
Abstract
Background
Critical care transesophageal echocardiography (ccTEE) is an increasingly popular tool used by intensivists to characterize and manage hemodynamics at the bedside. Its usage appears to be driven by expanded diagnostic scope as well as the limitations of transthoracic echocardiography (TTE) – lack of acoustic windows, patient positioning, and competing clinical interests (eg, the need to perform chest compressions). The objectives of this scoping review were to determine the indications, clinical impact, and complications of ccTEE.
Methods
MEDLINE, EMBASE, Cochrane, and six major conferences were searched without a time or language restriction on March 31st, 2021. Studies were included if they assessed TEE performed for adult critically ill patients by intensivists, emergency physicians, or anesthesiologists. Intraoperative or post-cardiac surgical TEE studies were excluded. Study demographics, indication for TEE, main results, and complications were extracted in duplicate.
Results
Of the 4403 abstracts screened, 289 studies underwent full-text review, with 108 studies (6739 patients) included. Most studies were retrospective (66%), performed in academic centers (84%), in the intensive care unit (73%), and were observational (55%). The most common indications for ccTEE were hemodynamic instability, trauma, cardiac arrest, respiratory failure, and procedural guidance. Across multiple indications, ccTEE was reported to change the diagnosis in 52% to 78% of patients and change management in 32% to79% patients. During cardiac arrest, ccTEE identified the cause of arrest in 25% to 35% of cases. Complications of ccTEE included two cases of significant gastrointestinal bleeding requiring intervention, but no other major complications (death or esophageal perforation) reported.
Conclusions
The use of ccTEE has been described for the diagnosis and management of a broad range of clinical problems. Overall, ccTEE was commonly reported to offer additional diagnostic yield beyond TTE with a low observed complication rate. Additional high quality ccTEE studies will permit stronger conclusions and a more precise understanding of the trends observed in this scoping review.
Background
Point-of-care ultrasound (POCUS) has become an important tool for the modern intensivist. 1 An iconic application of POCUS is the assessment of cardiorespiratory failure where critical care echocardiography (CCE – a sub-domain of POCUS) has been shown to rapidly and accurately inform management of the anatomic, hemodynamic and non-cardiac etiologies of shock and is endorsed as a first-line assessment tool for shock by the European Society of Intensive Care Medicine.1–6
While CCE has traditionally been viewed as a transthoracic technique, challenges with patient positioning, limited acoustic windows, and the need to perform other interventions (eg, chest compressions) are common barriers to its use. 7 In response to these challenges, critical care transesophageal echocardiography (ccTEE) has seen increased adoption.8,9 The probe's close proximity to the heart yields reliable, high quality images no matter patient body habitus or positioning. As well, its indwelling nature facilitates serial assessments and the ability to be performed during cardiac arrest without interrupting chest compressions.10,11–13 These factors have led the American Society of Echocardiography to state that a primary indication for TEE is the lack of transthoracic windows in a critically ill patient where echo is expected to change management. 9
ccTEE is a modality of scalable complexity, from goal-directed TEE that uses “core” views to guide resuscitation, 14 to detailed assessments of hemodynamics and the assessment of extra-cardiac structures in the thorax and abdomen.15–17 ccTEE differs from consultative TEE (eg, cardiology performed) in that the ccTEE provider's role in patient care includes the real time integration of findings into diagnosis, hemodynamic management and prognosis. 18
As the literature supporting ccTEE grows, a synthesis of primary studies is expected to aid in understanding and influencing the adoption of ccTEE among intensivists. In conducting this scoping review, our objectives were to characterize the indications, clinical impact, complications and domains requiring further inquiry for the ccTEE modality.
Methods
The study protocol and all data are available on Open Science Framework (OSF) (https://osf.io/fsnt3/). Ethics approval for scoping reviews is not required at our institutions. The study adheres to the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping reviews (PRSIMA-SCR) guidelines. 19
Search Strategy
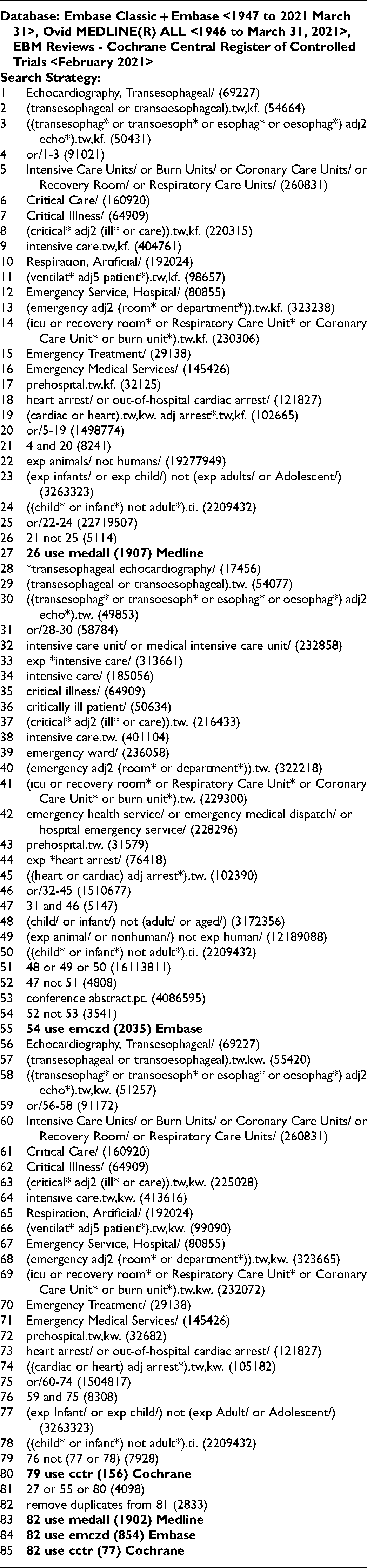
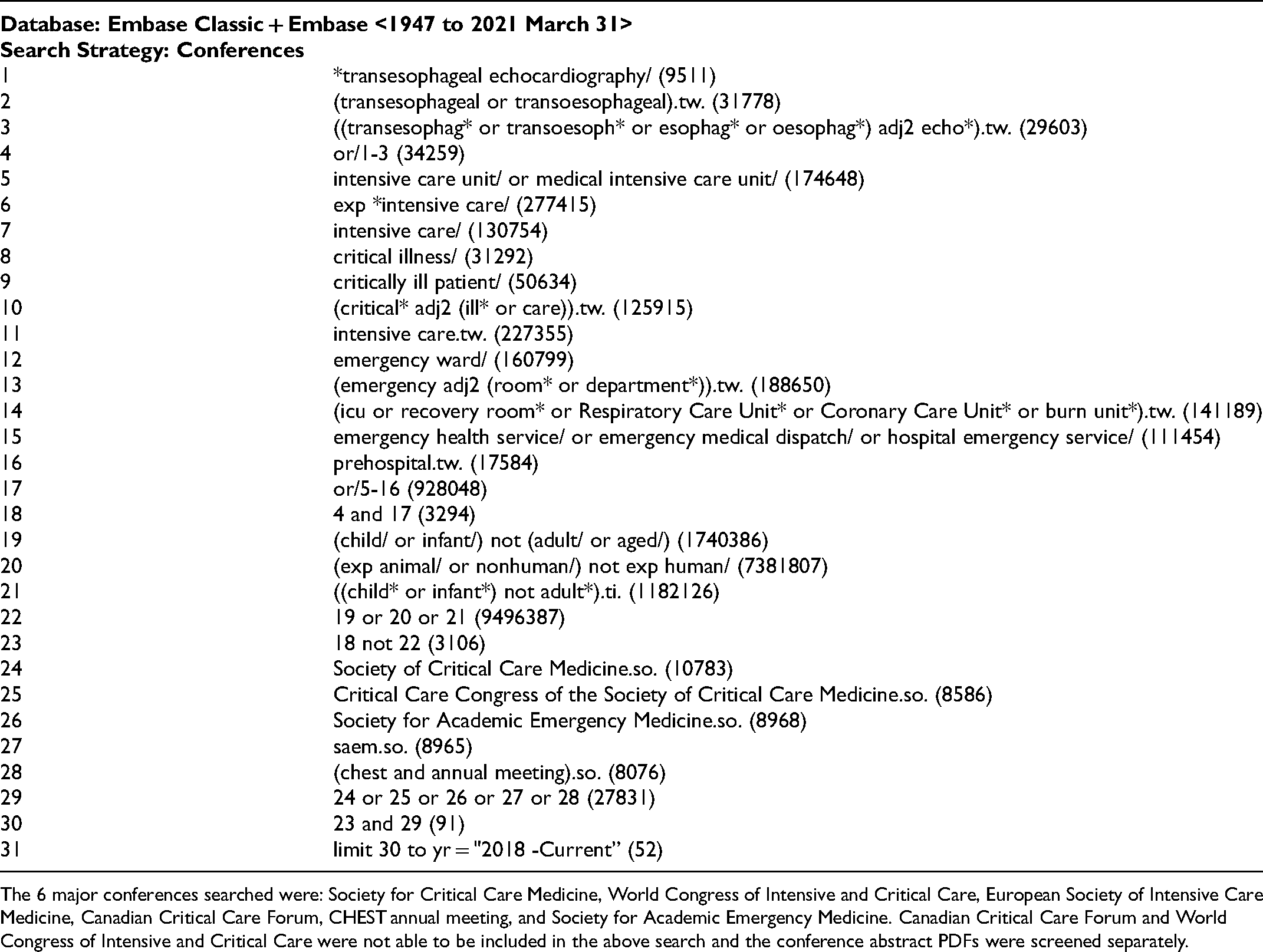
The search strategy was designed with the help of a research librarian (RS) and is summarized in Appendix 1. MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials were searched without a time or language restriction on March 31st, 2021. Clinicaltrials.gov and OSF were also searched for ongoing TEE studies (Appendix 2). Six critical care and emergency medicine conferences had their abstracts searched form 2018 to present (Appendix 3). Any relevant systematic review identified by our search had its references screened. Google Translate (Google, USA) was used for non-English studies with a human translator employed when needed.
Study Selection
Studies were included if they: (1) assessed adult human subjects (≥ 16 years old); (2) investigated the use of TEE in critically ill patients; (3) the TEE was performed in a critical care context with focused indications (as opposed to comprehensive TEE performed by cardiologists); (4) the TEE was performed in the intensive care unit (ICU), emergency department (ED), or pre-hospital setting (eg, ambulance). Goal directed TEE performed by cardiologists were included.
Studies were excluded if they: (1) investigated comprehensive cardiology performed TEE; (2) investigated intra-operative or post-cardiac surgical TEE; (3) used TEE to determine cardiac dimensions without a direct clinical application; (4) were reviews, opinion pieces, educational studies, or letters to the editors.
Covidence software (Veritas Health Innovation, Australia) was used for abstract and full-text screening. Abstracts and full texts were screened independently and in duplicate by 2 authors (RP and JB) with consensus used for discrepancies. Screening of the conference literature was done in duplicate by RP and MP.
Data Extraction
The following data was extracted independently and in duplicate by two authors (RP and JB), with discrepancies resolved through consensus discussion: study author, year of publication, country of corresponding author, setting (academic, community, mixed), study type, study design (prospective, retrospective), clinician performing TEE (intensivist, anesthesiologist, emergency physician), training of clinician performing TEE, number of patients, indication for TEE, primary outcome being measured, main finding(s), and TEE-related complications. Two pilot extractions were done by RP and JB.
Bias Assessment
In keeping with the PRISMA-SCR guidelines, studies were not assessed for applicability, risk of bias, or publication bias.
Outcomes
The primary questions addressed by this review are: (1) What are the reported indications for ccTEE? (2) What is the reported impact of ccTEE on diagnosis, management, and patient outcomes? The secondary questions addressed by this review are: (1) What are the study demographics? (2) What complications are reported for ccTEE?
Analyses
No analyses were performed. Descriptive statistics, count data, and percentages were used for the demographic information of the primary studies. All data extraction was done in Microsoft Excel (Washington, USA).
