
Abstract
Keywords
Introduction
Pediatric patients admitted to the pediatric intensive care unit (PICU) are routinely transferred to an acute care ward prior to discharge to home. Discharging a patient is a complex process that requires coordination of care, follow-up planning, and education to ensure a safe transition out of the hospital and minimize the risk of avoidable hospital readmission. Prompt discharge coordination is an important practice to avoid unnecessary delays. 1
Despite discharge directly home from the PICU (DDH) occurring for some patients, it is not the standard pathway to discharge. DDH of pediatric patients occurs for a variety of reasons including: rapid resolution of severe symptoms, high occupancy on acute care wards resulting in the patient meeting discharge goals before a bed for transfer is available, or admission to a PICU due to patient dependence on technology (eg, home ventilator) that may not be suitable for an acute care ward based on a hospital's unit guidelines.2,3 Studies of this practice in adult and neonatal intensive care units suggest that it is generally safe.4–12 However, the frequency and safety of this practice compared to the standard transfer to an acute care floor prior to discharge (ACD) lacks rigorous study in the general PICU population. A recent study of pediatric cardiac intensive care unit patients demonstrated no increased risk of unplanned readmission in this select pediatric population. 13 A 2020 investigation by Australian researchers showed that DDH is increasingly common and potentially related to delays in discharge at their institution. 14 A 2023 review article on this topic highlighted the need for more research of this practice. 15
To evaluate this practice, we sought to define the prevalence of DDH and evaluate baseline characteristics of patients leaving the hospital via DDH compared to ACD at our institution. Patients with ventilator dependence are known to have high readmission rates. 16 Given that this was likely a significant population of our DDH patients we thought it would be beneficial to repeat the analysis excluding those ventilator-dependent at time of discharge and repeat the analysis only looking at one admission per patient to better assess drivers of the DDH practice. Finally, to add additional insight into possible risk factors for DDH readmissions, we aimed to compare the group of DDH patients who were readmitted within 30 days to those that were not readmitted.
Materials and Methods
We performed a retrospective cohort study of pediatric patients (age ≤ 18 years old at time of admission) admitted to a 20-bed multi-disciplinary PICU in an academic tertiary care nested children's hospital between January 1, 2015 and December 31, 2020. Data were extracted for review from the electronic medical record via a central data repository. Patients who died during the hospitalization, were discharged to another facility, or were admitted to other ICUs in the medical center were excluded.
Data extracted included demographic data (age, sex, primary race, and ethnicity) and primary admission ICD-9 or ICD-10 codes. ICD-9 codes were converted to correlated ICD-10 codes for consistency. ICD-10 codes were categorized utilizing the Pediatric Clinical Classification System (PECCS) for analysis to regroup related ICD-10 codes into 834 distinct clinical categories. 17 Data regarding use of vasoactive infusions and ventilator use during the hospitalization were collected as markers for illness severity. Vasoactive infusions were defined as epinephrine, norepinephrine, vasopressin, milrinone, dopamine, and dobutamine. Use of a ventilator was described as any patient who required use of mechanical ventilation via a tracheostomy or endotracheal tube (including home ventilators). Patients with a diagnosis of tracheostomy were identified and manual chart reviews were performed to confirm the diagnosis of tracheostomy dependence at discharge as well as home ventilator dependence at discharge (including patients who require only mechanical ventilator during sleep). Of note, our institution adopted a policy to care for a small subset of patients with home ventilator dependence on acute care floors in the middle of the study period (2019), but most chronically ventilated patients continued to be cared for in the PICU.
