
Abstract
Background:
Physical rehabilitation can benefit critically ill patients during intensive care unit (ICU) admission, but routine clinical practice remains inconsistent nor examined in prolonged mechanical ventilation patients transferred to a specialist ventilator weaning unit (VWU). Behavioral mapping is a sampling approach that allows detailed reporting of physical activity profiles. The objective of this study was to characterize the physical activity profile of critically ill patients in a UK ICU and VWU.
Methods:
Single-center, prospective observational study in a university teaching hospital. Patient observations, conducted Monday through Sunday from 08:30
Results:
Forty-two ICU and 11 VWU patients were recruited, with 2646 and 693 observations, respectively, recorded. In the ICU, patients spent a median (interquartile range) of 100% (96%-100%) of the day (10.5 [10.0-10.5] hours) located in bed, with minimal/no activity for 99% (96%-100%) of the day (10.4 [9.7-10.5] hours). Nursing staff were most frequently observed in attendance with patients irrespective of ventilation or sedation status, although patients still spent approximately two-thirds of the day alone. Bed-to-chair transfer was the highest activity level observed. In the VWU, patients spent 94% (73%-100%) of the day (9.9 [7.7-10.5] hours) in bed and 56% (43%-60%) of time alone. Physical activity levels were higher and included ambulation. All physical activities occurred during physical rehabilitation sessions.
Conclusions:
These profiles of low physical activity behavior across both patients in the ICU and VWU highlight the need for targeted strategies to improve levels beyond therapeutic rehabilitation and support for a culture shift toward providing patients with, and engaging them in, a multidisciplinary, multiprofessional environment that optimizes overall physical activity.
Background
Rehabilitation is the cornerstone of management of post critical illness morbidity 1 and a mandated component of clinical practice across the recovery continuum. 2,3 During intensive care unit (ICU) admission, physical rehabilitation is typically characterized by early mobilization and delivery of interventions aiming to restore functional ability, with data demonstrating safety, feasibility, and benefit. 4 –11 Indeed, focusing attention on delivering therapy at this early stage of the recovery process has been suggested in light of increasing studies that have shown no difference in effect from rehabilitation interventions delivered post ICU discharge. 12 –14 However, data from point prevalence and observational studies have highlighted the discordant translation of research findings into routine clinical practice, 15 –19 an “evidence–reality gap.” Low levels of activity appear commonplace among these patients, albeit the restrictions on data acquisition via these approaches to specific time or data points means they fail to capture temporal variations in physical activity levels in patients throughout the day which may be more informative. The fact that activity levels may importantly be influenced by clinical factors is also not possible to explore with these study designs.
Behavioral mapping, involving frequent intermittent sampling throughout a defined duration, is an alternative method for prospective reporting of physical activity levels including location, type, and persons present during the activity. This technique has previously been applied in the stroke population 20,21 and more recently in critically ill patients where low levels of physical activity were observed. 16 To date, there have been no similar UK behavioral mapping data describing physical activity in the ICU population. Furthermore, there are no data profiling post-ICU patients transferred to a ventilator weaning unit (VWU) with prolonged mechanical ventilation requirements. These patients may demonstrate greater levels of activity secondary to a more stable clinical status and where the emphasis of management on overall weaning and rehabilitation differs from that required in the acute stages of ICU admission. 22 Such data may be informative for optimizing service delivery and rehabilitation strategies.
The aims of this study were therefore to prospectively characterize the physical activity profile of critically ill patients in both a UK ICU and VWU using behavioral mapping.
Methods
Study Design and Setting
This was a single-center, prospective, observational study conducted in a university teaching hospital. The study was confirmed as a service evaluation that did not require ethical approval (UK Health Research Authority, http://www.hra.nhs.uk/research-community/before-you-apply/determine-whether-your-study-is-research/) and was registered with the local institutional clinical audit department (Guy’s and St. Thomas’ NHS Foundation Trust Project Number 5309), with no requirement for participant consent. The study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement for the reporting of observational cohort studies (http://www.strobe-statement.org).
Behavioral mapping was performed in both the ICU and VWU (further descriptions of each location are reported in Online Appendix E1 (“Study locations”). In brief, the adult ICU is a 30-bed unit, split over 2 floors, of mixed medical and surgical admissions, and is also a tertiary referral center for management of severe respiratory failure and delivery of advanced respiratory support including extracorporeal membrane oxygenation (ECMO). There is no written rehabilitation protocol in operation on the ICU. Physiotherapy rehabilitation is determined locally by appropriate sedation scale (Richmond Agitation and Sedation Scale [RASS], −2 to +2) and autonomous clinical reasoning for initiating/continuing physical rehabilitation. The adult VWU is a 14-bed tertiary referral weaning unit for neuromuscular, chronic respiratory, and post-critical illness patients.
Participants
Patients were included if they had been invasively mechanically ventilated for at least 48 hours during their ICU admission with the likelihood to remain on the ICU or VWU for the following 24 hours to allow for observation. Patients were excluded if they were for palliative treatment, had a severe neurological injury influencing rehabilitation management, or if they had previously been observed in the study. Screening for eligibility occurred daily on the ICU and per new patient admission (post-critical illness patients only) on the VWU. At least 3, and at most 6, consecutively eligible patients on any day were required for mapping to proceed following screening of ICU admissions according to numerical order of bed number.
Study Size
A purposive sample size of 41 patients has been deemed representative of activity data in an acutely ill cohort 23 and is in keeping with previously reported behavioral mapping data in critically ill patients. 16 A pro rata convenience sample size of 10 patients (approximately one-quarter that of the ICU cohort) was a priori deemed representative for the VWU secondary to the reduced patient throughput associated with the differing clinical acuity of this cohort.
Behavioral Mapping Procedure
This was conducted in keeping with a previously reported methodology adopted in critically ill patients.
16
Further details are reported in Online Appendix E2 (“Behavioral mapping procedure”). In brief, patients were observed for 1 minute of every 10 minutes throughout the day (8.30
Expanded ICU Mobility Scale and Intensity Classification.
