
Abstract
This secondary analysis examined the association between preexisting mental health conditions and clinical recovery trajectories in adolescents with concussion. Adolescents (13-17; n = 1238) completed clinical assessments (Post-Concussion Symptom Inventory [PCSI] ≤48 hours postinjury; PCSI/ Pediatric Quality of Life [PedsQL] for 3 months) and were categorized into control, anxiety, depression, or combined anxiety/depression groups. Acute outcomes were analyzed using analysis of variance or χ2, whereas linear and logistic regression analyzed recovery trajectories. A main effect of group was present for acute symptom scores (P = .03), but post-hoc testing revealed no significant comparisons. Main effects of group and time were observed for PCSI and PedsQL outcomes (P < .007), but interaction effects were nonsignificant. The combined anxiety/depression group reported more symptoms, worse quality of life, and had greater odds of experiencing persistent postconcussion symptoms (defined as ≥3 new/worse symptoms at 4 weeks; OR = 2.31, 95% CI = 1.18-4.67, P = .02) in univariate models. However, multivariable models found no association between preexisting mental health conditions and the presence of PPCS (P = .62). Preexisting mental health conditions were associated with similar longitudinal trajectories but higher symptom and lower quality of life scores overall, highlighting their importance in adolescent concussion management.
Concussions are prevalent among children and adolescents, now accounting for 1 in 70 pediatric emergency department visits in Canada annually. 1 After concussion, children report symptoms in somatic, vestibular, cognitive, psychiatric, and sleep domains, which can negatively impact activities of daily living and overall quality of life. 2 Most children and adolescents (defined here as youth aged 5-18 years) experience symptom recovery within 4 weeks of concussion, 3 but ∼30% have persistent postconcussive symptoms (PPCSs) that last beyond the first month after injury.4–7 Along with ongoing symptoms, children with PPCSs may struggle with declines in academic performance and behavior changes, 8 further exacerbating the negative effects of concussion in pediatric patients.
Many demographic factors are related to increased risk of prolonged recovery after pediatric concussion, including sex,9,10 age, 11 prior concussion history, 7 and migraine disorders. 12 Depression and anxiety disorders often emerge during adolescence 13 and, as more than 30% of adolescents are affected by anxiety disorders globally, 13 there is growing interest into the effect of preexisting mental health disorders on concussion recovery. Children with preexisting anxiety disorders have increased symptoms acutely, take longer to reach symptom resolution, and experience protracted return to school and physical activity compared to children without preexisting anxiety.3,14 Further studies also suggest that anxiety and depression disorders lengthen pediatric concussion recovery times, taking 2 (anxiety) and 2.2 (depression) times longer to recover from concussion respectively. 15 However, the literature is somewhat mixed, as other studies report no association between mental health disorders and prolonged recovery in children injured through sport-related mechanisms.16,17 Thus, the current findings regarding the effect of preexisting mental health conditions on concussion recovery are inconsistent.
Beyond recovery time, both concussion and mental health disorders are individually associated with reduced quality of life in children. Adolescents with anxiety and depression disorders have generally worse physical and mental health than those without mental health disorders, which is related to overall poorer quality of life.18,19 Similarly, children with concussion generally report decreased quality of life up to 12 weeks after injury, 20 although quality of life impairments typically resolve once children are clinically recovered from concussion.19,21 Furthermore, mental health and quality of life may be intertwined after concussion. Concussion can increase mood-related symptoms, with the majority of children reporting ≥1 new or worsening emotional symptom after injury. 22 Thus, this increase in negative emotional symptoms specific to concussion may exacerbate preexisting mental health symptoms and contribute to the overall reduced quality of life experienced by children after injury.
Most prior studies investigating the associations between preexisting mental health conditions and concussion recovery are largely cross-sectional; thus, the association between anxiety and/or depression and longitudinal recovery trajectories over time is poorly defined.3,15,18,23,24 Furthermore, new research suggests a dose-response relationship between mental health disorders and concussion recovery. 14 This suggests that more detrimental effects are observed with additional mental health diagnoses, but this finding is yet to be confirmed in independent studies. Our objective was to determine the relationship between preexisting mental health conditions on acute clinical presentation and symptom and quality of life outcomes over time in adolescents with concussion. We hypothesize that adolescents with both preexisting depression and anxiety disorders will display worse acute clinical presentation and slowed clinical recovery trajectories over time compared to adolescents with no or one preexisting mental health condition.
Methods
Study Design and Participants
This study was a secondary analysis of data collected during the Predicting and Preventing Postconcussive Problems in Pediatrics (5P) study. The full study protocol was published previously 1 ; here we highlight only the procedures and outcomes pertinent to our analysis. The 5P study was a prospective multicenter cohort design with participants enrolled from 9 pediatric emergency departments of the Pediatric Emergency Research Canada network between August 2012 and May 2015. Children were enrolled into the 5P study if they were aged 5-17 years, diagnosed with a concussion as defined by the Zurich consensus statement, 25 presented to an associated pediatric emergency department within 48 hours of injury, and were proficient in English or French. Children were excluded if they had (1) a Glasgow Coma Scale score ≤13, (2) abnormal neuroimaging, (3) severe or multisystem injury requiring surgical intervention and/or hospital admission, (4) neurologic developmental delay, (5) intoxication at the time of presentation to the emergency department, and (6) no clear traumatic mechanism of injury. All enrolled participants and their parent/guardian provided written consent and/or assent as required by each participating institution's research ethics boards. Our study focused on adolescents aged 13-17 years from the full sample because the presence of self-reported depression, anxiety, or both disorders in younger children was too uncommon to draw meaningful conclusions.
Data Collection Procedure
Patient demographics, age-appropriate postconcussion symptom checklists, and cognitive, balance, and neck examinations were completed on enrollment at the pediatric emergency department. Follow-up visits were completed at 1, 2, 4, 8, and 12 weeks after initial study enrollment. Symptom checklists were administered at every follow-up visit, whereas the quality of life questionnaire was administered at the 4-, 8-, and 12-week follow-up visits only. Participants and their families were given the choice of completing the follow-up visits via telephone with a research assistant or through a secure online survey based on their individual preference.