Patients were divided into 2 groups to assess outcomes: (1) DDH patients; and (2) ACD patients. Groups were assigned based on the patient's primary medical team at time of discharge in the medical record. The primary outcome was readmission to the hospital within 30 days. This outcome variable is similar to other studies previously reported on in the pediatric and adult literature.11,13,18,19 To assess outcomes based on individual patients as opposed to individual admissions, we additionally performed this analysis only utilizing the first admission to the PICU per patient in the study period. We also repeated the analysis after removing patients discharged home with a ventilator, as these patients can have technology dependence best suited for care in an ICU. Within the subset of patients who experienced DDH, a secondary subgroup analysis was performed comparing those patients with DDH who had a readmission within 30 days to patients with DDH who did not have a readmission within 30 days.
Standard descriptive statistics were reported for all above-mentioned groups. Continuous data are presented as median and interquartile range and are compared using Wilcoxon Rank Sum tests. Categorical variables are presented as percentages and are compared using Chi-squared tests. Due to small numbers and many categories, binarization of race was performed for statistical analysis comparing Black versus non-Black for the primary race characteristic. Statistical analysis was performed using SAS 9.4.
This study was approved by the University of North Carolina at Chapel Hill Institutional Review Board (21-0004, approved 4/19/2021). Consent for inclusion in the study was waived.
Results
Baseline Characteristics
The total number of admissions to the PICU during the study period meeting inclusion criteria was n = 4042 admissions for 3009 unique patients. Of that group, 768 admissions (or 19%) resulted in DDH for 532 unique patients. ACD occurred for 3274 (81%) admissions for 2827 unique patients. There were no differences in baseline demographics and the median age of both groups was 2 years old (Table 1). DDH patients had significantly