
Abstract
Background
Cerebral palsy is a group of nonprogressive motor disorders resulting from early brain development impairment. Its prevalence is higher in low- and middle-income countries, where health care resources are limited. Data on cerebral palsy in refugee settings remain scarce, particularly in regions marked by prolonged displacement.
Methods
This cross-sectional study examined 29 children with cerebral palsy in the Sahrawi refugee camps in Tindouf, Algeria. Detailed demographic, medical history, neurological findings, and comorbidity data were collected during outpatient visits conducted as part of a humanitarian mission.
Results
Perinatal distress was reported in 65.5% of cases. Motor impairments were significant, with only 44.8% able to walk and 20.7% lacking head control. Language delays (65.5%), feeding difficulties (65.5%), and epilepsy (52%) were highly prevalent. Diagnostic evaluations, such as magnetic resonance imaging (MRI) and electroencephalography (EEG), were scarce and inconsistent. Access to rehabilitation services was discontinuous, and pharmacologic treatments for spasticity and pain were unavailable. Environmental factors, such as sandy terrain, further complicated mobility.
Conclusion
Cerebral palsy in the Sahrawi refugee camps reflects patterns seen in low- and middle-income countries but is exacerbated by displacement and resource scarcity. Improved access to early diagnosis, structured rehabilitation, and targeted pharmacologic therapies is urgently needed to address these unmet needs and improve outcomes for affected children.
Cerebral palsy is a group of disorders affecting movement and posture that are caused by nonprogressive disturbances in the developing fetal or infant brain. It is frequently associated with additional impairments, including those affecting sensory, cognitive, communication, and perception, as well as seizure disorders. 1
Cerebral palsy can be classified into 4 main categories: spastic, dyskinetic (dystonic and choreoathetoid subtypes), ataxic, and mixed forms. 2 The condition typically manifests in early childhood, before the age of 18 months, with diagnosis occurring between 12 and 24 months in high-income countries.1,3,4 The advent of improved diagnostic instruments, including MRI, General Movements Assessment, and the Hammersmith Infant Neurological Examination, has enabled earlier diagnosis, in some cases before 6 months of age, with predictive sensitivities of 86% to 98%. 5 An early diagnosis allows for timely intervention, with the aim of optimizing motor, cognitive, and communication outcomes, preventing secondary impairments and supporting the mental health of caregivers. 5
In high-income countries, the prevalence of pre- and perinatal cerebral palsy is approximately 1.5 per 1000 live births, increasing to 1.6 per 1000 when post-neonatal cases are included. 3 The improvement in neonatal care has contributed to a decline in the prevalence of pre- and perinatal cerebral palsy, although the post-neonatal rates remain unchanged. 3 The estimated lifetime costs for an individual with cerebral palsy in the United States are approximately US$1 million, comprising health care, education, social services, and lost economic opportunity. 6
In contrast, data on cerebral palsy prevalence and clinical profiles in low- and middle-income countries are scarce. 7 Low- and middle-income countries tend to report higher cerebral palsy prevalence rates because of less comprehensive neonatal care and greater exposure to post-neonatal risk factors, including infections and malnutrition. 3 Epidemiologic studies have estimated that the prevalence of cerebral palsy in low- and middle-income countries ranges from 2.9 to 4.0 per 1000 live births, which is nearly double the rates observed in high-income countries. 8 It is estimated that 80% of cerebral palsy cases occur in low- and middle-income countries. 9
Children with cerebral palsy in low- and middle-income countries encounter distinctive challenges. A longitudinal cohort study conducted in Uganda revealed that children with cerebral palsy exhibited lower mobility and self-care skills compared with their counterparts in Sweden, indicating disparities in developmental trajectories. 10 These findings indicate that a considerable number of children in low- and middle-income countries, even those with less severe forms of cerebral palsy, fail to achieve their full developmental potential. 10 Furthermore, the challenges faced by parents are compounded by factors such as isolation, marginalization, and discrimination, which limit their ability to work and strain family resources. In the absence of appropriate assistance, families may be prone to heightened levels of stress and diminished mental well-being. 11
Barriers to intervention for children with cerebral palsy in low- and middle-income countries include delayed diagnosis, lack of access to evidence-based early intervention, insufficient state support, financial constraints, poor accessibility, a shortage of specialized health care workers, and pervasive stigma and social exclusion. 11 It is imperative that these obstacles be overcome if the vicious cycle of disability and poverty is to be broken.
