
Abstract
Background
Femoral cannulated extracorporeal membrane oxygenation (ECMO) has been associated with neurologic complications in the lower extremity ipsilateral to the cannulation. There is uncertainty about the prevalence of these complications and their mechanisms of development.
Objective
Aim of this systematic review was to investigate the prevalence of neurological complications after ECMO and to describe possible underlying mechanisms.
Method
A systematic literature search was performed in Medline-Ovid, Embase, Cochrane Library, CINAHL, and PEDro until April 2021 for clinical trials in English or German language which quantified neurologic complications in the lower extremity ipsilateral to the ECMO cannulation of adults. The complications had to be delimitable to intensive care unit–acquired weakness. Methodological quality was assessed by 2 independent investigators using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies of the National Heart, Lung, and Blood Institute.
Results
Eight observational studies were included in the synthesis. Study quality was good to fair in 88% of the papers. Overall, 47 of 202 patients (23.3%; ranging from 3% to 48% across studies) with femoral ECMO cannulation showed neurologic complications of the lower extremity ipsilateral to the cannulation. Peripheral ischemia and compression of nerves by the ECMO cannula are discussed as mechanisms of injury.
Conclusion
The occurrence of neurological complications after ECMO was common and can lead to long-term impairment. The mechanisms are largely unknown but currently there is no sufficient evidence for the involvement of ECMO. Standardized assessments are needed to systematically screen for neurological complications early after ECMO, to enable countermeasures and prevent further complications.
Keywords
Introduction
Extracorporeal membrane oxygenation (ECMO) is a potentially lifesaving intervention for patients with acute cardiac, pulmonary, or cardiopulmonary failure that is no longer treatable with conventional therapies. According to the Extracorporeal Life Support Organization, the number of patients supported with ECMO is steadily increasing. 1 In particular, during severe acute respiratory syndrome coronavirus 2 pandemic, the use of ECMO for therapy of coronavirus disease (COVID-19) and associated Acute Respiratory Distress Syndrome has increased.2,3
Complications following the use of ECMO include bleeding, infection, and vascular and neurologic deficits. 4 In a systematic review, the most common reported neurological complications during therapy with ECMO were hemorrhagic or ischemic strokes and seizures. 5 Long-lasting physical impairments are common in ECMO survivors and have a large impact on their quality of life. 6 In addition to intensive care unit–acquired weakness (ICU-AW) which frequently occurs in critically ill patients, 7 peripheral nerve lesions of the lower extremity are repeatedly reported in both, venoarterial (VA) and venovenous (VV) ECMO. The mechanisms leading to these lesions could not be conclusively explained in all cases.8,9 One study describing 21 patients who underwent femoral ECMO cannulation pre- or post-heart transplantation found that 11 of those patients experienced leg complications, often including neurologic complications such as drop foot, paresthesias, or weakness of one leg. 10 Local damage or irritation of the femoral nerve by the cannula in the groin was reported as a possible cause of such failures in another study. 11 These neurological complications of the lower extremity represent severe limitations in daily life and thus a significant burden for the caregivers, the patients, and the health infrastructure. 12
Aim of this systematic review was to investigate the prevalence of neurological complications in the lower extremity ipsilateral to the femoral cannulation in adults after ECMO and to describe possible underlying mechanisms.
Materials and Methods
This systematic review was reported and structured according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline 13 (see Appendix A). A protocol for this review was prepared before the start of formal screening of search results and registered in the International Registry of Systematic Reviews (PROSPERO) in May 2021 (registration number: ID = CRD42021253028).
Search Strategy
The concept of population, exposition, and outcome was used to develop the search strategy. 14 Neurological complications in the lower extremity ipsilateral to the femoral cannulation in adults after ECMO were sought. Neurologic complications were defined as any lower extremity paresis, plegia and hypesthesia, paraparesis, and paraplegia. The outcome measurement procedure and its timing were not specified.