Clinical Outcome Measures
Preexisting Mental Health Disorders
The Acute Concussion Evaluation (ACE) is a 26-item questionnaire that assesses children and adults with a suspected or confirmed concussion. 26 The ACE contains questions pertaining to the patient's medical history (ie, history of concussion, psychiatric conditions) and injury characteristics that are answered in a yes-or-no format. 26 The ACE captures preinjury anxiety and depression diagnoses, which were used to categorize patients into depression, anxiety, both anxiety and depression, or no preexisting anxiety or depression disorder groups. We have interpreted selecting “yes” to anxiety and/or depression on the ACE more broadly than having a definitively diagnosed mood or anxiety disorder (eg, major depressive disorder) and instead assume that a “yes” response might reflect having a “condition” or a “problem” with depression, anxiety, or both.
Sport Concussion Assessment Tool–Version 3
The Sport Concussion Assessment Tool–Version 3 (SCAT-3, the most recent version of this tool at the time of data collection) is a standardized concussion assessment tool for individuals aged 13 years or older. 27 Assessments administered from the SCAT-3 included the Standard Assessment of Concussion (SAC), a modified version of Balance Error Scoring System (BESS), and a neck examination. The SAC is a brief cognitive examination that measures orientation, immediate and delayed memory, and concentration, resulting in a total score from 0 to 30 (higher scores indicating better cognition). The modified BESS assessed balance in double-leg and tandem stance positions. 27 The number of errors during each stance was recorded with a maximum of 10 errors per position (higher score indicating worse performance). 27 The neck examination determined cervical spine strength, tenderness, and range of motion, which were rated as present or not present.
Symptom Reporting and Presence of Persistent Postconcussion Symptoms
The Post-Concussion Symptom Inventory (PCSI) is considered to be a reliable and valid concussion symptom checklist designed for pediatric patients and/or their parents.26,28 The PCSI version for adolescents contains 26 items on a 7-point scale (0 [not present] to 6 [present and severe]). Adolescents rated their symptoms twice: once to retrospectively report their preinjury symptoms and once to rate their current postconcussion symptoms over the past 24 hours. 26 The total symptom change score (postinjury symptom total minus preinjury symptom total) was calculated for each patient. The PCSI was also used to determine the presence (yes/no) of PPCS, which was defined as 3 new or worsening symptoms compared with preinjury symptoms at the 4-week follow-up assessment in alignment with the original 5P study.
Quality of Life
The Pediatric Quality of Life (PedsQL) is a 23-item questionnaire that measures quality of life in children. 29 The PedsQL is considered reliable and valid in children 29 and has shown good internal consistency and test-retest reliability among children with concussion. 30 The PedsQL includes situations regarding physical, emotional, social, and academic domains. Children were asked to rate problems on a 5-point scale (0-4), from 0 (never) to 2 (sometimes) to 4 (almost always). 29 An average quality of life score from 0 to 100 is calculated, with higher scores indicating increased quality of life.
Statistical Analysis
The data were analyzed in SAS (version 9.4; SAS Institute, Inc), with associated visualizations created in RStudio using the ggplot2 package. 31 Descriptive statistics including means (with SD) or frequencies (with percentages) are reported for each variable. The main independent variable was group (anxiety only, depression only, anxiety and depression, or no preexisting mental health diagnoses). Analysis of variance (continuous) or χ2 (categorical) tests examined differences in patient demographics and acute clinical outcomes collected at the initial visit. To examine pairwise comparisons, Tukey post hoc analyses were performed for all analyses of variance with significant main effects. Mixed linear models determined the effects of preexisting mental health conditions, time, and their interaction on symptom and quality of life outcomes. Logistic regressions evaluated the association between preexisting mental health diagnoses and the presence of PPCS (yes/no) at the 4-week postconcussion visit only. Univariate and multivariable models were run for both mixed linear and logistic regression models. Multivariable models controlled for age, sex, preexisting migraine history, concussion history (previous concussion with symptoms lasting ≥1 week), learning disability, and BESS tandem stance score. These variables were selected as covariates because they were previously shown to be related to PPCS in this data set. 5
Results
A total of 1245 participants aged 13-17 years enrolled into the 5P study. Seven participants had missing mental health diagnosis data; thus, 1238 participants were included in this secondary analysis. Most participants (n = 1070, 86.4%) did not self-report a preexisting depression or anxiety disorder, whereas the remaining participants reported having anxiety only (n = 95, 7.7%), depression only (n = 25, 2.0%), or both depression and anxiety (n = 48, 3.9%). Adolescents with 1 or more preexisting mental health diagnosis were slightly older, more likely to be female, and more likely to have a prior history of concussion. In addition, adolescents with 1 or more preexisting mental health diagnosis were more likely to have other preexisting conditions, including attention deficit/hyperactivity disorder, developmental disorders, learning disabilities, migraine disorders, sleep disorders, and other psychiatric conditions. Detailed information about patient demographics can be found in Table 1.