higher rates of tracheostomy dependence (30% vs 5%, P < .01) and home ventilator dependence at discharge (24% vs 1%, P < .01) compared with patients experiencing ACD. Pooling across the study period, percent of DDH varied monthly from 13% to 21% (Figure 1A). Percent of DDH patients varied annually from 14% to 24%, with a peak in 2017 (Figure 1B).
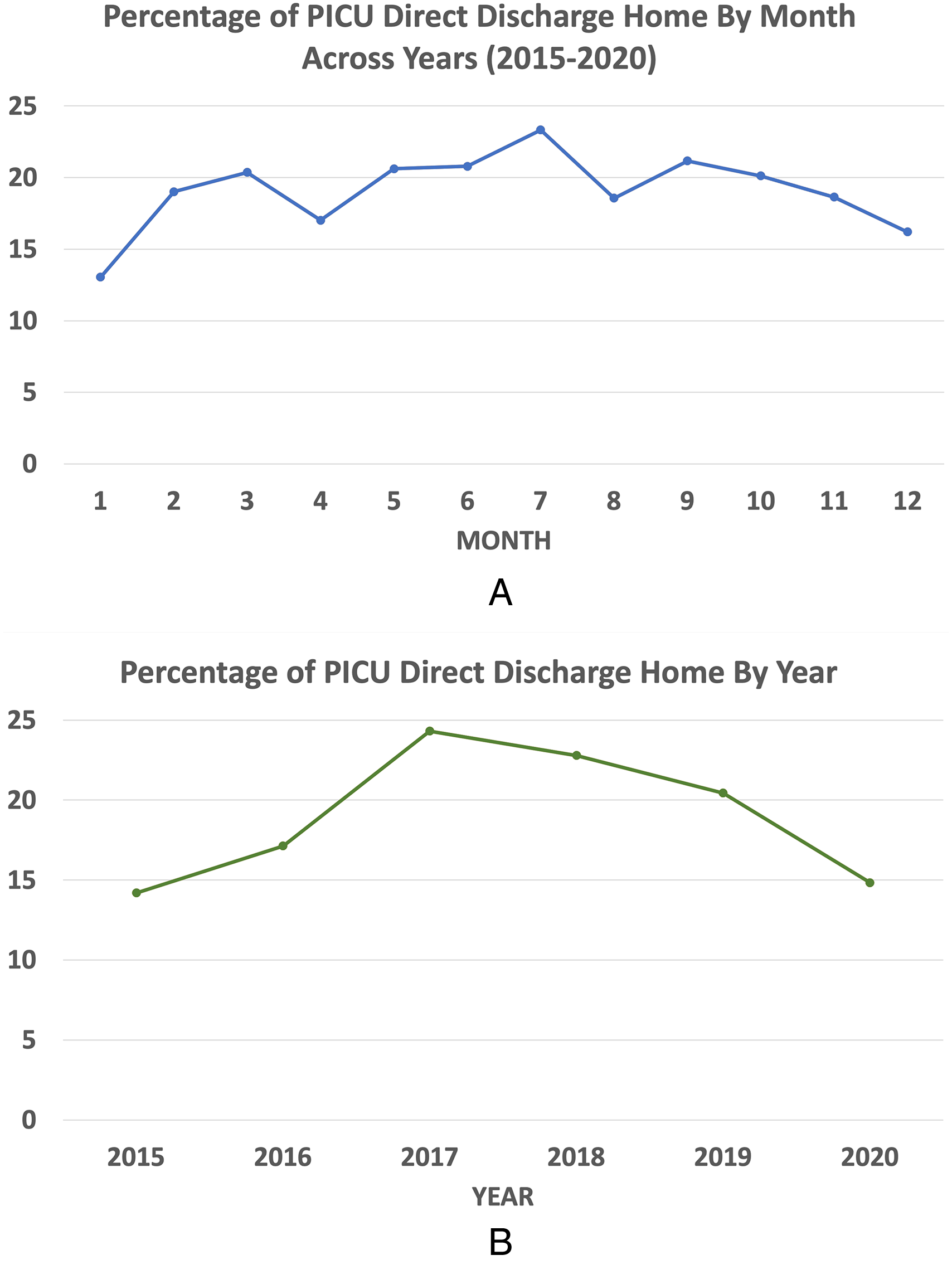
This figure demonstrates the time variation of the direct discharge home from PICU practice. In (A), the variation by month is shown aggregated across all years (2015-2020) and in (B), the variation by year is exhibited.
Baseline Characteristics, All PICU Admissions.
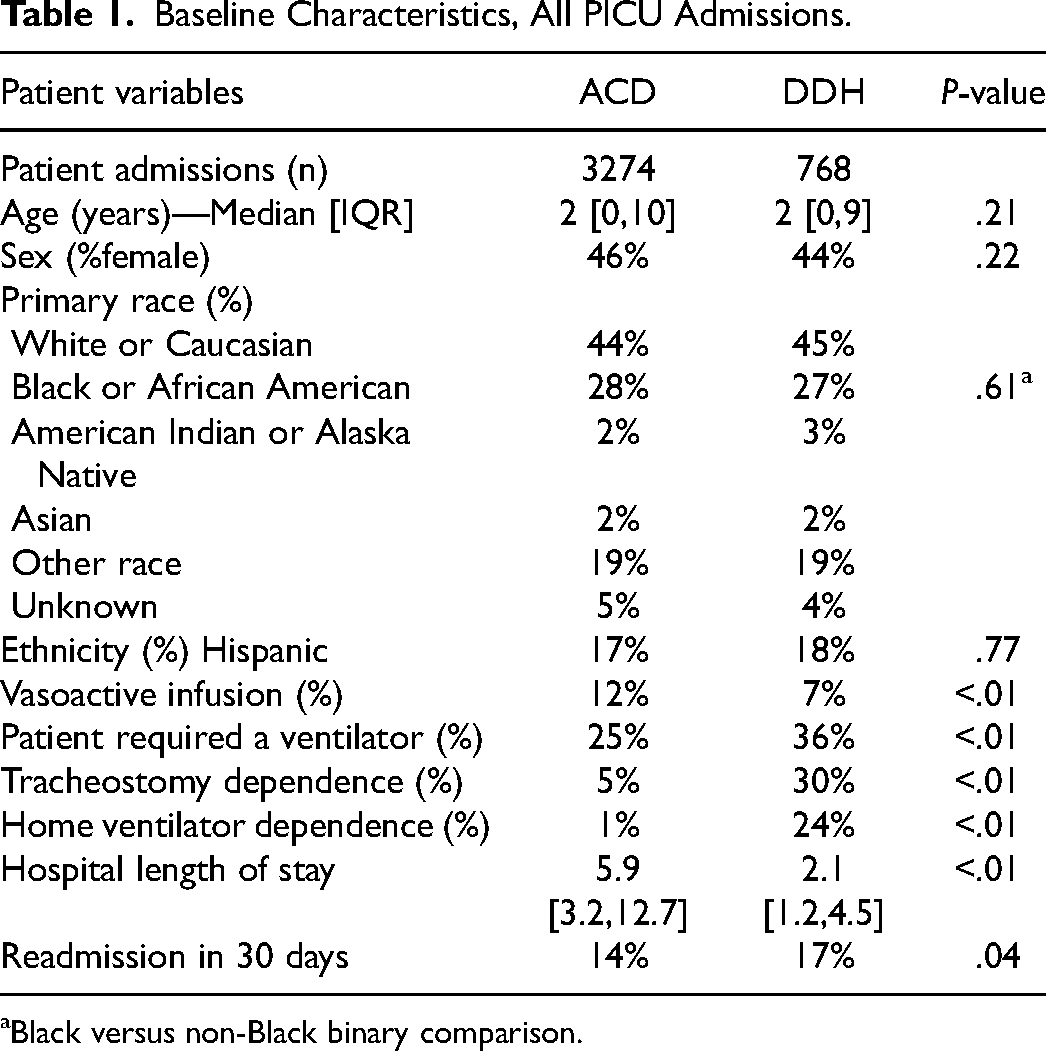
Black versus non-Black binary comparison.
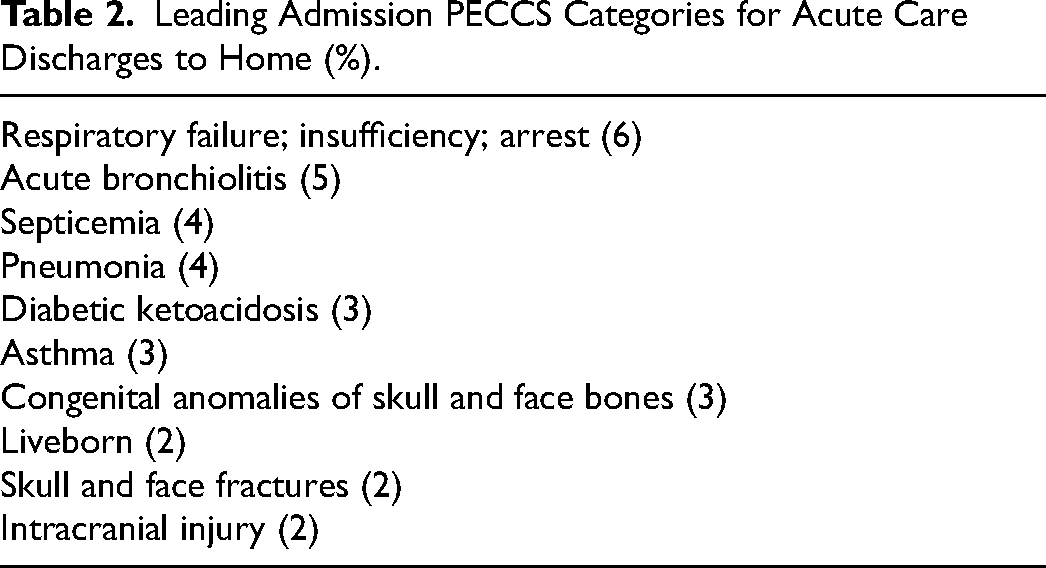
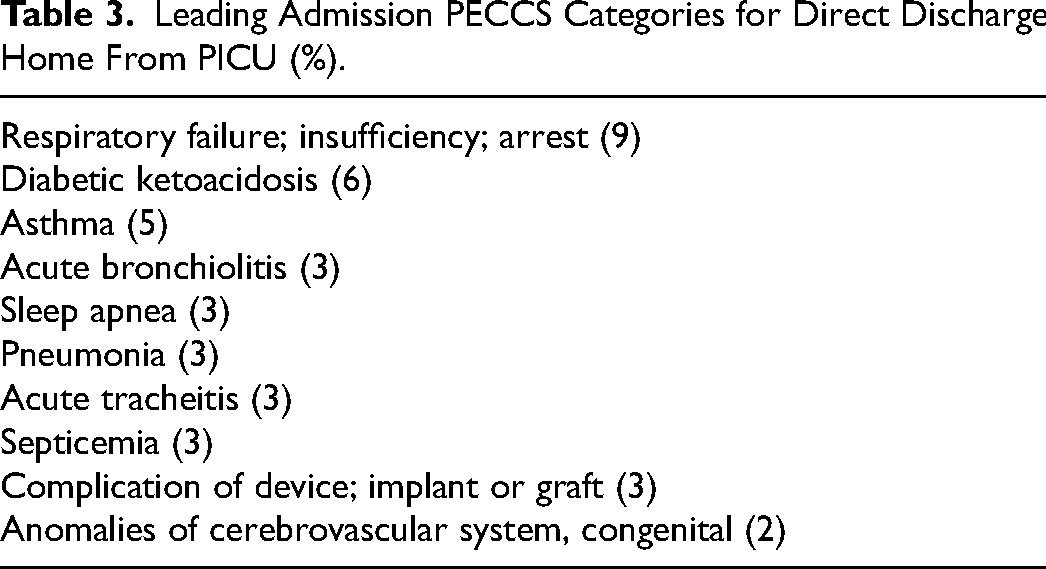
The most common PECCS Group admission diagnosis category was “respiratory failure, insufficiency, or arrest” for both groups and 6 of the top 10 PECCS Groups by admission diagnosis were the same (Tables 2 and 3). Diabetic ketoacidosis and asthma were common in both groups but ranked higher in the DDH patient population. Neurosurgical issues were more common in ACD, with 3 of the top 10 diagnoses being congenital anomalies of the skull and face bones, skull and face fractures, and intracranial injury. Diagnosis categories reflecting tracheal issues were more common in the DDH patient group with acute tracheitis ranked seventh and tracheostomy complications ranked eleventh.
Leading Admission PECCS Categories for Acute Care Discharges to Home (%).
Leading Admission PECCS Categories for Direct Discharge Home From PICU (%).
Outcomes
With respect to illness severity, DDH patients had less need for vasoactive infusions (7% vs 12%, P < .01). After removing patient admissions with baseline ventilator-dependence, DDH patients had less frequent need for new mechanical ventilation (17% vs 25%, P < .01) (Table 4). DDH patients also had a shorter length of stay (LOS) when compared to ACD patients (median of 2.1 days vs 5.9 days, P < .01).
Baseline Characteristics, Excluding Patients With Home Ventilator Dependence.
