
Abstract
Transition of care (TOC) poses challenges across medical subspecialties, each with distinct patient needs. Understanding patient and caregiver awareness and readiness within specific patient populations is essential for developing effective population-specific TOC programs. Limited data exist describing TOC readiness in patients with neuroimmune disorders. We conducted a cross-sectional survey on youth with neuroimmune disorders and their caregivers assessing TOC readiness, challenges, and support needs. Thirty-one participants completed the survey (39% Hispanic, 29% Caucasian, 19% African American). Respondents with MOG antibody-associated disease (29%), multiple sclerosis (26%), and anti–N-methyl-
Introduction
Transition of care (TOC) is not simply transfer of care, but rather an intricate process to educate and prepare children, their families, and providers for the shift from pediatric to adult health care systems.1,2 Successful TOC requires early awareness, focused education, preparation, and clear communication among all parties to prevent medical care disruption and minimize adverse health outcomes. Each year in the United States, more than 500 000 children leave pediatric care to transition to adult care, yet less than half of these children receive the necessary transition support.3,4 Efforts within neurology have been made to improve the TOC process, with the American Academy of Neurology (AAN) issuing a consensus statement endorsing a stepwise approach to TOC centered around 8 common principles of transition in child neurology and through the creation of TOC models within child neurology.5–7 Despite these efforts to address and eliminate lapses in care, many barriers to successful transition persist. Moreover, advances in life-prolonging therapies have increased the number of children with complex neurologic conditions surviving into adulthood, thereby heightening the need for adult neurologists experienced in pediatric-onset disorders.
Patients with neuroimmune disorders represent a significant and growing portion of this population, yet few studies have examined TOC readiness, barriers, or facilitators within this group. Disorders such as multiple sclerosis, myelin oligodendrocyte glycoprotein antibody–associated disease, neuromyelitis optica spectrum disorder, and autoimmune encephalitis present unique clinical features and therapeutic challenges that may not be adequately addressed by current TOC models developed for other neurologic conditions such as epilepsy or neuromuscular disease.8,9
Given these differences, it is essential to understand transition perceptions and preparedness in this population. Here we surveyed youth with neuroimmune disorders and their caregivers to characterize transition readiness, identify perceived barriers and facilitators, and inform the design of future transition programs tailored to their specific needs.
Methods
Study Design and Setting
We conducted a cross-sectional descriptive survey between April 2024 and August 2025 in a pediatric neuroimmunology clinic at Dell Children's Medical Center in Austin, Texas. Surveys were administered prior to routine clinical visits via iPad. The study was approved by the institutional review board.
Participants
Eligible participants included patients aged 10-21 years with a diagnosed neuroimmune disorder and their caregivers. Diagnosis of a neuroimmune disorder was confirmed by a pediatric neuroimmunologist and the most up-to-date published diagnostic criteria.10–14 Patients with significant cognitive impairment precluding survey participation were excluded. A total of 31 patient-caregiver dyads were enrolled and completed the survey. Consent was obtained before survey administration.
Survey Instrument
The surveys (Supplementary Files 1 and 2) assessed patient and caregiver understanding of transition of care concepts, perceived readiness, health care navigation skills, and resource needs. The survey was developed using established transition of care frameworks, including the Transition Readiness Assessment Questionnaire (TRAQ) 15 and published TOC principles endorsed by the American Academy of Neurology. 5 These resources guided the selection of domains related to transition awareness, readiness skills, health care navigation, and perceived barriers and facilitators relevant to pediatric neuroimmunology. There are currently no validated TOC instruments for this specific population. Therefore, items were modified to reflect the unique features of neuroimmune disorders while retaining alignment with standard TOC concepts. Items were reviewed by a neuroimmunologist trained in pediatric and adult neuroimmunology to ensure content was relevant and clear. Formal content validity procedures and structured cognitive interviewing were not performed. The survey consisted of mostly fixed-choice response options, and free-text responses were limited. The survey was offered in both English and Spanish through REDCap and Spanish-speaking families were provided the Spanish language version with staff support available as needed.
