
Abstract
Headache disorders are one of the most frequent pediatric health complaints and are associated with impairments in daily functioning and increased rates of anxiety and depression. In adults with headache disorders, self-management education has successfully improved headache self-efficacy; however, no studies have evaluated this in a pediatric population. Hence, a pre-post comparison pilot study was conducted to evaluate the feasibility, acceptability, and effectiveness of a 1-time, 90-minute, in-person, group workshop on headache self-management. Participant-reported headache self-efficacy and chronic illness self-efficacy were assessed before the intervention to evaluate changes in self-efficacy 2 weeks after the intervention. Thirty participants completed the study [mean (SD) = 14.7 (1.5) years; 73% female]. Of those who responded to the acceptability survey (n = 13), all reported being very satisfied. Headache self-efficacy increased (P = .002), whereas chronic illness self-efficacy was unchanged (P = .445). The results from this pilot study will inform a larger-scale trial.
Keywords
Headache disorders are one of the most frequent pediatric health complaints in North America.1,2 Fifteen percent of Canadian children experience weekly episodes of headache 1 and 10% of North American youth are diagnosed with migraine. 2 Headache disorders in the pediatric population negatively influence quality of life and daily functioning. 3 Pediatric headache disorders are associated with disturbed sleep patterns,4–6 increased rates of bullying,7,8 school-reported problems, 9 anxiety,10–12 depression,10–12 and suicidality. 8
Self-management is described as an emphasis on both the patient and the provider actively treating a disease, with the patient managing the disease outside the clinical setting. 13 Self-management requires confidence, knowledge, and motivation to make decisions and problem solve. 14 Current guidelines highlight the importance of self-management for chronic diseases such as headache disorders.13,14 An individual's confidence in managing their condition, known as self-efficacy, is an important factor influencing their ability to self-manage symptoms.15,16 Greater levels of self-efficacy are positively associated with the initiation of self-care practices, the degree of effort invested, and the duration for which that effort is maintained in the face of obstacles.15,17 In the pediatric population with chronic conditions (eg, type 1 diabetes, juvenile rheumatoid arthritis, cystic fibrosis, urologic conditions, and neuromuscular disorders), perceived self-efficacy has been positively associated with emotional, physical, and social quality of life. 18
Headache-specific self-efficacy is defined as “a patient’s confidence that they can take actions that prevent headache episodes or manage headache-related pain and disability”. 19 In the adult headache population, higher rates of self-efficacy have been associated with lower rates of anxiety and the use of positive psychological coping strategies to prevent and manage headache attacks. 19 Similarly, children with headache disorders who have higher pain self-efficacy and acceptance experience less disability, improved school functioning, and fewer depressive symptoms. 20
Current literature supports the use of self-management strategies to improve patient outcomes for individuals with headache disorders. However, to our knowledge, no studies have examined the impact of headache self-management education (HSME) on self-efficacy in pediatric populations. Hence, we conducted a pilot study to evaluate the feasibility, acceptability and effectiveness of HSME at a large tertiary care pediatric hospital. Information and data from the pilot study will be used to refine the intervention, assess recruitment potential, and inform a larger-scale study. 21
Objectives
The objectives of the pre-post comparison pilot study were to evaluate the eligibility criteria, informed consent, data collection, recruitment and retention rates, and participant and caregiver acceptability of the HSME intervention. Participant-reported outcomes included headache self-efficacy, chronic illness self-efficacy, and behavioural change.
Patients and Methods
Setting and Participant Population
Individuals aged 12-17 years who were referred for headache disorders to a large tertiary care children's hospital between March and June 2024 were considered for participation. To be eligible, participants needed to have the capacity to provide informed consent for themselves and to be able to speak and understand English. The potential participant's capacity to consent was determined during the consent discussion by asking questions about their understanding of the study. If the potential participant demonstrated a comprehensive understanding of the study objectives, participant responsibilities, and risks of participation, they were deemed to have the capacity to consent for themselves. Exclusion criteria included triage to urgent consultation or lack of primary care provider. Because participants were awaiting consultation and were not actively being followed by the Neurology Clinic at the time of HSME, a primary care physician was essential to ensure that participants were under the care of a physician for any follow-up questions or mental health concerns, which are discussed during HSME. Eligible children were initially contacted by phone by a member of their circle of care (neurologist or nurse practitioner) to introduce the study. If they expressed interest, research staff contacted them to complete the informed consent process. Written electronic informed consent was obtained from all participants via REDCap. REDCap is a secure, web-based application designed exclusively to support data capture for research studies.