Western Sahara is a site of a longstanding geopolitical dispute between Morocco and the Polisario Front. Because of previous armed conflict, many civilians have been seeking sanctuary in the Tindouf camps in the Algerian desert for 45 years. Figure 1 shows a map to understand the localization of refugee camps. 12 The population of these camps is estimated to be 173 000, including 65 000 children, all of whom are reliant on humanitarian aid for survival. 13 Although hospitals and first-aid centers provide basic health care, chronic disease management is severely affected by a lack of resources. 14 Children with neurologic conditions are referred to special education centers (ages 3-18) that offer programs specific to age and disability, incorporating education and activities to improve daily living skills. The Sahrawi population in refugee camps is a closed population suitable for demographic and epidemiologic studies. 15 However, no data are available on consanguinity rates within this population.
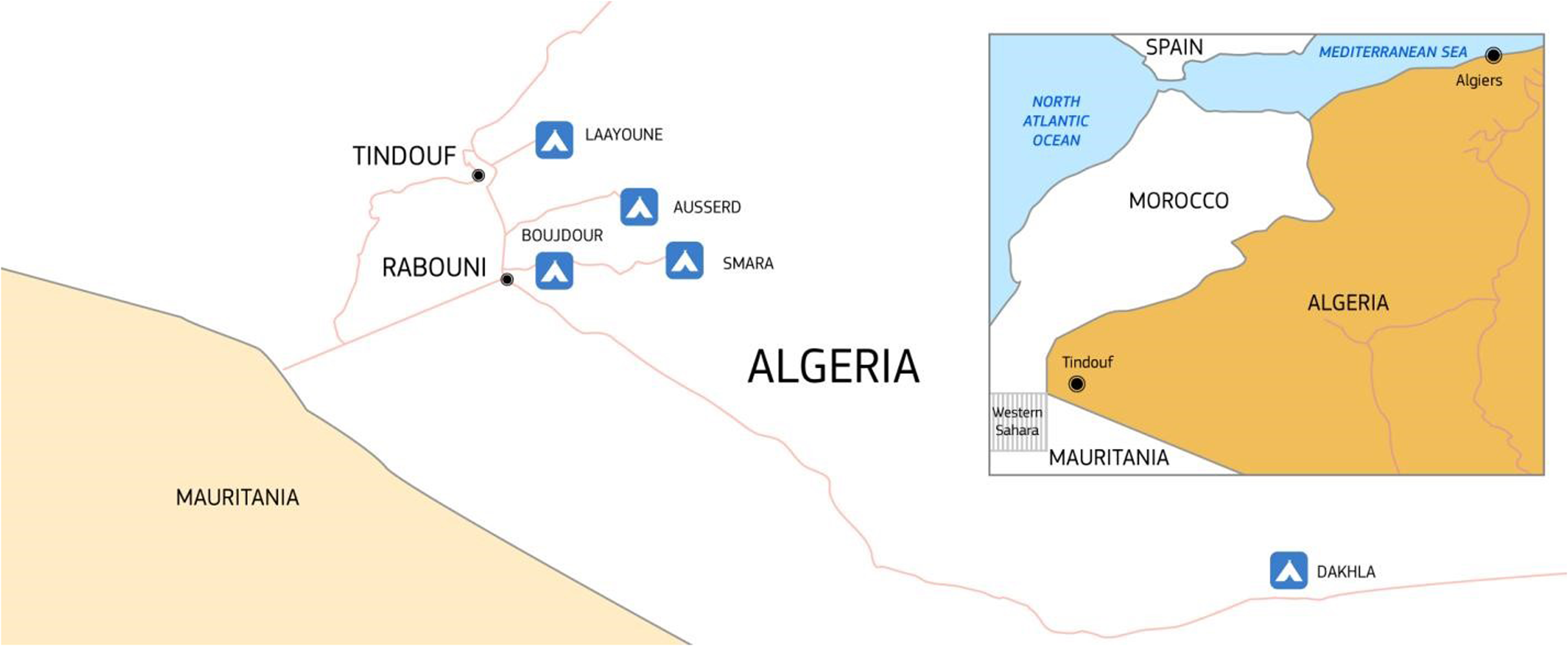
Geographical overview of the Sahrawi refugee camps in Tindouf, Algeria. The camps are home to approximately 173 000 individuals, including 65 000 minors, living in conditions of prolonged displacement and reliant on humanitarian aid. Image source: © European Union, licensed under CC BY 4.0 12
This article has 3 objectives: (1) to describe the clinical characteristics and epidemiologic details in children diagnosed with cerebral palsy within the specified population; (2) to compare the prevalence of cerebral palsy comorbidities in this population with data from high-income countries; and (3) to highlight disparities in the diagnosis and treatment of cerebral palsy between high-income countries and this resource-limited setting.