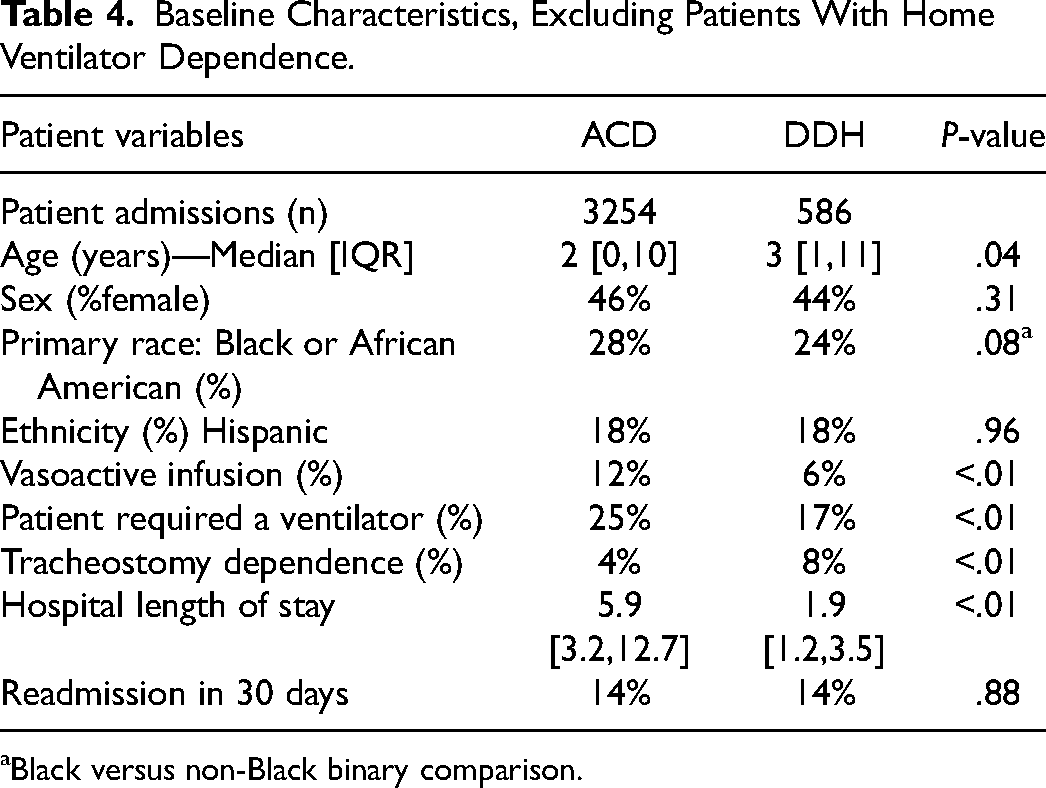
Black versus non-Black binary comparison.
For all admissions the 30-day readmission rate was higher in the DDH patients (17% vs 14%, P < .05). However, when excluding patients with baseline ventilator-dependence, 30-day readmission rate was the same for both groups (14% vs 14%, P = .88).
First Admission Only Analysis
To account for frequent readmission over the course of the study period in a subset of patients, we repeated this analysis using only the first admission to the PICU per patient in the study period. The dataset for this analysis included 427 DDH patients and 2582 ACD patients. Demographics were again similar between groups. Consistent with our previous analysis, need for vasoactive infusion (7% vs 12%, P < .01) was lower and LOS (1.9 vs 5.6 days, P < .01) was shorter when analyzing the first admission per patient in the DDH population. Ventilator usage was similar between the 2 groups (23% DDH vs 26% ACD, P = .22) in this comparison. The 30-day readmission rates in the DDH and ACD groups were similar (11% vs 11%, P = .59).