A total of 6 workshops were scheduled biweekly over a 10-week period. To facilitate group learning and collaboration, each workshop was held only if a minimum of 5 participants enrolled. Enrollment was capped at 12 participants per session to allow adequate time for introductions, feedback, and to comply with room capacity restrictions.
Intervention
The intervention consisted of a 1-time, 90-minute, in-person, group workshop on HSME, delivered on-site at the study hospital. The intervention was developed by a pediatric neurologist with extensive training, experience treating, and knowledge of pediatric headaches. Workshops were scheduled on weekdays (Monday through Thursday) starting at 17:30. One of 2 nurse practitioners with specialized training in pediatric headache management or a pediatric neurologist facilitated the workshops. The pediatric neurologist led a 60-minute training session detailing how to facilitate the workshop. The training session began with a general overview of the workshop and the study objectives. This included characteristics of attendees (participants, caregivers), length of workshop, and modality of workshop. Next, the slides were presented one-by-one, and the purpose and context of each was discussed. A script was not provided, but general talking points were highlighted. The trainees had a chance to ask questions after each slide. There was additional time for questions at the end of the training session. The training session ended once all questions were answered. Each workshop was separated into two 45-minute phases, and participants were required to attend both phases. Caregivers were welcome, but not required, to attend the first phase. The second phase was for participants only.
The first phase began with introductions, followed by a didactic teaching session. Topics covered included headache types, migraine aura, strategies for preventing and treating headache attacks, medication overuse headaches, and the use of a headache diary.
The second phase of the workshop focused on coping with psychosocial impacts of frequent headaches, including physical, emotional, social, and school-related challenges. The relationship between headache disorders and mental health was discussed, and participants were provided with information on available mental health support resources. An icebreaker activity was used to facilitate introductions among participants, followed by 6 case scenario questions related to the workshop content. The facilitator prompted and encouraged group discussion to address the scenarios.
Participants received a resource portfolio at the workshop that included a SMART goal worksheet, headache diary and medication history worksheets, community mental health resources, Migraine Canada pediatric dosing guidelines, Migraine Canada school letter templates, and the Children's Hospital of Eastern Ontario “Help with Headaches” handout.
Data Collection
Demographic information, including age at the time of the workshop and sex assigned at birth, was collected. Questionnaire administration and data collection were conducted using REDCap. A visual depiction of the study flow is displayed in Figure 1. Two questionnaires were administered at baseline (0-3 days prior to the workshop): Headache Self-Efficacy Scale 22 (HSES) and the Pediatric Rating of Chronic Illness Self-Efficacy (PRCISE). 23 The HSES is a 25-item questionnaire that measures an individual's confidence in headache prevention, headache pain management, and headache-related disability. 22 Responses range on a scale of 1 = strongly disagree, to 7 = strongly agree. 22 The HSES has only been validated in the adult population, 22 which limits the interpretation in this study population. However, to our knowledge, it is the only measure specific to headache self-efficacy. The PRCISE scale is a 15-item Likert-style questionnaire. 23 Participants are required to circle a number from 0 (not at all sure) to 10 (very sure) that best describes how sure they are in managing their illness, mood, symptoms, exercise, obtaining help, and recreational activities. 23 The PRCISE questionnaire has been preliminary validated as a reliable measure of self-efficacy in 7-20-year-olds. 23 At the conclusion of the workshop, participants and caregivers were encouraged to complete an anonymous feedback survey. Respondents indicated whether they were a participant or caregiver and rated their overall satisfaction with the HSME workshop on a scale of 1 (very dissatisfied) to 5 (very satisfied). An open-text field was provided for additional feedback. Two weeks post intervention, participants completed 3 follow-up questionnaires: HSES, PRCISE, and a behavioural change survey. An unvalidated four-item behavioural change survey was developed by the authors to determine whether participants modified their behaviour known to influence headaches following the HSME. Participants were asked to indicate their level of agreement (agree, neutral or disagree) to the following 4 statements: “Since the headache self-management education workshop, I… (a) have a more regular sleep schedule, (b) skip fewer meals, (c) drink less caffeine, and (d) am more physically active.” These questionnaires could be completed up to 6 weeks after HSME, provided they were submitted prior to the participant's scheduled consultation appointment.