Participant Demographics Presented Overall and Separately for Each Preexisting Mental Health Group.a
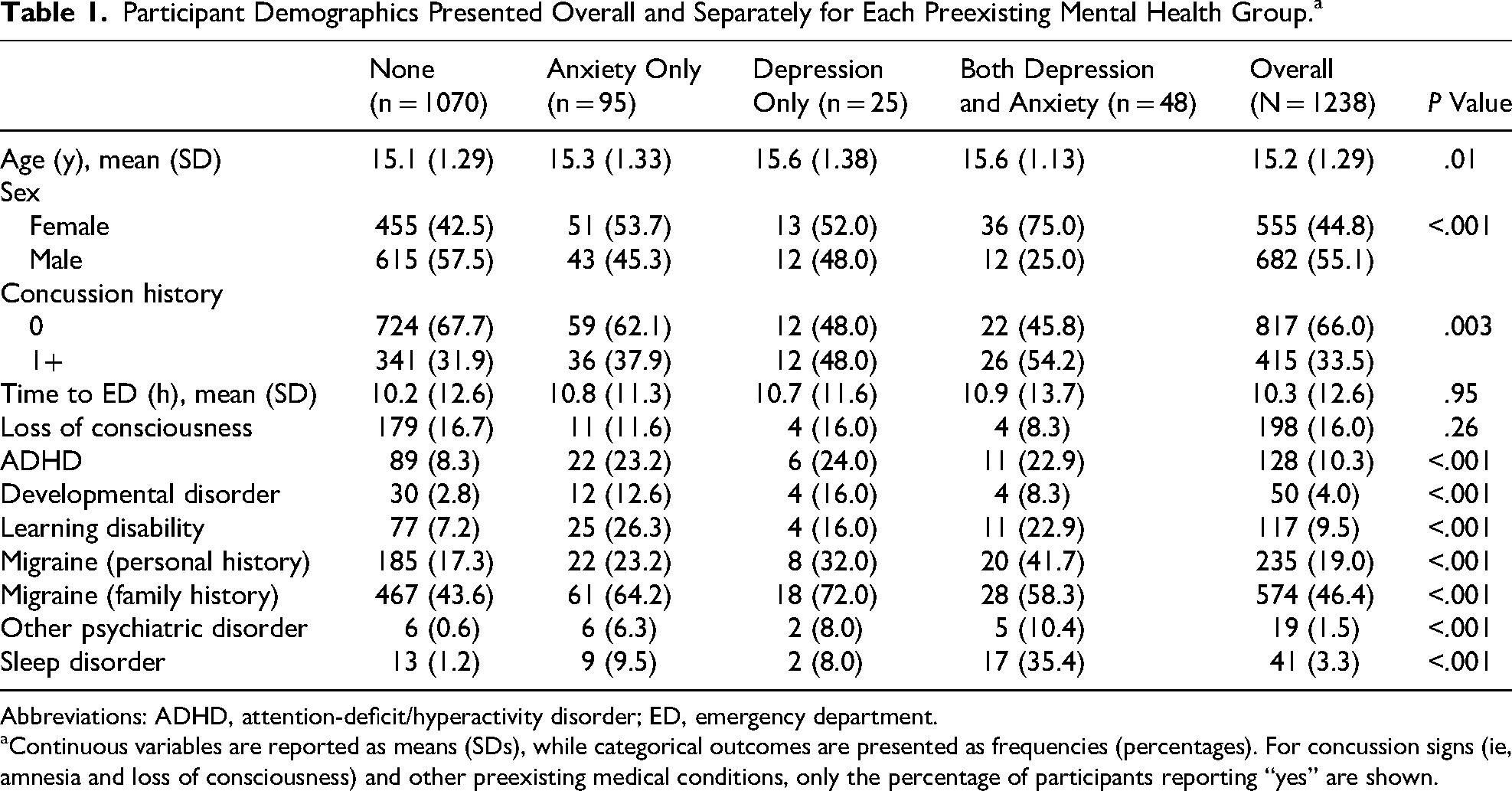
Abbreviations: ADHD, attention-deficit/hyperactivity disorder; ED, emergency department.
Continuous variables are reported as means (SDs), while categorical outcomes are presented as frequencies (percentages). For concussion signs (ie, amnesia and loss of consciousness) and other preexisting medical conditions, only the percentage of participants reporting “yes” are shown.
Acute Symptom Presentation Minimally Differs Between Preexisting Mental Health Groups
A significant group difference was observed for the acute patient-reported symptom change score captured in the emergency department (F(3,1214) = 3.01, P = .03). Although the depression only and combined anxiety/depression groups reported the highest mean symptom scores, Tukey post hoc testing revealed no significant pairwise differences. No differences were observed for any other clinical outcomes (ie, parent reported PCSI, SAC, BESS, or cervical spine assessment) collected in the emergency department within 48 hours of injury. Detailed information about acute clinical outcomes is found in Table 2.
Acute Clinical Postconcussion Outcomes Presented Overall and Separately for Each Preexisting Mental Health Group.a
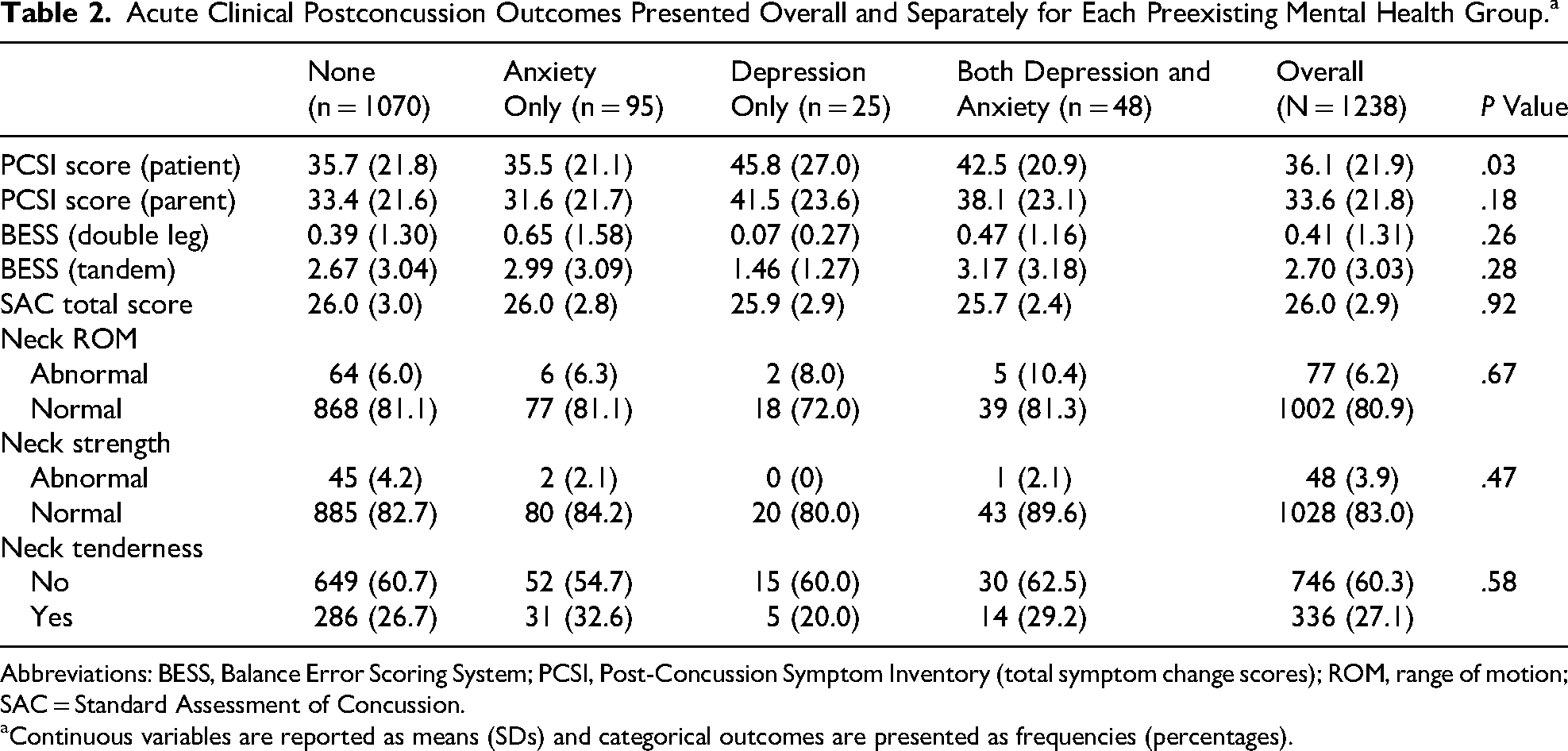
Abbreviations: BESS, Balance Error Scoring System; PCSI, Post-Concussion Symptom Inventory (total symptom change scores); ROM, range of motion; SAC = Standard Assessment of Concussion.