Results
Study Demographics
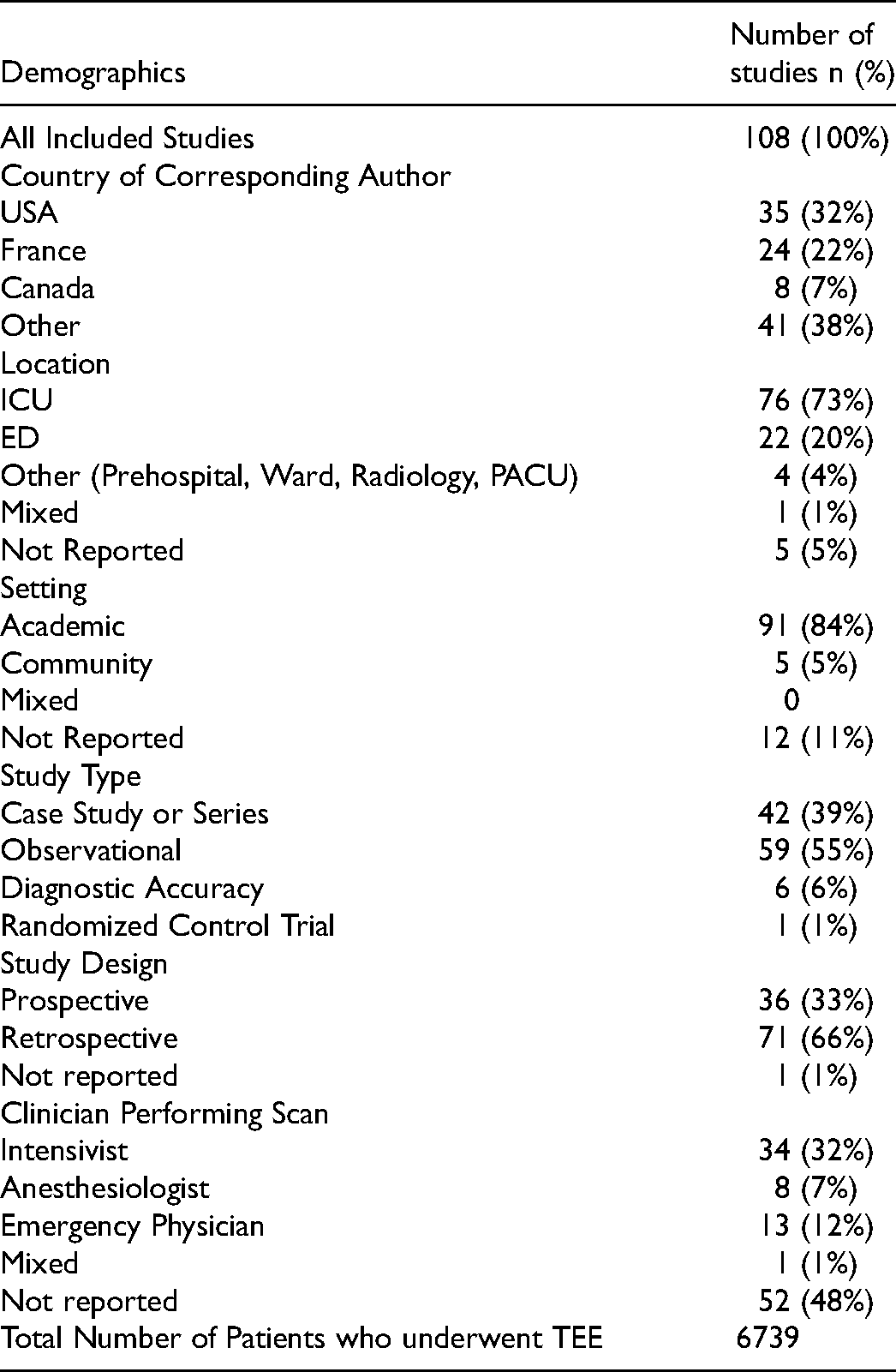
Of the 4403 abstracts screened, 289 studies underwent full-text review, with 108 studies (6739) patients) included (Figure 1). Study demographics are provided in Table 1. Case studies are summarized in Appendix 4. All included studies are listed in Appendix 5.
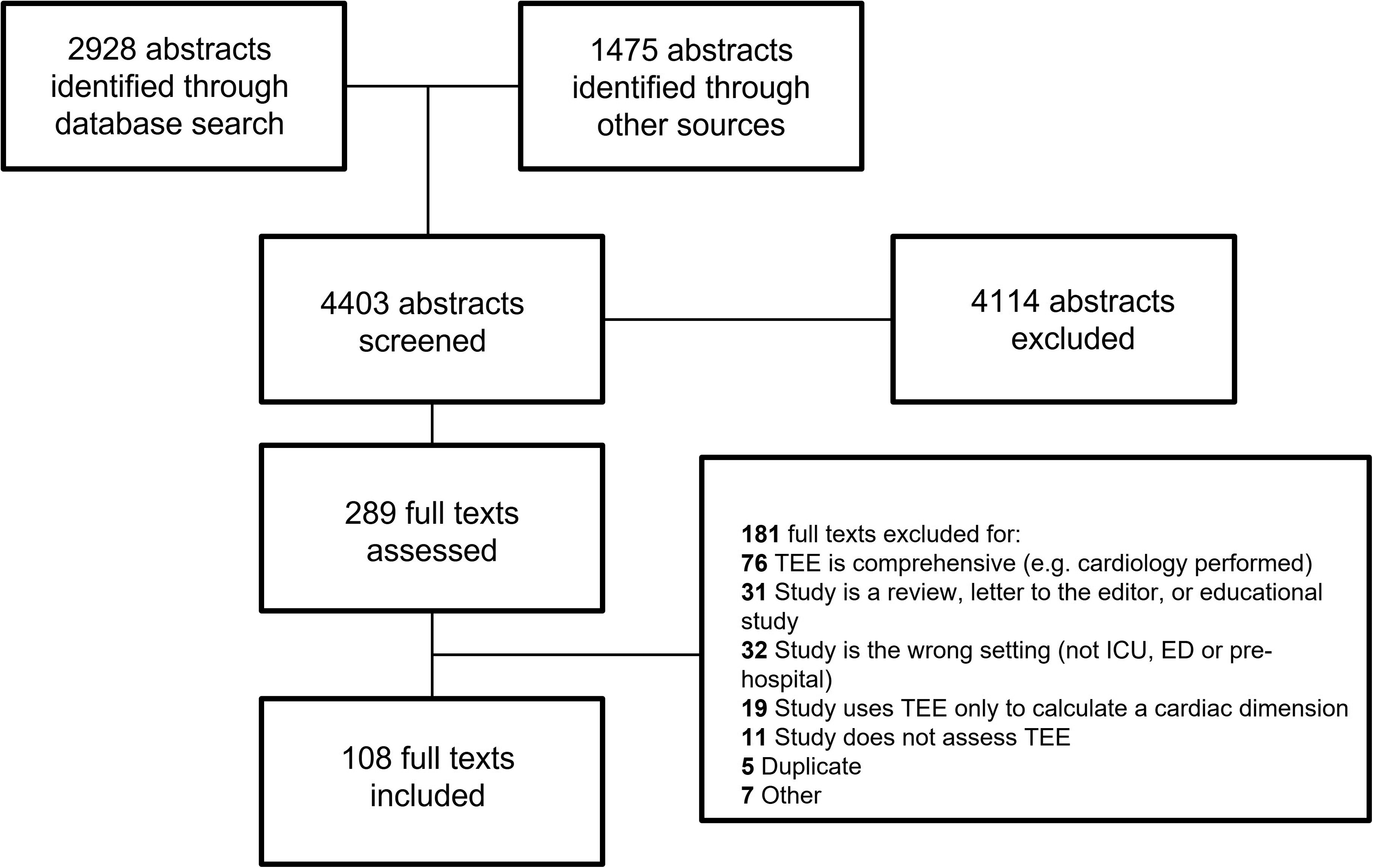
Flow Diagram.
Study Demographics.
ccTEE in Critically Ill Patients
For studies assessing the general use of ccTEE (ie studies not focused on a single indication), the most common indications were to assess hemodynamics (40%-70% of patients),10,20,21 to rule out endocarditis (18%-33% of patients),10,20–22 and for cardiac arrest (20% of patients) (Table 2). 10 ccTEE was reported to help change diagnosis in 52% to 78% of cases23,24 and resulted in a change in management in 32% to 79% of cases.10,20,21,23,25,26 When miniature or disposable TEE probes were compared to standard TEE probes, the miniature probes had similar diagnostic performance for 2 dimensional echocardiography.27–29
Studies That Reported the General Use of ccTEE (ie, Not Limited to One Specific Indication).
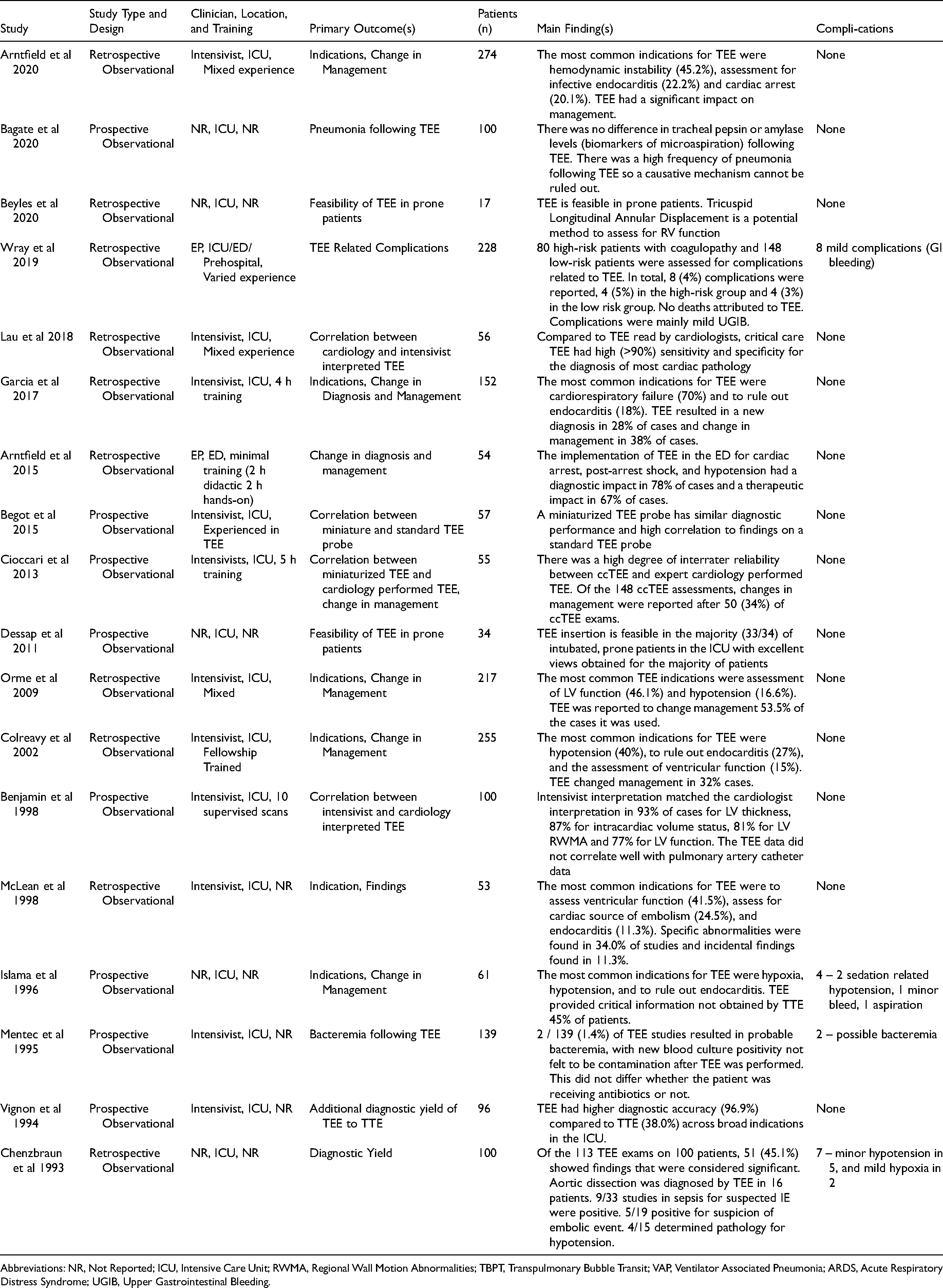
Abbreviations: NR, Not Reported; ICU, Intensive Care Unit; RWMA, Regional Wall Motion Abnormalities; TBPT, Transpulmonary Bubble Transit; VAP, Ventilator Associated Pneumonia; ARDS, Acute Respiratory Distress Syndrome; UGIB, Upper Gastrointestinal Bleeding.
ccTEE to Investigate Hemodynamic Instability and Shock
In many cases, ccTEE was reported to help clarify the etiology of shock (Table 3). ccTEE was used to correctly identify right ventricular (RV) failure from acute pulmonary embolism,30–34 for managing the peripartum patient with hemodynamic collapse,35,36 and for identifying unexpected causes of shock like dynamic left ventricular outflow tract (LVOT) obstruction.37,38 There were a number of case reports of ccTEE identifying rare causes of shock that may not have been visualized on TTE: right atrial compression from intrabdominal hematoma, 39 thoracic tamponade post lung transplant, 40 and regional pericardial tamponade in the ED after discharge home from cardiac surgery. 41 For patients who already had TTE performed, ccTEE resulted in additional changes in management in 40% of cases, and refuted TTE diagnoses in approximately 20% of cases (Table 3).42,43
ccTEE for Shock and Hypotension.