For the purposes of this study and for simplicity given the age of patient respondents, “Transition of care” was defined within the survey as simply the process of switching from pediatric medical care to adult medical care. We defined “transition readiness” as the skills, knowledge, and preparation required to independently manage care within an adult system. We included items addressing emergency planning, knowledge of provider contact information, and understanding insurance changes as these components represent core readiness domains emphasized in prior transition frameworks.5,15
Data Collection and Analysis
Survey data were collected via REDCap and analyzed descriptively. Quantitative variables were summarized using means, SDs, and percentages.
Results
Participant Characteristics
Thirty-one participants (mean age 15.5 ± 2.4 years, 48% female) completed the survey. The majority of the patients were Hispanic (39%) followed by Caucasian (29%) and African American (19%) (Table 1). Diagnoses included multiple sclerosis (26%), myelin oligodendrocyte glycoprotein antibody–associated disease (29%), neuromyelitis optica spectrum disorder (6%), and N-methyl-
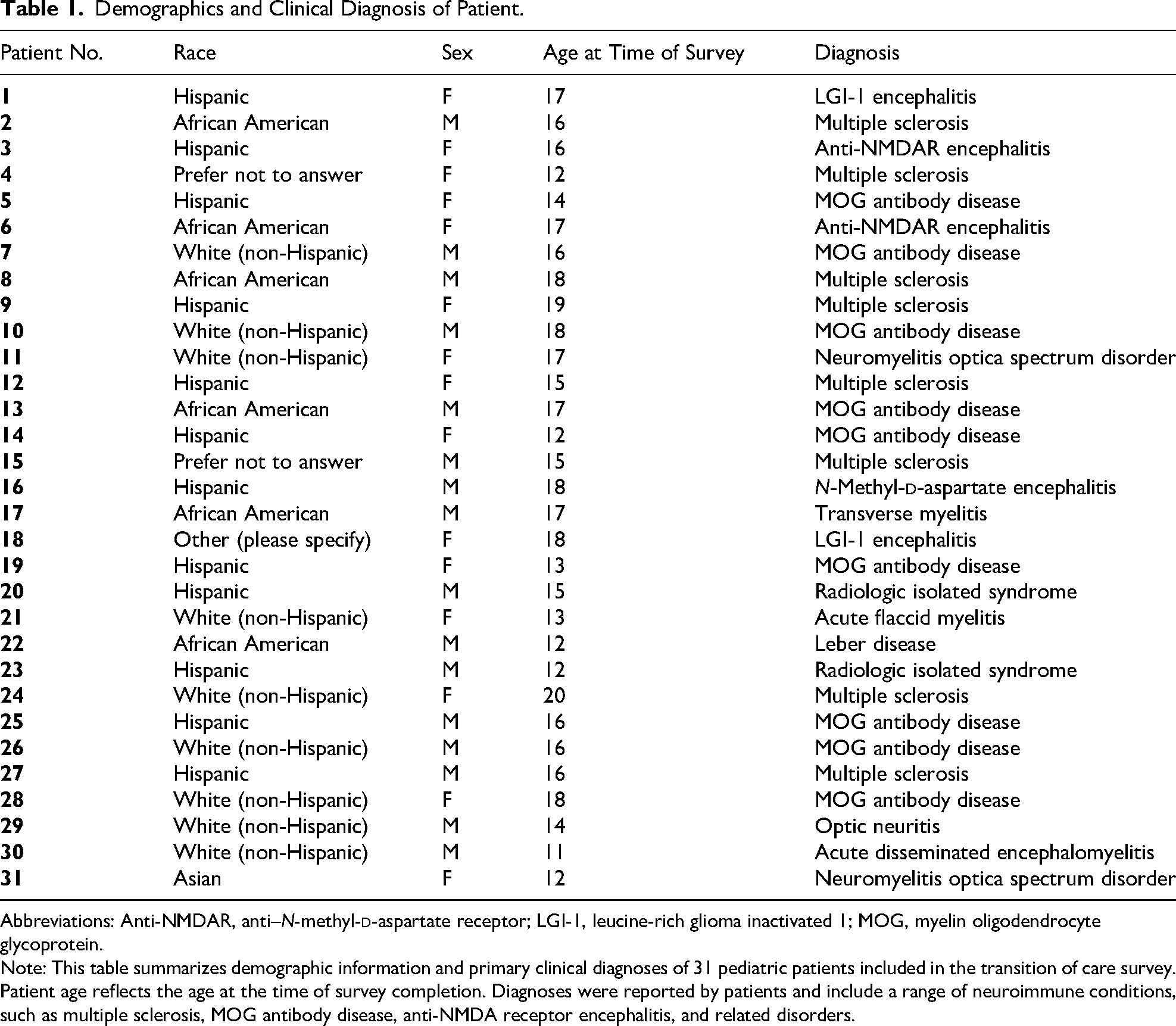
Demographics and Clinical Diagnosis of Patient.
