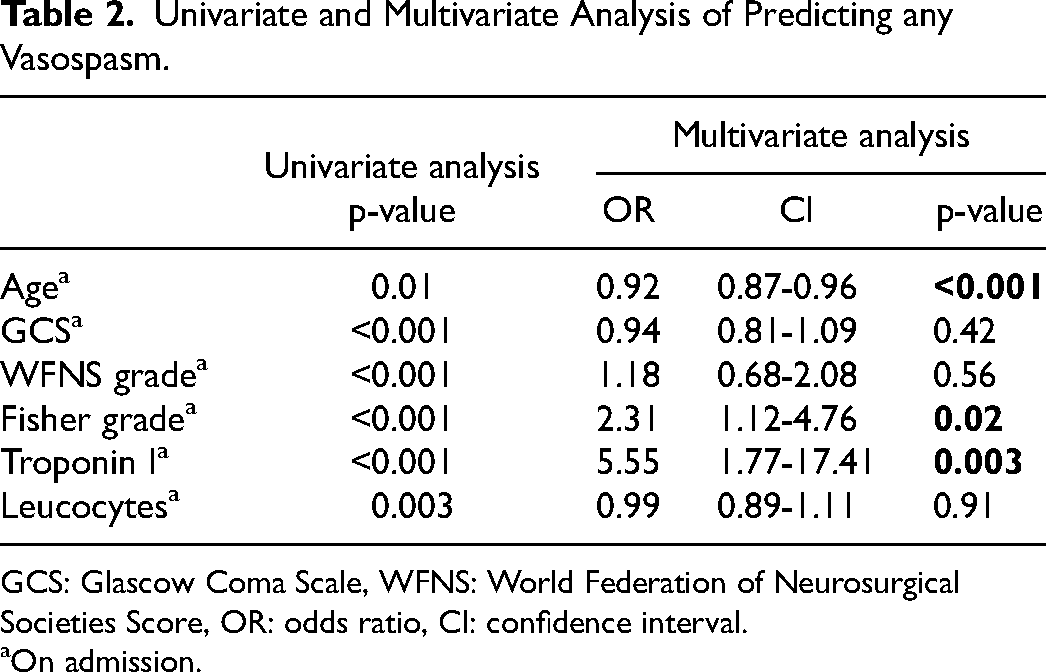
GCS: Glascow Coma Scale, WFNS: World Federation of Neurosurgical Societies Score, OR: odds ratio, CI: confidence interval.
On admission.
Univariate and Multivariate Analysis of Predicting Severe Vasospasm.
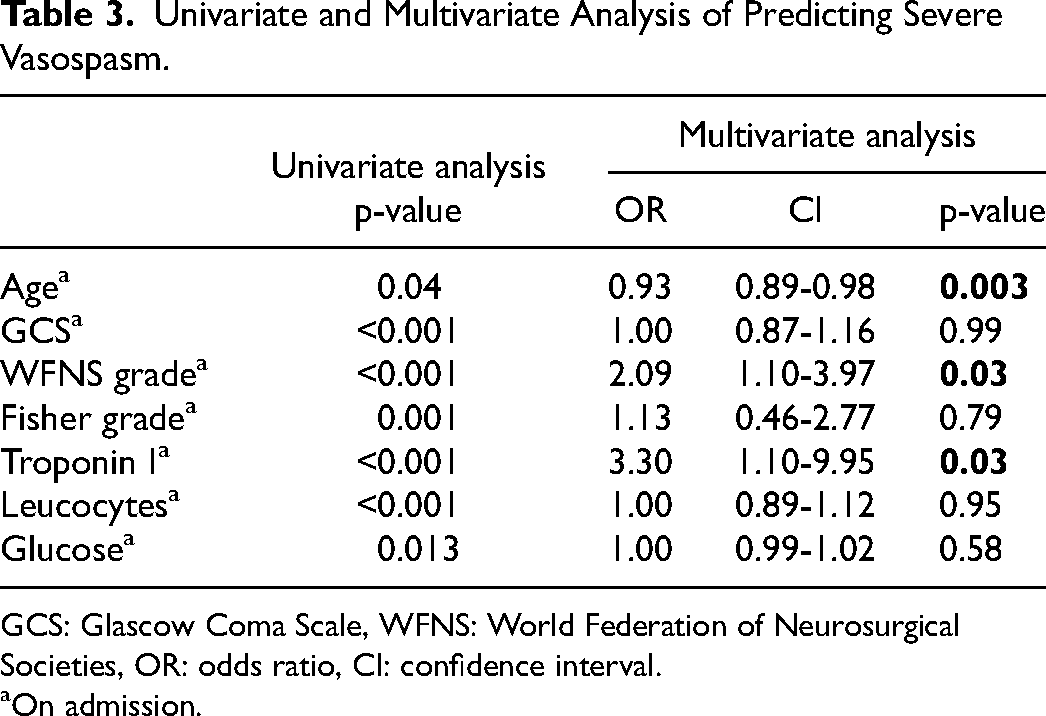
GCS: Glascow Coma Scale, WFNS: World Federation of Neurosurgical Societies, OR: odds ratio, CI: confidence interval.