The search strategy contained MeSH terms and free text words and can be viewed in detail in Appendix B. All types of clinical trials and observational studies were included; solely case series and case studies were not eligible for inclusion. Electronic literature searches in the Medline-Ovid, Embase, CINAHL, PEDro, and Cochrane Library databases were performed by a librarian at the University of Zurich (SK) up to April 21, 2021, with no time limit on the publication period (see Appendix C). Studies with children, with animals, or those written in another language than English or German were excluded.
Study Selection
The neurological complications sought had to be quantifiable and distinguishable from ICU-AW. Intensive care unit–acquired weakness is characterized by symmetric flaccid paresis of the extremities, which is often more pronounced proximally than distally, and sensory disturbances may occur. 15 The neurologic complications, especially if they occur bilaterally, should be distinguishable from this symmetrical occurrence of ICU-AW and were described and discussed in more detail when unclear.
Title and abstract screening based on predefined inclusion and exclusion criteria was performed by 2 independent reviewers (FJ and RV). The second step involved full-text screening with the references that remained. In case of different results regarding the inclusion or exclusion of studies, an attempt was made to reach agreement by means of a discussion. In case of disagreement, a third independent investigator would have been consulted.
Data Extraction
Prior to commencing the electronic literature search, a data extraction table was created by the author, following the data extraction form for prevalence studies from the Joanna Briggs Institute. 16 The following study data are extracted: (1) study information (reference, publication year, location), (2) Study design, (3) Population (age, sex, reason for hospital admission, or the disease that led to ECMO insertion, disease severity), (4) ECMO characteristics (type, placement of a distal cannula, duration), (5) Assessment of neurological complications (methods, follow-up period), and (6) neurological complications. The frequency of neurological complications of the lower extremity and any descriptions of causes and localizations of injury are documented. Enumerations of lower extremity paresis, plegia, hypesthesia, paraparesis, and paraplegia are scored as neurological complications and were included in the data synthesis. Data extraction took place by the author.
Data Synthesis
We distinguished between point prevalence (percent of patients reporting neurological complications at the time of follow-up assessment) and cumulative prevalence (prevalence of any neurological complication from time of ECMO commencement until follow-up assessment). Due to the low number of studies and the differences in assessment methods and follow-up periods, we did not make an attempt to estimate an overall prevalence. We reported the prevalence for each study and summarized the total number of observed cases with neurological complications in the lower extremity.
Study Quality Assessment
The methodological quality of the studies was assessed by 2 independent investigators using a modified version of the National Heart, Lung, and Blood Institute's Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 17 In case of disagreement, this would have been discussed with a third independent investigator and thus an agreement reached. In order to assess the agreement of the reviewers for the quality assessment the Cohen's Kappa coefficient was calculated. 18
Results
Literature Search
The literature search identified 1177 studies, of which 388 were duplicates. Of 789 titles and abstracts screened, 113 were subjected to a full-text review, of which 8 studies met the criteria for inclusion in the systematic review (Figure 1).
