
Abstract
Background:
Temporary extracorporeal life support (ECLS) by venoarterial extracorporeal membrane oxygenation is an emerging therapy for patients with severe, ongoing cardiogenic shock. After stabilization of the hemodynamic status and end-organ function, sedation weaning, extubation, and noninvasive ventilation (NIV) can be attempted. The goal of this study was to analyze the feasibility of extubation and NIV during versus after ECLS for cardiogenic shock.
Methods:
Single-center retrospective observational study of 132 patients undergoing ECLS due to severe cardiogenic shock between January 2015 and December 2016 at a tertiary care university hospital.
Results:
Patients received ECLS due to acute myocardial infarction (20.6%), ongoing cardiogenic shock (15.2%), postoperative low-cardiac-output syndrome (24.2%), and extracorporeal cardiopulmonary resuscitation (40.2%). Overall, intensive care unit survival was 44.7%. Sixty-nine (52.3%) patients could never be extubated. Forty-three (32.6%) were extubated while on ECLS support (group 1) and 20 (15.1%) were extubated after weaning from ECLS (group 2). Patients extubated during ECLS had a significantly shorter total time on ventilator (P = .003, mean difference: −284 hours [95% confidence limits: −83 to −484]) and more invasive ventilation free days (P = .0018; mean difference 8 days [95%CL: 2-14]). Mortality and NIV failure rates were similar between groups.
Conclusions:
Extubation and NIV are feasible in patients who stabilize during ECLS therapy. Further studies need to address whether extubation has the potential to improve patients outcome or if the feasibility to extubate is a surrogate for disease severeness.
Keywords
Introduction
Extracorporeal life support (ECLS) by venoarterial extracorporeal membrane oxygenation (va-ECMO) is a rescue therapy for patients with severe ongoing cardiogenic shock or postoperative low-cardiac-output syndrome (LCOS) or as an adjunct to cardiopulmonary resuscitation. 1 –3 Recent studies underscore the benefit of this therapeutic approach in a variety of settings, including encouraging data on patient mortality. 4,5 Furthermore, there are several unknown factors most likely contributing to ECLS success, such as fluid management, renal replacement therapy, and the optimal ventilatory regime. To date, cannulation for va-ECMO is mostly performed in patients with rapidly deteriorating hemodynamics who were already endotracheally intubated and mechanically ventilated due to severe shortness of breath. However, as the patient’s hemodynamics stabilize and organ function recovers, it is still debated whether the patient should be extubated while on ECLS or after ECLS has been terminated successfully and the cannulas have been removed. While noninvasive ventilation (NIV) is known to be a strategy to improve patients’ outcomes in different clinical settings, this therapy might also be beneficial for patients supported by va-ECMO. 6,7 Therefore, the objective of this retrospective observational cohort study was to study the feasibility of extubation and NIV in patients during and after ECLS and to assess the possible impact of this maneuver on patient’s outcome.
Methods
Study Design and Data Collection
Prior to the start of this study, ethical approval was given by the Institutional Review Board at the University Hospital Tübingen (IRB #182/2017BO2). All patients undergoing extracorporeal membrane oxygenation (ECMO) from January 2015 to December 2016 were retrospectively screened for possible inclusion. Only adult patients (≥18 years of age) needing ECLS by va-ECMO for cardiogenic shock, postoperative LCOS, or extracorporeal cardiopulmonary resuscitation were included in the analyses. Patients supported by venovenous ECMO (vv-ECMO) and patients supported for primary pulmonary reasons were excluded. All data were retrospectively collected from the clinical databases. The decision as to whether extubation was attempted was made by the critical care team based on daily evaluation of the patient’s status addressing the institutional extubation criteria (see “Extubation Criteria as per Institutional Standard” section). Ventilator parameters and time marks of therapy (eg, duration of ventilation, time on ECLS, renal replacement therapy, length of stay [LOS] in the intensive care unit [ICU]) together with clinical parameters were recorded.
Extracorporeal Life Support Cannulation Strategy
Based on our institutional protocol, the venous drainage cannula was implanted percutaneously using the femoral veins. The venous drainage cannula was advanced into the right atrium under transoesophageal echocardiography guidance. 8 Percutaneous femoral artery cannulation was used as a first choice for emergent situations. To minimize the risk of limb ischemia, an antegrade femoral perfusion was established. Only when femoral access could not be established or severe harlequin syndrome developed, the right subclavian artery surgically accessed for arterial ECLS cannulation.
Ventilation Strategy
All patients received invasive pressure-controlled ventilation with an endotracheal tube during the early phase of ECLS. Per institutional protocol, the tidal volume was adjusted to a target of 6 mL/kg ideal body weight. The positive end-expiratory pressure (PEEP) level was kept between 5 and 12 cm H2O based on individual clinical assessment by the intensivists using established guidelines for lung protective ventilation. 9 After extubation, intermittent NIV with PEEP levels between 5 and 10 cm H2O and pressure support was performed using a mask covering the mouth and nose or a full-face mask. Based on clinical judgment, patients could receive high-flow nasal oxygen between phases of NIV.
Extubation Criteria as per Institutional Standard
As per institutional standard, evaluation for possible extubation was attempted after hemodynamic stabilization with low vasopressor support (noradrenaline below 0.2 µg/kg/min), end-organ recovery, and sedation weaning. Patients needed to be fully alert, show protective reflexes, have a body temperature below 38°C, and successfully complete a spontaneous breathing test for 30 minutes. For the spontaneous breathing test, the PEEP level was set to 5 cm H2O, the inspiratory oxygen fraction was set to 40% and the spontaneous breaths were augmented with a pressure support level between 0 and 5 cm H2O. Success in the spontaneous breathing test was documented if the patient did not develop anxiety or a sympathetic stress response, the rapid shallow breathing index (respiratory rate divided by tidal volume in liters) was below 105, the blood gases showed no signs of respiratory acidosis, and the oxygen saturation stayed above 95%.