Abbreviations: Anti-NMDAR, anti–N-methyl-
Note: This table summarizes demographic information and primary clinical diagnoses of 31 pediatric patients included in the transition of care survey. Patient age reflects the age at the time of survey completion. Diagnoses were reported by patients and include a range of neuroimmune conditions, such as multiple sclerosis, MOG antibody disease, anti-NMDA receptor encephalitis, and related disorders.
Transition Awareness and Readiness
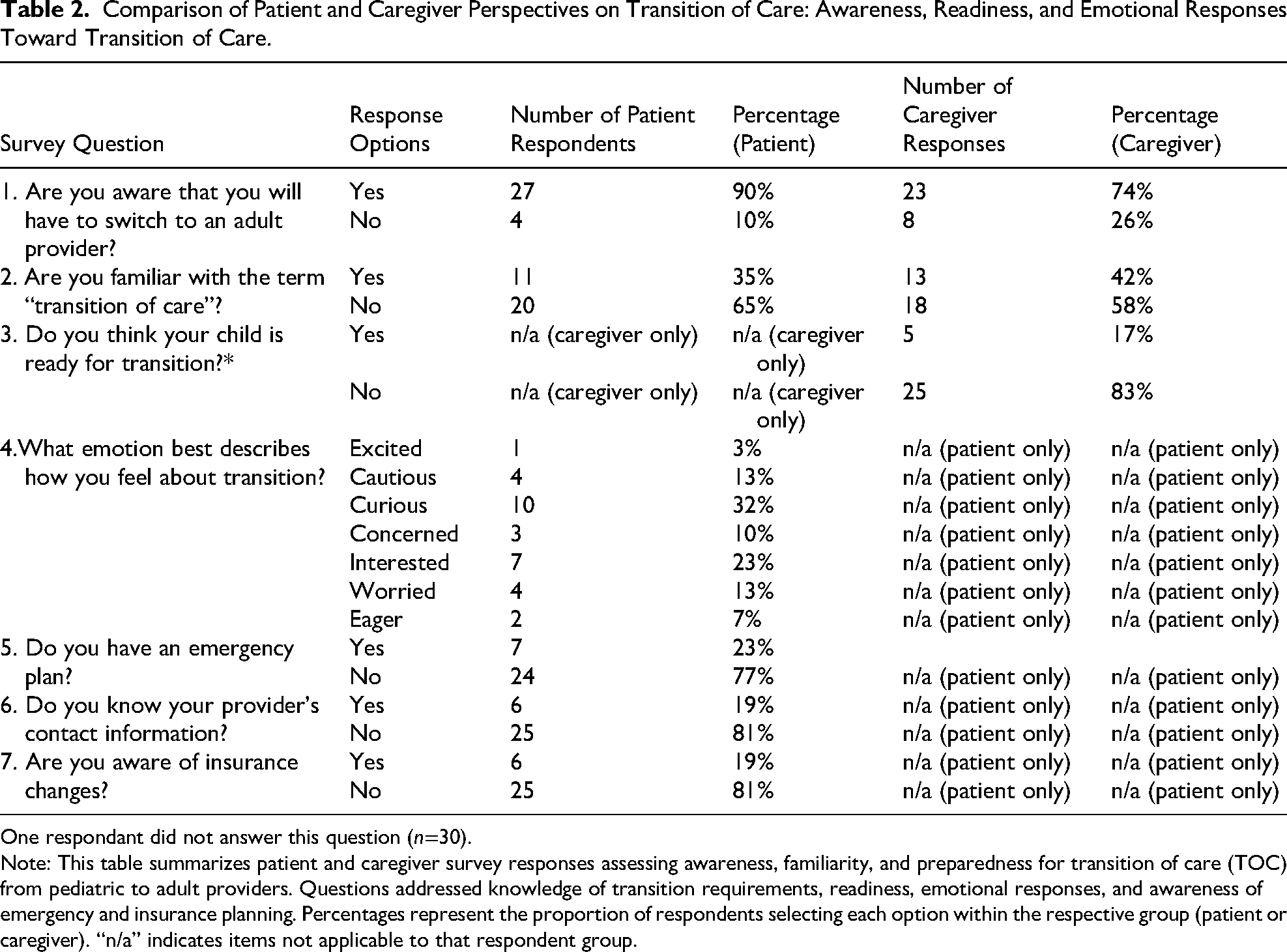
Only 35% of patients had heard of the term “transition of care”; however, 90% acknowledged they would eventually switch to an adult provider. Similarly, only 42% of caregivers reported being familiar with the term, but 74% were aware that their child would need to see an adult provider in the future. Eighty-three percent of caregivers felt that their child was not ready for transition, whereas patients’ attitudes toward transition were mixed with most patients feeling curious (32%) about the transition process. The most commonly identified readiness gaps included lack of knowledge of provider contact information (81%), lack of an emergency plan (77%), and poor understanding of insurance changes (81%) (Table 2).