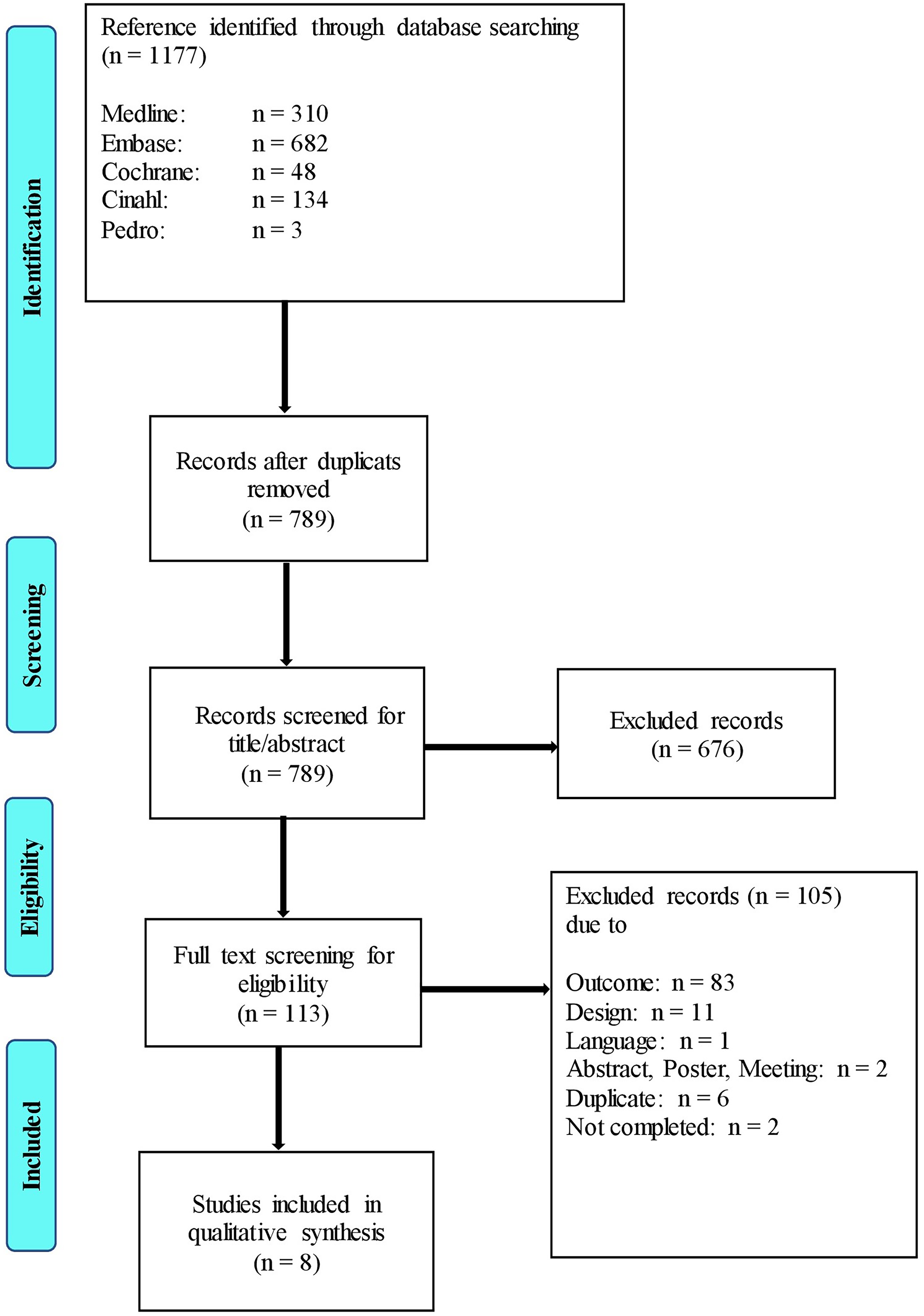
Flowchart of the study selection process.
Study Characteristics
Two studies were prospective observational and 6 retrospective observational. Three studies included a control group of patients not treated with ECMO, and of these, only one reported neurological complications in both groups, thus allowing a group comparison. 19 In none of the studies, neurologic complications of the lower extremity after femoral ECMO cannulation were predefined as outcome measure. Only 3 studies assessed neurological complications with neurological assessments, the other studies used retrospective chart reviews or questioned the patients. The studies were published between 2008 and 2020 and included a total of 329 patients (range 17-82 patients). All patients were intensive care patients. The detailed characteristics of the included studies are presented in Table 1.
Study Characteristics.