Criteria for Reintubation
Reintubation was performed due to 2 indications. Planned reintubation was performed for surgeries and procedures under general anaesthesia with subsequent extubation after the surgical procedure. Unplanned reintubation was performed in patients with NIV-failure. The decision to perform the reintubation was made by the clinical team based on the following criteria: stress response with signs of shortness of breath, hypoxemia or hypercapnia not treatable with adjusted ECLS settings, or alterations in consciousness with the risk for aspiration.
Statistical Analysis
The normality of the distribution of continuous variables was assessed using skewness, kurtosis, and the Shapiro-Wilk test. Normally distributed continuous variables are reported as the mean values ± standard deviation. Comparison of normally distributed continuous variables between the different groups was performed using Student t test. Non-normally distributed variables are reported as median and interquartile range (IQR). Comparison of these variables was performed using the Wilcoxon rank sum test. For all comparisons between 2 groups, 95% confidence-limits of the mean are reported. Categorical variables are reported as percentages. Comparisons of categorical variables were performed using the χ2 test or Fisher exact test. Differences in the variables were interpreted as significant at P values < .05. For the identification of factors associated with a dichotomized outcome variable, univariate logistic regression analysis was performed.
Results
Patient Selection
During the study period, a total of 192 patients were given extracorporeal support. Forty-eight patients were excluded because they received venovenous support due to acute respiratory distress syndrome (ARDS). Another 9 patients were excluded because they received va-ECMO due to ARDS with right heart insufficiency, pulmonary embolism, pneumonia, transfusion-associated lung injury, or trauma. We aimed to only include patients needing genuine support for heart failure in this study group. Two patients were excluded who had never received invasive ventilation. Finally, 132 patients, 35 female (26.5%) and 97 male (73.5%), were included in the final analysis (see patient selection chart, Figure 1).
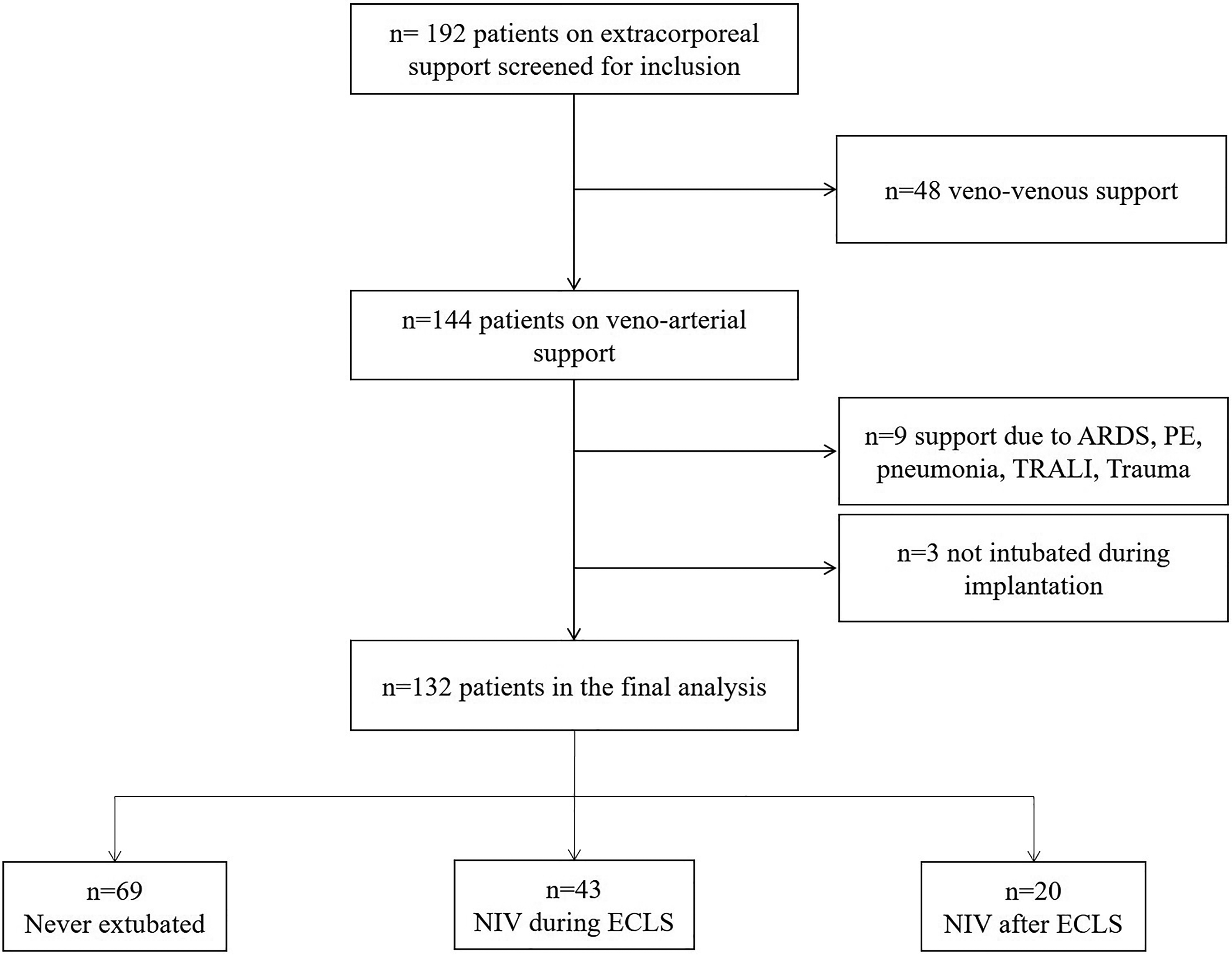
Patient selection chart. ARDS indicates acute respiratory distress syndrome; ECLS, extracorporeal life support for cardiogenic shock; NIV, noninvasive ventilation; PE, pulmonary embolism; TRALI, transfusion associated lung injury.