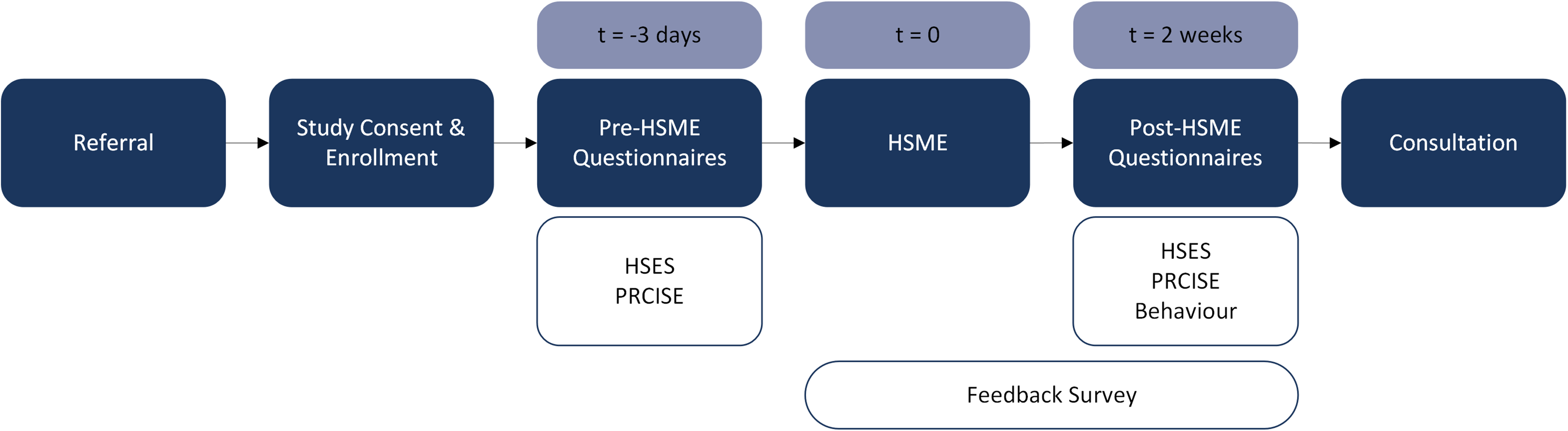
Study flow diagram. Abbreviations: Behaviour, behavioural change survey; HSES, headache self-efficacy scale; HSME, headache self management education; PRCISE, pediatric rating of chronic illness self-efficacy; t, time.
Feasibility
The pilot study evaluated the feasibility of the eligibility criteria, informed consent process, and data collection methods. During the recruitment phase, researchers identified the suitability of the inclusion and exclusion criteria. To evaluate the informed consent process, the research coordinator documented the consent process for each participant. During the consent process, the coordinator noted any questions that suggested revisions to the consent form. The coordinator also tracked any issues with data collection in the REDCap system.
To assess the recruitment rate, the total number of participants who enrolled in the study during the recruitment phase was tracked. Retention was reported as the percentage of enrolled participants who attended the HSME and completed the postintervention questionnaires.
Acceptability
Participant and caregiver acceptability of the HSME was evaluated based on responses to the anonymous satisfaction and feedback survey.
Effectiveness
Descriptive statistics [mean and standard deviation (SD)] were calculated for the participants’ age, pre- and post-intervention HSES, 22 and PRCISE 23 scores. The Shapiro-Wilk test was used to assess for normality. Paired samples t tests were conducted to compare pre- and post-intervention scores on the HSES and PRCISE scores. Missing data were accounted for using the baseline observation carried-forward method. 24 All analyses were performed using SPSS v. 29. 25
Results
Participant Characteristics
Thirty participants attended HSME. Participants had a mean (SD) age of 14.7 (1.5) years, and 73% were female. The assumption of normality was met for all data sets, as confirmed by independent Shapiro-Wilk tests.