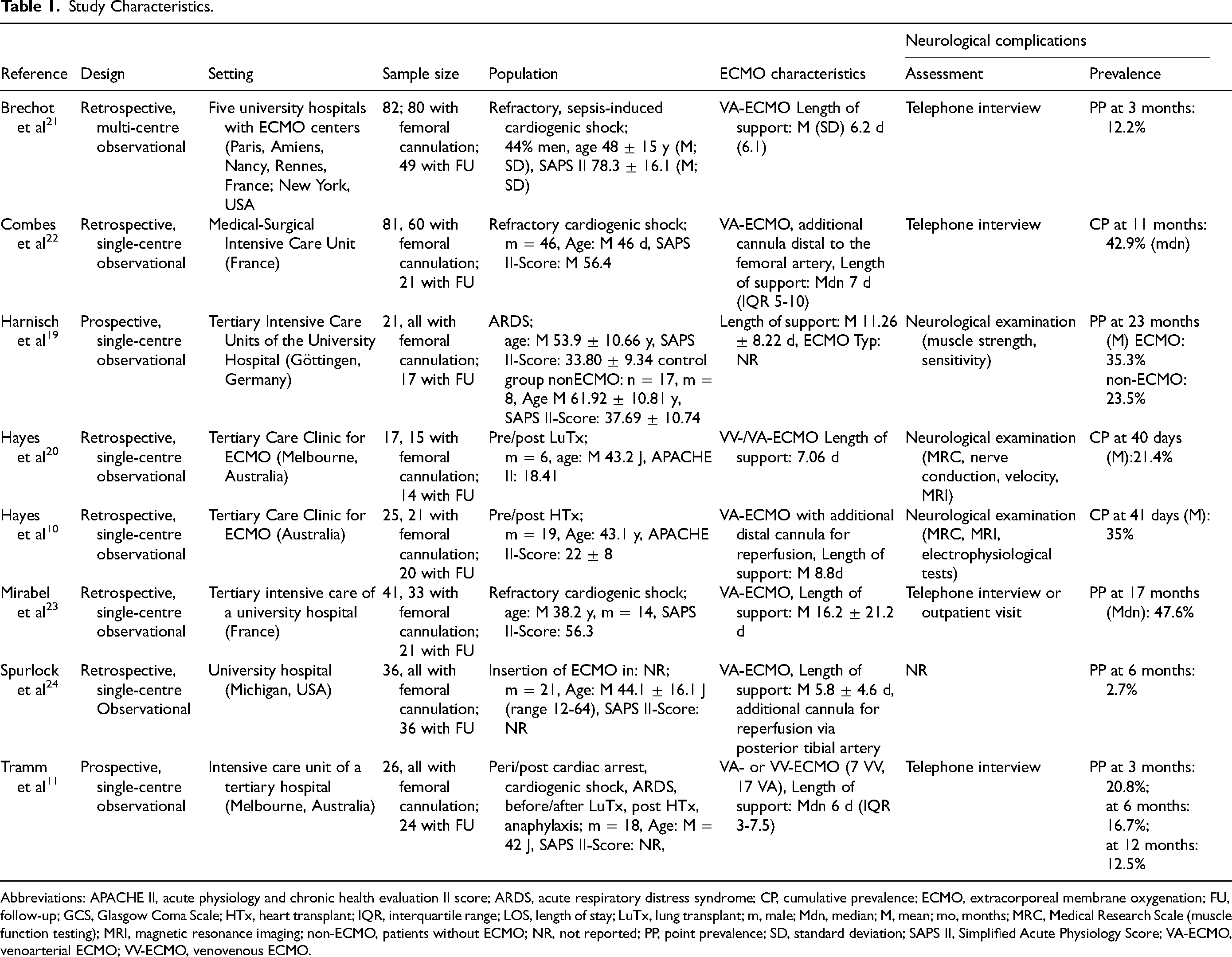
Abbreviations: APACHE II, acute physiology and chronic health evaluation II score; ARDS, acute respiratory distress syndrome; CP, cumulative prevalence; ECMO, extracorporeal membrane oxygenation; FU, follow-up; GCS, Glasgow Coma Scale; HTx, heart transplant; IQR, interquartile range; LOS, length of stay; LuTx, lung transplant; m, male; Mdn, median; M, mean; mo, months; MRC, Medical Research Scale (muscle function testing); MRI, magnetic resonance imaging; non-ECMO, patients without ECMO; NR, not reported; PP, point prevalence; SD, standard deviation; SAPS II, Simplified Acute Physiology Score; VA-ECMO, venoarterial ECMO; VV-ECMO, venovenous ECMO.