Comparison of Patient and Caregiver Perspectives on Transition of Care: Awareness, Readiness, and Emotional Responses Toward Transition of Care.
One respondant did not answer this question (n=30).
Note: This table summarizes patient and caregiver survey responses assessing awareness, familiarity, and preparedness for transition of care (TOC) from pediatric to adult providers. Questions addressed knowledge of transition requirements, readiness, emotional responses, and awareness of emergency and insurance planning. Percentages represent the proportion of respondents selecting each option within the respective group (patient or caregiver). “n/a” indicates items not applicable to that respondent group.
Patient and Caregiver Concerns
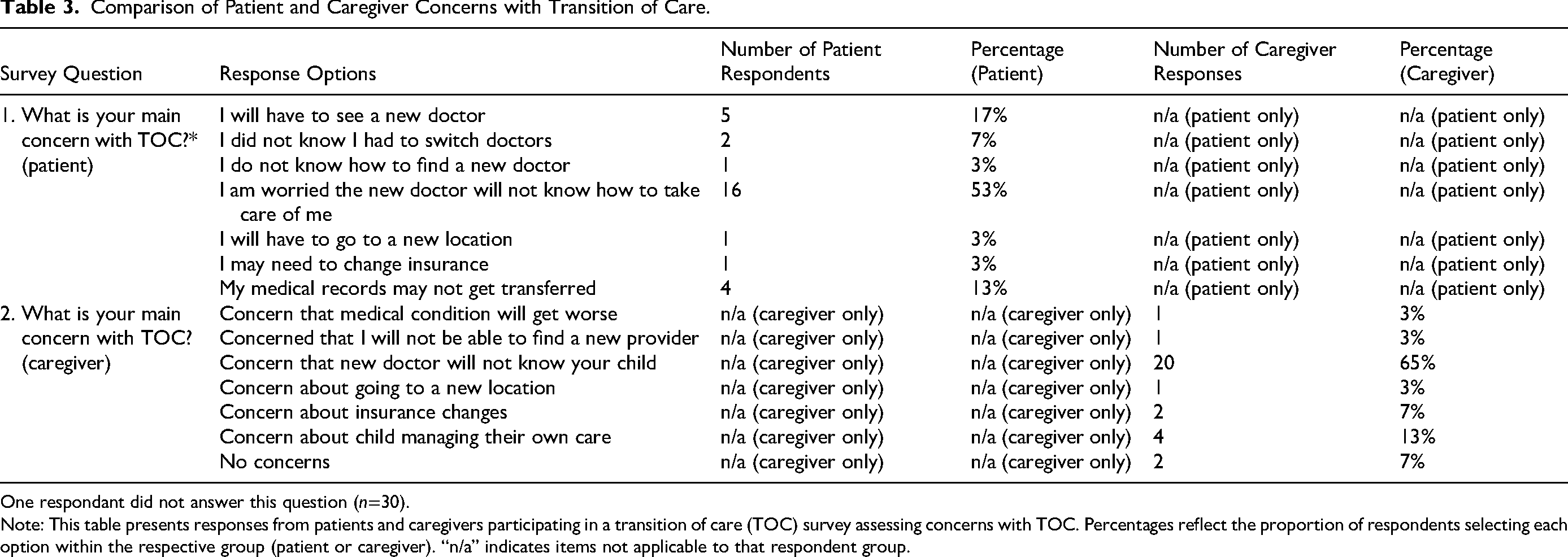
Both patients (53%) and caregivers (65%) identified fear that their new doctor would be unfamiliar with the patient and their condition as the most significant TOC challenge. Other common barriers reported by patients included having to see a new doctor (17%) and concern that medical records would not be appropriately transferred (13%) (Table 3).