Feasibility
Recruitment and retention rate
A total of 95 individuals were assessed for study eligibility. Seventy-five patients were deemed eligible for participation, of which 37 (49%) enrolled. Eighty-one percent (n = 30) of the enrolled participants received the intervention by attending the HSME. Twenty-four HSME attendees completed all the post-HSME questionnaires (80%), and 1 participant partially completed the post-HSME questionnaires. Five participants were lost to follow-up.
Fifty-eight were excluded because they were not interested in participating (n = 38) or they did not meet eligibility criteria (n = 20). Among the 20 ineligible participants, reasons included language barrier (n = 5), no primary care provider (n = 4), lack of capacity to consent (n = 4), urgent referral (n = 1), and atypical presentation (n = 6). Seven consented but did not attend HSME: 4 were no-shows, and 3 had their workshop cancelled because of low enrollment. A summary of participant screening, enrollment, and follow-up is presented in a CONSORT flow diagram (Figure 2
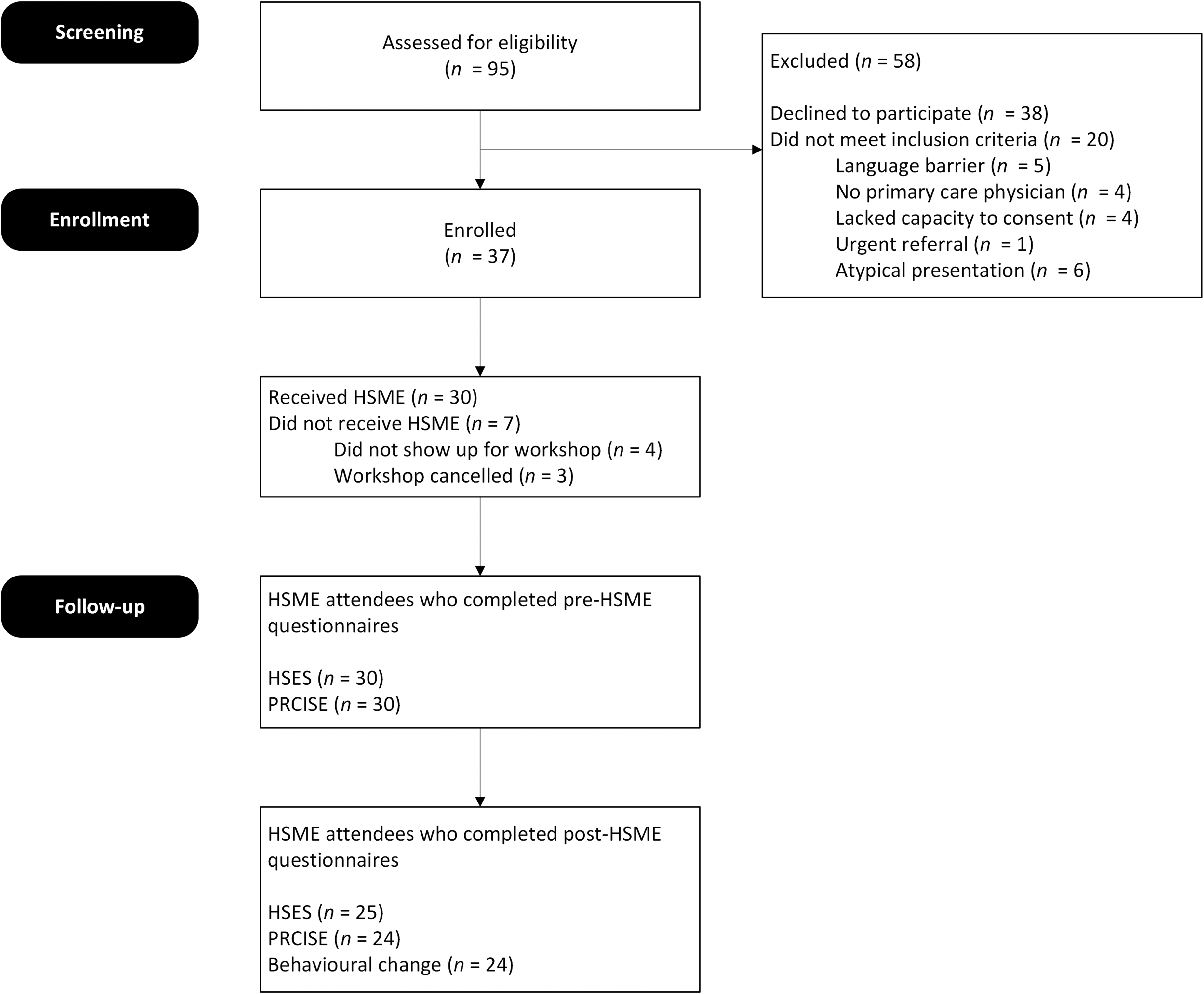
CONSORT flowchart of screened and enrolled participants.