Methods
Study Design and Setting
This cross-sectional observational study was conducted over a period of 2 weeks (April 13-27, 2024) in 2 hospitals located within the Sahrawi refugee camps in Tindouf, Algeria.
The research team included 3 child neurologists and psychiatrists, 2 developmental psychologists, a speech therapist, and an Italian-Arabic interpreter, each fulfilling a distinct role.
The child neurologists conducted anamnestic interviews and neurologic assessments with the assistance of an interpreter, whereas the psychologists and speech therapist evaluated family settings, support systems, and identified comorbidities when feasible. This interdisciplinary approach guaranteed a comprehensive evaluation of the clinical and developmental challenges faced by children with cerebral palsy in this context of limited resources.
By using structured records to collect detailed clinical, developmental, and caregiver-related data, the study aimed to build a contextualized understanding of cerebral palsy comorbidities within the Sahrawi refugee population. These findings were compared with the wider global literature to identify strengths and weaknesses in care and identification of cerebral palsy in this population and to inform potential interventions.
This study was conducted and reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. A completed STROBE checklist is provided in the supplementary material (Supp_1_STROBE). 16
Study Population
All children who presented for outpatient child neurologic and psychiatric consultation to the clinics underwent an initial evaluation to collect general information, preliminary history, and reasons for consultation. Eligible participants included those referred for consultations with neurologic or psychiatric symptoms.
This approach was considered more culturally appropriate than door-to-door assessments, as it allowed families to independently decide whether to bring their children to the clinic. This method respected local customs while ensuring ethical data collection.
Data Collection
A structured clinical record, available in the supplementary material (Supp_2_ClinicalRecord), was developed to standardize data collection and facilitate subsequent analysis. Designed for accuracy and efficiency in a time-constrained, resource-limited setting, the record included the following sections:
- General Information: subject demographics and referral details. - Medical History: birth and neonatal events, motor and language development, feeding difficulties, sleep-wake patterns, undiagnosed epilepsy indicators, and current treatments (eg, school attendance, pharmacologic or rehabilitative therapies). - Clinical Evaluation: findings from general and neurologic examinations, global motor functioning using the Gross Motor Function Classification System (GMFCS), pain assessment using the r-FLACC Pain Rating Scale
17
(a validated tool for assessing pain in children with developmental disabilities), and prior diagnostic evaluations (eg, EEG, neuroimaging). The Eating and Drinking Ability Classification System (EDACS)
18
was employed to evaluate feeding difficulties. Language development was evaluated based on caregiver reports, as direct assessments were frequently precluded by linguistic barriers. - Interventions and recommendations: recommendations for further diagnostic tests, pharmacologic treatments, or rehabilitative therapies. -Psychological evaluation: information on family structure, primary caregivers, caregiving responsibilities, and associated challenges.
Data from the clinical records were digitized using an optical reader to ensure efficient and accurate analysis.
In the context of this study, cerebral palsy was diagnosed when children exhibited nonprogressive neurologic signs originating in the perinatal period, supported by a history of perinatal injury and corroborative MRI findings. In situations where clinical and historical evidence strongly indicated the presence of cerebral palsy, a diagnosis was made without the need for MRI confirmation. Some children had been diagnosed with cerebral palsy by other medical practitioners.
Ethical Considerations
The study was conducted as part of a humanitarian initiative by the nonprofit volunteer organization Medicina e Assistenza ai Margini with the approval of the Institutional Review Board of the IRCCS Stella Maris Foundation and endorsed by the Ministry of Education of the Sahrawi Arab Democratic Republic (SADR). Verbal informed consent was obtained from all participants’ legal representatives, in accordance with local regulations and ethical guidelines. The study adhered to the principles outlined in the Declaration of Helsinki.
Literature Review
A comprehensive literature review was conducted to contextualize the study findings, using leading scientific databases including MEDLINE (via PubMed), Embase, and Scopus. The search strategy employed a combination of keywords such as epidemiology, cerebral palsy, and child, focusing on full-text articles published between 2014 and November 2024. The review was not conducted systematically with a predefined protocol; studies were prioritized based on their ability to compare the prevalence of cerebral palsy and its comorbidities in high-income countries and low- and middle-income countries. Articles selected for inclusion were those that provided robust epidemiologic data, including large sample size, well-defined study populations, and data on comorbidities. The selection process involved a thorough review of abstracts and full-text articles to ensure their relevance to the study's aims.
Statistical Analysis
Data from the clinical records were digitized using an optical reader and subsequently incorporated into a database. Given the sample size of 29 children, the analysis was conducted using descriptive statistics to characterize the study population.