Patient Characteristics and Overall Outcome Data
The overall patient characteristics are given in Table 1. The mean time on ECLS was 10 days (standard deviation: ±7.5 days). A total of 57.6% of patients could be successfully weaned off the ECLS. Intensive care unit mortality was 55.3% (73/132), of whom 26% (19/73) died within 24 hours after ICU admission. Intensive care unit mortality was 51.6% in male patients and 65.7% in female patients; 13.4% (13/97) of male patients and 17.1% (6/35) female patients died within 24 hours.
Patient Characteristics.
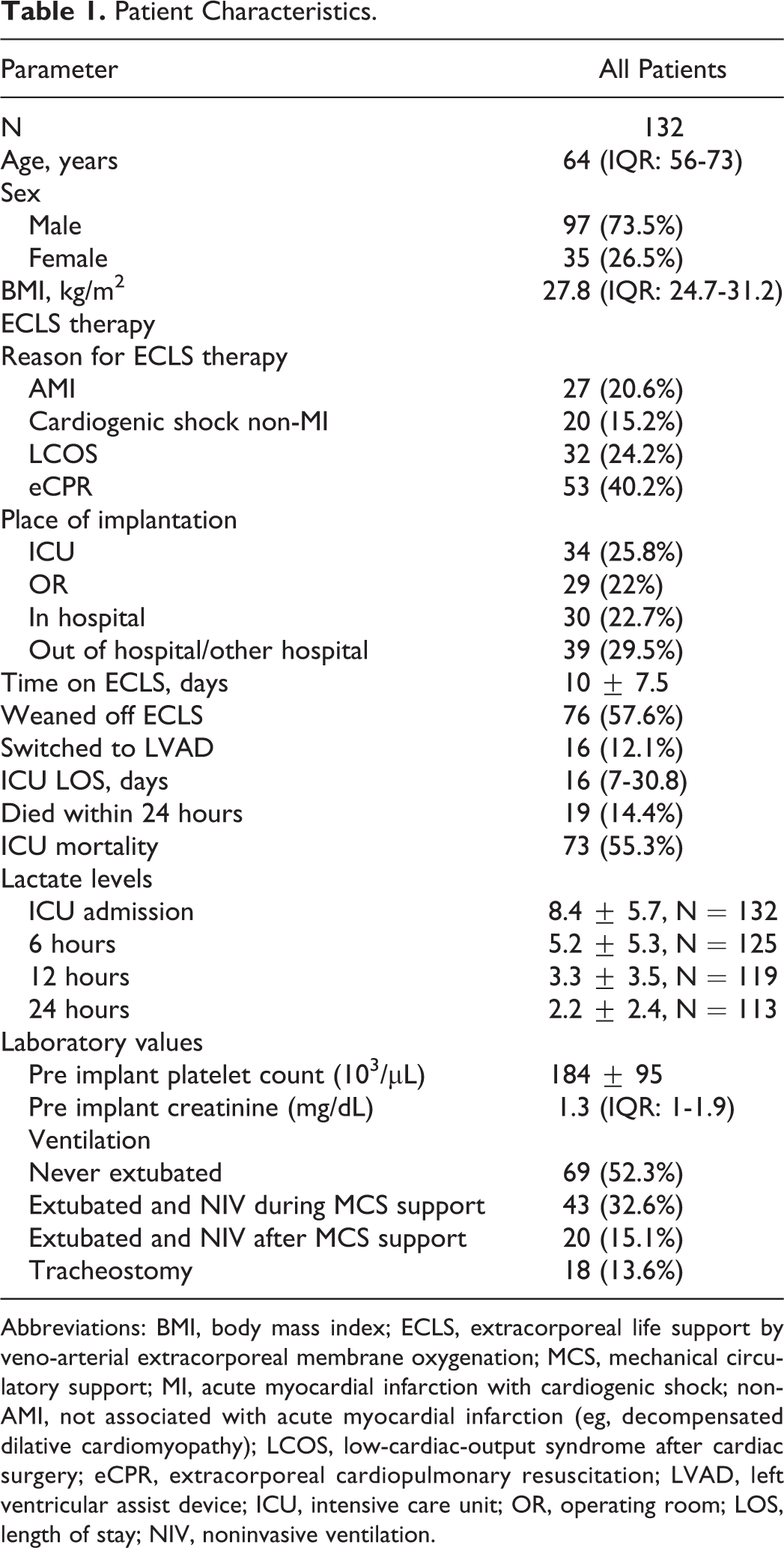
Abbreviations: BMI, body mass index; ECLS, extracorporeal life support by veno-arterial extracorporeal membrane oxygenation; MCS, mechanical circulatory support; MI, acute myocardial infarction with cardiogenic shock; non-AMI, not associated with acute myocardial infarction (eg, decompensated dilative cardiomyopathy); LCOS, low-cardiac-output syndrome after cardiac surgery; eCPR, extracorporeal cardiopulmonary resuscitation; LVAD, left ventricular assist device; ICU, intensive care unit; OR, operating room; LOS, length of stay; NIV, noninvasive ventilation.
Extubation and NIV Therapy
Of the finally included patients, 69 were never extubated (Supplement 1). Five (7.3%) patients in this group survived ICU therapy and were discharged to a rehabilitation center with a tracheostomy in situ. Forty-three patients could be extubated and received NIV therapy while still on ECLS (Table 2). Out of this subgroup, 33 patients (77%) required reintubation during the following ICU therapy, 18 (42%) of them due to planned surgical procedures and 15 (34.9%) due to NIV failure. A third group of 20 patients were extubated and received NIV therapy after weaning from the ECLS. Eleven (55%) patients in this group needed reintubation after first extubation, 2 (10%) of them due to planned surgical procedures, and 9 (45%) due to NIV failure.