Six workshops were scheduled; however, 2 were cancelled because of low enrollment. Therefore, 4 workshops were run with 6 to 9 participants in each.
Assessment of informed consent form
The informed consent form was found to be largely thorough and detailed. However, information was missing in the informed consent form and protocol regarding the cancellation of HSME workshops. Five participants were required to run a workshop; however, there was no information on when the decision to cancel a workshop would occur, and when or how participants would be notified. The following statement should be added to the informed consent form: “A minimum of five participants are needed to run a workshop. There is a chance that the workshop you sign up for will be postponed or cancelled due to not having enough participants. You will be notified by email at 12:00 pm the day before the workshop with a cancellation notice if this occurs.”
Assessment of eligibility criteria
The proposed eligibility criteria were generally acceptable; however, 1 additional exclusion criterion was required, which excluded 6 of the 95 participants assessed for eligibility. This exclusion was for an “atypical presentation, in the opinion of the triaging neurologist”. Three of the 6 patients who were excluded for this were noted to have “too many comorbidities.” These were serious or life-threatening comorbidities, in which the HSME was felt to be inappropriate. The other 3 excluded patients had an atypical presentation of headaches, which indicated to the triaging neurologist that the information in the HSME would not be suitable.
Assessment of the data collection method
No issues were noted with the REDCap platform for obtaining informed consent or questionnaire data.
Acceptability
Thirteen responses to the participant and caregiver anonymous feedback survey were received. Three respondents were patient participants, and 10 were parents or caregivers. All respondents were very satisfied, and open-text feedback was extremely positive and enthusiastic.
Effectiveness
Headache self-efficacy
A paired samples t test was conducted to compare pre- and post-HSES scores (Figure 3). There was a significant increase in headache self-efficacy using the HSES tool [pre = 72.6 ± 21.5 to post = 78.8 ± 23.3; t(29) = 3.1, P = .002], with a small effect size (d = 0.28).
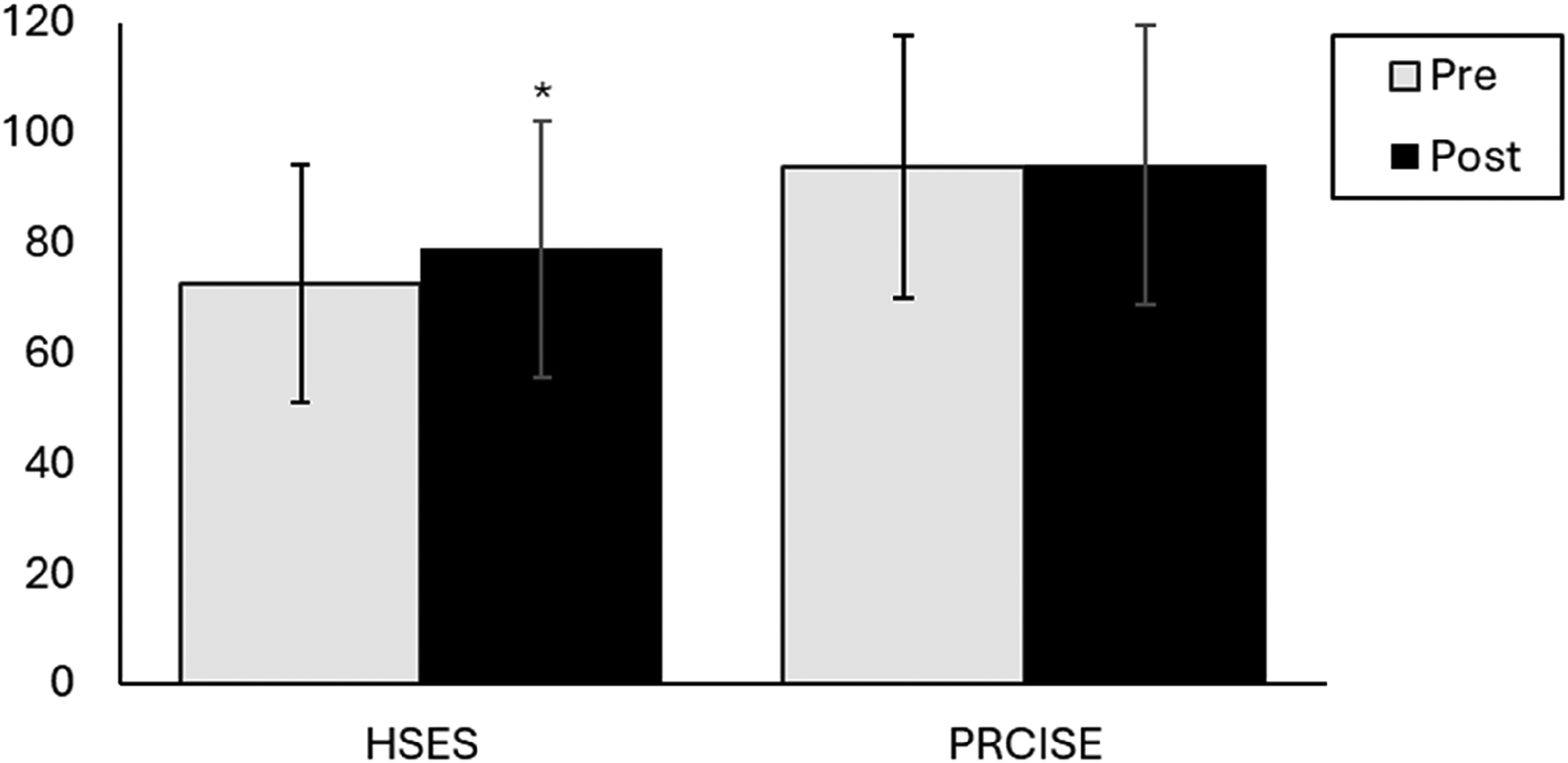
Pre- and post-intervention HSES and PRCISE scores (*P < .05). HSES, headache self-efficacy scale; HSME, headache self-management education; PRCISE, pediatric rating of chronic illness self-efficacy.