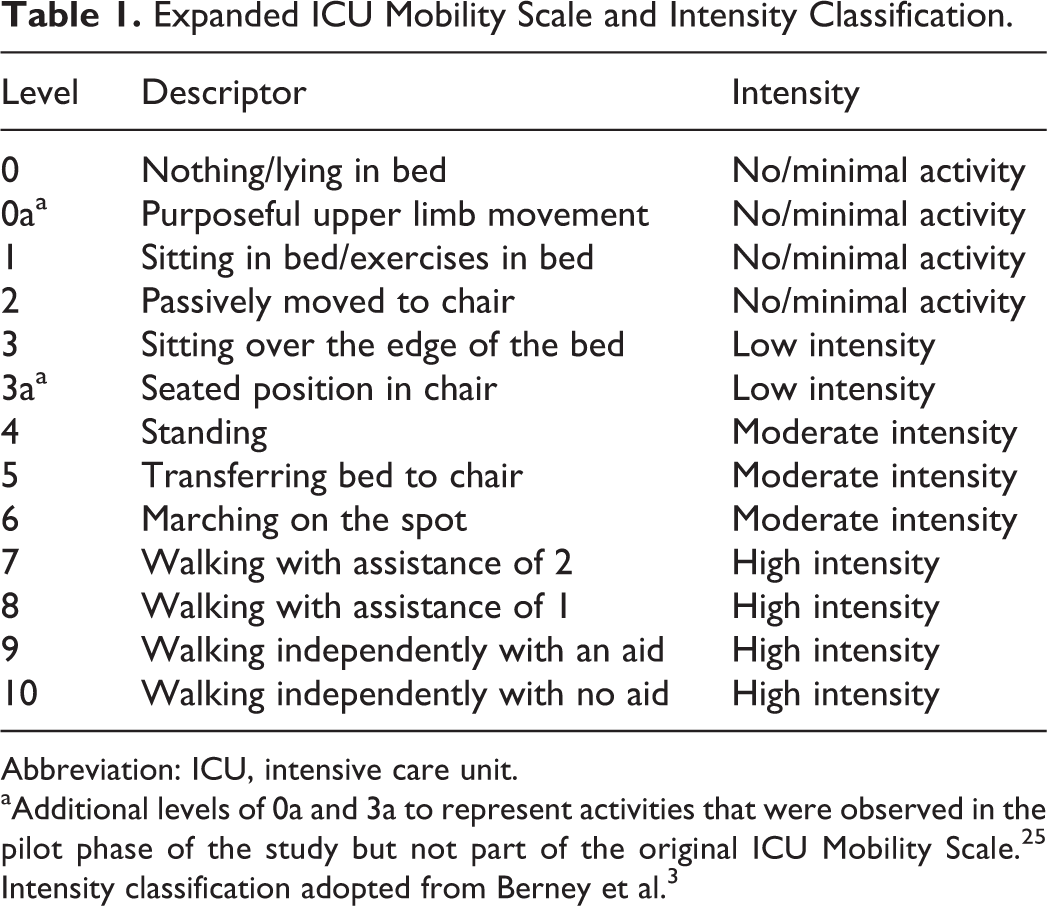
Abbreviation: ICU, intensive care unit.
Clinical Data Collection
Additional demographic and clinical data associated with ICU or VWU admission and during the observation day were collected including age, sex, ventilation status, admission diagnosis, illness acuity, source of referral, premorbid status and prior receipt of physical rehabilitation, sedation status (RASS 26 ), and pharmacotherapy such as sedation, inotropic support, and neuromuscular-blocking agents. Details of physiotherapy contacts received on the day of observation were documented including amount and type of interventions delivered.
Statistical Analysis
Data were tested for normality and appropriate parametric and nonparametric testing applied. Descriptive statistics to analyze binary variables were reported as counts and proportions and continuous variables as mean ± standard deviation (SD) for normally distributed data or median (interquartile range [IQR]) for nonparametric data. Aggregate (summation) percentages were used to analyze individual patient observations for location, people present, and activity level. Median and IQRs were then calculated for the whole group data.
Separate data are presented for subcategories of the whole data set, including ventilation status, sedation score, ICU length of stay, and weekdays and weekends. For VWU patients, due to the small sample size, we did not compare observations across weekday and weekend day or between day (up to 5.00
Time spent in each category was approximated by multiplying the aggregate percentages of individual participants by 630 minutes (11.5-hour observation day with 6- × 10-minute observer breaks subtracted from the total). For comparison of binary variables, contingency analysis was used including χ2 testing and Fisher exact test. Unpaired nonparametric Mann-Whitney U testing was used for comparison of continuous variables. A P value of less than .05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism version 6.0d (GraphPad Software, La Jolla, California; www.graphpad.com).
Results
Physical Activity in the ICU
Two hundred twenty-six patients were screened for eligibility between June and July 2015, of whom 44 were included (Figure 1). Two patients were discharged unexpectedly during the observation day precluding complete data collection. Observations from 42 patients were therefore used for analysis. Baseline characteristics of the cohort are reported in Table 2. Illness severity (Sequential Organ Failure Score) on the day of observation was 10.6 ± 3.9, with 31 (73.8%) patients mechanically ventilated via endotracheal tube. Eleven patients were receiving inotropic support (minimum–maximum dose range: 0.03-7.28 μg/min). Intensive care unit length of stay prior to observation was 7.9 (4.3-12.7) days. One patient was restricted to bed rest on the day of observation due to medical instability. Prior to observation, 15 (35.7%) patients had received physical rehabilitation (range: 0-42 sessions). Time to first exercise therapy session was 7.7 ± 5.2 days from ICU admission. Eight patients had achieved sitting over the edge of the bed, 6 standing, and 1 ambulating away from the bed space.