Comparison of Patient and Caregiver Concerns with Transition of Care.
One respondant did not answer this question (n=30).
Note: This table presents responses from patients and caregivers participating in a transition of care (TOC) survey assessing concerns with TOC. Percentages reflect the proportion of respondents selecting each option within the respective group (patient or caregiver). “n/a” indicates items not applicable to that respondent group.
Facilitators and Supports
Patients and caregivers identified several facilitators for a successful transition. Most patients felt that an educational curriculum (35%) or a single TOC appointment (35%) would be the most helpful support (Figure 1A). Both patients (55%) and caregivers (87%) were interested in participating in a support group with other families navigating the transition process (Figure 1B). Both patients (52%) and caregivers (61%) also preferred a TOC model with a continuity provider managing care through the transition and into adulthood (Figure 1C). When asked what information new providers should know (Figure 1D), patients emphasized physical aspects of their condition (42%), followed by treatment history (32%) and cognitive/emotional aspects (13%). Caregivers emphasized physical aspects (29%), followed by diagnostic history (26%) and treatment (26%).
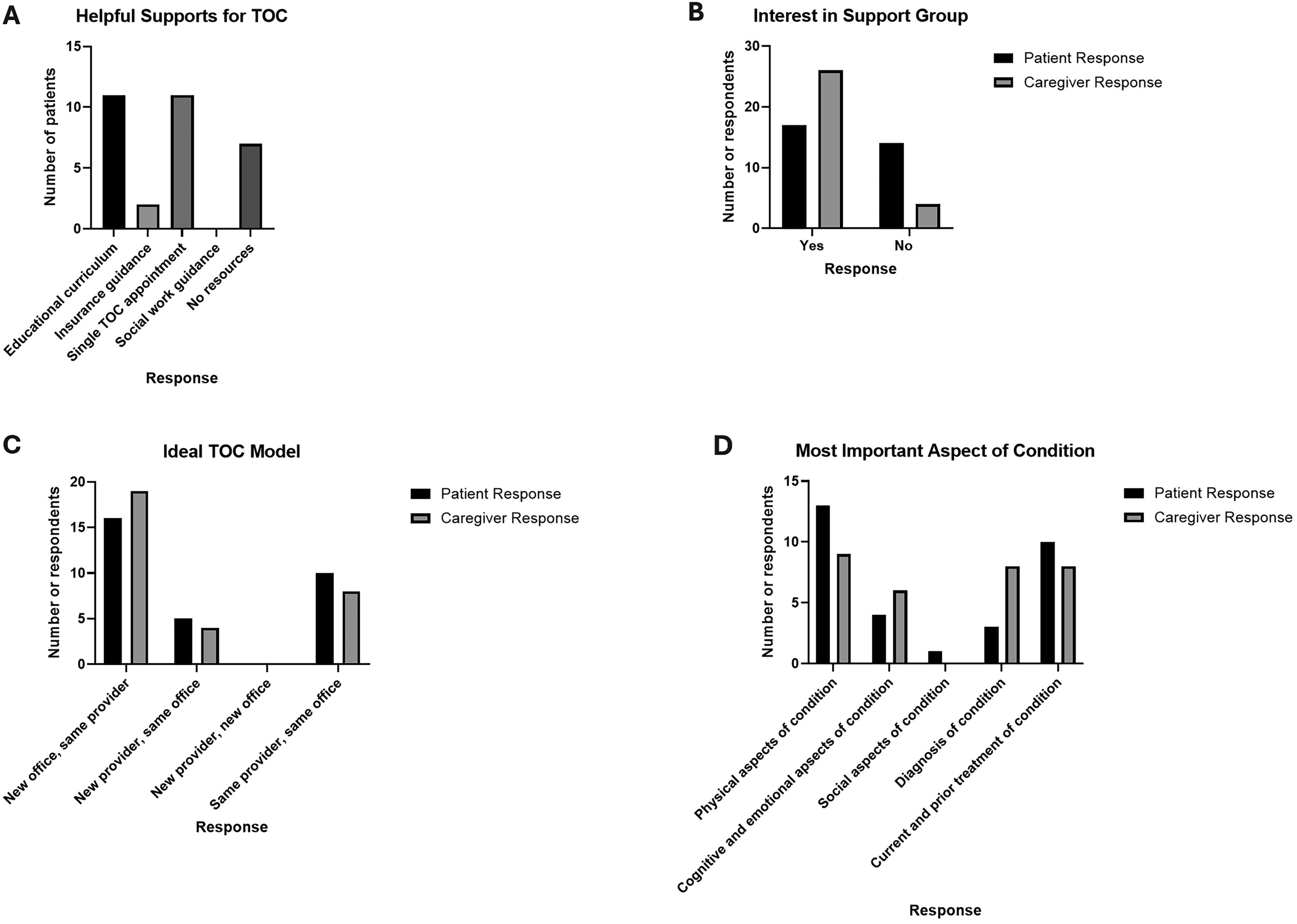
Transition of care (TOC) supports and preferred TOC model. (A) Patient-reported supports most likely to help with transition. (B) Patient and caregiver interest in participating in support groups for families navigating the TOC process. (C) Comparison of patient vs caregiver TOC model preference. (D) Most important aspects of the patient’s condition that new adult providers should understand, as identified by patients and caregivers.
Discussion
Principal Findings
To our knowledge, this is the first study to specifically explore perceptions of TOC among patients with neuroimmune disorders and their caregivers. Our study highlights key readiness gaps, transition challenges and facilitators, as well as the perceived need for a TOC model centered on a continuity provider and disease-specific education.
Transition Readiness and Barriers to a Successful Transition
Despite published guidelines on best TOC practices and online tools5,16 to support providers with transition, TOC remains a challenge for many families. Readiness assessment is a fundamental step in successful transition. Previous studies demonstrate that patients with limited self-management skills, poor disease knowledge, and inadequate emergency preparedness experience more unsuccessful transitions and worse outcomes. For instance, in a study assessing TOC in patients with chronic kidney disease, higher transition readiness scores were associated with fewer self-reported emergency department visits and better medication adherence. 