Continuous variables are reported as means (SDs) and categorical outcomes are presented as frequencies (percentages).
PCSI Total Symptom Change and PedsQL Total Scores (Means and SDs) Presented Separately for Each Preexisting Mental Health Group Across Study Visits.a
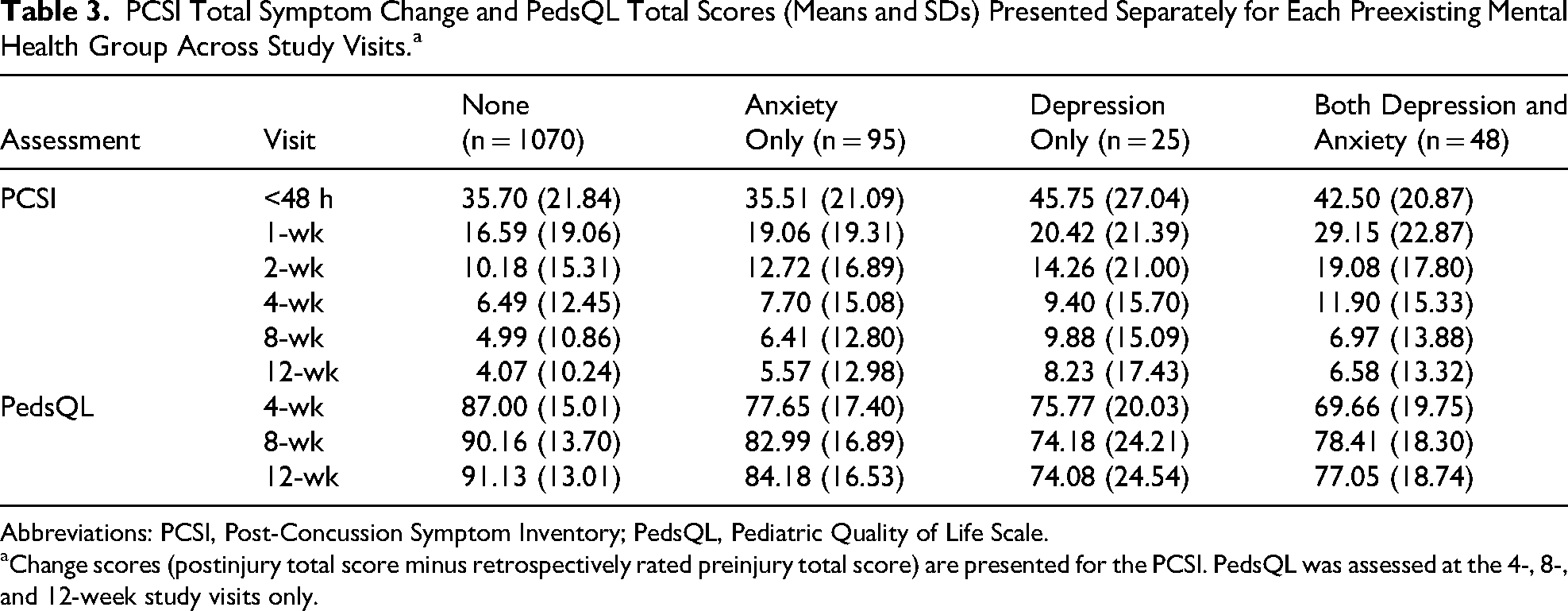
Abbreviations: PCSI, Post-Concussion Symptom Inventory; PedsQL, Pediatric Quality of Life Scale.
Change scores (postinjury total score minus retrospectively rated preinjury total score) are presented for the PCSI. PedsQL was assessed at the 4-, 8-, and 12-week study visits only.
Preexisting Mental Health Conditions Are Associated With Clinical Symptom Scores
Univariate models revealed significant main effects of mental health group (F(3,22) = 11.43, P = .0001) and time (F(1,6197) = 248.63, P < .0001) on total symptom change scores, but interaction effects were not significant (P = .14, Figure 1). The depression-only group (t = 2.38, P = .027) and combined anxiety/depression group (t = 5.40, P < .0001) reported higher total symptom change scores than adolescents with no preexisting mental health conditions. However, for all groups, total symptom change scores generally decreased over time. Main effects of mental health group (F(3,22) = 3.96, P = .02) and time (F(1,6191) = 272.82, P < .0001) were retained in the multivariable model controlling for age, sex, preexisting migraine history, concussion history, learning disability, and BESS tandem stance score. However, only the combined depression and anxiety group (t = 2.97, P = .007) had higher total symptom change scores than the no preexisting mental health conditions group when controlling for other covariates. Total symptom change scores for each mental health group at each study visit can be found in Table 3.