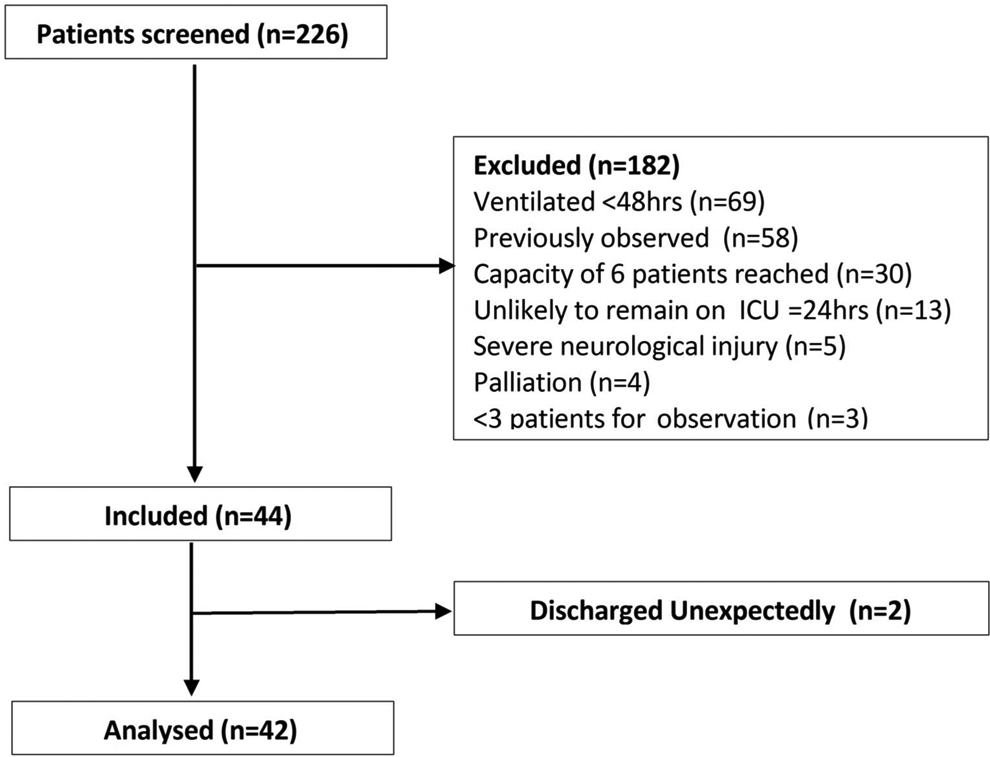
Intensive care unit patient flow through the study.
Characteristics of Intensive Care and Ventilator Weaning Unit Patients.a
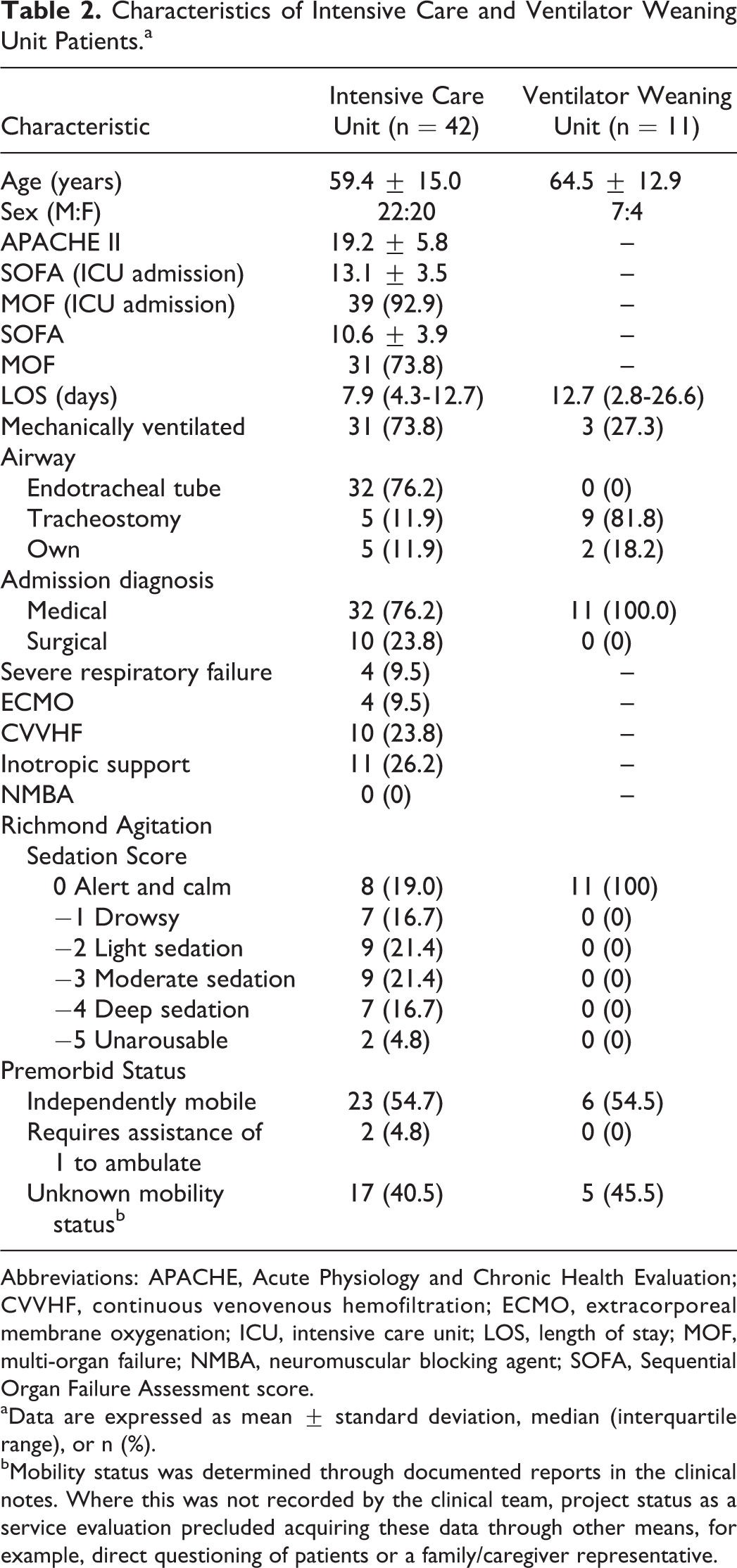
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CVVHF, continuous venovenous hemofiltration; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; LOS, length of stay; MOF, multi-organ failure; NMBA, neuromuscular blocking agent; SOFA, Sequential Organ Failure Assessment score.
aData are expressed as mean ± standard deviation, median (interquartile range), or n (%).
bMobility status was determined through documented reports in the clinical notes. Where this was not recorded by the clinical team, project status as a service evaluation precluded acquiring these data through other means, for example, direct questioning of patients or a family/caregiver representative.