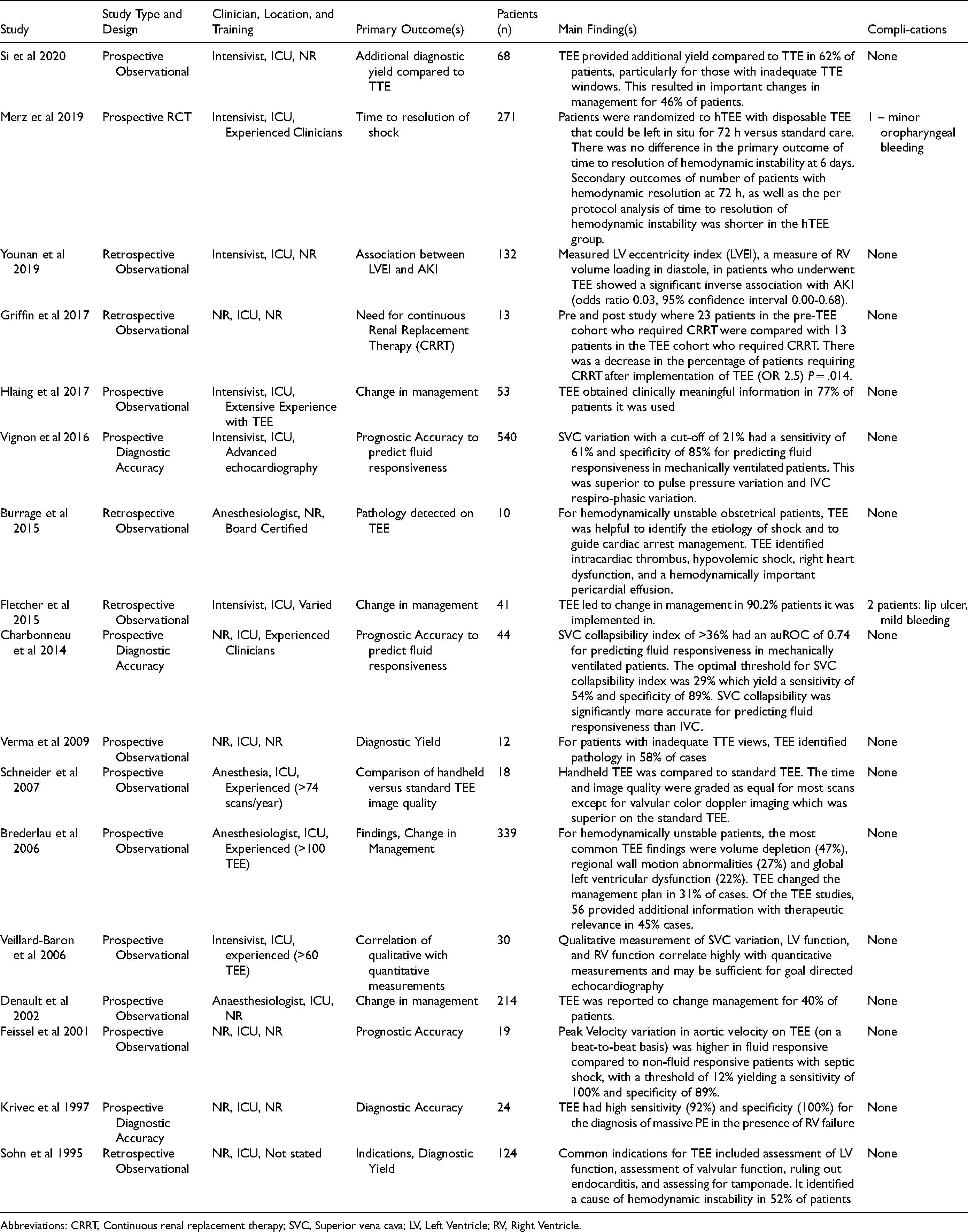
Abbreviations: CRRT, Continuous renal replacement therapy; SVC, Superior vena cava; LV, Left Ventricle; RV, Right Ventricle.
ccTEE use in Cardiac Arrest.
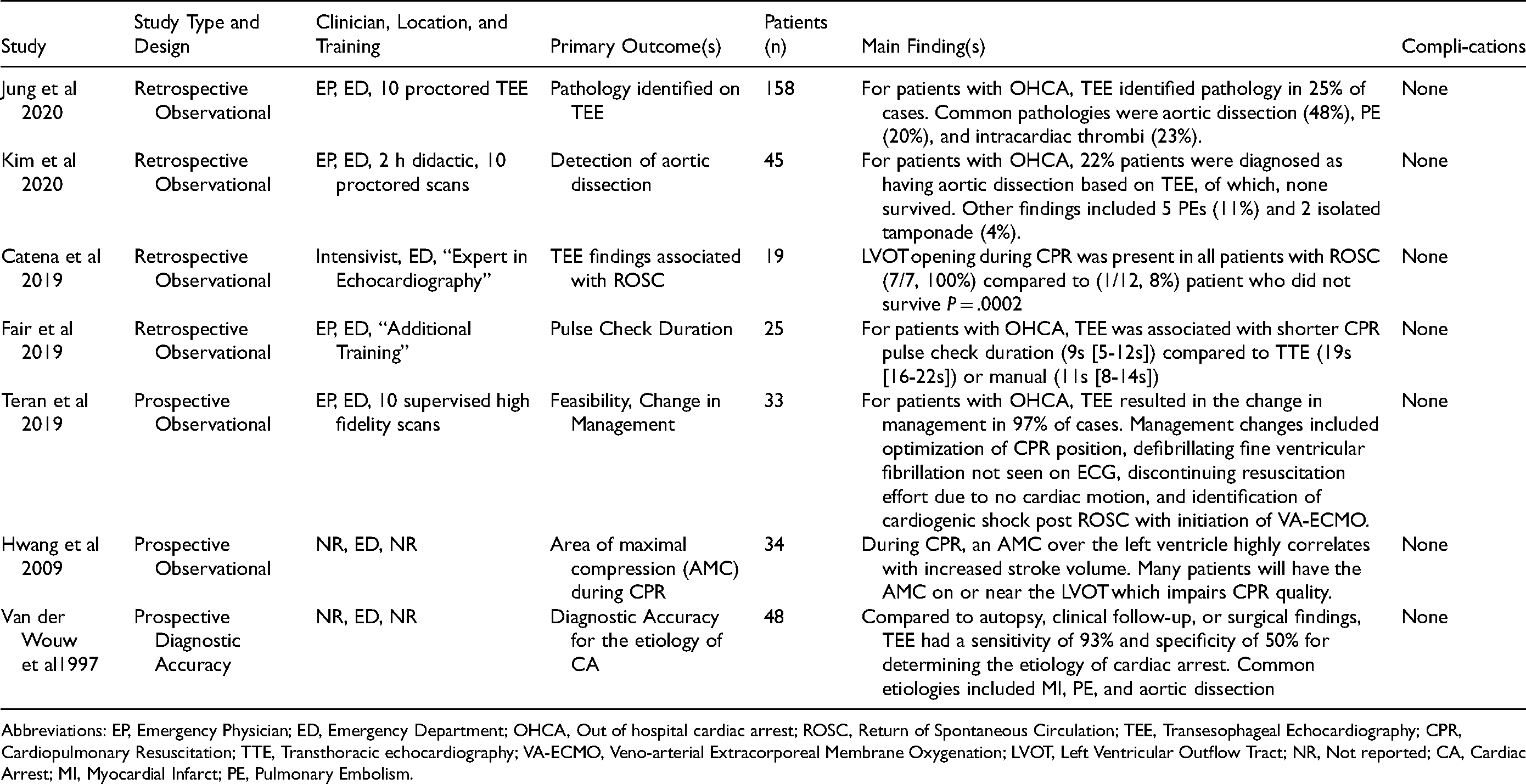
Abbreviations: EP, Emergency Physician; ED, Emergency Department; OHCA, Out of hospital cardiac arrest; ROSC, Return of Spontaneous Circulation; TEE, Transesophageal Echocardiography; CPR, Cardiopulmonary Resuscitation; TTE, Transthoracic echocardiography; VA-ECMO, Veno-arterial Extracorporeal Membrane Oxygenation; LVOT, Left Ventricular Outflow Tract; NR, Not reported; CA, Cardiac Arrest; MI, Myocardial Infarct; PE, Pulmonary Embolism.
For patients in shock, ccTEE was also able to predict fluid responsiveness.44–46 Superior vena cava (SVC) collapsibility assessment performed using TEE had moderate diagnostic accuracy to predict fluid responsiveness, with thresholds for collapsibility of 21% to 29% yielding a sensitivity of 54% to 61% and specificity of 85% to 89%.44,45 ccTEE also identified ventricular failure that resulted in the initiation or titration of vasopressors and inotropes in 4% to 73% of cases.43,47,48
Although most ccTEE studies are observational, a randomized controlled trial (n = 550) was performed to determine whether a disposable TEE (hTEE) impacted time to resolution of hemodynamic instability for critically ill patients. Although there was no difference in the intention-to-treat (ITT) analysis of the primary outcome of resolution of hemodynamic instability at 6 days (sub-hazard ratio (SHR) 1.20, 95% confidence interval (CI) 0.98-1.46), there was a reduction in time to resolution of hemodynamic stability within 72 h of placement of the hTEE probe (SHR 1.26, 95% CI 1.02-1.55). 49
ccTEE use in Cardiac Arrest
ccTEE in cardiac arrest identified the etiology of cardiac arrest in 25% to 35% of cases,50–53 and in one study was reported to change management in 97% of cases in the intra or peri-arrest period. 52 Multiple studies reported that ccTEE identified fine ventricular fibrillation (VF) not seen on surface electrodes.32,36,52 In one study, ccTEE detected pseudo-pulseless electrical activity (PEA) in 28% of cases of PEA, where ventricular contraction occurred but did not generate a palpable pulse. 52 Intra-arrest TEE was reported to improve CPR quality through guiding chest compressions to avoid ineffective compressions over the LVOT or aortic root.11,23,52 Proper compression location over the LV was associated with increased stroke volume generated by chest compressions, and potentially improved survival.13,52,54 ccTEE was also associated with shorter pulse checks when compared to both TTE and manual pulse checks. 11 Using protocols that focus on core TEE views, ccTEE in cardiac arrest was feasible and safe for providers with limited training.11,50–52,55 A summary of the use of ccTEE in cardiac arrest is provided in Table 4.
Procedural Guidance with ccTEE
ccTEE was also used to help guide invasive procedures, including confirming guidewire placement during the initiation of veno-venous (VV) and veno-arterial (VA) extracorporeal membrane oxygenation (ECMO) (Table 5).40,52,55–59 Once ECMO was established, ccTEE was used to troubleshoot flow issues and guide cannula repositioning, which was required in up to 38% of patients in one VV-ECMO cohort. 59 In one small cohort of patients on VA-ECMO, TEE guided weaning protocols performed by intensivists had high predictive accuracy (100%) for successful weaning. 60 TEE was also used to provide real-time guidance for the insertion of transvenous pacemakers.36,61,62
TEE Guided Procedures.
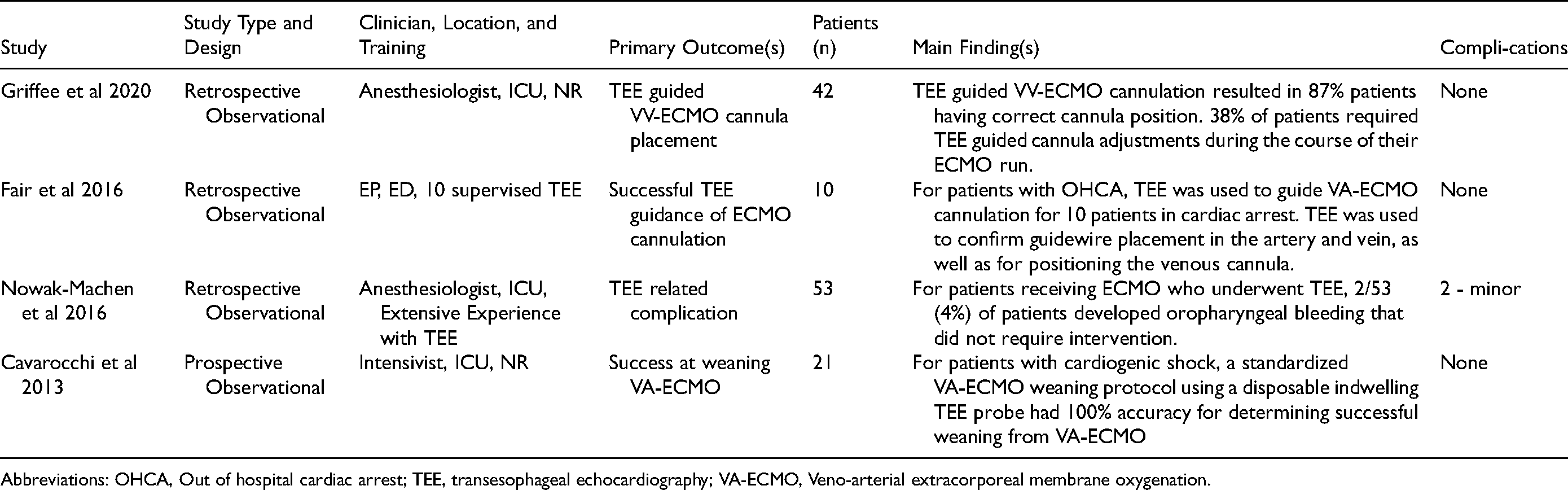
Abbreviations: OHCA, Out of hospital cardiac arrest; TEE, transesophageal echocardiography; VA-ECMO, Veno-arterial extracorporeal membrane oxygenation.
ccTEE use in Trauma
TEE use in trauma had high diagnostic accuracy (>90%) for the detection of traumatic aortic injuries.63–65 After initial surgical hemostasis, TEE helped identify other etiologies of shock including LV and RV dysfunction, blunt cardiac injury, and traumatic valvular abnormalities.66,67 TEE was also described during the management of critically ill burn patients, with its use associated with a change in diagnosis and management in several small studies.68–71 The use of TEE in trauma is summarized in Table 6.