On admission.
Discussion
Summary of Findings
A retrospective study of 142 neurosurgical SAH patients was conducted to investigate the impact of initially elevated TnI level upon admission on the occurrence of TCD-defined cerebral vasospasm. In accordance with previous studies, patients with an initially elevated TnI value had a lower GCS score, higher WFNS score, higher Fisher grade upon admission as well as higher mRS and increased mortality at discharge.16–20,26 This group also has a higher rate of status post stroke, an increased white blood cell count, a higher blood glucose level upon admission, and a higher average overall MMFV during inpatient treatment, higher MMFV within vasospasm period, higher necessity of hypertensive treatment, a longer duration of hypertensive treatment, and a higher rate of ischemic brain lesions. The multivariate analysis revealed that younger age and higher Fisher grade up on admission were independent predictors for any vasospasm as well as younger age and higher WFNS score for severe vasospasm, which is in accordance to several previous studies.1,3,27,28 Additionally, to the best of our knowledge, the current study identified for the first time, an initially elevated TnI level upon admission as a new independent predictor for the occurrence of any and severe vasospasm. Therefore, the initial TnI level seems to be a helpful early serum biomarker for improving ICU treatment, especially for the early detection of patients with an increased risk to develop cerebral vasospasm.
Troponin I
In the present study, 36.6% of the SAH patients had an elevated TnI level upon admission, which is comparable to those of previous studies.15–19 The troponin complex is subdivided into three isoforms, troponins T, I, and C. Troponins T and I are the cardiac isoforms, and troponin C the isoform of skeletal and cardiac muscle. 29 TnI is routinely used for management of the acute coronary syndrome, especially in combination with angina pectoris symptoms, echocardiographic abnormalities and ECG changes. Elevation of TnI in these patients is often caused due to an occlusion or stenosis of a coronary artery.18,20,26,30,31 However, elevation of TnI in combination with EGC abnormalities and reversible cardiac complications, eg left ventricular apical systolic akinesia resembling Takotsubo cardiomyopathy and myocardial stunning, are also frequently seen in patients shortly after SAH. This phenomenon is caused on a type of focal subendocardial contraction band necrosis that results from an excessive release of catecholamines within the myocardium without an occlusion or acute stenosis of the coronary artery.18,20,26,30,31 Nevertheless, the pathophysiological pathway is not completely understood. Several studies reported about an association of an initially elevated TnI level and a lower GCS score, higher WFNS score, higher Fisher grade as well as a higher mRS and increased mortality rate at discharge, which was verified in the current study.16–20,26 TnI is a serum biomarker for cardiopulmonary and cardiovascular diseases, so that the increased number of patients with a history of stroke in the TnI positive group could be associated with a higher vulnerability of these patients to new cerebrovascular events. In addition, the increased white blood cell count, and the higher blood glucose level at admission in SAH patients with elevated TnI level emphasize the hypothesis of an excessive release of catecholamines due to activation of the central sympathetic nerve system after SAH, which could lead to hyperglycemia, leukocytosis and increased TnI. 32
TCD-Defined Cerebral Vasospasm
Apart from medical complications eg, stunning myocardium or neurogenic pulmonary edema, the occurrence of cerebral vasospasm is a serious complication, which can lead to increased morbidity and mortality in SAH patients.1,3,11,26–32 Cerebral vasospasm is caused by intracranial arterial narrowing due to vasoconstriction, subendothelial fibrosis, and swelling of the endothelium and may lead to DCI and ischemic brain lesions.1,3,11 Moreover, several studies reported the association of systemic inflammation with the occurrence of vasospasm.33–35 Nevertheless, the pathophysiological pathway of cerebral vasospasm is still not completely understood.