In total, 2646 observations were recorded over 8 observation days (6 weekdays and 2 weekend days): 1953 observations in mechanically ventilated patients (n = 31) and 693 on patients who no longer required mechanical ventilation (n = 11). One hundred eighty-eight data points across 17 patients were not recorded (2.4% of all data; n = 42, curtains closed, n = 146, patient off the ICU). Patients with incomplete data sets showed no characteristic differences (data not presented).
Across all reported observations, patients spent 100% (96%-100%) of the day (>10 [10.0-10.5] hours) located in bed with no or minimal activity for 99% (92%-100%) of the day (approximately 10.4 [9.7-10.5] hours). Table 3 presents findings for observations categorized according to ventilation status (mechanically ventilated or nonmechanically ventilated), sedation status (awake and cooperative RASS −2, −1, 0, +1, +2 [group A] or heavily sedated and combative RASS −5, −4, −3, +3, +4 [group B]), and day of observation (weekday or weekend day).
Behavioral Mapping Data for ICU Patients.a
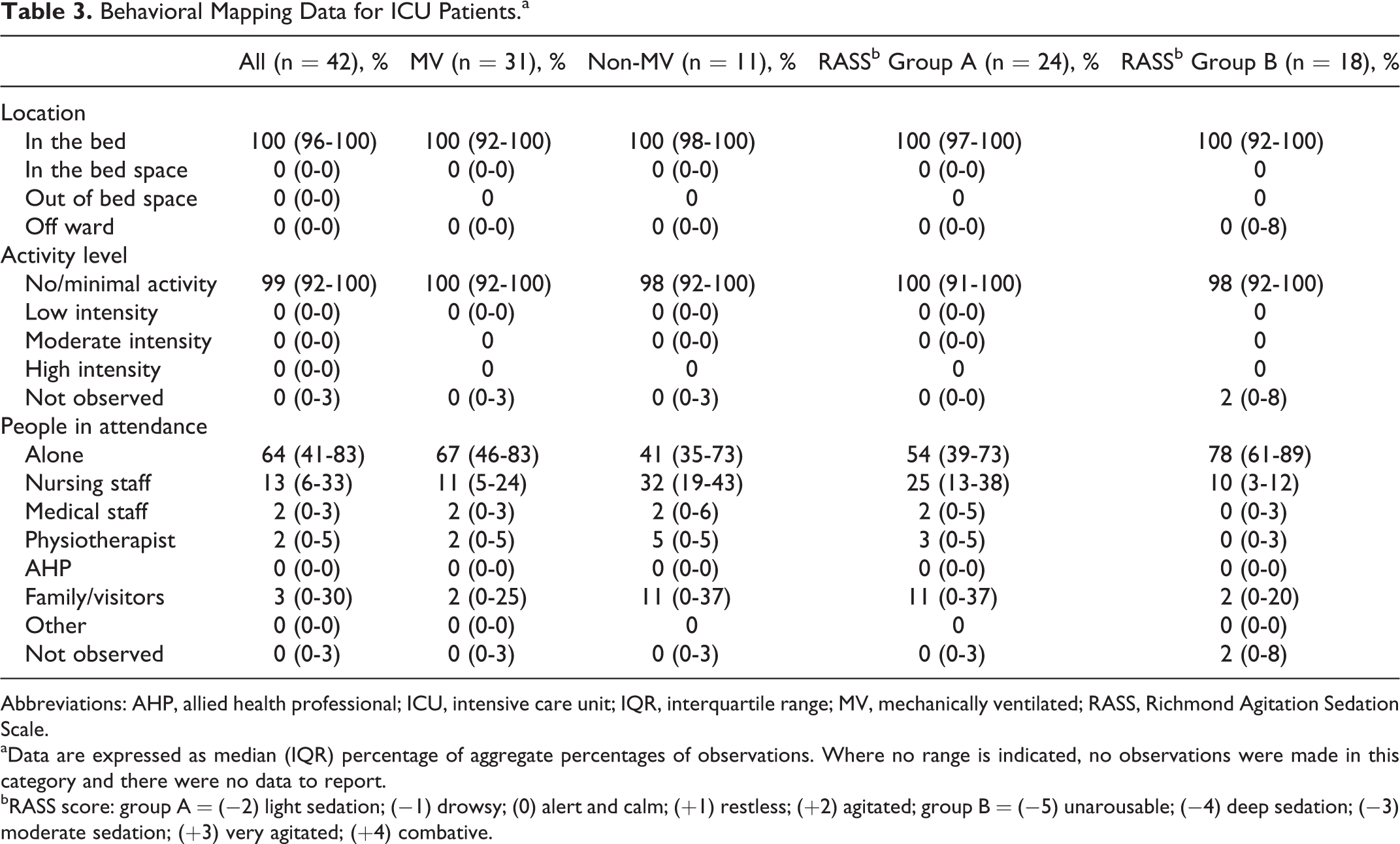
Abbreviations: AHP, allied health professional; ICU, intensive care unit; IQR, interquartile range; MV, mechanically ventilated; RASS, Richmond Agitation Sedation Scale.
aData are expressed as median (IQR) percentage of aggregate percentages of observations. Where no range is indicated, no observations were made in this category and there were no data to report.
bRASS score: group A = (−2) light sedation; (−1) drowsy; (0) alert and calm; (+1) restless; (+2) agitated; group B = (−5) unarousable; (−4) deep sedation; (−3) moderate sedation; (+3) very agitated; (+4) combative.
The proportion of time spent engaged in no/minimal activity was similar regardless of mechanical ventilation or sedation status. Overall, ICU patients spent 64% (41%-83%) of the observation day alone. Nonmechanically ventilated patients spent proportionately less time alone (41% [35%-73%] vs 67% [46%-83%]) and more time with nursing staff (32% [19%-43%] vs 11% [5%-24%]) than mechanically ventilated patients. Heavily sedated patients spent 78% (61%-89%) of their day alone, which is proportionately higher than patients who were lightly sedated or awake (54% [39%-72%]). There were no differences in location, activity level, or people in attendance between patients observed weekdays and weekend days (Table 3; all P = not significant and not presented) or between day (up to 5.00
Nonmechanically ventilated and awake patients still spent a median of 100% (92%-100%) of their time in bed, engaged in no or minimal activity throughout the majority of the day (99% [87%-100%]; Table 4). Nursing staff were most frequently observed in attendance irrespective of the patient’s ventilation or sedation state (Table 4), although patients still spent approximately two-thirds of the day alone regardless of status. All ICU patients observed within 72 hours of admission were nursed in bed (100%) and completed no or minimal activity (99%). Similarly, there remained minimal activity evident in patients as length of stay increased (72 hours to 7 days, 98% [92%-100%], and >7 days, 100% [84%-100%] of time spent participating in no/minimal activity; Online Appendix E3, “Activity profile of intensive care unit patients”).