Subgroup Analysis of PICU Direct Discharge Home Patients That Had a Readmission in 30 Days
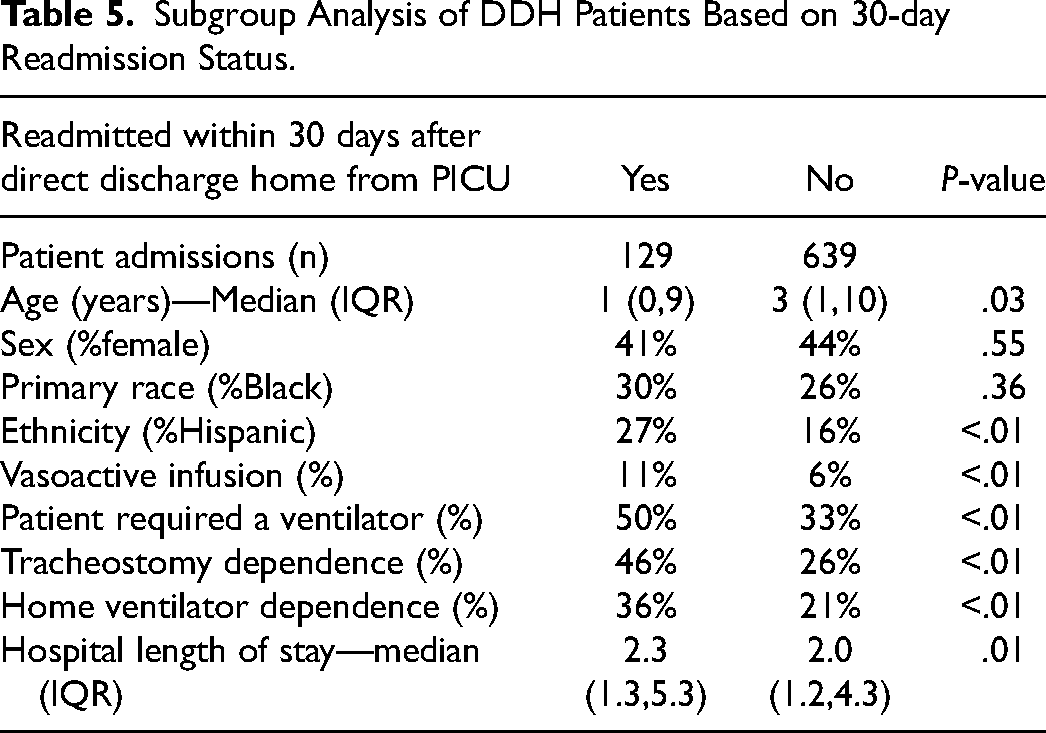
When analyzing DDH patient cases who had a readmission within 30 days compared to those who did not, DDH patients that were readmitted within 30 days were younger (median 1 vs 3 years old, P = .03), more frequently Hispanic (27% vs 16%, P < .01), had higher utilization of vasoactive infusion(s) (11% vs 6%, P = .03), more commonly had tracheostomy dependence (46% vs 26%, P < .01), and home ventilator dependence (36% vs 21%, P < .01) (Table 5).
Subgroup Analysis of DDH Patients Based on 30-day Readmission Status.
Discussion
This study assessed differences between pediatric patients requiring intensive care admission who are directly discharged to home versus those first transferred to an acute ward prior to discharge home with respect to demographics; markers of illness severity; technology dependence; and hospital readmission within 30 days. It adds to the limited pediatric literature on the practice of DDH. Improved characterization of these patient populations and their health outcomes is critical to assess safety and identify ideal patient populations for this increasingly frequent practice.
DDH occurred for 19% of PICU admissions during the study period, which is consistent with published reports of 4% to 44% of patients undergoing DDH.18,19 This represents a significant percentage and indicates that this is an important practice to investigate and better understand. The population of patients that experience DDH is demographically similar to patients who are transferred to the ward before discharge.
DDH and ACD patients differ in markers of illness severity, LOS, ventilator dependence, and common admission diagnosis categories. This suggests that there may be patient and illness characteristics that align better with the practice of DDH. Similar to findings in the adult and pediatric cardiac literature, DDH patients in this analysis had a shorter overall hospital LOS—indicating they either had less severe illness or their disease process recovered quickly. 18 As noted above, DDH patients also had less need for vasoactive infusions, which when coupled with lower LOS may further indicate a lower illness severity or fast recovery.