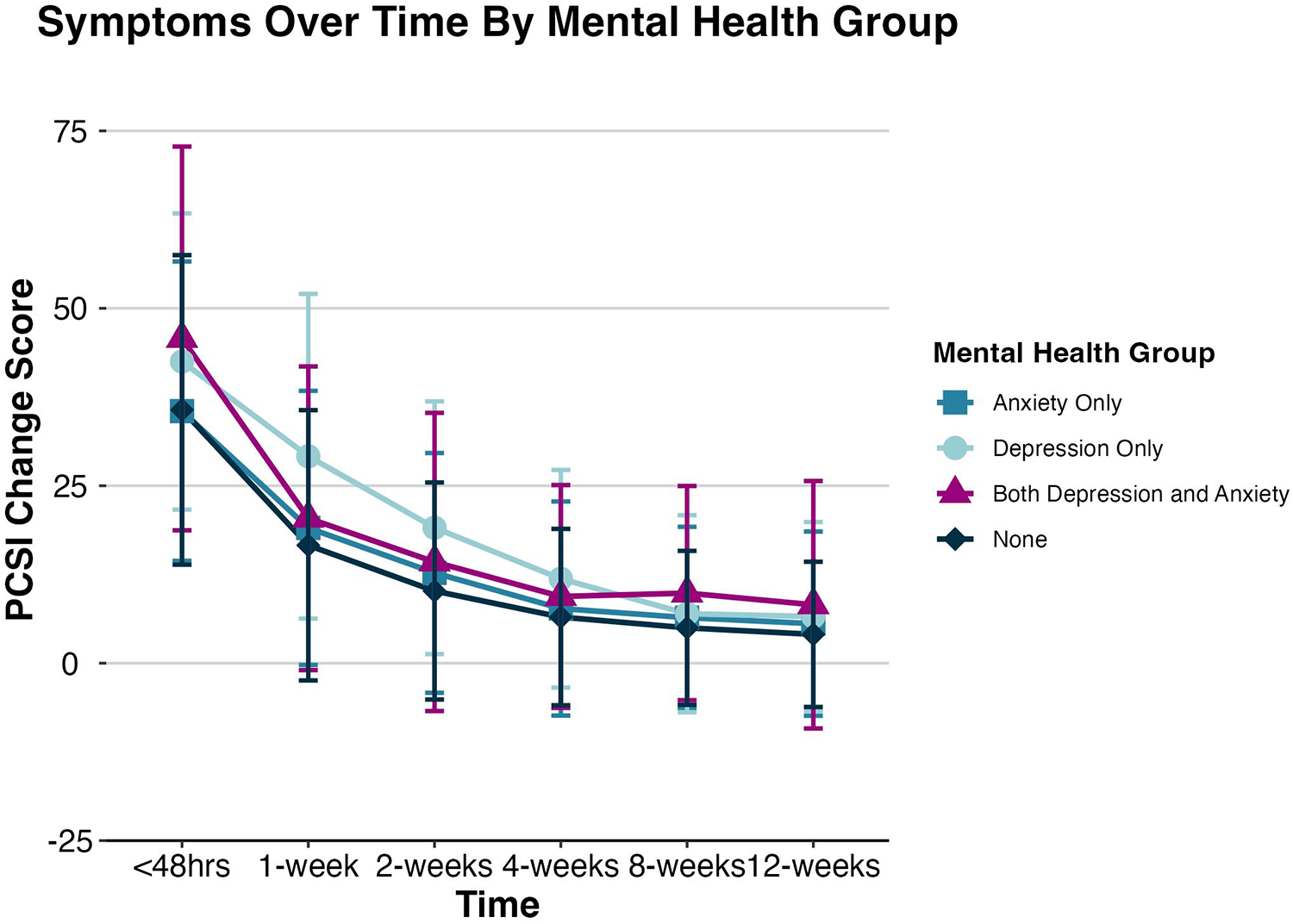
The trajectory of PCSI total symptom change scores separately for each preexisting mental health group across all study visits. The mean change scores represent the average postinjury total score minus the retrospectively rated mean preinjury total score for each group; error bars represent the SD. PCSI, Post-Concussion Symptom Inventory.
For quality of life outcomes, univariate models revealed similar effects of mental health group (F(3,22) = 31.96, P < .0001) and time (F(1,2833) = 13.53, P = .0002). The anxiety only group (t = −5.95, P < .0001), the depression only group (t = −7.53, P = .0001), and the combined anxiety and depression group (t = −3.43, P < .0024) all reported lower quality of life scores compared with adolescents reporting no preexisting mental health conditions (Figure 2). Regardless of group assignment, quality of life scores generally improved over time after concussion. Main effects of mental health group (F(3,22) = 18.51, P < .0001) and time (F(1,2627) = 15.56, P < .0001) were retained in the multivariable model. All 3 mental health groups (Anxiety: t = −4.71, P = .0001; Depression: t = −3.03, P = .006; Combined: t = −5.49, P < .0001) continued to show lower quality of life scores compared with the comparison group even when controlling for additional factors known to influence concussion recovery. Overall, recovery trajectories appear similar between preexisting mental health groups, but total symptom change scores were higher and quality of life scores were lower in the combined anxiety/depression group. Quality of life scores for each mental health group at each study visit can be found in Table 3.