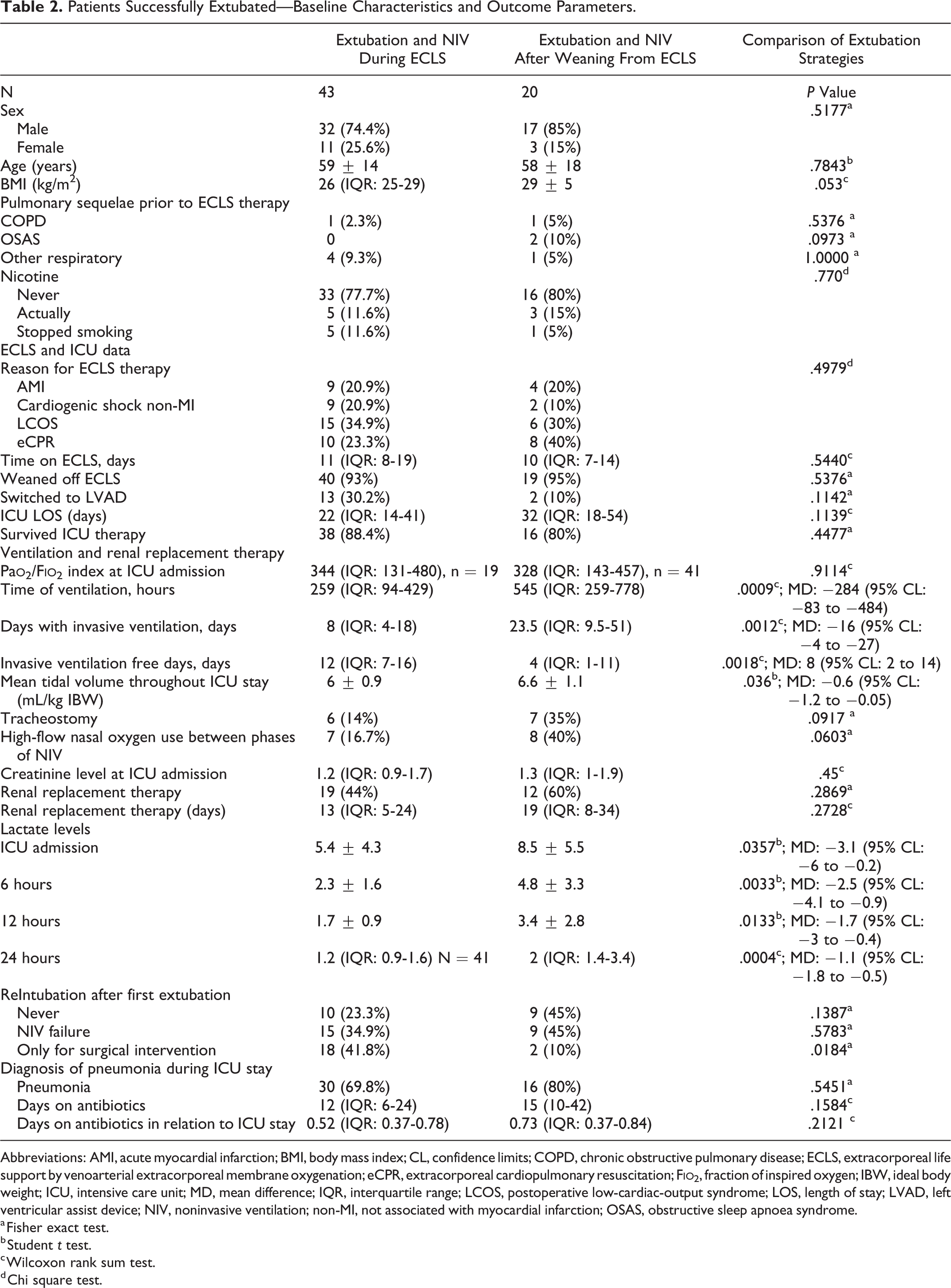
Patients Successfully Extubated—Baseline Characteristics and Outcome Parameters.
Abbreviations: AMI, acute myocardial infarction; BMI, body mass index; CL, confidence limits; COPD, chronic obstructive pulmonary disease; ECLS, extracorporeal life support by venoarterial extracorporeal membrane oxygenation; eCPR, extracorporeal cardiopulmonary resuscitation; F
a Fisher exact test.
b Student t test.
c Wilcoxon rank sum test.
d Chi square test.
Comparison of the Patients Extubated and Receiving NIV Therapy During and After ECLS Support
There were no differences regarding age, sex, reason for the ECLS, place of va-ECMO implantation, time on ECLS, ECLS therapy survival, requirement for renal replacement therapy, or ICU LOS between the 2 groups. Patients extubated during the ECLS had a significantly shorter total time on ventilator (including invasive and NIV): 259 hours (IQR: 94-429 hours) versus 545 hours (IQR: 259-778 hours; Table 2, Figure 2). A significantly shorter time of invasive ventilation was also observed: 8 days (IQR: 4-18 days) versus 23.5 days (IQR: 9.5-51 days; Figure 2). Invasive ventilation free days were significantly longer in the group of patients extubated during ECLS support (12 days [IQR: 7-16 days] vs 4 days [IQR: 1-11 days]). The NIV failure rate and the rate of tracheostomy were similar in both groups. There were no differences regarding the rate of pneumonia diagnosis or pneumonia-associated antibiotic use. Chest radiographs within 24 hours after extubation showed a significantly higher rate of pulmonary venous congestion in the patients extubated after the termination of the ECLS (supplement 2).