TEE use in Trauma.
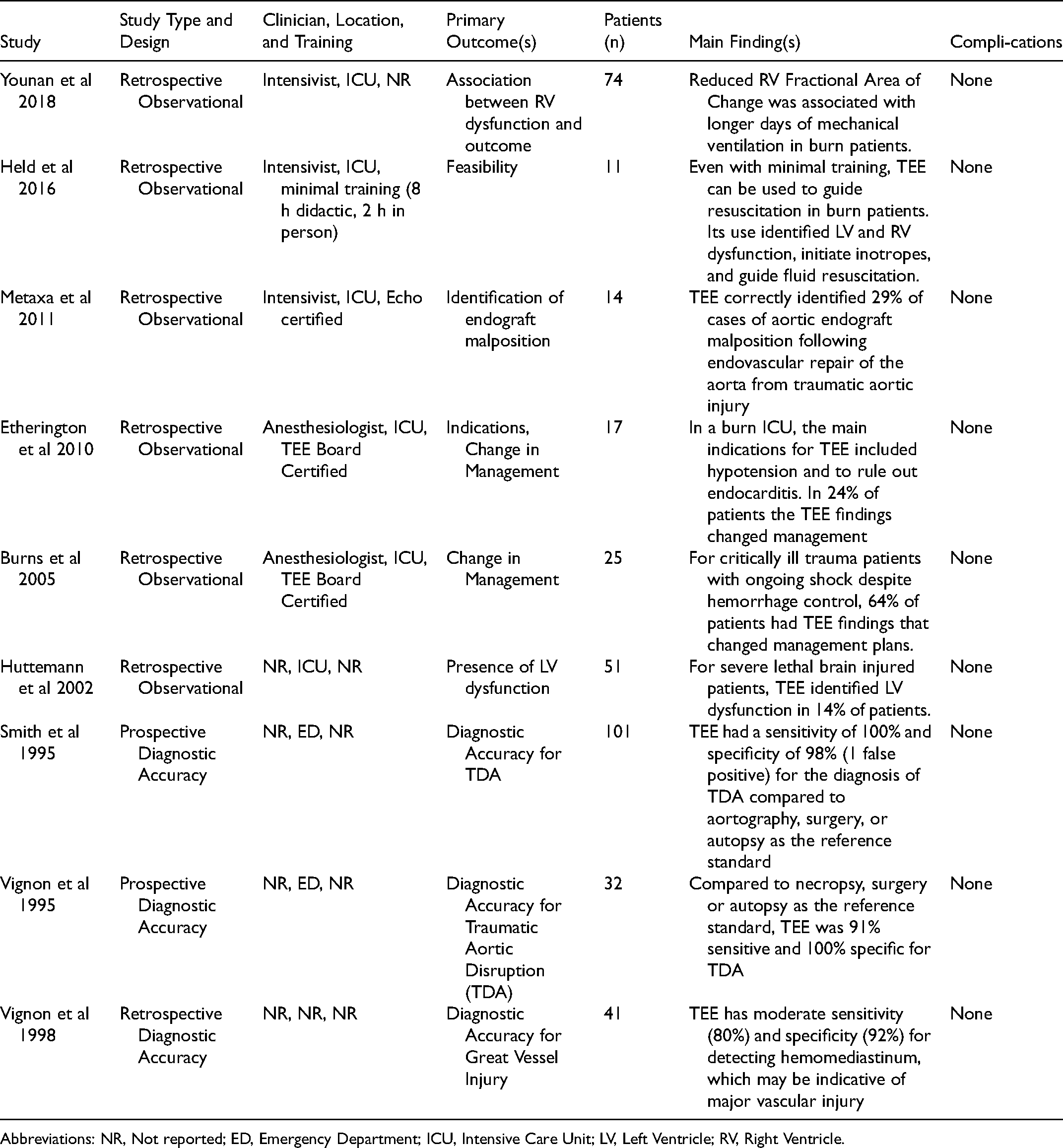
Abbreviations: NR, Not reported; ED, Emergency Department; ICU, Intensive Care Unit; LV, Left Ventricle; RV, Right Ventricle.
TEE use in Respiratory Failure
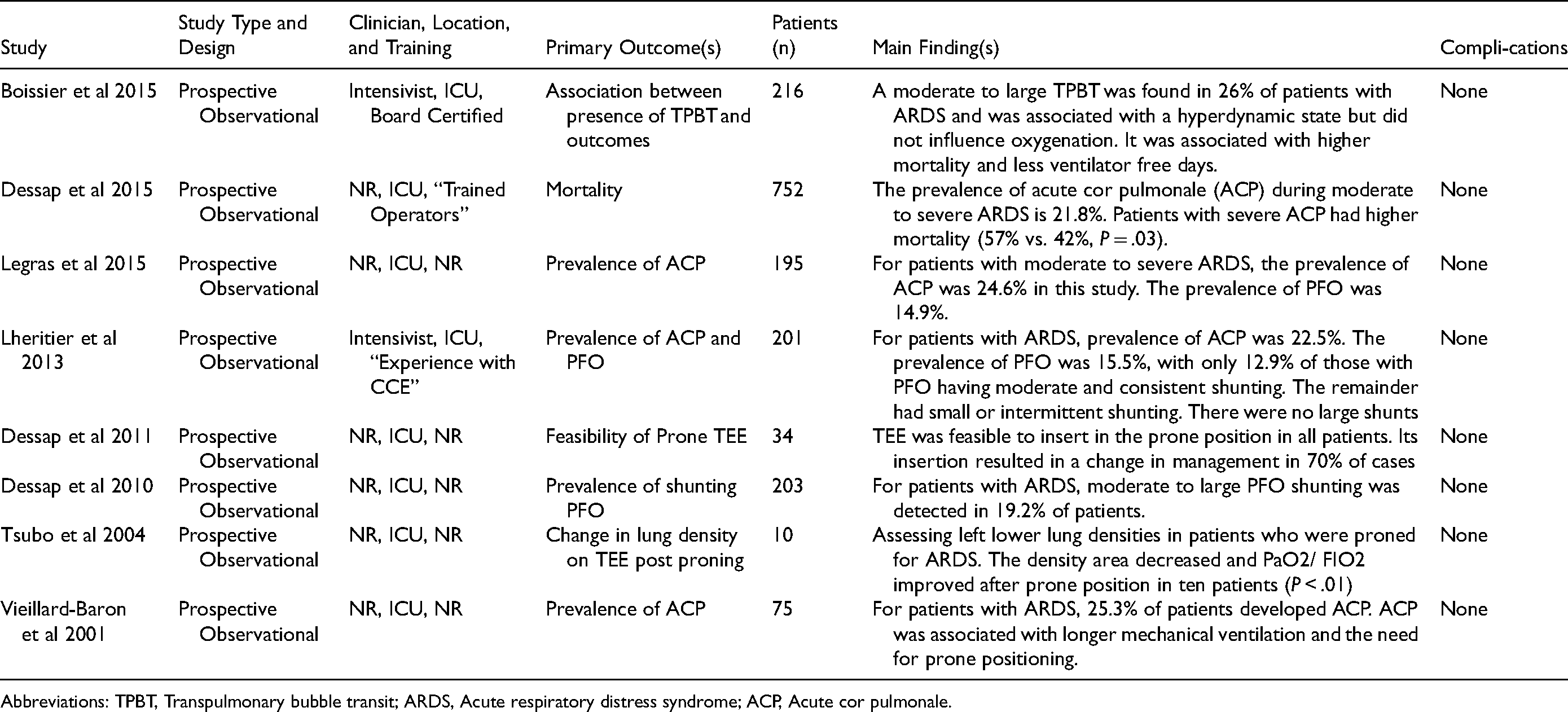
Several studies have described the use of transesophageal lung ultrasound (TELUS), which is effective at identifying basal and posterior lung pathology.72,73 Additionally, ccTEE use in patients with ARDS can identify RV failure and intracardiac shunting.74–77 TEE use in respiratory failure is summarized in Appendix 6 and 7.
TEE-Related Complications
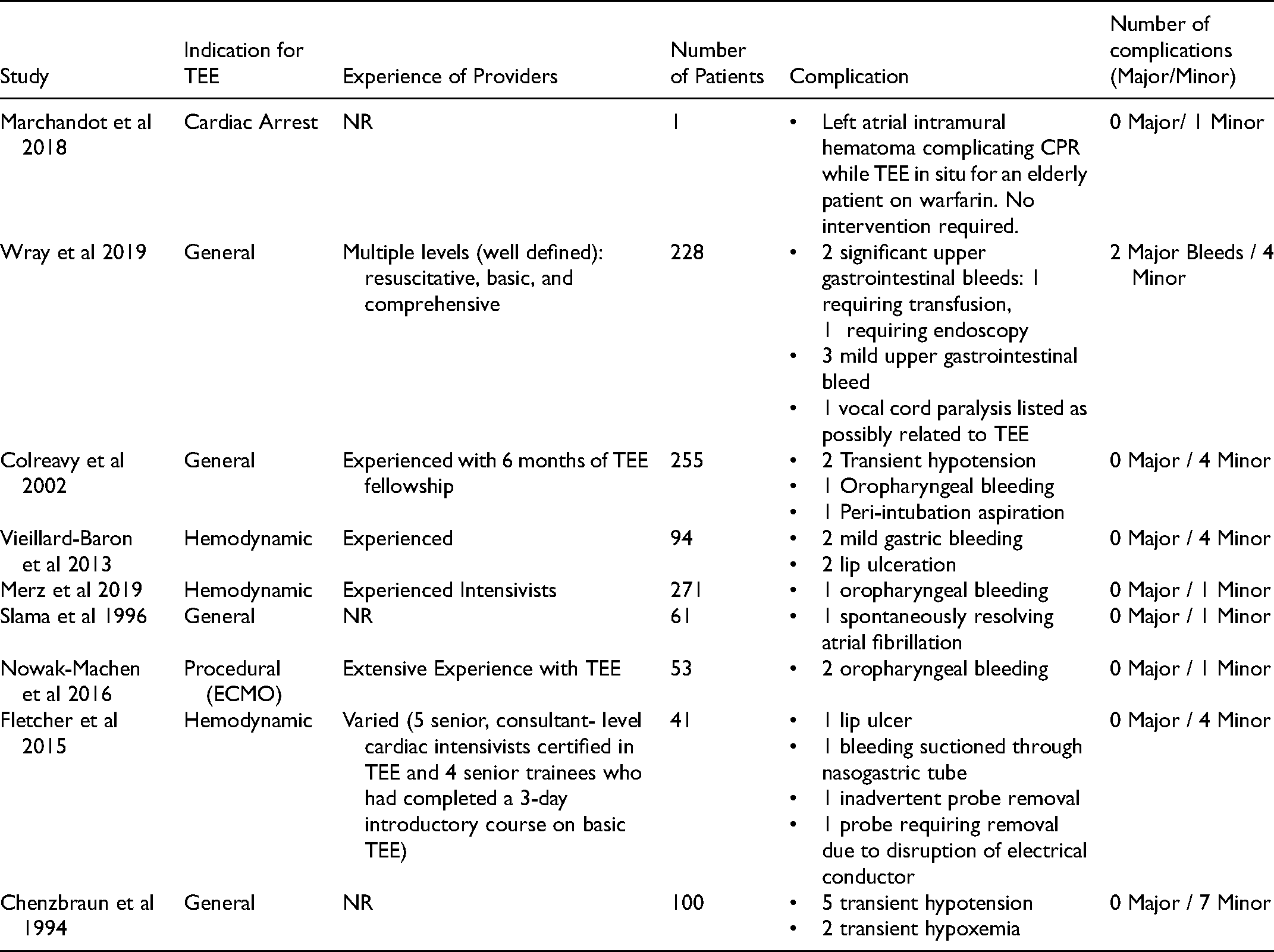
There were two significant gastrointestinal bleeds reported as a complication of ccTEE: one requiring endoscopic intervention, and the other requiring transfusion for hypovolemia. 78 There were no other major ccTEE associated complications (death or esophageal perforation) reported. There were 29 minor complications reported in 6739 patients, with those studies reporting a 1.6% to 9.8% minor complication rate (Table 7). One study identified 2 cases of bacteremia that they felt were likely associated with TEE use. 79 Another showed TEE was not associated with biomarkers of aspiration. 80
Summary of ccTEE Related Complications.