Behavioral Mapping Data of ICU Patients According to Ventilation and Sedation Status.a
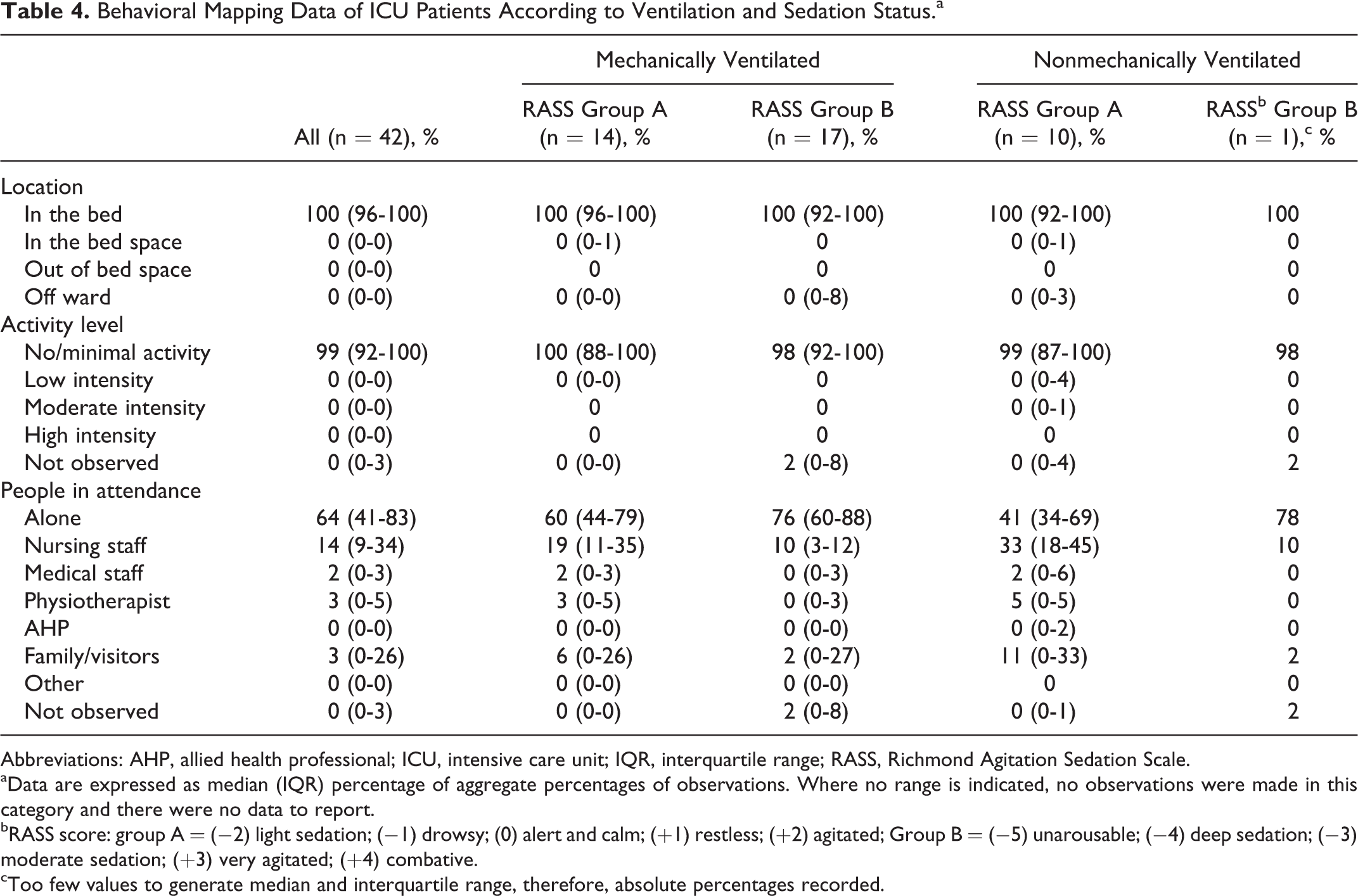
Abbreviations: AHP, allied health professional; ICU, intensive care unit; IQR, interquartile range; RASS, Richmond Agitation Sedation Scale.
aData are expressed as median (IQR) percentage of aggregate percentages of observations. Where no range is indicated, no observations were made in this category and there were no data to report.
bRASS score: group A = (−2) light sedation; (−1) drowsy; (0) alert and calm; (+1) restless; (+2) agitated; Group B = (−5) unarousable; (−4) deep sedation; (−3) moderate sedation; (+3) very agitated; (+4) combative.
cToo few values to generate median and interquartile range, therefore, absolute percentages recorded.
Details of physical therapy sessions delivered on the day of observation are reported in the Online Appendix E4 (“Physical therapy sessions delivered to ICU patients on the day of observation”). Ten patients participated on exercise rehabilitation with activities ranging from sitting over the edge of the bed to transferring to the chair. No high-intensity activities were performed, for example, ambulation.
Physical Activity in the VWU
Eleven patients were included between August and December 2015. Characteristics of the cohort are reported in Table 2. Three patients (27.3%) required mechanical ventilation via tracheostomy. Length of stay prior to observation was 12.7 (2.8-26.6) days. Of the 11 patients included, none had any restrictions to physical activity in place on the day of observation. Nine (81.8%) patients had received exercise therapy (range: 1-24 sessions) prior to observation, with 3 achieving a sitting over the edge of the bed, 2 standing, 3 ambulating with assistance, and 1 independently mobilizing greater than 100 m with a frame.