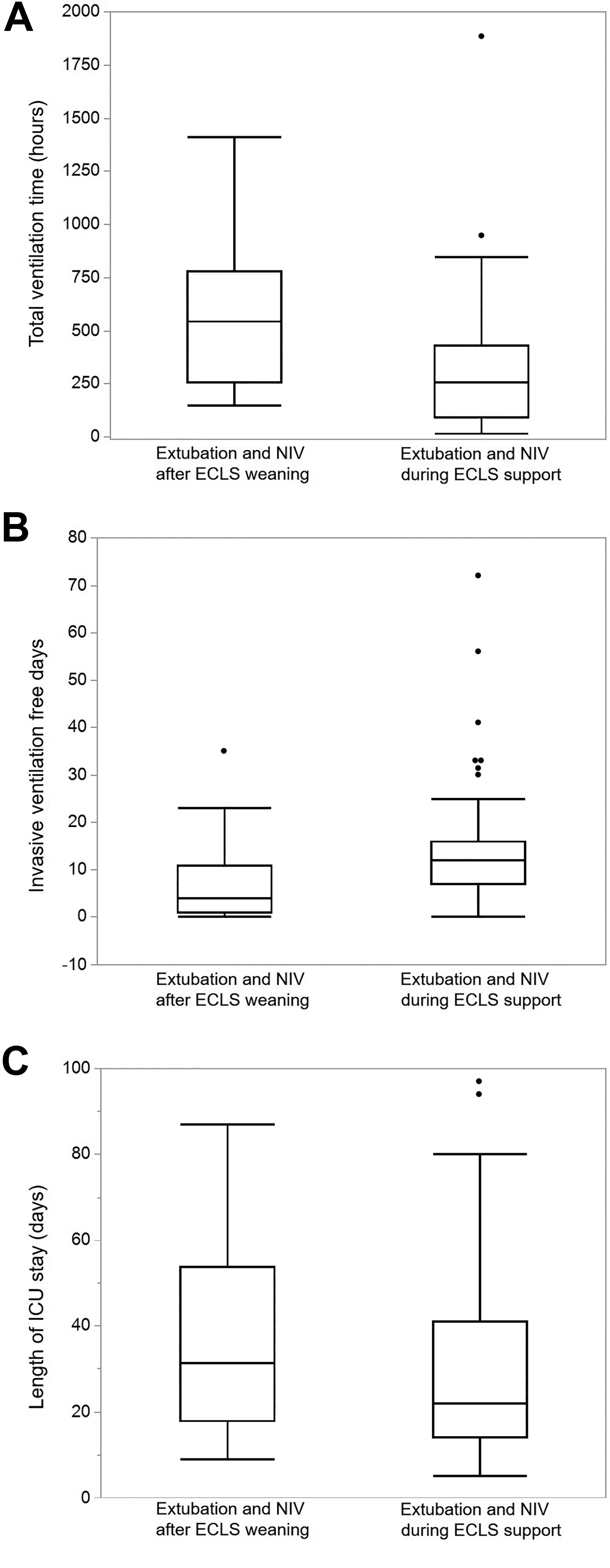
A, Box-plot diagrams comparing total time on ventilator (hours). Significant difference between the group of patients extubated after and during ECLS could be observed (545 hours [IQR: 259-778 hours] vs 259 hours [IQR: 94-429 hours]; P = .0009). B, Box plot diagrams comparing invasive ventilation free days (days). Significant difference between the group of patients extubated after and during ECLS could be observed (4 days [IQR: 1-11 days] vs 12 days [IQR: 7-16 days]; P = .0018). C, Box plot diagrams comparing ICU LOS. No significant difference was observed for ICU LOS between the extubation groups. ECLS indicates extracorporeal life support; ICU, intensive care unit; LOS, length of stay; NIV, noninvasive ventilation.
Characteristics of Patients With NIV Failure After First Extubation
Twenty-four patients needed to be reintubated due to severe respiratory distress despite ongoing NIV therapy (NIV failure group). Reintubation needed to be performed within a median of 2.5 days (IQR: 0.5-4.8 days). Seven patients received a tracheostomy after the first reintubation. A second extubation attempt was performed in 14 patients of whom 10 again needed to be reintubated within a median of 1.5 days (IQR: 0-3.3 days) suffering from respiratory failure. Two of these 10 patients were extubated successfully at the third attempt, 5 received a tracheostomy and the remaining 3 died with their endotracheal tube in-situ. On the other hand, 19 patients needed no reintubation after extubation at any time-point (nonreintubation group). There were no differences between the NIV failure group and the nonreintubation group regarding the age, gender, body mass index, and reason for ECLS therapy. Intensive care unit LOS was significantly longer in the NIV failure group (median 43 days [IQR: 23-55 days] vs median 14 days [IQR: 9-20 days]; P < .0001) as was the total ventilatory time (median 489 hours [IQR: 348-901 hours] vs median 169 hours [IQR: 46-246 hours]; P = .0002). There was a trend toward a higher rate of ICU mortality in the group with NIV failure (8/24 [33.3%] vs 1/19 [5.3%]; P = .0551).
Factors Associated With Extubation and NIV Therapy During ECLS
The univariable logistic regression analysis identified lactate levels at different time points as factors associated with successful extubation during ECLS (Table 3). Higher lactate levels at ICU admission, 6 hours, 12 hours, and 24 hours were associated with a lower chance for extubation and NIV during ECLS (odds ratio: 0.879, 0.624, 0.549, and 0.221, respectively). Due to the high correlations between the lactate levels at the different time points, we’ve chosen the lactate level at ICU admission for a multivariable analysis. In this multivariable analysis, combining the lactate level with baseline characteristics and renal function, the lactate level persisted as the only factor associated with successful NIV during ECLS support (Table 3).
Factors Associated With Extubation and NIV Therapy During ECLS Support.