Discussion
The range of applications for ccTEE is broad, from resuscitative views acquired during cardiac arrest to advanced applications that mimic the complexity of consultative TEE. 18 Given the relative infancy of ccTEE, it's evidentiary base consists largely of case studies and retrospective observational studies, however, there are a number of well-designed prospective studies advancing the field. The existing ccTEE literature has characterized the indications for ccTEE and highlighted cases of additional diagnostic yield compared to TTE but has not consistently demonstrated improvement in patient important outcomes from the integration of ccTEE into existing diagnostic pathways. This is not surprising given the number of steps required for a diagnostic test to improve outcomes: correct patient selection, acquisition, interpretation, synthesis, and then implementation of a therapy with proven benefit, however, still remains an important goal for future research to enhance adoption of ccTEE. 81
ccTEE for the Patient in Shock
For the patient in shock, a transthoracic approach is typically used given its availability and non-invasive nature. In many critically ill patients, however, transthoracic windows are limited.10,42 For these patients, ccTEE is indicated and may give additional diagnostic yield beyond TTE.42,43,82
Perhaps the most powerful application of ccTEE is its ability to quickly phenotype shock and identify causes that have targeted treatments such as pulmonary embolism, effusion, or severe ventricular dysfunction.30–40,83,84 Its use to phenotype shock is valuable even when only core “resuscitative” TEE views are used, although refining management often requires additional views and quantitative measurements. A simplified “resuscitative” ccTEE protocol like the one shown in Figure 2 allows for the assessment of LV and RV function, pericardial disease, and catastrophic valvular failure. 23 Given the scalable complexity of ccTEE, these core views can be safely and effectively performed by intensivists with only focused training. 85
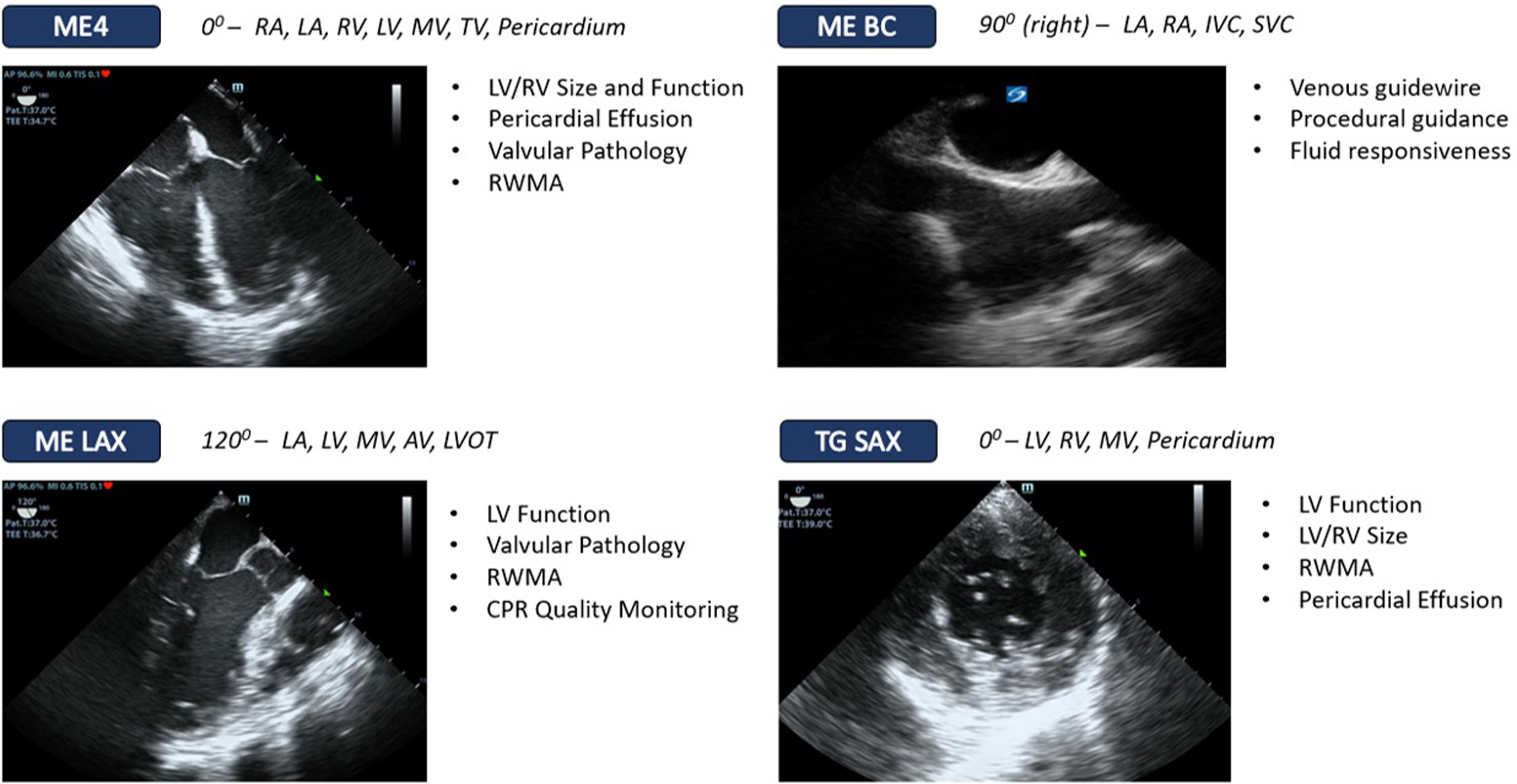
Resuscitative ccTEE views used for phenotyping of shock in the unstable patient Legend. Abbreviations: ME4, Mid-esophageal 4 chamber; MEBC, Mid-esophageal bicaval; MELAX, mid-esophageal long axis; TG SAX, Transgastric short axis; LA, Left Atrium; RA, Right Atrium; MV, Mitral Valve; TV, Tricuspid Valve; AV, aortic valve; LVOT, Left Ventricular Outflow Tract; LV, Left Ventricle; RV, Right Ventricle; RWMA, Regional Wall Motion Abnormalities; CPR, Cardiopulmonary Resuscitation.
After phenotyping shock, ccTEE can play an important role in refining its ongoing management through titration of fluids, inotropes, and vasoactive medications. One approach to fluid resuscitation is to restrict IV fluids to patients with proven fluid responsiveness with signs of end organ hypoperfusion. Transthoracic approaches to predicting fluid responsiveness have variable diagnostic accuracy and generalizability, in part due to requirements for patients to be ventilated, not spontaneously breathing, and in sinus rhythm.44,45,86–89 ccTEE measured SVC respiratory variability is an attractive approach to assessing fluid responsiveness given its relative ease of acquisition, repeatability, and moderate predictive accuracy, however, additional prospective studies are needed to properly define positivity thresholds.44–46
For patients with ventricular failure, ccTEE is valuable to provide serial assessments of biventricular function during the titration of inotropes, as well as non-invasive cardiac output assessment using LVOT velocity time integral measurements (VTI). Although thermodilution derived cardiac output measurements from pulmonary artery catheters have similar accuracy to TEE, 90 ccTEE provides the advantage of offering anatomic information that may also inform the mechanism behind any distorted cardiac output physiology.
Given the diagnostic potential of ccTEE for the management of shock, there are a number of areas for future research. Prospective studies assessing ccTEE markers of fluid responsiveness are needed to determine the diagnostic accuracy and thresholds for test positivity. Ultimately, however, studies assessing the impact on patient important outcomes from integrating ccTEE into resuscitation paradigms are needed to help justify more widespread adoption of the technique.
ccTEE use During Cardiac Arrest
POCUS use in cardiac arrest has been adopted by many clinicians, particularly for the identification of reversible causes and futility of further resuscitation.91,92 Despite its enthusiastic implementation, some studies suggests POCUS TTE is associated with longer pulse checks, which is antithetical to high quality CPR.11,93 TEE affords reliable acoustic windows to guide clinicians without interfering with chest compressions or prolonging pulse checks. 11 This can help identify arrythmias like ventricular fibrillation not seen on ECG (Video 3),32,36,52 and also distinguish true pulseless electrical activity (PEA) from pseudo-PEA, with the latter having higher survival rates and the potential to respond to pharmacologic therapies.52,94
The use of ccTEE in cardiac arrest also has the potential to improve CPR quality. The American Heart Association suggests to perform compressions mid chest on the lower portion of the sternum compressing to a depth of at least 5cm, 95 however, from observational TEE data this results in almost half of chest compressions occurring over the LVOT or aortic root. CPR over the aortic root in animal and human studies is ineffective, with little cardiac output generated and poor survival.13,52,96 ccTEE can be used to reposition compressions over the LV in real-time (Videos 1 & 2). 52
There are several areas for future research for intra-arrest TEE. These include the feasibility of implementing intra-arrest TEE to improve CPR quality and whether this correlates with improved proximal (end-tidal CO2 and arterial pressure) and distal outcomes (ROSC and survival). Additionally, as more intra-arrest TEE is performed and pseudo-PEA is detected, determining the optimal therapeutic management of this entity is needed.
Procedural use of ccTEE
ccTEE also has a role for the initiation and management of patients on ECMO. In some centers, ECMO cannulation is done with fluoroscopic guidance, however, TEE guided cannulation is an alternate strategy that may increase its portability.55,58
For centers performing ECMO, the ability to troubleshoot flow problems and catheter placement is essential. TEE can help identify catheter misplacement, recirculation of venous blood, and mechanical complications from the cannula. Additionally, the weaning of VA-ECMO requires serial assessments of ventricular function which is feasible by intensivists and provides flexibility with respect to the timing of weaning trials, however, the optimal strategy for VA-ECMO weaning is still an area of important research. 60
ccTEE use in Trauma
In trauma, the extended focused assessment with sonography in trauma (eFAST) exam has become a well integrated into acute resuscitation. The role of ccTEE in trauma patients is poorly defined, however, it has been shown to be feasible with some diagnostic value in select clinical cases.63–65,97 Regional mediastinal or pericardial hemorrhage in particular, typically occult to TTE, can be readily identified on TEE.17,41 Additionally, when there are no transabdominal or transthoracic windows due to subcutaneous emphysema or body habitus, ccTEE can potentially sequence immediate priorities or disposition. The “TREE” protocol for acute trauma resuscitation TEE focuses on identifying hypovolemia, aortic injuries, pericardial disease, and pleural pathology, 98 however, prospective studies validating its use are lacking.
Given the relative paucity of studies assessing ccTEE use in trauma, prospective research assessing the feasibility of integrating ccTEE into the management of major trauma is warranted to ensure that it offers additional diagnostic information to existing trauma algorithms, and that it does not delay the sequencing of other life saving interventions or disposition.
ccTEE use for Respiratory Failure
A natural extension to TEE use for shock has been for the evaluation of patients with severe respiratory failure. These patients may have acute cor pulmonale and intracardiac shunting that can be identified with ccTEE.74–76,99,100 Identifying these pathologies may help optimize ventilation strategies, PEEP, and the use of inhaled pulmonary vasodilators.
Additionally, transesophageal lung ultrasound (TELUS) is highly effective at imaging the posterior and basal lung zones, which often contain pathology for the intubated critically ill patient (Video 4). 73 TELUS can detect significant consolidation that may account for clinically important hypoxia, even when it is not visible on chest x-ray. 73 Additional research to assess the diagnostic accuracy of TELUS and also the impact of TEE guided lung recruitments is needed (Video 5 & 6).
Safety of ccTEE
Probe insertion is a commonly cited concern for clinicians learning ccTEE. The complication rate of ccTEE in the literature is low, with no major complications such as death or perforation reported, although there is likely underreporting due to the retrospective nature and ad-hoc reporting of studies. Gastrointestinal bleeding is a known risk of TEE, however, most cases are self limited and do not require intervention. 78 As well, incomplete reporting of whether patients were intubated limits the ability to generalize complication rates to different ICU populations. Additional prospective research systematically screening for complications is important to ensure that clinicians can accurately weigh the risks and benefits of ccTEE.
Limitations
There are several limitations to this study. Incomplete reporting of primary TEE studies, particularly with respect to who performed the TEE, made it difficult to assess whether the TEE was consultative or goal-directed. In these cases, discussion between authors was used to generate consensus using other domains like the setting (eg, ED or pre-hospital) and indication (eg, cardiac arrest) to help determine whether the TEE was comprehensive or ccTEE. Given this and the scope of this review, there is likely incomplete retrieval of the ccTEE literature. As well, ad-hoc reporting of complications in many studies means that the true complication rate is still unknown and is an important area for future research.
Conclusions
Although critical care TEE is still in its relative infancy, the indications and clinician-reported impact of ccTEE have been preliminarily characterized. Additional studies evaluating the impact of ccTEE on patient outcomes are still forthcoming and will assuredly have the greatest impact on priority domains for ccTEE adoption.
Footnotes
Abbreviations
Abstract Presentation
This work has been presented in abstract form at the Canadian Critical Care Forum on December eighth 2021 in Toronto, Canada.
Acknowledgments
None.
Author Contributions
RP takes responsibility for the content of the manuscript, including the study design, data extraction, data analysis, and manuscript writing. RP, MP, JB, JC, MM, and RA all contributed to the study design, data analysis, data interpretation, and manuscript writing. RP, MP, JB all performed data extraction.