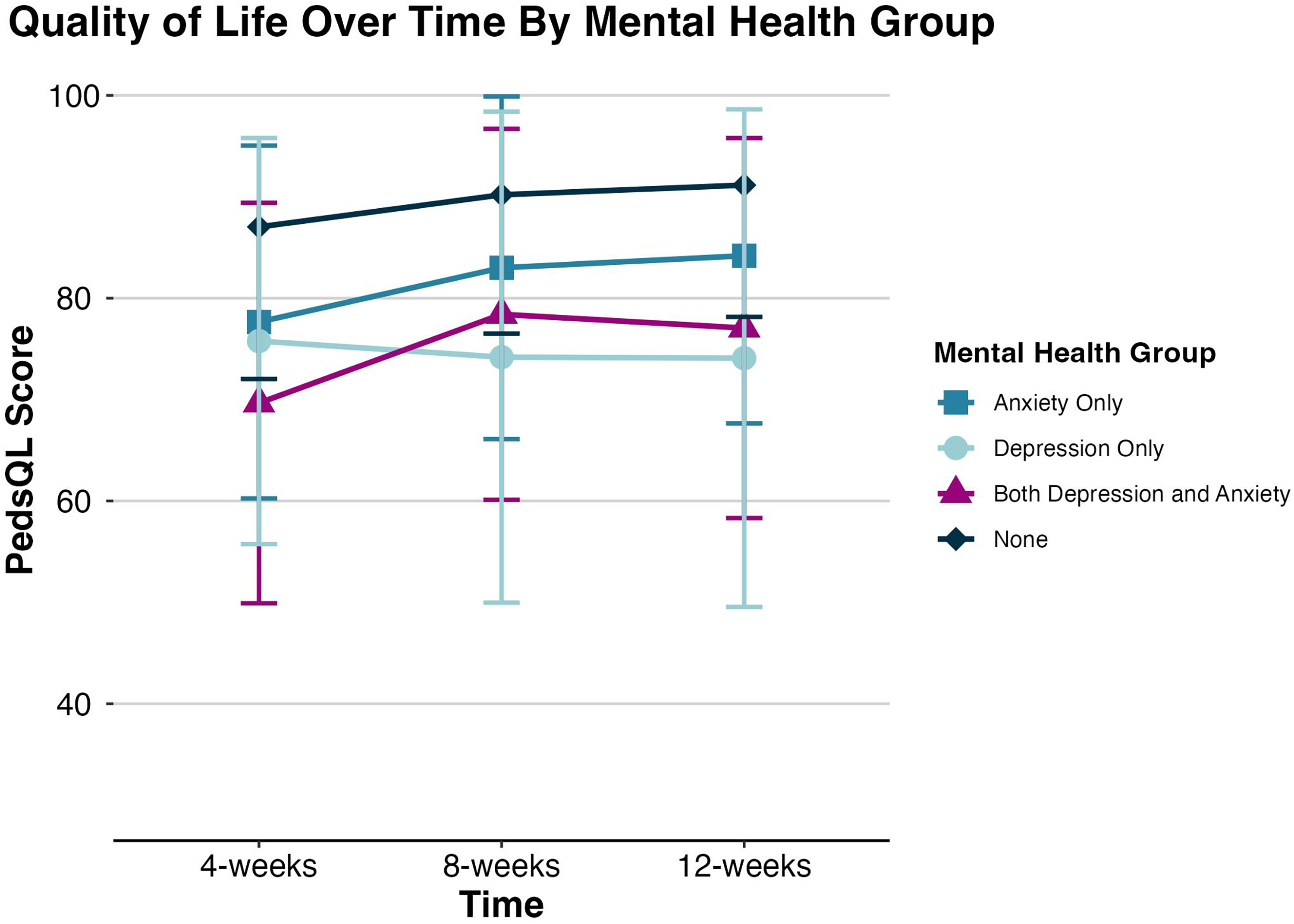
The trajectory of PedsQL scores separately for each preexisting mental health group from 4 to 12 weeks following concussion. Higher scores represent fewer symptoms and better quality of life. Mean scores are presented; error bars represent the SD. PedsQL, Pediatric Quality of Life.
PPCS Is More Common With Multiple Preexisting Mental Health Diagnoses
A total of 907 (out of 1238, 73.3%) participants completed the PCSI at the 4-week visit and were included in the PPCS analysis. Overall, 388 (42.8%) of adolescents experienced PPCS based on our study definition (ie, 3 new or worsening symptoms compared with preinjury symptoms at the 4-week follow-up assessment). The combined anxiety/depression group had the highest proportion of patients experiencing PPCS (n = 23, 62.2%), followed by the anxiety only (n = 33, 45.8%), depression only (n = 7, 43.8%), and no preexisting mental health condition groups (n = 325, 41.6%). In univariate models, the combined anxiety/depression group had significantly greater odds of experiencing PPCS compared to the control group (OR = 2.31, 95% CI = 1.18-4.67, P = .02). However, multivariable models found no significant association between preexisting mental health conditions and the presence of PPCS (P = .62). The percentages of each mental health group experiencing PPCS are shown in Figure 3.
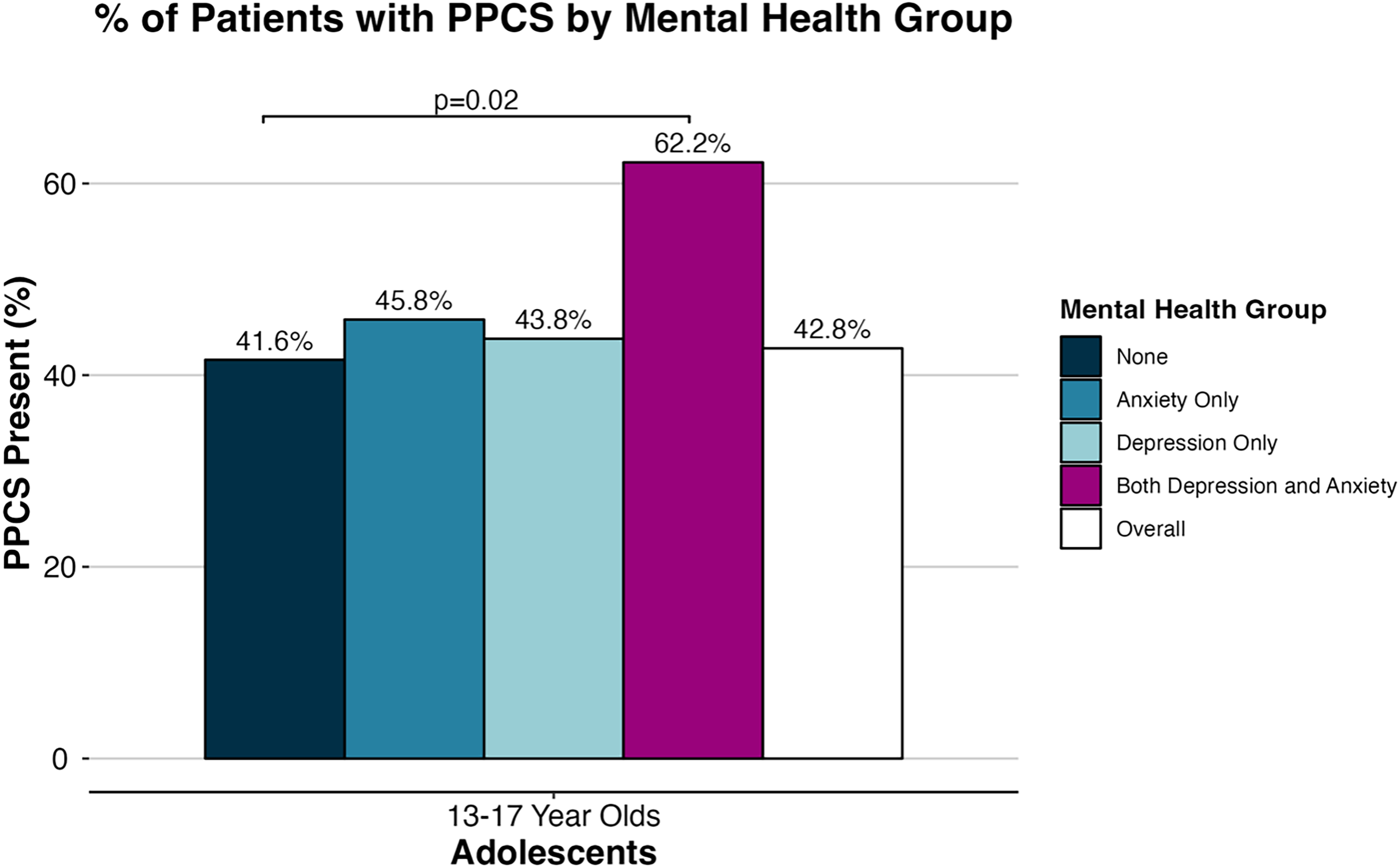
Percentages with PPCS presented overall and separately for each preexisting mental health group, highlighting the statistically significant difference between the comparison and the preexisting depression and anxiety groups present in univariate analyses. PPCS, persistent postconcussion symptoms.