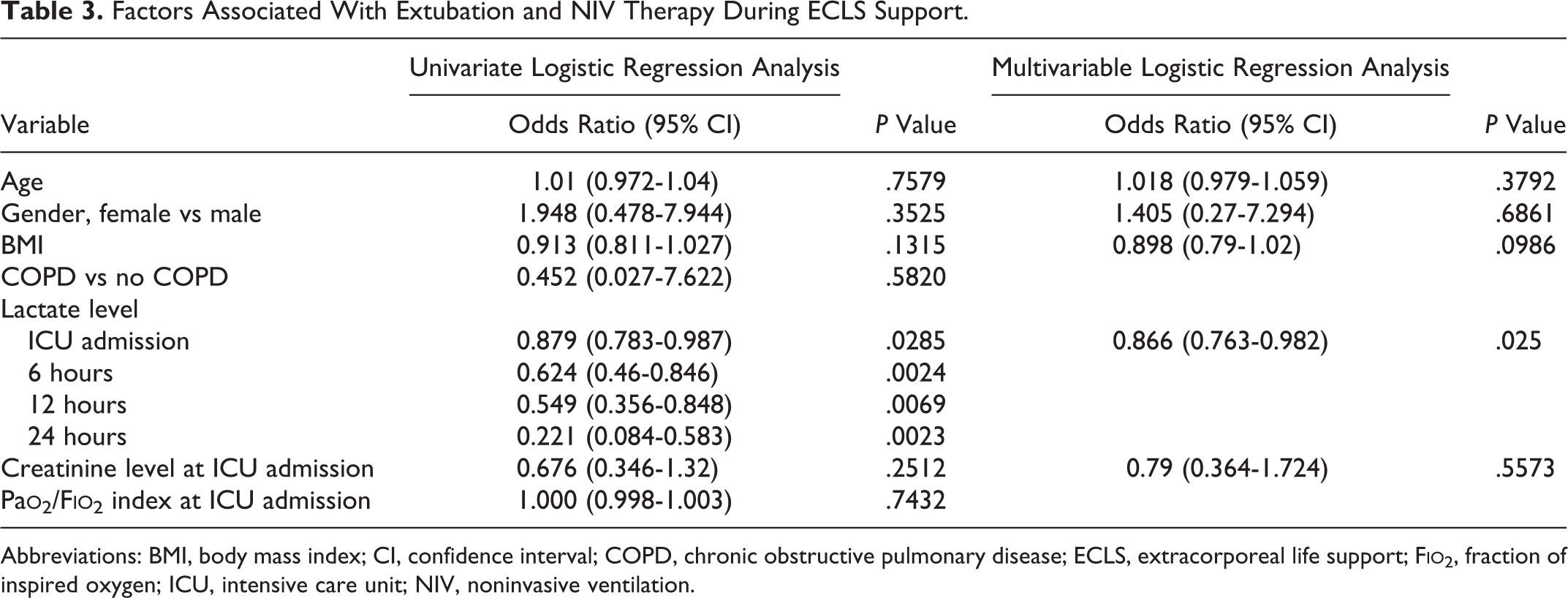
Abbreviations: BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ECLS, extracorporeal life support; F
Impact of Extubation and NIV Therapy on Patients’ Outcome
To assess the impact of extubation and NIV therapy on 2 outcome variables (ICU mortality and NIV failure), logistic regression analyses were performed using the parameter “extubation and NIV therapy during ECLS” as the focal predictor and other variables that could explain potential effects as covariates. However, extubation and NIV therapy during ECLS therapy was not associated with ICU mortality and NIV failure in this approach controlling for potential confounders (Table 4).
Influence of Extubation During ECLS Therapy on Outcome Variables.
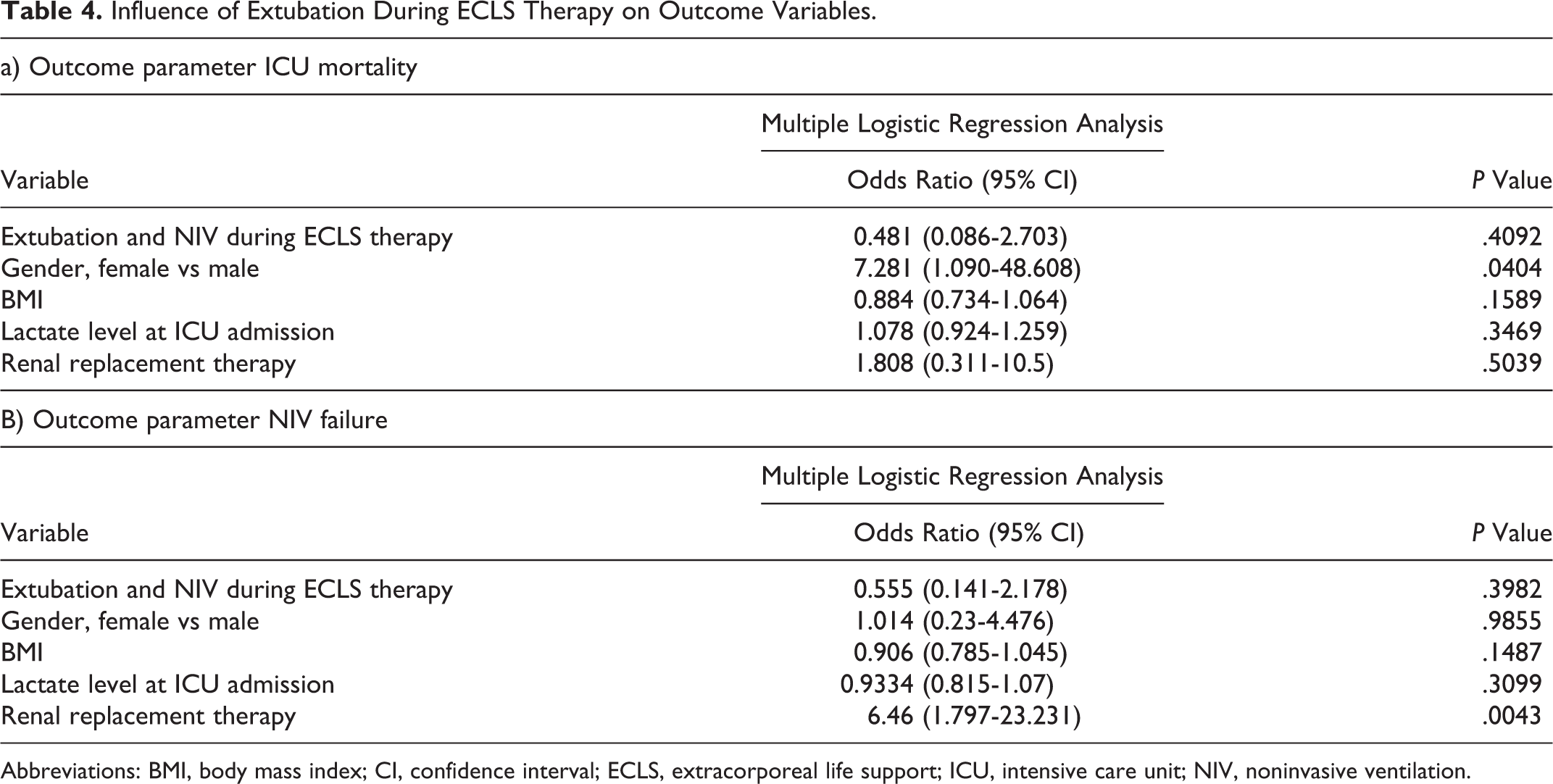
Abbreviations: BMI, body mass index; CI, confidence interval; ECLS, extracorporeal life support; ICU, intensive care unit; NIV, noninvasive ventilation.