Our findings are generally consistent with other research in adult and pediatric cardiac critical care units.11,13 Despite the frequency, there is a paucity of data about the risks and outcomes in pediatric patients undergoing DDH. To attempt to better define outcomes for this population, we measured hospital readmission rates. Thirty-day readmission rates were higher in the DDH group overall. Often transfer to acute care floor is not an option for patients with ventilator dependence, depending on hospital policy and overall acuity, resulting in DDH for many patients with home ventilator-dependence. Repeat readmission analysis excluding patients with home ventilator dependence demonstrated similar readmission rates between DDH and ACD patients. Similarly, analyzing only first admissions, we found similar rates between DDH and ACD patients, suggesting that a small proportion of the population with multiple repeat readmissions was contributing to the difference in the primary analysis. This may indicate that the driver of this difference was patients with multiple admissions and those with technology dependence, specifically tracheostomy with home ventilator dependence. This finding is consistent with research from Bucholz et al who demonstrated hospital admissions and readmissions are increasing for children with complex chronic conditions. 20 Similar outcomes have also been reported previously by Tarfa et al, demonstrating a high readmission rate of 44% at 90 days after tracheostomy placement. 16 This supports the concept that these medically complex, technologically dependent patients likely complicate assessment of readmission rate due to higher baseline risk of readmission, which has been previously reported.21,22
In further subgroup analysis of DDH patients readmitted compared to those that were not readmitted, aside from higher rates of tracheostomy and home ventilator dependence, patient factors that were more frequent in DDH patients who were readmitted were younger age, Hispanic ethnicity, and vasoactive infusion administration during admission. Using vasoactive infusion as a surrogate marker for critical illness during hospitalization, this finding may again highlight a baseline increased risk of readmission due to illness rather than be attributed to the process of discharging from the PICU. Individuals of Hispanic ethnicity were more likely to have a 30-day readmission, which may highlight a disparity and need for attention to improved communication efforts at time of discharge home directly from the PICU. Patients with limited English proficiency—or who have primary caregivers with limited English proficiency—may be especially vulnerable to communication-related issues. 23 Given the nature of the study it is difficult to draw significant conclusions from this subgroup analysis, but these variables should be targeted for analysis in future research. In adult patients, similar analyses have been done and factors related to the discharge process (including leaving against medical advice and having community support services) were associated with higher rates of readmission. 18 In the current study we did not examine the discharge process closely or differences between discharge planning for patients DDH from PICU compared with those discharged after transfer to the ward.
Limitations
We present a single center, retrospective study at a multi-disciplinary PICU within a larger healthcare system at an academic tertiary care nested children's hospital, which may limit generalizability. Additionally, due to the retrospective nature of this observational study it is difficult to determine rationale for DDH, reasons for readmission or medical or hospital factors (eg, census) impacting admission duration or discharge location. Utilization of hospital readmissions as a surrogate for safety has additional limitations, as above. Though this approach is utilized in other studies safety would be better determined with long-term morbidity and mortality data that we did not have access to for this study.13,18,19 Determination of severity of illness is also limited in this retrospective cohort study. Use of vasoactive infusion and new mechanical ventilation were used as surrogate markers of severity of illness but data on different acuity scoring systems (such as PRISM III or PIM3) were not available. These type of scoring metrics could provide insight into risk assessment in future studies. 24 As mentioned, these data are also limited due to differences in baseline ventilator-dependence in the groups, which is common in a children's hospital population.
Further research ideally would include multi-site or large database investigations and prospective data collection. To better assess safety, long-term morbidity and mortality data would ideally be collected and reported. If ideal or common populations for DDH could be further elucidated, hospitals could also standardize processes for common DDH populations to ensure safety and consistent discharge planning and follow-up regardless of the discharging unit. Similarly, it would be informative to assess the data after the addition of a discharge coordinator, as this role can be beneficial in decreasing LOS and potentially readmission.25,26
Conclusions
In summary, direct discharge home from the PICU is a common practice. Similar rates of 30 days readmissions were seen between DDH and ACD groups, when patient admissions with home ventilator dependence were excluded. Further research is needed to support the safety of this practice as well as to identify which populations it is most suited to benefit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Department of Pediatrics funding at the University of North Carolina at Chapel Hill.