Discussion
Adolescents with combined preinjury anxiety and depression diagnoses reported worse clinical outcomes following concussion despite recovering along similar trajectories. In other words, the rate of improvement in clinical outcomes over time was similar for all groups, but individuals with combined preinjury mental health diagnoses reported more symptoms and lower quality of life overall than patients with individual preinjury anxiety or depression diagnoses or no mental health diagnoses altogether. This indicates a subtle but important association between preexisting mental health conditions and clinical recovery trajectories after pediatric concussion. This generally aligns with Master et al's findings illustrating that children and adolescents with ≥3 mental health diagnoses had longer recoveries (average 38 days) than children with 1 (27 days) or 2 (32 days) preexisting mental health diagnoses. 14 Although some studies suggest that preexisting anxiety and depression are individually associated with prolonged recovery after concussion,3,15 others find no associations. 16 These inconsistencies, along with our results and those from Master et al, 14 suggest that anxiety and depression in combination may be associated with worse concussion recovery than each condition individually.
For acute clinical outcomes captured in the emergency department, only patient-reported symptom scores significantly differed based on the mental health group. Although the depression only and combined anxiety/depression groups reported the highest average symptom scores, no significant pairwise comparisons were observed. Previous literature is inconsistent regarding the association between preexisting mental health and acute postinjury symptom scores, with some studies suggesting greater3,23 symptom severity acutely following concussion in adolescents with preexisting anxiety or depression and other studies suggesting no such differences exist.24,32 Additional factors, such as biological sex, may also play an important role in acute clinical presentation regardless of preexisting mental health conditions. Females report higher symptom scores, potentially because of increased willingness to disclose postinjury problems and greater care-seeking behaviors,33,34 and have higher rates of anxiety and depression than men. 3 Because all 3 mental health groups had higher proportions of females compared with the control group, this may be an important moderator in the relationship between preexisting mental health conditions and symptom presentation after concussion. No significant group differences were observed for any other acute clinical outcome in our study. This is consistent with previous literature reporting no significant differences in SAC scores and BESS scores between individuals with and without preexisting mental health conditions. 32
Although the combined anxiety/depression group reported more symptoms overall, symptom trajectories over time were similar between mental health groups. Many prior studies reporting an association between preexisting mental health conditions and longer clinical recovery recruited patients from specialty clinics, which may suggest that these participants had worse clinical problems predisposing them to prolonged symptomology.3,15 Studies recruiting acutely from pediatric emergency departments similarly found that children with preexisting mental health conditions had slower recovery of neurophysiological function 35 and represent a distinct clinical phenotype 36 than concussed children with no preexisting mental health complaints. Patients in the 5P study were recruited from pediatric emergency departments within 48 hours of injury and may have experienced milder symptoms and clinical deficits that were more likely to resolve naturally. Receiving care within 2 days of injury can improve recovery outcomes37,38 and prior emergency department–based studies investigated a combination preexisting conditions (ie, sleep disorders, migraines) in conjunction with anxiety and depression,35,36 which may also explain why the adolescents in our sample had similar longitudinal trajectories regardless of group. Still, pediatric concussion recovery appears to be influenced by a variety of preexisting and injury-related variables; the association between preexisting mental health and longitudinal concussion recovery remains mixed and in need of further investigation.
Quality of life improved over time in all groups but children with preexisting mental health conditions, individual or combined. Although trajectories were similar, children with preexisting mental health conditions continued to report lower quality of life scores relative to the comparison group across the 12-week follow-up period. Children with mental health conditions generally report lower quality of life compared to children without mental health conditions,18,39 which is consistent with our results. The combined anxiety/depression group had significantly greater odds of experiencing PPCS compared with the control group in univariate analyses, but these results did not remain significant in the multivariable model similar to the original 5P study. 5 This suggests that preexisting mental health conditions alone might not predispose adolescents to PPCS, which is inconsistent with prior literature.3,15 However, most (∼2/3) of the combined depression anxiety group developed PPCS, whereas the proportion of patients with PPCS in the anxiety only, depression only, or no mental health diagnoses was approximately 40%. The cell sizes in the PPCS analysis were smaller, particularly within each respective mental health group, which may be contributing to the lack of statistical significance observed in the multivariable model. Additionally, it is possible that previous studies did not control for possible modifiers of concussion recovery (eg, age, sex, concussion, and history) in their analyses, which would align with our univariate results suggesting that the combined mental health group was associated with greater odds of experiencing PPCS.