Chronic illness self-efficacy
A paired samples t test was conducted to compare pre- and post-PRCISE. There was no statistically significant change observed [pre = 93.7 ± 23.9 to post = 94.0 ± 25.4; t(29) = 0.1, P = .445], with a negligible effect size (d = 0.01).
Behavioural change
Of the 24 respondents, 10 (42%) stated that they drink less caffeine, 8 (33%) were more physically active and skipped fewer meals, and 6 (25%) kept a more regular sleep schedule following HSME.
Discussion
The current pilot study aimed to evaluate the eligibility criteria, informed consent, data collection, recruitment and retention rates, and participant and caregiver acceptability as well as examine changes in headache self-efficacy after the intervention. To our knowledge, this is the first study to show positive outcomes for self-efficacy following self-management education in a pediatric population.
The current literature on pediatric studies with an active headache self-management or education intervention arm includes 3 RCTs with 30-37 participants in each, none of which examined self-efficacy.26–28 Walter et al's 27 intervention was in-person, with multiple sessions over 6 weeks and had both individual and group components. Hickman et al 26 had both in-person and remote components, individual and group components, and was completed over multiple sessions spanning 7 weeks. Connelly et al 28 designed an individual, remote intervention with four 1-hour sessions.
In our study, half of the eligible participant population provided consent to attend the HSME workshop. This 49% enrollment rate is lower than comparable studies in the pediatric population. For example, Walter et al, 27 Hickman et al, 26 and Connelly et al 28 had enrollment rates of 86%, 84%, and 74%, respectively. Several factors may explain the lower enrollment rate in our study. Our hospital has a wide catchment area, making in-person attendance challenging for some referred patients who live hundreds of kilometres from the hospital. Additionally, a limited number of workshops were offered over a relatively short period of time, which may have logistically limited the number of participants. Workshops were scheduled on weekday evenings (Monday through Thursday) which may have conflicted with school and family obligations. Offering weekend sessions in future studies may improve accessibility. A focus group or interview study including all eligible individuals may help identify specific barriers to enrollment and inform future recruitment strategies.