17 In our study, most respondents were unfamiliar with the term “transition of care” and demonstrated readiness gaps such as lack of knowledge of provider contact information, limited emergency planning, and poor understanding of insurance changes. These findings highlight the need for early TOC discussions and preparation involving both patients and caregivers.
Even after readiness gaps are addressed, patients still face numerous TOC barriers. Commonly cited obstacles include difficulty identifying an appropriate adult provider, inadequate insurance coverage, limited adult-provider familiarity with pediatric-onset conditions, poor communication, nonstandardized handoffs, and incomplete medical record transfer.6,18,19 In our cohort, the predominant concern was that adult providers would be unfamiliar with the patient's history and prior treatment, which is consistent with prior literature identifying lack of trust in adult services as a major barrier. 18 In contrast, disorder-specific barriers have also been described. For example, caregivers of patients with Dravet syndrome reported inability to find an adult provider, lack of knowledge of Dravet syndrome, and adult provider discomfort with treating adults with intellectual disabilities and challenging behaviors as the most common barriers to TOC. 20 Similarly, caregivers of children with cerebral palsy cited logistical challenges, differences in care models, and lack of adult provider comfort as the main concerns with TOC. 21 These differences underscore that TOC barriers may vary across neurologic conditions.
Differences in Perception of TOC Between Patients and Caregivers
Our survey revealed notable differences and similarities in the perception of transition between patients and caregivers. Caregivers were generally uncomfortable with the idea of transitioning care and expressed concern regarding readiness, patient autonomy, and continuity of care. Most felt their child was not yet ready to transition. Patients, on the other hand, reported mixed feelings—ranging from curiosity to uncertainty—about the process.
Although both patients and caregivers emphasized the value of a continuity provider to act as a core element of an ideal TOC model, patients also reported need for disease-specific education. Both groups viewed peer or support groups as beneficial and agreed that new adult providers should have strong awareness of the physical manifestations of their condition. These findings underscore the importance of tailoring TOC education and communication to both patients and caregivers to promote readiness and shared confidence in the process.