In total, 693 observations were recorded over a period of 5 observation days which comprised 3 weekdays and 2 weekend days, with no missing data points. Across all observations, patients spent 94% (73%-100%) of the day (>9.9 [7.7-10.5] hours) located in bed, with no or minimal activity for 92% (73%-100%) of the day (approximately 9.7 [7.7-10.5] hours; Table 5). Nonmechanically ventilated patients spent a similar proportion of time alone as those mechanically ventilated patients. However, patients requiring mechanical ventilation (6% [6%-10%]) were observed to spend proportionately less time with nursing staff than those not requiring mechanical ventilation (16.5% [13.3%-21.8%]; Table 5).
Behavioral Mapping Data for Ventilator Weaning Unit Patients.a
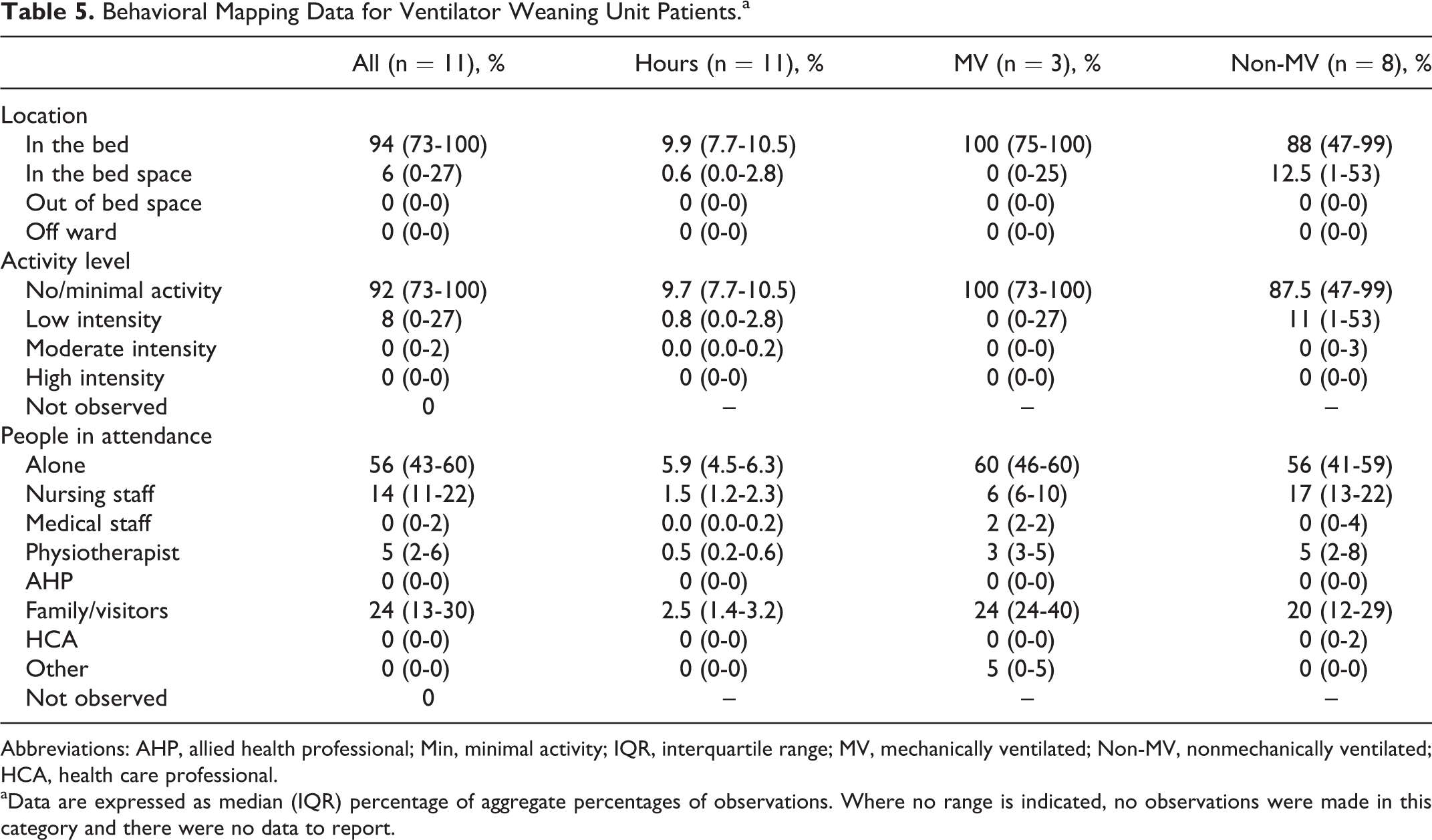
Abbreviations: AHP, allied health professional; Min, minimal activity; IQR, interquartile range; MV, mechanically ventilated; Non-MV, nonmechanically ventilated; HCA, health care professional.
aData are expressed as median (IQR) percentage of aggregate percentages of observations. Where no range is indicated, no observations were made in this category and there were no data to report.
The proportion of patients with a tracheostomy (n = 9) and those without (n = 2) precluded examining differences between these groups. Furthermore, all VWU patients had previously spent more than 7 days in an ICU, with a preobservation length of stay in the weaning unit of nearly 2 weeks; hence, an analysis of observations according to length of stay was not considered appropriate. Details of therapy sessions delivered on the day of observation are reported in the Online Appendix E5 (“Physical therapy sessions delivered to VWU patient on the day of observation”). Among the 9 patients who participated in exercise therapy, 2 engaged in high-intensity activity, mobilizing between 80 and 200 m.
Discussion
Data from this study demonstrate low levels of physical activity in a representative cohort of critically ill patients in a UK ICU irrespective of ventilator, sedation status, or day of the week. Patients spent approximately two-thirds of the day alone and the whole day in bed. These findings were echoed in a cohort of longer-term critically ill patients in a VWU, albeit with a small increase in the proportion of time spent engaging in activity evident. Physical activity in both patient cohorts primarily occurred during physiotherapy rehabilitation sessions, with higher-intensity activity achieved by patients on the weaning unit. These data underscore the urgency of strategies required to increase the physical activity behavior profile of critically ill patients during acute and subacute stages of recovery from critical illness.
Clinical Significance of the Findings
The benefits of physical rehabilitation delivered in the ICU are well established. 10 However data from previous observational point prevalence and observational studies indicate the reality of clinical practice deviates from the evidence base, 15,17,18,24 resulting in an “evidence–reality” gap. Specifically, our findings mirror those recently published from a behavioral mapping study conducted in an Australian ICU of similar construct and involving a patient cohort with similar clinical features. 16 Physical activity levels in current ICU patients were minimal regardless of ventilator or sedation status, with little change observed with increasing duration of ICU length of stay. Physiotherapeutic interventions represented the focal point of activity during the observation period but occurred in only a small number of patients. Active engagement with patients was also low, with patients classified as alone for two-thirds of the day.