The association of TnI and the occurrence of TCD-defined cerebral vasospasm has been investigated in few studies only, in which no significant correlation was found.18,21,22 In contrast, the present study identified a significant correlation between elevated TnI level upon admission and the occurrence of any vasospasm, severe vasospasm and ischemic brain lesions, as well as higher average overall MMFV, higher MMFV within vasospasm period, higher necessity and longer duration of hypertensive treatment within inpatient treatment. However, no association between elevated TnI and the occurrence of mild vasospasm and DCI was found.
Parekh et al and Ramapa et al identified no correlation of elevated TnI level and the evidence of TCD-related cerebral vasospasm, which is in accordance to the results of our study with respect to mild vasospasm, however, in contrast to any and severe vasospasm.20,21 Furthermore, Jeon et al identified no difference between patients with and without elevated TnI level and the incidence of symptomatic vasospasm as well as the duration of hyperdynamic therapy for symptomatic vasospasm. 36 This difference could be explained by inhomogeneous definition of MMFV for the diagnosis of TCD-defined vasospasm.
Only Naidech et al reported about an association of elevated TnI level and vasospasm; however the authors did not state the method of vasospasm detection (TCD vs angiography vs CT perfusion scan etc) and the incidence of vasospasm in patients with and without elevated TnI level. 18 Moreover, several studies reported a higher risk for the occurrence of DCI and ischemic brain lesions in SAH patients with elevated TnI, which is in accordance to the results of the present study with respect to ischemic brain lesions but not to DCI.18,29 This difference could be explained by various systolic blood pressure managements in these studies. This hypothesis is sustained by similar results regarding ischemic brain lesion, and difference concerning DCI. Patients with neurological deterioration due to vasospasm were routinely treated with increased systolic hypertension, to improve the neurological status and avoid ischemic brain lesion in the CT. All patients included in present study were early treated with a moderate hypertension (systolic blood pressure of 140 to 160 mm Hg), which is a possible explanation for the lower evidence of DCI.
The results of the present study suggest that TnI can be considered a helpful biomarker for early identification of SAH patients with a high risk for the occurrence of any and severe vasospasm. Those patients may benefit from early extended cardiopulmonary and cerebral monitoring, for example, by using a Swan-Ganz catheter and/or pulse contour cardiac output system (PiCCO) and/or intermittent or continuous transthoracic/transesophageal echocardiography or microdialysis catheter.
Limitations and Strengths of the Study
The current study has some strengths but also several limitations. The most important limitation is the monocentric and retrospective character of the study. Secondary, TCD measurements could significantly vary between different examiners and were not verified with cerebral angiography in the present study. Nevertheless, Gonzalez et al observed a global accuracy of 81.1% for the diagnosis of clinical vasospasm and a global accuracy of 77.2% for the diagnosis of angiographic vasospasm for TCD velocities above 120 cm/s at the MCA. 37 Additionally, Kumar et al reported a high accuracy of TCD-defined evidence of vasospasm for DCI with a specificity of 71% (95% CI: 51-84%), sensitivity of 90% (95% CI: 77-96%), and negative predictive value of 92% (95% CI: 83-96%). 38 Both studies emphasize that TCD is an appropriate method for vasospasm detection. Moreover, no serial TnI measurements, especially during the period of evident cerebral vasospasm, were available due to the retrospective design of the study. Nevertheless, this important aspect should be investigated in further studies.
The strength of the present study was the large study population with comprehensive demographic, laboratory chemistry, clinical, and radiological records of ICU-admitted neurosurgical patients with SAH. In addition, to our knowledge, this is the first study reporting elevated TnI level upon admission as a new independent predictor for the occurrence of TCD-defined cerebral vasospasm in SAH patients.
Conclusion
An elevated TnI level at admission is an independent predictor for the occurrence of any and severe vasospasm in SAH patients. This finding could be helpful for an early identification of SAH patients with an increased risk for the occurrence of vasospasm in the later course of the disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.