In the current study, 80% of HSME participants fully completed the follow-up questionnaires. This is slightly lower than Hickman et al 26 (86%), Walter et al 27 (87%), and Connelly et al 28 (84%). It is also notable that there was no incentive for participants to complete the follow-up questionnaires, as it did not affect the scheduling of their consultation appointments, there was no financial incentive, and they would receive no further HSME. When designing and budgeting for a larger-scale study, incorporating a modest incentive, such as a gift card, stipend, or entry into a prize draw, may improve retention rates. 29
Although the responses to the satisfaction survey were overwhelmingly positive, the response rate was low, with only 3 of 30 participants and 10 caregivers completing the survey. The satisfaction and feedback survey could not be mandatory because of the need to maintain respondent anonymity. The survey was presented during the workshop, at the end of phase 1, and included in the participant handouts. However, additional efforts could have been made to improve response rates. For example, sending a follow-up email with a survey link the day after the workshop may have encouraged greater participation. Before developing an RCT, it would be beneficial to invite participants and caregivers from the current study to attend focus groups. These sessions could provide deeper feedback on the enrollment process, preferred delivery mode, workshop duration and content of the HSME, as well as follow-up procedures.
Analysis of the behavioural change survey indicated a need to revise the response options. Participants responded to directional statements (eg, “Since the workshop, I am more physical active”) using a 3-point scale: agree, neutral, and disagree. However, the distinction between neutral and disagree was unclear, making interpretation difficult. Therefore, for future larger-scale studies, we recommend removing the neutral response option to improve clarity and analytic value.
Baseline headache self-efficacy scores of 72.6 ± 21.5 observed in our pediatric population were lower compared to published literature in adult headache patients, where baseline scores range from 97 to 114.30–32 However, direct comparison is limited, as the HSES 22 has only been validated in the adult population. Therefore, interpretation in the pediatric study population is limited. It is plausible that self-efficacy in this sample population may be lower because of a greater reliance on caregivers for managing care and advocacy.
The self-efficacy score using the HSES 22 increased by 6 points 2 weeks after HSME; however, the pre-post study design limits our ability to attribute this increase solely to the HSME intervention. Additional data are needed to determine whether this change is clinically meaningful. For example, an assessment and comparison of improvements in headache frequency, headache-related disability, or quality of life to improvements in headache self-efficacy would provide insight to determine a clinically meaningful increase in the HSES. Bromberg et al 32 conducted an RCT with 185 adult participants, where headache self-management education was compared to standard of care. The intervention was fully remote, with participants being required to complete eight 20-minute modules in the first 4 weeks, followed by one 20-minute module monthly for 5 months. The modules involved completing self-assessments, using interactive tools, reading articles, and using a pain tracker. Headache self-efficacy was measured using the HSES, and at 6 months the standard of care group increased by 8 points, whereas the intervention group increased by 18 points. However, the decrease in migraine disability after 6 months was similar between groups (12.8% in the HSME group compared with 13.0% in the standard of care group). This suggests that even modest increases on the HSES may be clinically meaningful, such as in our study.
The baseline PRCISE score in our study population was 94.7 ± 23.9. This is lower than scores reported in published studies. In the preliminary validation study of the PRCISE scale, the mean score was 114 ± 32 among children with various chronic diseases and 114 ± 33 in the subgroup of children with neurologic disorders. 23 Gürcan and Turan 33 validated the PRCISE in 220 Turkish children with chronic illnesses and reported a mean PRCISE score of 106 ± 18. The PRCISE scores were slightly lower in the subgroup analysis for children with neurologic disorders, at 105 ± 22. Öncel and Solmaz 34 found a mean PRCISE score of 102 ± 22 in a pediatric multiple sclerosis cohort. Similar to HSES findings, our baseline PRCISE scores were lower than those reported in other published studies.