So how can these data inform our current understanding around physical activity and rehabilitation in critically ill patients? The recent volume of interventional trials of early mobilization that have failed to show a difference in outcome 13,27,28 might infer skepticism as to the value of early mobilization-based physical rehabilitation interventions where there is widespread empirical evidence of clinical value. 29 Where benefit has been shown in previous studies, factors such as premorbid functional status 30 and timing of intervention commencement 31 may have selected a patient group more likely to benefit. Certainly, optimizing features around methodological study design may assist in future investigations and may have contributed to the findings from “negative” trials thus far. 32 –34
However, data from this study, and indeed its precedent, 16 would support the need for a broader shift in ICU culture toward providing patients with, and engaging them in, a multidisciplinary, multiprofessional environment that enhances overall physical activity levels. Early mobilization currently appears discretionary against a backdrop of routinely sedentary behavior in patients, which could also explain a failure to show difference if interventional trials involve a “dose” of physical rehabilitation insufficient to overcome residual inactivity throughout the remainder of the day. Furthermore, detailed process evaluation of reporting interventions would elucidate on the amount of time within a rehabilitation session that involved patient participation (whether active or passive) as opposed to “preparatory” time.
Early mobilization can be safely delivered across the spectrum of multi-organ support including to patients receiving ECMO, 35 renal hemofiltration, 36 and inotropic/vasopressor support, 37 with consensus criteria to assist in clinical decision-making. 37 While clinical stability is a prerequisite for commencement, which will vary in time across patients, the current findings were nonetheless acquired in patients with reducing illness acuity levels at a median of 8 days admission. There, therefore, seems significant scope for potentially affecting the degree of activity within the ICU for such patients.
Broadening our interpretation of “rehabilitation” may facilitate this. In the rapid expansion of interest in management of critical illness morbidity, this term may have colloquially become synonymous with meaning “physical” therapy. Certainly, exercise-based interventions delivered by physiotherapists represent a key component of rehabilitation and increasing physiotherapy sessions may result in commensurate increased activity, although a linear relationship between the two is unlikely, given the optimal “dose” of physical rehabilitation for critically ill patients has yet to be determined but highly individualized. Other domains of occupational, psychological, and cognitive therapy are also vital. Employment of strategies related to these aspects may contribute to increasing the volume of activity and minimizing sedentary behavior for patients throughout the day, excluding focal periods of physiotherapy, with the potential added benefit to reduced incidence of delirium. Furthermore, the routine of physical rehabilitation delivery itself may need further adaptation. Dose–response analyses of very early rehabilitation delivered to patients with stroke revealed improved odds of favorable outcome with shorter, more frequent mobilization sessions focusing on out-of-bed activities. 38 Our findings were against a backdrop of physiotherapy staffing that met UK national guidelines for ICU 2 where participation in physiotherapy rehabilitation represented the highest activity levels for patients. Units with lower staffing profiles may find alternative models of delivering rehabilitation valuable for optimizing resource utilization and allocation and/or demonstrate the need for increasing personnel.
We found no difference in levels of physical activity across weekdays or weekend days. In contrast, addition of a Saturday service across 2 long-term rehabilitation centers resulted in higher levels of functional independence at discharge, albeit these settings did not encompass post-critical illness patients. 39 Our patients admitted to a long-term VWU were generally more active than the acute ICU cohort, although this was again only evident from the activity undertaken as part of exercise rehabilitation delivered by physiotherapists. This could be surprising, given that these patients were typically in single-organ (respiratory) failure and where the emphasis in the setting was on weaning and rehabilitation. Such data are similarly borne out in activity data from other chronically critically ill patient cohorts. 24 Again, maximizing multiprofessional interaction may counter these levels of reduced activity.
Data from the current study suggest a greater role for involvement of families and caregivers in the rehabilitative management of patients; certainly, in the VWU, this group was most frequently observed with patients. Psychosocial morbidity including stress, anxiety, and depression is common among ICU caregivers, with the critical care admission period the most high risk. 40 Engagement with these advocates in the rehabilitation process of patients may benefit both the patients and caregivers alike.
Critique of the Method
Our study adopted a rigorous behavioral mapping protocol previously reported in the ICU population, 16 allowing for direct standardization, comparison, and contrast across data sets. Replication of methodology is a notable strength of the current study, validating the process and allowing opportunity to corroborate prior published findings in a separate location and context. Randomized controlled trials are inherently challenging to conduct in critical care rehabilitation due to recruitment restrictions, attrition, and clinical acuity of patients 13,27,28 ; hence, demonstrating utility of alternative approaches to investigating this field is of benefit until elements of randomized trial design are optimized. A single researcher was responsible for conducting all observations to maximize robustness of the data, and data were recorded throughout the entirety of a daily working shift and across weekdays and weekend days to capture all potential episodes of physical activity. A standardized and pragmatic approach to screening was also adopted to determine sufficient numbers of eligible patients, whereby ICU admissions were reviewed in order of bed number each day. However, we acknowledge the potential for recruitment bias where eligible patients were not included once the maximum number (n = 6 due to feasibility of data acquisition) had been achieved, or conversely the minimum number (n = 3 due to labor intensity of data acquisition) was not available on any given day. That said, apart from the 6 designated ECMO beds contained within a discrete area of the ICU, there are no other local protocols in place such that only certain diagnostic categories of patient are admitted to certain beds (notwithstanding infection control/necessary isolation requirements for side room usage, but which in itself would not have excluded any patient).