Strengths
This study investigates the associations between preinjury depression and anxiety diagnoses, individually and combined, and postconcussion recovery outcomes. Although anxiety and depression diagnoses frequently co-occur (ie, they are often comorbid), 40 their combined associations with concussion recovery trajectories are rarely investigated. Middle adolescence (13-17 years) is a period of dynamic neurodevelopment and common time for mental health conditions to present; thus, it is important to investigate the effects of brain injury during this clinically important window of time. The PCSI was used to assess symptoms in this study, and this scale is unique because it includes both preinjury and postconcussion symptom reporting. 41 Concussion-like symptoms are nonspecific, and children and adolescents with preexisting depression and anxiety are known to endorse many of these symptoms in the absence of concussion.3,42 By using a change score (ie, postinjury minus preinjury ratings), our analyses account for presumed dispositional preexisting symptoms and are more focused on the new or increased symptomology associated with the concussion. This study investigated longitudinal trajectories over a 3-month period, extending prior literature that are predominantly cross-sectional in nature. Finally, this study includes a large sample size recruited through 9 different pediatric emergency departments across Canada, greatly increasing the ability to generalize findings to broader adolescent concussion populations.
Limitations
Participants were only evaluated by a health care provider at study enrollment; although symptom reports and quality of life measures were recorded throughout the study, we are unable to establish if and when true clinical recovery occurred for patients. Participants self-reported their mental health diagnoses, which were not confirmed through medical records or other methods. It is possible that individuals without a formal diagnosis may have self-reported a preexisting mental health disorder based on their own feelings or symptoms. Treatment (eg, medication, therapy) for preexisting mental health conditions was not captured in this data set; how this may affect clinical presentation and recovery after concussion remains unknown. Conversely, there may also have been adolescents with clinically significant levels of depression and/or anxiety who have not yet received a formal diagnosis (ie, lack of access to care, or stigma around mental health) and were, therefore, incorrectly included in our comparison group. Although our overall sample size was large, the mental health groups were small because of the relatively low percentage of adolescents with anxiety and/or depression diagnoses. However, our mental health groups were comparable in size to previous studies.14,24,40 No specific treatment or recovery guidelines were provided as part of the 5P study. However, participants may have received recovery recommendations from their emergency department physician or from other health care professionals outside of the study. Furthermore, best practice clinical care for pediatric concussion evolved throughout the 5P study period. As such, any outside treatments may have modulated clinical recovery trajectories but cannot be accounted for as they were not provided or captured in this study.
Clinical Significance
Our results suggest that adolescents with combined preinjury anxiety and depression diagnoses have higher symptom scores and worse quality of life compared to adolescents with no preexisting mental health conditions. Thus, the presence of preexisting mental health conditions is an important factor for clinicians to consider when diagnosing and managing adolescents with concussion and health care providers are encouraged to collect history of mental health disorders as part of their clinical intake procedures. Adolescents with preexisting mental health conditions report higher symptoms scores in the absence of injury.3,42 Thus, clinicians are encouraged to consider carefully preinjury temperamental, personality, neurodevelopmental, 43 health, 44 and mental health 42 factors that might be associated with how an adolescent conceptualizes, experiences, and reports symptoms in the days, weeks, and months following a concussion. Individuals with preexisting mental health conditions who have a high level of symptoms for more than 2 weeks following concussion may benefit from referral to a mental health provider, which may help with both preinjury problems and increases in emotional symptoms that can occur following concussion. 45 Regardless of preexisting health conditions, clinicians should consider referrals to interdisciplinary concussion specialists or other health care providers for adolescents at higher risk for persisting symptoms and for adolescents whose symptoms have not resolved within 2-4 weeks after injury. 45
Conclusions
Adolescents with combined preinjury anxiety and depression diagnoses endorse more concussion symptoms and present with worse quality of life than individuals with no preexisting mental health conditions. Given that mental health disorders, such as depression and anxiety, are frequently comorbid in adolescents, future studies should continue investigating youth with a combination of mental health disorders and their concussion outcomes. Almost 2 of 3 adolescents (62.2%) who report having a preinjury diagnosis of both depression and anxiety experience persistent symptoms 1 or more months following a concussion. Therefore, these adolescents with a personal history of depression and anxiety may benefit from early referral to concussion specialty clinics and/or health care professional specialized in psychosocial interventions to improve clinical recovery outcomes.
Footnotes
Acknowledgments
We would like to acknowledge the individuals and organizations that collected the original data and facilitated the open sharing of these data used for this research including the Ontario Brain Institute, the Brain-CODE platform, the Government of Ontario, and the Pediatric Emergency Research Canada (PERC) 5P study investigators, research team, and study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is a secondary analysis of data collected in the Predicting and Preventing Postconcussive Problems in Pediatrics (5P) study. The original 5P study was funded through the Canadian Institutes of Health Research (operating grant 126197, planning grant 119829) and the Canadian Institutes of Health Research–Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team (TM1: 127047). Grant L. Iverson acknowledges unrestricted philanthropic support from the Mooney-Reed Charitable Foundation, Heinz Family Foundation, Boston Bolts, ImPACT Applications, Inc, National Rugby League, and the Schoen Adams Research Institute at Spaulding Rehabilitation. Roger Zemek's program of research has received financial support through competitively funded research grants from Canadian Institutes of Health Research, Ontario Neurotrauma Foundation, Physician Services Incorporated Foundation, CHEO Foundation, University of Ottawa Brain and Mind Research Institute, Ontario Brain Institute, National Football League, Ontario Ministry of Health, Public Health Agency of Canada, Health Canada, Parachute Canada, and Ontario SPOR Support Unit. He is supported by a Tier 1 Clinical Research Chair in Pediatric Concussion from the University of Ottawa. All grant funding goes directly to the institution. There is no direct funding related to the secondary analysis presented in this manuscript. The above entities were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Grant L. Iverson has a clinical practice in forensic neuropsychology, including expert testimony involving individuals with mild TBIs. He has received research support from the Harvard Integrated Program to Protect and Improve the Health of NFLPA Members, and a grant from the National Football League. He serves or has served as a scientific advisor for NanoDx, Sway Medical, Inc, and Highmark, Inc. Nathan E. Cook has a clinical practice in forensic neuropsychology, including expert testimony involving individuals with mild TBIs. Roger Zemek sits on the board of directors for North American Brain Injury Society (NABIS), which is a volunteer (unpaid) role. He is a founding partner and a minority shareholder of 360 Concussion Care (a learning health system and network of interdisciplinary concussion clinics in Ontario); no proceeds have been transferred to him.