Availibility of Data and Materials
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethics approval is not required for this scoping reviews at the authors institutions as it does not involve human participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Search strategy.
|
|
|
|
|
|
| 1 | Echocardiography, Transesophageal/ (69227) |
| 2 | (transesophageal or transoesophageal).tw,kf. (54664) |
| 3 | ((transesophag* or transoesoph* or esophag* or oesophag*) adj2 echo*).tw,kf. (50431) |
| 4 | or/1-3 (91021) |
| 5 | Intensive Care Units/ or Burn Units/ or Coronary Care Units/ or Recovery Room/ or Respiratory Care Units/ (260831) |
| 6 | Critical Care/ (160920) |
| 7 | Critical Illness/ (64909) |
| 8 | (critical* adj2 (ill* or care)).tw,kf. (220315) |
| 9 | intensive care.tw,kf. (404761) |
| 10 | Respiration, Artificial/ (192024) |
| 11 | (ventilat* adj5 patient*).tw,kf. (98657) |
| 12 | Emergency Service, Hospital/ (80855) |
| 13 | (emergency adj2 (room* or department*)).tw,kf. (323238) |
| 14 | (icu or recovery room* or Respiratory Care Unit* or Coronary Care Unit* or burn unit*).tw,kf. (230306) |
| 15 | Emergency Treatment/ (29138) |
| 16 | Emergency Medical Services/ (145426) |
| 17 | prehospital.tw,kf. (32125) |
| 18 | heart arrest/ or out-of-hospital cardiac arrest/ (121827) |
| 19 | (cardiac or heart).tw,kw. adj arrest*.tw,kf. (102665) |
| 20 | or/5-19 (1498774) |
| 21 | 4 and 20 (8241) |
| 22 | exp animals/ not humans/ (19277949) |
| 23 | (exp infants/ or exp child/) not (exp adults/ or Adolescent/) (3263323) |
| 24 | ((child* or infant*) not adult*).ti. (2209432) |
| 25 | or/22-24 (22719507) |
| 26 | 21 not 25 (5114) |
| 27 |
|
| 28 | *transesophageal echocardiography/ (17456) |
| 29 | (transesophageal or transoesophageal).tw. (54077) |
| 30 | ((transesophag* or transoesoph* or esophag* or oesophag*) adj2 echo*).tw. (49853) |
| 31 | or/28-30 (58784) |
| 32 | intensive care unit/ or medical intensive care unit/ (232858) |
| 33 | exp *intensive care/ (313661) |
| 34 | intensive care/ (185056) |
| 35 | critical illness/ (64909) |
| 36 | critically ill patient/ (50634) |
| 37 | (critical* adj2 (ill* or care)).tw. (216433) |
| 38 | intensive care.tw. (401104) |
| 39 | emergency ward/ (236058) |
| 40 | (emergency adj2 (room* or department*)).tw. (322218) |
| 41 | (icu or recovery room* or Respiratory Care Unit* or Coronary Care Unit* or burn unit*).tw. (229300) |
| 42 | emergency health service/ or emergency medical dispatch/ or hospital emergency service/ (228296) |
| 43 | prehospital.tw. (31579) |
| 44 | exp *heart arrest/ (76418) |
| 45 | ((heart or cardiac) adj arrest*).tw. (102390) |
| 46 | or/32-45 (1510677) |
| 47 | 31 and 46 (5147) |
| 48 | (child/ or infant/) not (adult/ or aged/) (3172356) |
| 49 | (exp animal/ or nonhuman/) not exp human/ (12189088) |
| 50 | ((child* or infant*) not adult*).ti. (2209432) |
| 51 | 48 or 49 or 50 (16113811) |
| 52 | 47 not 51 (4808) |
| 53 | conference abstract.pt. (4086595) |
| 54 | 52 not 53 (3541) |
| 55 |
|
| 56 | Echocardiography, Transesophageal/ (69227) |
| 57 | (transesophageal or transoesophageal).tw,kw. (55420) |
| 58 | ((transesophag* or transoesoph* or esophag* or oesophag*) adj2 echo*).tw,kw. (51257) |
| 59 | or/56-58 (91172) |
| 60 | Intensive Care Units/ or Burn Units/ or Coronary Care Units/ or Recovery Room/ or Respiratory Care Units/ (260831) |
| 61 | Critical Care/ (160920) |
| 62 | Critical Illness/ (64909) |
| 63 | (critical* adj2 (ill* or care)).tw,kw. (225028) |
| 64 | intensive care.tw,kw. (413616) |
| 65 | Respiration, Artificial/ (192024) |
| 66 | (ventilat* adj5 patient*).tw,kw. (99090) |
| 67 | Emergency Service, Hospital/ (80855) |
| 68 | (emergency adj2 (room* or department*)).tw,kw. (323665) |
| 69 | (icu or recovery room* or Respiratory Care Unit* or Coronary Care Unit* or burn unit*).tw,kw. (232072) |
| 70 | Emergency Treatment/ (29138) |
| 71 | Emergency Medical Services/ (145426) |
| 72 | prehospital.tw,kw. (32682) |
| 73 | heart arrest/ or out-of-hospital cardiac arrest/ (121827) |
| 74 | ((cardiac or heart) adj arrest*).tw,kw. (105182) |
| 75 | or/60-74 (1504817) |
| 76 | 59 and 75 (8308) |
| 77 | (exp Infant/ or exp child/) not (exp Adult/ or Adolescent/) (3263323) |
| 78 | ((child* or infant*) not adult*).ti. (2209432) |
| 79 | 76 not (77 or 78) (7928) |
| 80 |
|
| 81 | 27 or 55 or 80 (4098) |
| 82 | remove duplicates from 81 (2833) |
| 83 |
|
| 84 |
|
| 85 |
|
Appendix 2. Search strategy for clinicaltrials.gov and Open Science Framework
| Line | Search |
|---|---|
| 1 | Transesophageal |
| 2 | Transoesophageal |
| 3 | TEE |
| 4 | 1 OR 2 OR 3 |
Appendix 3. Search strategy for conference abstracts
|
|
|
|
|
|
| 1 | *transesophageal echocardiography/ (9511) |
| 2 | (transesophageal or transoesophageal).tw. (31778) |
| 3 | ((transesophag* or transoesoph* or esophag* or oesophag*) adj2 echo*).tw. (29603) |
| 4 | or/1-3 (34259) |
| 5 | intensive care unit/ or medical intensive care unit/ (174648) |
| 6 | exp *intensive care/ (277415) |
| 7 | intensive care/ (130754) |
| 8 | critical illness/ (31292) |
| 9 | critically ill patient/ (50634) |
| 10 | (critical* adj2 (ill* or care)).tw. (125915) |
| 11 | intensive care.tw. (227355) |
| 12 | emergency ward/ (160799) |
| 13 | (emergency adj2 (room* or department*)).tw. (188650) |
| 14 | (icu or recovery room* or Respiratory Care Unit* or Coronary Care Unit* or burn unit*).tw. (141189) |
| 15 | emergency health service/ or emergency medical dispatch/ or hospital emergency service/ (111454) |
| 16 | prehospital.tw. (17584) |
| 17 | or/5-16 (928048) |
| 18 | 4 and 17 (3294) |
| 19 | (child/ or infant/) not (adult/ or aged/) (1740386) |
| 20 | (exp animal/ or nonhuman/) not exp human/ (7381807) |
| 21 | ((child* or infant*) not adult*).ti. (1182126) |
| 22 | 19 or 20 or 21 (9496387) |
| 23 | 18 not 22 (3106) |
| 24 | Society of Critical Care Medicine.so. (10783) |
| 25 | Critical Care Congress of the Society of Critical Care Medicine.so. (8586) |
| 26 | Society for Academic Emergency Medicine.so. (8968) |
| 27 | saem.so. (8965) |
| 28 | (chest and annual meeting).so. (8076) |
| 29 | 24 or 25 or 26 or 27 or 28 (27831) |
| 30 | 23 and 29 (91) |
| 31 | limit 30 to yr = "2018 -Current” (52) |
The 6 major conferences searched were: Society for Critical Care Medicine, World Congress of Intensive and Critical Care, European Society of Intensive Care Medicine, Canadian Critical Care Forum, CHEST annual meeting, and Society for Academic Emergency Medicine. Canadian Critical Care Forum and World Congress of Intensive and Critical Care were not able to be included in the above search and the conference abstract PDFs were screened separately.
Study design, indication, main findings, and complications for TEE case studies and small case series

| Author and year | Study Design, Clinician and Level of Training | Indication | # of pts | Main Findings | Complications |
|---|---|---|---|---|---|
| Jelic et al, 2017 | Case Study, EP, NR | Cardiac Arrest | 1 | 86F presented w/ dyspnea, then went into PEA. TEE performed for diagnosis and management. Findings of large RV; small and hyperdynamic LV; distended noncollapsing SVC; suggestive of PE. TEE used for monitoring CPR quality and prognostication. | None |
| Saranteas et al, 2010 | Case Series, Intensivist, NR | Hemodynamic | 2 | Case 1 - 36M in MVC who required splenectomy. Day 5 in ICU experienced hemodynamic instability prompting TEE. Dense echogenic material identified on TEE coating the catheter in SVC consistent with thrombus. Case 2 - 30F post-op day 35 cesarian section found to have anti-phospholipid antibody syndrome. Deteriorated in ICU and TEE performed for hemodynamic instability. TEE detected thrombus formation in the SVC associated with a central line. | None |
| Agrawal et al, 2020 | Case Study, Intensivist, NR | Hemodynamic | 1 | 49M admitted to ICU for mixed respiratory failure secondary to pneumonia. On day 7 suffered hypoxic cardiac arrest. Post-ROSC TEE showed large RV, dilated IVC, large clot in main and right pulmonary artery. Diagnosis of PE made. Also found atrial septal aneurysm and right-to-left shunt through PFO. | None |
| Absalom et al, 1997 | Case Series, NR, NR | Trauma | 2 | Patient 1: 17F TEE performed in ICU following blunt trauma with a new murmur. TEE identified a dissection flap that was surgically repaired. Patient 2: 17M TEE performed given high energy mechanism, which showed a dissection flap that led to transfer and surgical repair | None |
| Lerner et al, 2019 | Case Study, EP, TEE credentialed | Cardiac Arrest | 1 | 82F cardiac arrest. TEE inserted to determine etiology of arrest and to improve CPR quality. Post-ROSC the patient was bradycardic and TEE was used to guide and position of transvenous pacemaker as difficult passing it blindly. | None |
| Giorgetti et al, 2019 | Case Study, EP, NR | Cardiac Arrest | 1 | 47M cardiac arrest. TEE used to rule out reversible causes, then was used to position hands for chest compressions to avoid compression over LVOT. Then TEE was used to confirm guidewire placement for VA-ECMO cannulation. | None |
| Orihashi et al, 2020 | Case Series, NR, NR | Cardiac Arrest | 4 | Case 1: 60F cardiac arrest. ECMO initiated. TEE failed to show retrograde flow in the aorta which identified a misplaced arterial cannula. Case 2: 40M flatline ECG but TEE showed fine ventricular fibrillation which was successfully defibrillated. Case 3: 60F cardiac arrest. TEE identified PE and also used to guide a transvenous pacemaker into proper position Case 4: 30F following vaginal birth cardiac arrest. TEE did not suggest amniotic fluid embolism. Instead, showed hypovolemia, increasing pericardial effusion, and intrabdominal hemorrhage. | None |
| Merlin et al, 2019 | Case Study, EP, 2 h didactic and 2 h of hands-on | Cardiac Arrest | 1 | 51F cardiac arrest. TEE inserted by pre-hospital physician to help identify cause of arrest. Cardiac motion seen so a small bolus of epinephrine and IV fluids were given and CPR held. ROSC obtained. | None |
| Rublee et al, 2020 | Case Study, EP, NR | Cardiac Arrest | 1 | 59M PEA cardiac arrest. TEE showed moderate pericardial effusion. Pericardiocentesis showed blood. TEE identified type A dissection and patient taken to OR. | None |
| Horowitz et al, 2021 | Case Study, Intensivist, NR | Cardiac Arrest | 1 | 34M COVID with RV failure and subsequent cardiac arrest. TEE showed clot in transit. Used to position compressions over LV. | None |