Quality of Included Studies
On average, the studies scored 8.25 out of a possible 14 points and thus achieved a “fair” overall quality. Three10,19,20 of the 8 included studies were rated “good,” 411,21–23 were rated “fair,” and one 24 study received a “poor” as quality rating (see Appendix D).
The interrater reliability of the 2 independent investigators (FJ and RV), in assessing study quality could be rated as “good” with a kappa value of 0.80. 25
Neurological Complications
Two studies performed by the same research group investigated the cumulative prevalence of complications from the start of ECMO support until hospital discharge.10,20 The other 6 studies investigated long-term outcomes after ECMO by contacting patients after follow-up periods ranging from 3 to 23 months.11,19,21–24
Overall, 47 of the 202 patients (23.3%) with femoral ECMO cannulation participating in follow-up assessments had neurologic deficits of the lower extremity ipsilateral to the cannula. However, this percentage ranged from 3% to 48% in the individual studies (Figure 2).
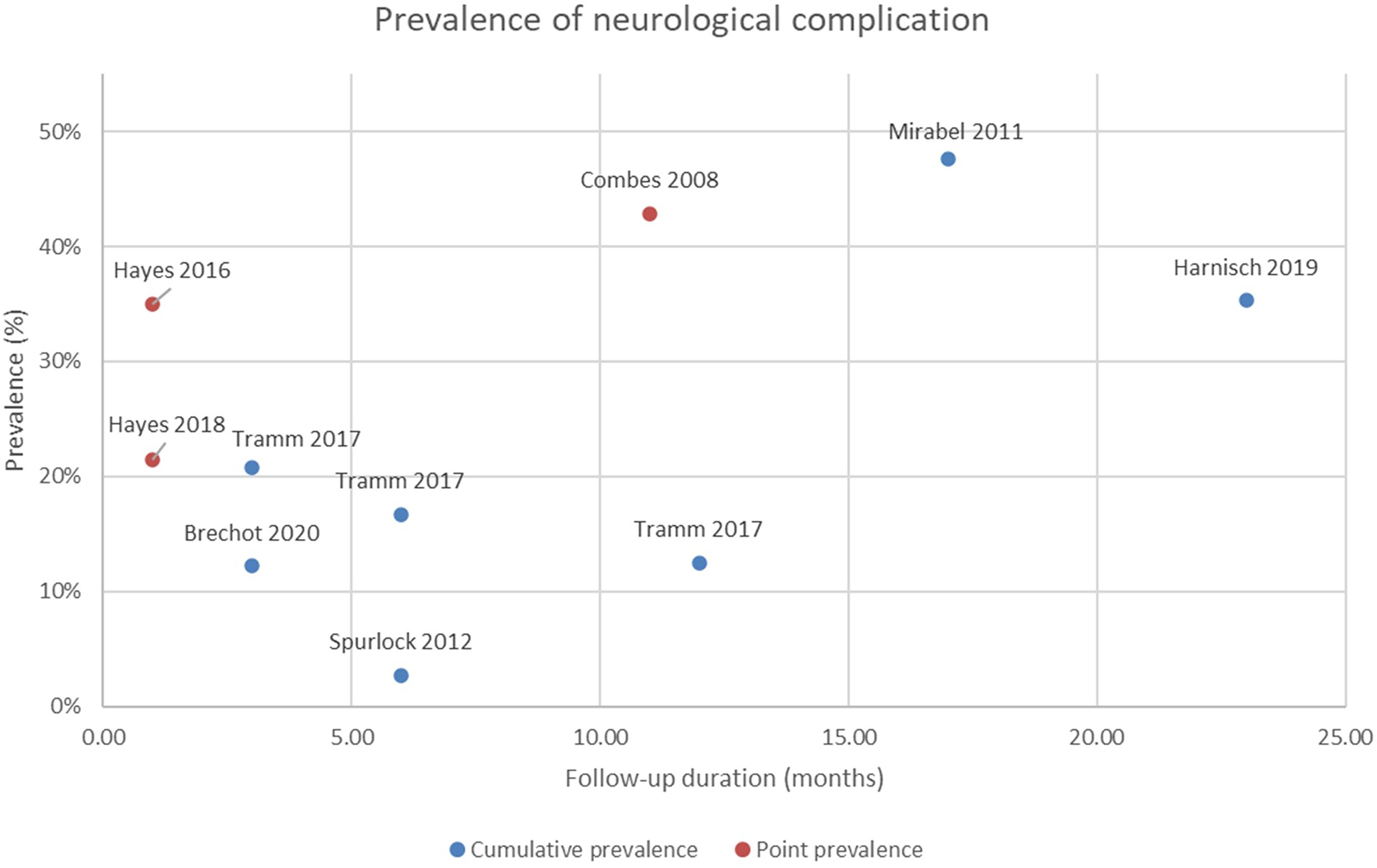
Prevalence of neurological complications in the individual studies.
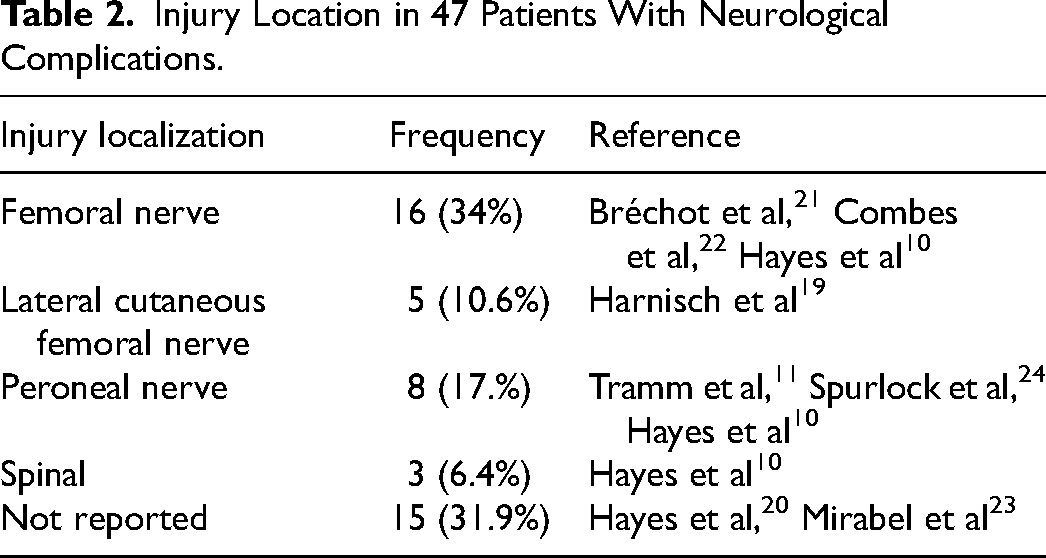
Eighteen patients showed sensory and motor deficits. Of these, 6 were sensorimotor, 17 purely sensory, and 6 purely motor impairments. In the only study comparing the ECMO group to a group without ECMO, the number of neurological complications was similar: paresthesias due to initial trauma or polyneuropathy occurred in 4 patients in the control group and 5 patients had paresthesias and one paresis in the ECMO group. 19 Injuries were observed with both VA-ECMO and VV-ECMO. None of the included studies reported a specific mechanism of onset. The locations of the injuries were described in 32 studies and occurred mostly at the femoral nerve (Table 2).