For categorical variables, frequencies and percentages were calculated. Continuous variables were expressed as medians and interquartile ranges (IQRs), where applicable. The normality of the continuous variables was evaluated using the Shapiro-Wilk test. When necessary, comparisons between categorical data were performed using Fisher exact test.
The objective of the analysis was to provide a summary of the demographic, clinical, and developmental characteristics of children with cerebral palsy in this resource-limited setting, thereby offering insights for comparison with existing epidemiologic literature.
Results
Study Population Characteristics
A total of 101 children were evaluated, of whom 29 (29%) were diagnosed with cerebral palsy. Among these, 20 (69%) were female and 9 (31%) were male. The mean age was 10 years 2 months (SD ± 7 years 5 months), with a median age of 9 years 6 months.
In 6 children, the diagnosis was classified as “highly suspicious” for cerebral palsy because of an unclear history of perinatal distress or absent MRI findings. This finding aligns with existing literature showing that although about 80% of individuals with cerebral palsy exhibit acquired brain injury on MRI, a significant minority do not. 19 Therefore, the absence of MRI findings does not exclude a clinical diagnosis of cerebral palsy when supported by history and neurologic examination.
Of the 101 subjects evaluated in the neurologic and psychiatric ambulatory setting, 19 (19%) were diagnosed with epilepsy; however, when cases of epilepsy associated with other diagnoses were included, the number increased to 34 (34%). Two patients (2%) had neurodevelopmental delay, 8 (8%) had features suggestive of genetic syndromes without specific neurologic manifestations, and 3 (3%) had predominant lower limb and cingulate weakness, suggesting a possible neuromuscular disease. One child exhibited symptoms of peripheral neuropathy.
Neurodevelopmental and psychiatric disorders were present in 5 patients (5%) with signs of autism spectrum disorder, or a high suspicion of this diagnosis, whereas 4 patients (4%) exhibited psychiatric conditions, including anxiety, mood disorders, or obsessive-compulsive disorders. Furthermore, 30 participants (30%) had other clinical conditions, such as brachial plexus palsy, headaches, hearing impairment, sleep disorders, and nutritional issues. Figure 2 provides a general overview of the reason for clinic referrals.
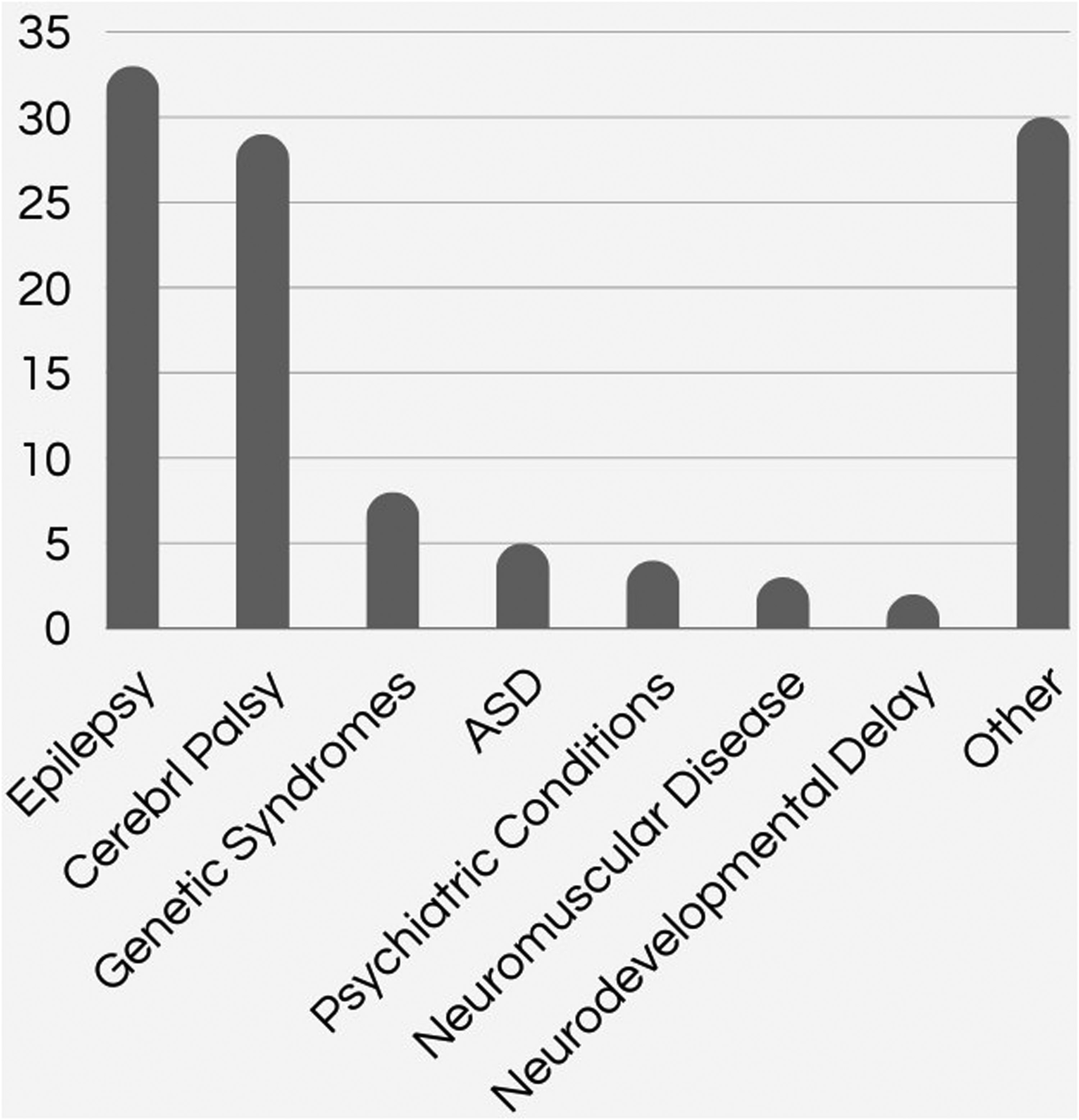
General overview of clinic referrals. This figure shows the reasons for clinic referrals, with epilepsy and cerebral palsy being the most common. Other diagnoses include genetic syndromes, autism spectrum disorder, psychiatric conditions, neuromuscular diseases, neurodevelopmental delay, and a range of additional conditions.
Medical History