| Krishnan et al, 2013 | Case Series, NR, NR | Procedural | 2 | Case 1: 71M inadequate TTE views. TEE used to guide transvenous pacemaker insertion. Case 2: 68M inadequate TTE views. TEE used to guide femoral transvenous pacemaker insertion | None |
| Cooper et al, 2000 | Case Study, NR, NR | Trauma | 1 | 60M polytrauma. TEE on day 2 identified partial dehiscence of left coronary cusp of aortic valve. Subsequent hemodynamic deterioration with identified worsening aortic insufficiency. Taken to OR with complete repair. | None |
| Fagnoul et al, 2013 | Case Study, NR, NR | Hemodynamic | 1 | 92M who suffered cardiac arrest. Post-ROSC was in cardiogenic shock and TEE performed was performed pre intra-aortic balloon pump insertion which identified thrombus, leading to cessation of the procedure. | None |
| Leuverink et al, 2019 | Case Study, NR, NR | Hemodynamic | 1 | 36F with refractory shock post laparoscopic cholecystectomy. TEE performed in ICU showed external compression of right atrium from an intrabdominal hematoma by the liver. Laparotomy resolved hematoma. | None |
| Mocavero et al, 2012 | Case Study, NR, NR | Hemodynamic | 1 | 70M with IVC filter in ICU with shock. TEE showed severe TR and an IVC filter tangled in the tricuspid valve. Taken to OR with successful surgical repair. | None |
| Poppe et al, 2021 | Case Study, NR, NR | Cardiac Arrest | 1 | 40F witnessed cardiac arrest. TEE intra-arrest positioned mechanical CPR device over LV then identified free floating thrombus in right atrium leading to thrombolysis. | None |
| Lee et al, 2019 | Case Study, NR, NR | Cardiac Arrest | 1 | 54M cardiac arrest. TEE initially showed small intimal tear in descending aorta. Post ROSC patient found to have pericardial effusion but no proximal dissection. Felt to be due to direct myocardial bleeding from CPR. | None |
| Koroneos et al, 2006 | Case Study, NR, NR | Cardiac Arrest | 1 | 53M 24 days post intracranial hemorrhage who suffered cardiac arrest in ICU. TEE showed RV dilation with clot in transit. Received thrombolytics with achievement of ROSC. | None |
| Lam et al, 2016 | Case Study, NR, NR | Cardiac Arrest | 1 | 65F polytrauma who had a cardiac arrest on post-admission day 4. TEE demonstrated pneumocardium following needle thoracostomy suggesting potential iatrogenic introduction of air from the procedure. | None |
| Lau et al, 2012 | Case Study, NR, NR | Hemodynamic | 1 | 46M 6 weeks post mitral valve replacement with new onset shock. TTE negative. TEE showed fibrous pericardial effusion with tamponade physiology, with resolved hemodynamics post operation. | None |
| Hsieh et al, 2003 | Case Study, NR, NR | Cardiac Arrest | 1 | 45F suffered PEA arrest in recovery room following laparoscopic vaginal hysterectomy. TEE showed clot in transit. Treated with IV heparin. | None |
| Awad et al, 2006 | Case Study, NR, NR | Hemodynamic | 1 | 68F chest pain and cardiac arrest. Post -ROSC ECG suggestive of inferior STEMI. TEE performed show clot in right atrium suggestive of PE. Patient treated with IV heparin with improvement. | None |
| Blaivas et al, 2008 | Case Series, EP, Experience with ECHO, 2 h of TEE video | Cardiac Arrest | 6 | Case 1: 35M PEA arrest. TEE showed cardiac motion without palpable pulse. CPR stopped and inopressors up-titrated with ROSC. Case 2: 73F cardiac arrest. ECG showed asystole. TEE showed VF and patient defibrillated. Eventually found to be hyperkalemic and treated with ROSC. Case 3: 73F cardiac arrest. ECG showed asystole, TEE showed VF which was defibrillated with subsequent ROSC. TEE also identified atrial clot going into RV. Case 4: 45M cardiac arrest. ECG asystole, TEE showed VF. successfully defibrillated. Case 5: 37M hx DVT/PE with cardiac arrest. Presumed PE, however, TEE showed a type A dissection. Taken to OR with successful repair and recovery. Case 6: 61F with prolonged intermittent VF and asystolic arrest. TEE showed VF when monitor was asystole. Successful defibrillation with ROSC, however, ultimately died. | None |
| Osman et al, 2020 | Case Series, EP, NR | Trauma | 5 | Case 1: 88F MVC unstable with hemothorax. TEE showed medial flap along ascending aorta suggestive of ruptured traumatic aortic injury which was confirmed on autopsy. Case 2: 73M with 20 foot fall and chest pain and cardiac tamponade. TEE which showed aortic dissection and patient was taken to OR for repair. Case 3: 55M MVC. Limited TTE views and concern for tamponade. TEE showed blunt aortic injury which was taken to the OR. Case 4: 17M MVC. TTE showed possible intimal flap, however, TEE ruled it out. Case 5: 16M motorcycle injury. TEE used to rule out tamponade but confirm traumatic aortic dissection. | None |
| Simpson et al, 2006 | Case Study, NR, NR | Hemodynamic | 1 | 80F admitted with fevers who had hemodynamic collapse post admission day 3. TEE showed dilated RV, clot in the IVC, RA, and pulmonary HTN consistent with PE. Patient received TPA but unfortunately died. | None |
| Hulin et al, 2016 | Case Series, Intensivist, National Board of Echocardiography Certification | Hemodynamic | 6 | Multiple cases describing the feasibility of TEE to detect abnormal hepatic vein flows, which could suggestive either local or systemic obstructive patterns (RV dysfunction, abdominal compartment syndrome, clot compressing venous return). | None |
| Peng et al, 2007 | Case Study, NR, NR | Hemodynamic | 1 | 45F undergoing dialysis line insertion with hemodynamic collapse. TEE identified large hemothorax compressing the right atrium. Drained with improvement in hemodynamics. | None |
| Krishnamoorthy et al, 2011 | Case Series, NR, NR | Hemodynamic | 1 | 27F fulminant hepatic failure with shock. TEE left in situ for 72 h. TEE identified a clot at the cavo-atrial junction + RV dilation and thickening. Felt that the patient had chronic micro-embolism leading to RV dysfunction. Treated with anticoagulation with improvement. Ultimately diagnosed with catastrophic anti-phospholipid antibody syndrome. | None |
| Kelly et al, 2019 | Case Study, NR, NR | Cardiac Arrest | 1 | 64M cardiac arrest. TEE used to position mechanical CPR device and confirm guidewire placement for ECMO. TEE identified dissection flap so ECMO not initiated. | None |
| Nowack et al, 2019 | Case Series, Intensivist, NR | Trauma | 4 | Case 1: 32M gun shot wound to chest, subsequent respiratory failure, TEE used to rationalize giving additional transfusion Case 2: 72M post appendectomy, intubated, TEE used to rationalize additional fluid resuscitation Case 3: 58M MVC TEE used to diagnose hypovolemia and give additional fluids Case 4: 24M spinal cord injury and neurogenic shock, TEE used to diagnose concurrent hypovolemia and guide resuscitation. | None |
| Wei et al, 2010 | Case Study, NR, NR | Cardiac Arrest | 1 | 36F post partum day 2 following c-section, TEE showed possible thrombus in pulmonary artery which was confirmed on 3 dimensional TEE. This led to initiation of VA ECMO and pulmonary thrombectomy with survival with good function. | None |
| Frietman et al, 2001 | Case Study, NR, NR | Trauma | 1 | 32M skydiving accident. Aortic arch rupture. TEE initially did not show any clear cardiac abnormality and could not visualize aorta. Patient placed on VV-ECMO for hypoxia. Day 4, TEE repeated showing papillary muscle rupture which was not seen on initial TEE. Underwent successful repair of arch and mitral valve. | None |
| Wagner et al, 2011 | Case Study, NR, NR | Hemodynamic | 1 | 73F with cardiac arrest. Miniaturized hemodynamic TEE post ROSC used to guide resuscitation and showed improvement in cardiac function from post ROSC hour 2 to hour 9. | None |
| Tsai et al, 2009 | Case Study, NR, NR | Cardiac Arrest | 1 | 58F post op day 10 radical hysterectomy with cardiac arrest. TEE showed massive clot in RA which was dislodged through suctioning through a central venous cannula and shaking the patient. The patient regained ROSC and went for ECMO then thrombectomy with discharge and good neurologic outcome. | None |
| Denault et al, 2003 | Case Study, NR, American Board of Anesthesia | Hemodynamic | 1 | 65F post single lung transplant with shock and hypoxia. TEE showed intermittent compression of the right atrium and RV outflow track, ultimately, in keeping with thoracic tamponade secondary to a non-compliant lung post-transplant. TEE then successfully used to guide ECMO cannulation and to wean from ECMO. | None |
| Turnage et al, 1993 | Case Study, NR, NR | Hemodynamic | 1 | 62F with CHF and shock. TTE limited views. TEE found dynamic LV outflow tract obstruction which improved with Esmolol. | None |
| Cavallaro et al, 2010 | Case Study, NR, NR | Hemodynamic | 1 | 77F retroperitoneal hematoma with hypotension, TEE showed systolic anterior motion of the mitral valve with severe subaortic obstruction. | None |
| Mazzeffi et al, 2013 | Case Study, NR, NR | Procedural | 1 | 53F with ARDS and ECMO placement. Poor flows with TEE identifying ECMO cannula in the RV which was repositioned with improvement in flows. | None |
| Marchandot et al, 2018 | Case Study, NR, NR | Cardiac Arrest | 1 | 84F on warfarin for Afib who had a cardiac arrest while undergoing TEE. After ROSC, a left atrial intramural hematoma was noted. This was stable on repeat imaging and didn't require intervention. | Yes |
| Poularas et al, 2009 | Case Study, NR, NR | Trauma | 1 | 26M polytrauma with sup-capsular splenic hematoma. Not well visualized on transabdominal imaging, but able to be monitored for stability with TEE. | None |
| Liu et al, 2019 | Case Series, NR, NR | Cardiac Arrest | 4 | Case1: 45M out-of-hospital cardiac arrest. TEE used to guide compression over LV Case 2: 84F cardiac arrest, mechanical CPR over aorta which was repositioned with TEE Case3: 54M COPD cardiac arrest. TEE identified compressions over LVOT which were repositioned. Case 4:74F with cardiac arrest, TEE identified compressions of inadequate depth and that they were over the LVOT. Repositioned hand placement with ROSC. | None |
| Evrard et al, 2020 | Case Series, NR, NR | Hemodynamic | 5 | It is feasible to perform TEE for monitoring hemodynamics of prone patients with COVID19. Of the 5 cases, there were no hemodynamic changes in 3; In one case, severe MR and SAAM was detected. | None |
Abbreviations: EP, Emergency Physician; NR, Not reported; PEA, Pulseless Electrical Activity; RV, Right Ventricle; LV, Left Ventricle; SVC, Superior Vena Cava: MVC, Motor Vehicle Collision; ROSC, Return of Spontaneous Circulation; VA-ECMO, Veno-arterial extracorporeal membrane oxygenation; IVC, Inferior Vena Cava.