Discussion
This present study shows that extubation and NIV was feasible in about one-third of ECLS patients. Patients extubated during ECLS had a significantly lower total time with ventilatory support and more invasive ventilation free days. Furthermore, patients who could be extubated and received NIV during ECLS had lower early lactate levels at ICU admission.
Extracorporeal life support is used in awake patients with ARDS to avoid invasive mechanical ventilation. 10,11 Awake venovenous ECMO is also used to bridge patients until they receive a lung transplantation. 10,12 –16 Reports are sparse on the use of ECMO in awake patients whose hemodynamics are not compensated with this technique but who require a venoarterial ECMO strategy for ECLS. 17 –20 One of the first studies was published in 2015 by Mohite et al that reported on 9 patients successfully extubated during ECLS. 20 A second retrospective observational study compared 41 extubated patients with 137 patients who had never been extubated. 21 Bataillard et al demonstrated that extubated patients had a lower incidence of ventilator-associated pneumonia. 21 This study also concluded that extubating patients on ECLS might be beneficial to patient prognosis. Recently, Ellouze et al published their single-center experience in extubating patients supported on ECLS. 19 They compared 15 patients extubated while supported by ECLS with 42 patients not extubated during ECLS. 19 Patients extubated showed better survival after 30 days. The previously published data have focused on a comparison of extubation during ECLS versus nonextubation during ECLS, and all studies demonstrate a higher mortality rate in the nonextubation group. However, there is no conclusion on whether there is a difference between extubation during ECLS versus extubation after weaning from ECLS, because patients who cannot be extubated mostly showed worse outcomes in previously published reports. 19 –21
Hence, the present study is the first to analyze a potential difference in outcomes of patients extubated while supported by ECLS compared to patients receiving extubation after successful ECLS weaning. Most of the patients on ECLS receive invasive mechanical ventilation in the early phase of extracorporeal support. After hemodynamic stabilization and end-organ recovery, sedation weaning and extubation can be attempted. However, the optimal point of time for weaning from invasive ventilation is unclear. As NIV has been shown to be a valuable tool for continued weaning from ventilatory support with the potential to reduce the risk of ventilator-induced pneumonia and other infectious complications, this therapy might be of benefit for patients with ECLS. 22,23 In ECLS-supported patients, an optimal unloading of the left ventricle will lead to a reduction in pulmonary venous congestion and avoid pulmonary edema. Lung function and gas exchange will recover, and consequently, extubation can be attempted. However, the optimal monitoring of adequate and recovered pulmonary function during ECLS still needs to be investigated.
Our data clearly demonstrate that the total time on ventilator was significantly lower in the group of patients extubated during ECLS therapy (259 hours [IQR: 94-429] versus 545 2hours [IQR: 259-778]; P = .0009), despite a similar total duration of ECLS therapy. This is in line with previously published reports that all showed significantly shorter durations of mechanical ventilation. 19 –21 Due to additional surgical procedures (eg, left ventricular assist device [LVAD] implantation or vascular surgery) reintubation needed to be performed in approximately 42% of patients who were extubated during ECLS support. None of our patients experienced a complication during airway management, but various complications of endotracheal intubation have been reported in the literature. 24,25 Interestingly, the NIV failure rate was similar in both of our groups although there was a higher rate of signs of pulmonary venous congestion in the group extubated after weaning from the ECLS. This might be due to a compromised left ventricular function with elevated filling pressures and might be the reason why significantly more patients with extubation after ECLS weaning received tracheostomy after being reintubated to facilitate weaning from ventilatory support. 26 Thus, the time point of possible extubation could also be associated with the severity of the underlying disease. Compared to other studies in the ICU setting, we can report a similar NIV failure rate in our patients, even if they were still supported by ECLS. 27 Patients needing reintubation due to NIV failure had a more complicated ICU stay in our patient collective. A second extubation attempt led to a high rate (71%) of recurring NIV failure. Therefore, it should be discussed at the bed-side whether a second extubation is attempted or immediate tracheostomy after reintubation is performed. Previously published findings showed a significant reduction in the rates of ventilator-associated pneumonia with patients being extubated during ECLS. 19,21 Our data show no difference regarding the diagnosis of pneumonia between NIV groups. The design of the present study, focusing on extubated patients only as well as differences in the studied patient collectives might be a possible reason for this conflicting result.