We classified activity levels according to an internationally standardized scale with proven psychometric properties, 25,41 albeit we expanded this scale to include 2 nonvalidated levels that were identified through the pilot phase of this study. These levels have been previously reported in the prior mapping study of ICU patients and were elements of an activity hierarchy scale developed by expert clinicians. 16
Our definition of being “alone” may have contributed to the high percentages of patients observed in this category especially for those in the ICU cohort, albeit our definition was in keeping with previous studies both in critically ill 16 and stroke 20 populations. Active interaction with the patient was required for an individual to be classified as in attendance with a patient. For this reason, “indirect” contact associated with the more “technical” aspect of management and which could be considered more passive on the part of the patient, for example, carrying out common clinical activities such as changing medications or taking arterial blood samples, or the presence of the medical ward round, did not suffice for this, although we accept that these are necessary aspects of patient care in the ICU in particular for those patients with greater illness acuity. We recognize the potential for error in this classification if the event is unclear in nature and that this method does not capture data on simple presence of individuals at the bed space. Nonetheless, alternatively, determining presence of individuals with a patient, for example, by way of a geographical boundary around the bed space, would still not have delineated between active and indirect forms of contact, which we considered to be an important consideration.
One key limitation of behavioral mapping is the assumption that each 1-minute period of observation is representative of the whole 10-minute unit of time. That minimal activity levels were observed in the current cohorts from the high volumes of observations performed throughout the day (including detail of physiotherapy sessions) and would suggest that higher levels of activity were not missed. The frequency of observations accumulated through the behavioral mapping approach allows for detailed characterization of physical activity patterns. 16 This is a more robust design than point prevalence or audit data that may artificially report high levels of physical activity based on single data collection points. 15,17,18,42 However, by only acquiring data on a single day, this precludes identifying higher activity levels that may have occurred prior to, or subsequently, during the ICU admission. In the future, detailed longitudinal data may assist in further characterizing physical activity levels during critical illness and, in particular, profiling delivery of exercise-based rehabilitation to greater reflect local service. 43
We acknowledge this is a single-center study limiting the generalizability of findings to other ICUs or weaning units with differing case mixes, service models, bed capacity, or local policy around rehabilitation practice. In particular, a recent survey of international ICUs on unit structure and mobilization practice revealed that half of UK sites surveyed (n = 150) had some form of early mobilization practice in place, and 20% according to a written protocol. 44 This variability is important to consider when interpreting the current findings which are inherently influenced by the local practice in the study site; there is no formal, written protocol for rehabilitation in operation and physiotherapists use autonomous clinical reasoning based on individual clinical assessment of each patient. This could have introduced a source of bias into physical activity findings where other factors such as culture, competence, knowledge, and attitudes toward rehabilitation (and thereby physical activity) could have been influential. 45
That said, the labor intensiveness of the behavioral mapping approach to data acquisition is likely to preclude the feasibility of more widespread replication; the strength of this more qualitative style to data collection is the rich detail of the resulting data set. These data represent the first of their kind from a UK ICU, reporting detailed levels of activity undertaken by critically ill patients and examining a sufficient sample size to produce robust findings. Furthermore, we expanded the previous data reported by Berney et al 16 by additionally examining a cohort of longer-term critical illness patients in a VWU. While the sample size for this cohort of long-term weaning patients is smaller than may be considered representative, 23 and this precluded certain descriptive analyses, we adopted a pragmatic approach to recruiting this convenience sample in light of differing admission rates and patient profiles in a VWU and felt that these novel data provide valuable information regarding physical activity in this particular subgroup of post-critical illness patients. In the future, these data could be used to support development of a larger, multisite, multinational study that could account for institutional- and ICU-level factors, in addition to patient-level factors, that contribute to outcomes. 19
We acknowledge that the different nurse to patient ratio of 1:2 on the VWU needs to be considered when interpreting results of frequency of patients being classified as “alone” when compared to the ICU cohort where the ratio is 1:1. In addition, we did not prospectively record any physiotherapy clinical decision-making around delivery of physical rehabilitation on the day of observation to explore this as a contributory factor in activity levels in greater depth nor did we capture the amount of time patients were actively participating in rehabilitation as a proportion of the overall session duration. We acknowledge some patients may have presented with barriers to mobilization, although only one had an existing medical restriction order.
Conclusion
We aimed to use behavioral mapping to prospectively characterize the physical activity profile of critically ill patients in both a UK intensive care and VWU. This approach revealed low levels of activity, further demonstrating the limited application of research findings around safety, feasibility, and potential efficacy of ICU rehabilitation to the clinical environment, the “evidence–reality gap.” Even in longer-term post-critical illness patients residing in a VWU with an emphasis on rehabilitation, scope for increasing physical activity was clear. In order to achieve this, increasing physical activity levels and minimizing sedentary behavior beyond therapeutic rehabilitation sessions delivered by physiotherapists appear essential. More broadly, given the prevalence of international data sets now reporting similar findings, it is evident a behavioral change toward providing critically ill patients with, and engaging them in, a multidisciplinary, multiprofessional environment that optimizes overall physical activity is warranted to reduce the gap in knowledge translation of the benefits of activity in this patient cohort.
Supplemental Material
APPENDICES - Low Levels of Physical Activity During Critical Illness and Weaning: The Evidence–Reality Gap
APPENDICES for Low Levels of Physical Activity During Critical Illness and Weaning: The Evidence–Reality Gap by Bronwen A. Connolly, Jessica L. Mortimore, Abdel Douiri, Joleen W. Rose, Nicholas Hart and Susan C. Berney in Journal of Intensive Care Medicine
Footnotes
Authors’ Note
Bronwen A. Connolly was responsible for study conception, design, data analysis, and interpretation, and drafted, revised, and agreed the final manuscript version for submission. Jessica L. Mortimore was responsible for data acquisition and contributed to data analysis and interpretation. Abdel Douiri contributed to data analysis and interpretation. Joleen W. Rose and Nicholas Hart contributed to data interpretation. Susan C. Berney contributed to study design and data interpretation. All authors contributed to manuscript revision and approved the final version for submission. Bronwen A. Connolly acts as the guarantor for the intellectual integrity of the data. For reasons of confidentiality, the data set supporting the conclusions of this article is not available in any repository.
Acknowledgments
We gratefully acknowledge the assistance of Craig Whiteley and Omar Shaikh for clinical data provision.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bronwen A. Connolly is funded by a National Institute for Health Research (NIHR) Postdoctoral Fellowship (PDF-2015-08-015). Bronwen A. Connolly, Abdel Douiri, and Nicholas Hart are supported by the NIHR Biomedical Research Centre based at Guy’s and St. Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors are not necessarily those of the NHS, the NIHR or the Department of Health.
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.