List of all included studies and case reports
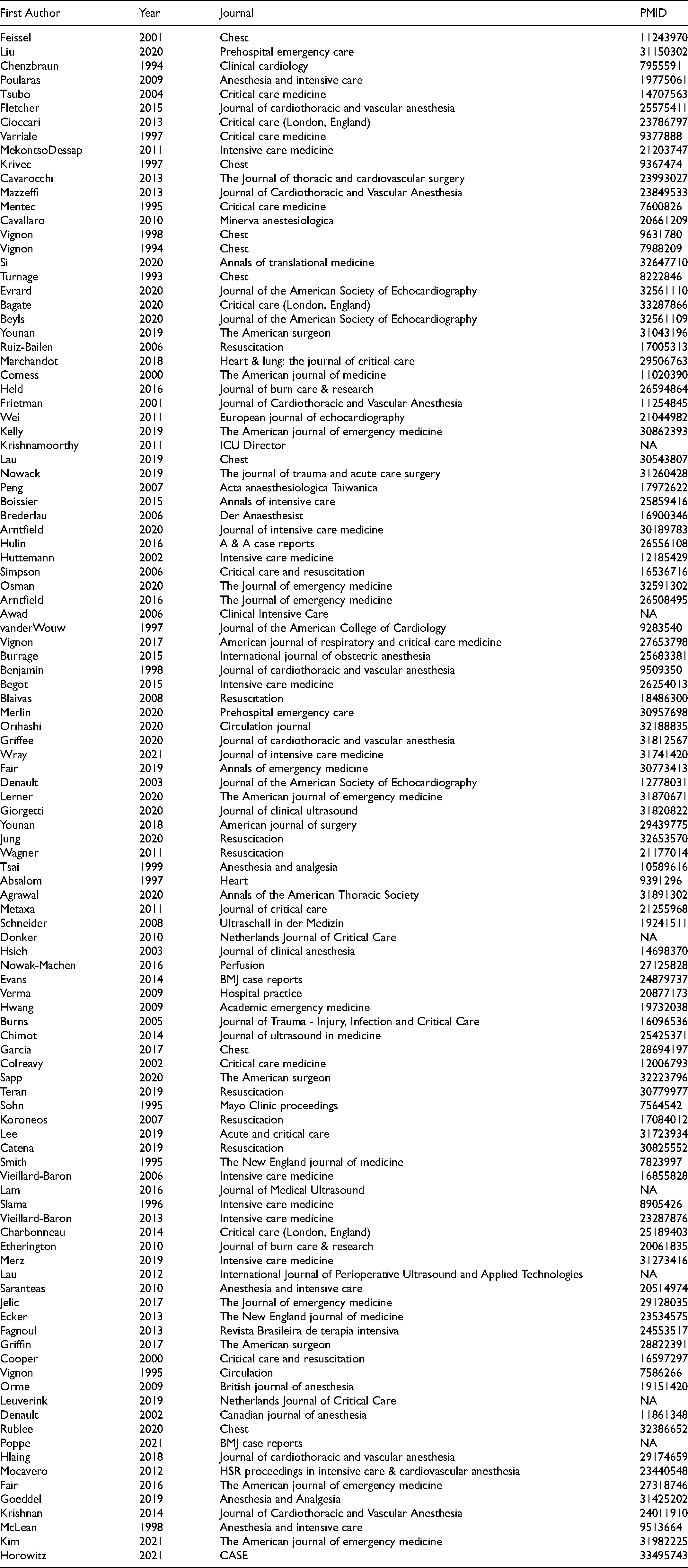
| First Author | Year | Journal | PMID |
|---|---|---|---|
| Feissel | 2001 | Chest | 11243970 |
| Liu | 2020 | Prehospital emergency care | 31150302 |
| Chenzbraun | 1994 | Clinical cardiology | 7955591 |
| Poularas | 2009 | Anesthesia and intensive care | 19775061 |
| Tsubo | 2004 | Critical care medicine | 14707563 |
| Fletcher | 2015 | Journal of cardiothoracic and vascular anesthesia | 25575411 |
| Cioccari | 2013 | Critical care (London, England) | 23786797 |
| Varriale | 1997 | Critical care medicine | 9377888 |
| MekontsoDessap | 2011 | Intensive care medicine | 21203747 |
| Krivec | 1997 | Chest | 9367474 |
| Cavarocchi | 2013 | The Journal of thoracic and cardiovascular surgery | 23993027 |
| Mazzeffi | 2013 | Journal of Cardiothoracic and Vascular Anesthesia | 23849533 |
| Mentec | 1995 | Critical care medicine | 7600826 |
| Cavallaro | 2010 | Minerva anestesiologica | 20661209 |
| Vignon | 1998 | Chest | 9631780 |
| Vignon | 1994 | Chest | 7988209 |
| Si | 2020 | Annals of translational medicine | 32647710 |
| Turnage | 1993 | Chest | 8222846 |
| Evrard | 2020 | Journal of the American Society of Echocardiography | 32561110 |
| Bagate | 2020 | Critical care (London, England) | 33287866 |
| Beyls | 2020 | Journal of the American Society of Echocardiography | 32561109 |
| Younan | 2019 | The American surgeon | 31043196 |
| Ruiz-Bailen | 2006 | Resuscitation | 17005313 |
| Marchandot | 2018 | Heart & lung: the journal of critical care | 29506763 |
| Comess | 2000 | The American journal of medicine | 11020390 |
| Held | 2016 | Journal of burn care & research | 26594864 |
| Frietman | 2001 | Journal of Cardiothoracic and Vascular Anesthesia | 11254845 |
| Wei | 2011 | European journal of echocardiography | 21044982 |
| Kelly | 2019 | The American journal of emergency medicine | 30862393 |
| Krishnamoorthy | 2011 | ICU Director | NA |
| Lau | 2019 | Chest | 30543807 |
| Nowack | 2019 | The journal of trauma and acute care surgery | 31260428 |
| Peng | 2007 | Acta anaesthesiologica Taiwanica | 17972622 |
| Boissier | 2015 | Annals of intensive care | 25859416 |
| Brederlau | 2006 | Der Anaesthesist | 16900346 |
| Arntfield | 2020 | Journal of intensive care medicine | 30189783 |
| Hulin | 2016 | A & A case reports | 26556108 |
| Huttemann | 2002 | Intensive care medicine | 12185429 |
| Simpson | 2006 | Critical care and resuscitation | 16536716 |
| Osman | 2020 | The Journal of emergency medicine | 32591302 |
| Arntfield | 2016 | The Journal of emergency medicine | 26508495 |
| Awad | 2006 | Clinical Intensive Care | NA |
| vanderWouw | 1997 | Journal of the American College of Cardiology | 9283540 |
| Vignon | 2017 | American journal of respiratory and critical care medicine | 27653798 |
| Burrage | 2015 | International journal of obstetric anesthesia | 25683381 |
| Benjamin | 1998 | Journal of cardiothoracic and vascular anesthesia | 9509350 |
| Begot | 2015 | Intensive care medicine | 26254013 |
| Blaivas | 2008 | Resuscitation | 18486300 |
| Merlin | 2020 | Prehospital emergency care | 30957698 |
| Orihashi | 2020 | Circulation journal | 32188835 |
| Griffee | 2020 | Journal of cardiothoracic and vascular anesthesia | 31812567 |
| Wray | 2021 | Journal of intensive care medicine | 31741420 |
| Fair | 2019 | Annals of emergency medicine | 30773413 |
| Denault | 2003 | Journal of the American Society of Echocardiography | 12778031 |
| Lerner | 2020 | The American journal of emergency medicine | 31870671 |
| Giorgetti | 2020 | Journal of clinical ultrasound | 31820822 |
| Younan | 2018 | American journal of surgery | 29439775 |
| Jung | 2020 | Resuscitation | 32653570 |
| Wagner | 2011 | Resuscitation | 21177014 |
| Tsai | 1999 | Anesthesia and analgesia | 10589616 |
| Absalom | 1997 | Heart | 9391296 |
| Agrawal | 2020 | Annals of the American Thoracic Society | 31891302 |
| Metaxa | 2011 | Journal of critical care | 21255968 |
| Schneider | 2008 | Ultraschall in der Medizin | 19241511 |
| Donker | 2010 | Netherlands Journal of Critical Care | NA |
| Hsieh | 2003 | Journal of clinical anesthesia | 14698370 |
| Nowak-Machen | 2016 | Perfusion | 27125828 |
| Evans | 2014 | BMJ case reports | 24879737 |
| Verma | 2009 | Hospital practice | 20877173 |
| Hwang | 2009 | Academic emergency medicine | 19732038 |
| Burns | 2005 | Journal of Trauma - Injury, Infection and Critical Care | 16096536 |
| Chimot | 2014 | Journal of ultrasound in medicine | 25425371 |
| Garcia | 2017 | Chest | 28694197 |
| Colreavy | 2002 | Critical care medicine | 12006793 |
| Sapp | 2020 | The American surgeon | 32223796 |
| Teran | 2019 | Resuscitation | 30779977 |
| Sohn | 1995 | Mayo Clinic proceedings | 7564542 |
| Koroneos | 2007 | Resuscitation | 17084012 |
| Lee | 2019 | Acute and critical care | 31723934 |
| Catena | 2019 | Resuscitation | 30825552 |
| Smith | 1995 | The New England journal of medicine | 7823997 |
| Vieillard-Baron | 2006 | Intensive care medicine | 16855828 |
| Lam | 2016 | Journal of Medical Ultrasound | NA |
| Slama | 1996 | Intensive care medicine | 8905426 |
| Vieillard-Baron | 2013 | Intensive care medicine | 23287876 |
| Charbonneau | 2014 | Critical care (London, England) | 25189403 |
| Etherington | 2010 | Journal of burn care & research | 20061835 |
| Merz | 2019 | Intensive care medicine | 31273416 |
| Lau | 2012 | International Journal of Perioperative Ultrasound and Applied Technologies | NA |
| Saranteas | 2010 | Anesthesia and intensive care | 20514974 |
| Jelic | 2017 | The Journal of emergency medicine | 29128035 |
| Ecker | 2013 | The New England journal of medicine | 23534575 |
| Fagnoul | 2013 | Revista Brasileira de terapia intensiva | 24553517 |
| Griffin | 2017 | The American surgeon | 28822391 |
| Cooper | 2000 | Critical care and resuscitation | 16597297 |
| Vignon | 1995 | Circulation | 7586266 |
| Orme | 2009 | British journal of anesthesia | 19151420 |
| Leuverink | 2019 | Netherlands Journal of Critical Care | NA |
| Denault | 2002 | Canadian journal of anesthesia | 11861348 |
| Rublee | 2020 | Chest | 32386652 |
| Poppe | 2021 | BMJ case reports | NA |
| Hlaing | 2018 | Journal of cardiothoracic and vascular anesthesia | 29174659 |
| Mocavero | 2012 | HSR proceedings in intensive care & cardiovascular anesthesia | 23440548 |
| Fair | 2016 | The American journal of emergency medicine | 27318746 |
| Goeddel | 2019 | Anesthesia and Analgesia | 31425202 |
| Krishnan | 2014 | Journal of Cardiothoracic and Vascular Anesthesia | 24011910 |
| McLean | 1998 | Anesthesia and intensive care | 9513664 |
| Kim | 2021 | The American journal of emergency medicine | 31982225 |
| Horowitz | 2021 | CASE | 33495743 |
Appendix 6. Additional MEDLINE search for studies assessing ccTEE in ARDS and respiratory failure

|
|
|
|
|
|
| 1 | Echocardiography, Transesophageal/ (22272) |
| 2 | (transesophageal or transoesophageal).tw. (22005) |
| 3 | ((transesophag* or transoesoph* or esophag* or oesophag*) adj2 echo*).tw. (20010) |
| 4 | 1 or 2 or 3 (32988) |
| 5 | intensive care unit/ or medical intensive care unit/ (65054) |
| 6 | exp *intensive care/ (37708) |
| 7 | Critical Care/ (57779) |
| 8 | Critical Illness/ (35321) |
| 9 | (critical* adj2 (ill* or care)).tw. (88488) |
| 10 | intensive care.tw. (168971) |
| 11 | emergency ward/ (81230) |
| 12 | (emergency adj2 (room* or department*)).tw. (132119) |
| 13 | (icu or recovery room* or Respiratory Care Unit* or Coronary Care Unit* or burn unit*).tw. (80473) |
| 14 | emergency health service/ or emergency medical dispatch/ or hospital emergency service/ (123967) |
| 15 | prehospital.tw. (13786) |
| 16 | Respiratory Distress Syndrome/ (22686) |
| 17 | ards.tw. (15888) |
| 18 | acute respiratory distress syndrome.tw. (18683) |
| 19 | respiratory failure.tw. (36312) |
| 20 | exp Pneumonia/ (246064) |
| 21 | exp Respiratory Insufficiency/ (66380) |
| 22 | exp Pulmonary Edema/ (17656) |
| 23 | Thoracic Injuries/ or Rib Fractures/ (15795) |
| 24 | Pneumothorax/ (17796) |
| 25 | exp Pulmonary Atelectasis/ (6900) |
| 26 | Lung Diseases, Obstructive/ or Pulmonary Disease, Chronic Obstructive/ (64393) |
| 27 | 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 (480601) |
| 28 | 4 and 27 (1606) |
| 29 | 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 (462280) |
| 30 |
|
| Study | Study Type and Design | Clinician, Location, and Training | Primary Outcome(s) | Patients (n) | Main Finding(s) | Compli-cations |
|---|---|---|---|---|---|---|
| Boissier et al 2015 | Prospective Observational | Intensivist, ICU, Board Certified | Association between presence of TPBT and outcomes | 216 | A moderate to large TPBT was found in 26% of patients with ARDS and was associated with a hyperdynamic state but did not influence oxygenation. It was associated with higher mortality and less ventilator free days. | None |
| Dessap et al 2015 | Prospective Observational | NR, ICU, “Trained Operators” | Mortality | 752 | The prevalence of acute cor pulmonale (ACP) during moderate to severe ARDS is 21.8%. Patients with severe ACP had higher mortality (57% vs. 42%, P = .03). | None |
| Legras et al 2015 | Prospective Observational | NR, ICU, NR | Prevalence of ACP | 195 | For patients with moderate to severe ARDS, the prevalence of ACP was 24.6% in this study. The prevalence of PFO was 14.9%. | None |
| Lheritier et al 2013 | Prospective Observational | Intensivist, ICU, “Experience with CCE” | Prevalence of ACP and PFO | 201 | For patients with ARDS, prevalence of ACP was 22.5%. The prevalence of PFO was 15.5%, with only 12.9% of those with PFO having moderate and consistent shunting. The remainder had small or intermittent shunting. There were no large shunts | None |
| Dessap et al 2011 | Prospective Observational | NR, ICU, NR | Feasibility of Prone TEE | 34 | TEE was feasible to insert in the prone position in all patients. Its insertion resulted in a change in management in 70% of cases | None |
| Dessap et al 2010 | Prospective Observational | NR, ICU, NR | Prevalence of shunting PFO | 203 | For patients with ARDS, moderate to large PFO shunting was detected in 19.2% of patients. | None |
| Tsubo et al 2004 | Prospective Observational | NR, ICU, NR | Change in lung density on TEE post proning | 10 | Assessing left lower lung densities in patients who were proned for ARDS. The density area decreased and PaO2/ FIO2 improved after prone position in ten patients (P < .01) | None |
| Vieillard-Baron et al 2001 | Prospective Observational | NR, ICU, NR | Prevalence of ACP | 75 | For patients with ARDS, 25.3% of patients developed ACP. ACP was associated with longer mechanical ventilation and the need for prone positioning. | None |
Abbreviations: TPBT, Transpulmonary bubble transit; ARDS, Acute respiratory distress syndrome; ACP, Acute cor pulmonale.