Our results indicate that the ICU LOS and ICU mortality are similar in the patients extubated during ECLS compared to after ECLS. At first glance, this finding is contrary to previously published data. 19,20 All patients in whom extubation had never been attempted (52%) were excluded from our analyses leaving only the patients extubated and receiving NIV in the final analysis. Only 7% of our patients in whom extubation was not feasible survived the ICU stay and were discharged with a tracheostoma. Despite the fact that NIV is able to reduce the total time on ventilator, our data leave unanswered whether NIV improves overall survival, as the severity of the underlying disease and end-organ dysfunction is of crucial importance for recovery. In our patient sample, the overall ICU mortality was approximately 55%, which is comparable to recently published data for patients receiving ECLS. 4,5,28 Even higher mortality rates have been shown for elderly patients above 60 years of age. 29 As in other published reports, more male than female patients are supported by ECLS what might be attributable to the gender differences in prevalence of cardiovascular diseases. 4,5,30 But we could not observe differences in mortality. The prognostic value of the initial lactate level for ICU and 30-day survival has been previously demonstrated however pathophysiology of elevated lactate levels is not completely understodd. 5,31 –33 Increased lactate levels are generally seen to be a surrogate of anaerobic glycolysis secondary to tissue hypoperfusion and/or hypoxia. 34 On the other hand, elevated lactate levels can result from increased glycolysis with or without reduced lactate clearance in situations with increased adrenergic stimulation. 35,36 In the case of cardiogenic shock, hyperlactatemia is therefore most likely a surrogate for a severe adrenergic stress response together with tissue hypoperfusion. Optimal ECLS therapy improves tissue perfusion and therefore endogenous adrenergic stimulation will be attenuated. Initial therapeutic positive inotropic adrenergic simulation by catecholamines can also be withdrawn. In our patient, collective early lower lactate levels were associated with the success of extubation during ECLS. As shown previously in terms of ICU mortality, hyperlactatemia might again reflect initial disease severity and differences in lactate clearance within the first 24 hours of ICU therapy might identify patients with improved outcomes. Further trials need to assess lactate levels in this situation.
Early sedation weaning and extubation do not influence respiratory function only. Previous reports have also shown that more intensive physiotherapy is facilitated. 37,38 Awake patients are also able to fully communicate with the ICU team and their relatives. The patient can actively take part in life-changing decisions such as the implantation of a permanent LVAD. This can tremendously improve patient self-determination and well-being.
Study Limitations
This retrospective cohort study only describes our single-center experience. As patients were not randomly assigned to a certain treatment group, we can only report on the feasibility of this technique and encourage further research in this field. Second, we report on a real-life sample of patients suffering from various causes of cardiogenic shock leading to ECLS. Trials assessing only one subgroup of patients (eg, cardiogenic shock due to myocardial infarction) might provide better insights into the value of early extubation and NIV during ECLS. Finally, as some patients were transferred to other hospitals after ECLS therapy, data on 30-day mortality are not available.
Conclusions
Patients requiring ECLS for acute cardiogenic shock still have a high mortality rate. Some of the patients die within the first 24 hours of extracorporeal support. Patients with stabilized hemodynamics and organ function are eligible for weaning from invasive mechanical ventilation while still supported by ECLS. Extubation during ECLS results in a significant reduction in ventilator time. This might improve patients’ comfort because they can actively communicate with the ICU team. Further prospective trials are needed to identify the optimal time point of extubation and to assess whether this maneuvre improves patients’ long-term outcomes.
Supplemental Material
Supplemental Material, sj-pdf-1-jic-10.1177_0885066620918171 - Extubation and Noninvasive Ventilation of Patients Supported by Extracorporeal Life Support for Cardiogenic Shock: A Single-Center Retrospective Observational Cohort Study
Supplemental Material, sj-pdf-1-jic-10.1177_0885066620918171 for Extubation and Noninvasive Ventilation of Patients Supported by Extracorporeal Life Support for Cardiogenic Shock: A Single-Center Retrospective Observational Cohort Study by Harry Magunia, Aida M. Guerrero, Marius Keller, Johann Jacoby, Christian Schlensak, Helene Haeberle, Michael Koeppen, Martina Nowak-Machen and Peter Rosenberger in Journal of Intensive Care Medicine
Supplemental Material
Supplemental Material, sj-pdf-2-jic-10.1177_0885066620918171 - Extubation and Noninvasive Ventilation of Patients Supported by Extracorporeal Life Support for Cardiogenic Shock: A Single-Center Retrospective Observational Cohort Study
Supplemental Material, sj-pdf-2-jic-10.1177_0885066620918171 for Extubation and Noninvasive Ventilation of Patients Supported by Extracorporeal Life Support for Cardiogenic Shock: A Single-Center Retrospective Observational Cohort Study by Harry Magunia, Aida M. Guerrero, Marius Keller, Johann Jacoby, Christian Schlensak, Helene Haeberle, Michael Koeppen, Martina Nowak-Machen and Peter Rosenberger in Journal of Intensive Care Medicine
Footnotes
Authors’ Note
Martina Nowak-Machen and Peter Rosenberger contributed equally and share authorship. Harry Magunia contributed substantially to all aspects of this manuscript, including study design, data collection, data analysis, data interpretation, and draft of the first manuscript; Martina Nowak-Machen and Peter Rosenberger contributed substantially to this manuscript, including study design, data analysis, data interpretation, and draft of the first manuscript; Aida M. Guerrero contributed substantially to data collection and data analysis; Johann Jacoby contributed substantially to statistics and data interpretation; Michael Koeppen, Christian Schlensak, Helene Haeberle, and Michael Koeppen contributed substantially to data interpretation and revision of the manuscript. All authors approved the final manuscript. Prior to the start of this study, ethical approval was given by the Institutional Review Board at the University Hospital Tübingen (IRB #182/2017BO2).
Acknowledgments
The authors thank all employees of the intensive care unit at the University Hospital Tübingen for their efforts in daily patient care.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Christian Schlensak serves as a consultant for Thoratec Corporation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by departmental funds.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.