Injury Location in 47 Patients With Neurological Complications.
Discussion
There are 2 main findings from this systematic review. First, it was shown that neurological complications of the lower extremity are very common in patients following ECMO treatment with femoral cannulation, presenting a prevalence of almost 25%, in the studies included. Second, the mechanisms of development are largely unknown. Several mechanisms have been discussed according to the region of damage.
The femoral nerve was most frequently reported as site of injury.10,21,22 Lesions might result from compression by the large ECMO cannulas or swelling of the surrounding tissue. 8 Seroma and hematoma formation in connection with the access of the ECMO cannulae in the groin are common,26,27 and lumbosacral plexopathies due to hematomas after femoral cannulation have been described previously.28,29 Case reports suggest that without a detailed diagnosis, these symptoms might be misdiagnosed as ICU-AW and therefore only recognized very late.30,31 Compression by the femoral ECMO cannula was also suspected for the damage to the lateral cutaneous femoral nerve, 19 this type of complication has also been described previously. 32 In making this assumption, it is important to consider the location of the lateral cutaneous femoral nerve. In contrast to the femoral nerve, which runs topographically very close to the femoral vein and artery in the groin, the lateral cutaneous femoral nerve runs relatively far lateral to the vessels to be cannulated. Seroma and hematoma formation and other similar sequels of ECMO cannula access may thus be more plausible causes of nerve compression. Furthermore, its anatomical course makes the lateral cutaneous femoral nerve vulnerable to injuries. Patients with femoral ECMO cannulation are mostly restricted to the bed in neutral zero position and their range of motion is severely limited. A long-lasting extension of the hip joint, as it is usually the case in the permanently flat supine position of these ECMO patients, could cause a lesion of the lateral cutaneous femoral nerve. 33 Such positional damage either by prolonged extension or superficial compression in patients with femoral ECMO cannulation should also be considered in the presence of a peroneal nerve lesion. Peroneal lesions after femoral ECMO cannulation were also reported in various case studies.9,34–36 Positional damage of the lateral cutaneous femoris nerve and the peroneal nerve could be prevented by consistent repositioning of the patient, which can usually take place in slight hip flexion, even with femoral canulation. In one patient with foot drop and neuropathic pain, Spurlock et al 24 suspected ischemia as the cause of the injury. Overall, ischemia is the most frequently reported vascular complication after femoral VA-ECMO cannulation, 37 and the severity of the nerve damage caused by this varies depending on the duration of the ischemia and the degree of occlusion. 38 The causes are usually multifactorial, can occur at any time during ECMO therapy, and may lead to severe nerve damage in the lower extremity. 38 For femoral cannulation, a distal perfusion cannula is suggested in addition to other recommendations on cannula size and insertion technique,39–41 but this is no guarantee of preventing ischemia.38,42,43
Other mechanisms have been discussed in the context of bilateral sensorimotor deficits in bifemoral canulated patients. The retrograde flow from the arterial ECMO cannula could lead to altered flow dynamics in the Adamkiewicz artery supplying the spinal cord, resulting in infarction and spinal ischemia. 10 However, often these patients also suffered a severe shock or cardiac arrest, both events requiring a high demand of vasopressors and additionally chest compression before ECMO insertion. Both procedures have also been suggested as possible causes of spinal infarction in connection with ECMO therapy. 44 This, together with ECMO-induced plexopathies due to hematomas, shows that neurological complications due to ECMO are not always unilateral but can also be bilateral.