Key Facilitators of TOC and Implications for Practice
Our findings align with previous TOC research but identify key facilitators particularly relevant to neuroimmune care. Disease-specific education and structured support groups emerged as central to a successful transition. Additionally, an awareness of the physical aspects of the patients’ disorders was also an important theme identified in this study, emphasizing the need for programs that not only teach condition-specific management skills but also prepare patients and caregivers for the evolving physical aspects of neuroimmune disorders throughout adulthood.
Another major insight from our study was the preference for a continuity provider TOC model. Existing transition frameworks often involve a single joint appointment, a combined pediatric-adult clinic, or a written/verbal handoff between providers.6,18,22,23 For instance, a multidisciplinary transition clinic at Nationwide Children's Hospital—featuring pediatric epileptologists, advanced practice providers, neuropsychologists, social workers, and an adult provider that visits the pediatric clinic monthly for a transition clinic appointment—demonstrated higher successful transition rates in patients seen in their TOC clinic compared with those that were not (91% vs 65%) and in less than 6 months (P = .013). 24 These models can be resource-intensive and face challenges with reimbursement, staffing, and sustainability.24,25
In contrast, with a continuity provider TOC model, the provider follows the patient through transition which may address patient and caregiver concerns about provider familiarity, ensure consistent knowledge transfer, and strengthen trust. This model may also eliminate challenges with reimbursement and sustainability. Given the complexity and expanding therapeutic landscape of neuroimmune disorders, this model may be particularly well suited for this patient population and merits further evaluation. We do, however, recognize feasibility of this type of model may vary across institutions.
Limitations
There are several limitations to this study including small sample size and single-center design that may limit generalizability. Another limitation is that the relatively young age of participants could have influenced both transition awareness and readiness gaps; however, we feel that surveying this age provides important insight regarding starting transition conversations early. Additionally, age-appropriate survey wording limited direct comparison with caregiver responses on some items. Although the survey was adapted from established TOC frameworks, formal cognitive interviewing or external content validity was not performed, and the use of fixed response items with minimal free-text options may have limited the depth of participant perspectives. Finally, although English and Spanish versions of the survey were available, the use of only these two languages may still limit generalizability for families with other primary languages.
Future Directions
Based on our findings we plan to develop a TOC program tailored to youth with neuroimmune disorders and their caregivers. This program will include a comprehensive educational curriculum on neuroimmune conditions, strategies to enhance autonomy and emergency preparedness, and focused content addressing the physical aspects of these disorders across the age span. In parallel, we intend to establish dedicated youth and caregiver support groups to foster community, shared learning, and promote confidence in the transition process. Finally, we aim to design and evaluate a continuity-provider-driven TOC model, measuring its impact on patient satisfaction, care continuity, and follow-up adherence.
Conclusion
Youth with neuroimmune disorders and their caregivers exhibit distinct gaps in transition readiness and express important TOC concerns and facilitators. The most common barrier was concern that new adult providers would be unfamiliar with the patient's condition and treatment. Structured education, provider continuity, and dedicated support programming emerged as central facilitators. Further research should evaluate continuity-provider TOC models to optimize transition experiences and long-term engagement in care.
Supplemental Material
sj-pdf-1-jcn-10.1177_08830738251408103 - Supplemental material for Transition Readiness and Care Needs Among Youth With Neuroimmune Disorders: A Descriptive Survey Study
Supplemental material, sj-pdf-1-jcn-10.1177_08830738251408103 for Transition Readiness and Care Needs Among Youth With Neuroimmune Disorders: A Descriptive Survey Study by Duriel Hardy in Journal of Child Neurology
Supplemental Material
sj-pdf-2-jcn-10.1177_08830738251408103 - Supplemental material for Transition Readiness and Care Needs Among Youth With Neuroimmune Disorders: A Descriptive Survey Study
Supplemental material, sj-pdf-2-jcn-10.1177_08830738251408103 for Transition Readiness and Care Needs Among Youth With Neuroimmune Disorders: A Descriptive Survey Study by Duriel Hardy in Journal of Child Neurology
Footnotes
Acknowledgments
I appreciate the assistance of Dr Karla Robles Lopez for administration of some of the surveys during the study time period and for her help with entering survey results into the RedCap database.
Author Contributions
Manuscript and survey concept, writing, and editing.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.