Unlike the HSES, PRCISE scores did not change following the HSME intervention. This discrepancy may reflect the difference in the focus between the 2 scales: the HSES measures headache-specific self-efficacy, whereas the PRCISE measures chronic illness self-efficacy more broadly. Pediatric headache disorders are associated with an elevated risk of several conditions, including attention-deficit hyperactivity disorder, depression, anxiety, epilepsy, obesity, atopic disorders, inflammatory bowel disease, and irritable bowel syndrome. 35 The HSME intervention primarily focuses on headaches, with some information and resources on psychological comorbidities, including depression and anxiety. However, it is possible that our study population had complex comorbidities, and as a result, the intervention did not significantly influence their overall chronic illness self-efficacy.
Behavioural modifications reported included drinking less caffeine (42%), skipping fewer meals (33%), being more physically active (33%), and keeping a more regular sleep schedule (25%). Walter et al's 27 RCT assessed changes in diet, caffeine, and sleep following an HSME intervention in a pediatric population. They found a significant improvement in diet in the intervention group, but no notable changes in sleep or caffeine intake. This is a difference from the current study, where nearly half of our participants reduced caffeine consumption following the intervention. Short 36 and Lagman-Bartolome et al 37 observed modest improvements in morning protein intake and sleep routines, following self-management interventions, aligning with the results observed in our study. Behaviours are often difficult to modify; therefore, we did not anticipate that our intervention would significantly improve any of the behaviours measured. Nonetheless, the observed trends suggest that even a single-session HSME workshop may support modest behavior change in adolescents with headaches.
To our knowledge, this is the first study to prospectively evaluate the association between HSME and self-efficacy in a pediatric population. The sample size is adequate for a pilot study and provides valuable evidence to support the future development of a large observational study or RCT to more definitively understand the role of HSME in this patient population.
The limitations of this study include the lack of a control group, the use of unvalidated surveys, participant self-selection, and a short follow-up period. Participants who chose to participate may have enhanced motivation for practicing self-management and improving self-efficacy, compared with those who declined participation. The population is likely not representative of the general pediatric headache population, given that they were referred to a tertiary care hospital, were required to speak English and have a primary care physician, and they were more likely to have the time, resources, and proximity to attend an in-person workshop. These factors limit the generalizability of the results. It is unknown whether increases in self-efficacy and behavioural changes are sustained over time because there was a single follow-up time point 2 weeks after HSME. Additionally, the response rate to the anonymous feedback survey was low, with only 3 participant and 10 caregiver responses.
Conclusion
Findings from this pilot study suggest that a single, in-person HSME intervention is feasible and may be acceptable for adolescents with headache disorders and may improve headache self-efficacy. To better understand and address recruitment rates, focus groups or interviews are warranted. This would allow for further refinement of the protocol and intervention. To distinguish whether HSME is causatively related to increased headache self-efficacy in this population, an RCT is warranted. Our pilot study provides valuable insights to inform and develop a future successful RCT in this population, including recruitment and retention estimates and effect size data for sample size calculations. Importantly, this research highlights the potential for brief, scalable educational interventions to improve self-management and health outcomes in pediatric headache populations. If supported by future trials, HSME could serve as a low-cost, early intervention strategy to enhance care delivery and reduce strain on tertiary services—offering meaningful implications for both clinical practice and health policy.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738261422878 - Supplemental material for Feasibility and Acceptability of a Self-Management Education Program for Adolescents with Headaches: A Pilot Study
Supplemental material, sj-docx-1-jcn-10.1177_08830738261422878 for Feasibility and Acceptability of a Self-Management Education Program for Adolescents with Headaches: A Pilot Study by Nicole Margaret Whitley, Daniela Pohl, Jennifer Ann Knopp-Sihota and Steven Thomas Johnson in Journal of Child Neurology
Footnotes
Acknowledgements
We thank all the children and their families for participating in this study, and Sammantha Dunseath, Pamella Fellbaum, Fatima Kazoun, and Eloise Deschenes for their assistance with facilitating the workshops.
Ethical Approval
This study was approved by the research ethics board at the CHEO Research Institute (No. 24/10X) and Athabasca University Research Ethics Board (No. 25635). Written informed consent was obtained by all participants.
Author Contributions
Nicole Whitley: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing. Daniela Pohl: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Supervision, Writing – review & editing. Jennifer Knopp-Sihota: Conceptualization, Methodology, Writing- review & editing. Steven Johnson: Conceptualization, Formal analysis, Funding acquisition, Methodology, Supervision, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research of this article: This study was supported by an internal grant from Athabasca University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.