Weakness of the extensors and flexors of the foot was noted in another patient. 19 Although the injury was ipsilateral to the ECMO cannulation and no other causes were given, this finding was not attributed to ECMO. The authors stated that injury to the sacral plexus or the sciatic nerve during percutaneous ultrasound-guided cannulation would be nearly impossible. However, precisely such injuries to the sacral plexus have not been recognized in other cases because no detailed diagnostics took place in time.30,31 As a consequence, therapy was delayed and the injury could not be remedied.
This is the first systematic review on neurological complications that also addresses peripheral neurologic complications in femoral ECMO cannulation. Previous reviews5,45,46 have focused on cerebral complications. Two other reviews examined the physical and psychological quality of life of patients after ECMO.6,47 They listed complications but did not explicitly address neurological complications. Physical quality of life was found to be significantly impaired in patients after ECMO, and severe and persistent neurological complications not only lower quality of life but also increase the burden on the nursing staff and the costs of rehabilitation. Five of the studies included in the current review were published within the last 6 years,10,11,19–21 which illustrates the timeliness of this topic and can be linked to the ever-increasing use of ECMO systems.
Limitations of this review are the small number of studies, small sample sizes, the observational study designs, and the lack of control groups. None of the studies explicitly investigated neurological complications of the lower extremity after femoral ECMO cannulation as an outcome; accordingly, the assessments were mostly not appropriate, and insufficiently or poorly reported. Complications were frequently assessed with questionnaires and telephone interviews which are subject to a high risk of bias, and the follow-up period also varied widely across studies. Only one study reported neurological complications in a comparable group without ECMO and half of the papers recorded preexisting neurological conditions or deficits. This, and the observational nature of the studies limit the extent to which the causal relationship between ECMO and neurological complications can be ascertained and make an estimation of the prevalence of ECMO-related neurological deficit difficult. Mechanisms were rarely investigated and little can yet be reported on the association of femoral ECMO cannulation and the development of neurologic complications of the lower extremity.
Furthermore, the diagnostic criteria to differentiate neurological complications from ICU-AW should be improved. The distinction criterion that ICU-AW occurs symmetrically in both lower extremities whereas neurological complications are restricted to one is imprecise and would for example result in a missed diagnosis of spinal infarction with paraparesis. Similarly, in patients with bifemoral cannulation, neurologic complications caused by ECMO could also occur symmetrically, as reported in one of the studies. 10
Long-term damage resulting from neurological complications might be prevented by detecting them as early as possible and initiating countermeasures. Patient's neurological status could be assessed daily during a sedation stop or during awake ECMO. Awake ECMO would allow patients to actively participate in assessments and rehabilitation measures, which is considered safe in selected patients.48–50
Preventive measures of neurological complications include the prevention of ischemia as suggested by recommendations39–41 and a careful evaluation during the choice of the cannulation site. 51 Furthermore, consistent repositioning and physical therapy could prevent positional damage and help to detect strength deficits and possible paresis early.52,53
Conclusions
Neurological complications are frequently observed with femoral ECMO cannulation. However, no studies have explicitly investigated neurological complications of the lower extremity after femoral ECMO cannulation and the underlying mechanisms are unclear. Further research is needed in this area. Early and detailed diagnosis with valid assessments may help to initiate countermeasures and to prevent long-term damage in these patients.
Supplemental Material
sj-docx-1-jic-10.1177_08850666231217679 - Supplemental material for Neurological Complications of the Lower Extremities After Femoral Cannulated Extracorporeal Membrane Oxygenation: A Systematic Review
Supplemental material, sj-docx-1-jic-10.1177_08850666231217679 for Neurological Complications of the Lower Extremities After Femoral Cannulated Extracorporeal Membrane Oxygenation: A Systematic Review by Frauke Johannes, PT, MSc, Rahel Frohofer-Vollenweider, PT, MSc, and Yvonne Teuschl, PhD in Journal of Intensive Care Medicine
Footnotes
Acknowledgments
Sc. nat. Sabine Klein (SK) from the Scientific Library of the University of Zurich is acknowledged for her help in developing and conducting the search strategy of this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.