In the cohort of the 29 children with cerebral palsy, the majority (80.3%) of the children were born at term, according to the parental report. However, the gestational age was not known for the remaining 6 (20.7%). Perinatal distress was reported in 19 children (65.5%), and 8 (27.6%) had experienced a history of infectious diseases in early life.
In the total sample of 29 subjects, 16 (55%) presented with epilepsy, whereas 7 (24%) had a history of seizure without a diagnosis of epilepsy.
Language impairments were observed in 19 children (65.5%), with 10 children (34.5%) exhibiting speech articulation difficulties, 2 (6.9%) being capable of pronouncing only a few words, 4 (13.8%) producing only communicative sounds, and 5 (17.2%) being nonverbal.
Feeding difficulties were common, affecting 19 children (65.5%), and 6 (20.7%) exhibited moderate to severe constipation.
Rehabilitation services were available for 15 children (51.7%), but access was inconsistent. Only 3 children (10.3%) had access to assistive devices such as a standing aid or walker. Pharmacologic treatment for spasticity was unavailable, and epilepsy treatment was often delayed because of limited diagnostic resources, such as EEG. Among children with epilepsy, 12 were receiving antiseizure medications, primarily valproic acid, lamotrigine, and carbamazepine, whereas others lacked access to necessary treatments.
A review of diagnostic procedures revealed that 18 children (62%) underwent at least 1 MRI. Among those, 3 (10.3%) had normal findings, whereas 5 (17.2%) MRI reports were unavailable as parents did not bring them to the consultation. The remaining reports showed heterogeneous findings, including white matter alterations, gray matter abnormalities, or a combination of both. Other reported findings included ventricular changes, concurrent ventricular and gray matter alterations, basal ganglia involvement, and periventricular leukomalacia. Additionally, 15 children (51.7%) underwent an EEG, with 12 of these being children diagnosed with epilepsy. A comparison of epilepsy prevalence between children diagnosed with bilateral cerebral palsy (13/26) and unilateral cerebral palsy (2/3) showed no statistically significant difference (p > .99) based on a Fisher exact test.
Clinical Findings
The results of the neurologic evaluation indicated that 21 children (72.4%) exhibited features of spastic cerebral palsy, 3 (10.3%) showed dyskinetic cerebral palsy, and 2 (6.9%) presented with ataxic cerebral palsy. Three children (10.3%) were too young (<2 years) to be classified clinically.
In terms of motor abilities, 8 children (27.6%) were able to walk independently, 6 (20.7%) could stand with assistance, and 3 (10.3%) could walk with assistive devices. Among those unable to walk, 7 children (24%) could sit independently, whereas 8 (27.6%) had not yet achieved head control. Figure 3 summarizes the motor abilities of the children in our sample. Global functioning was assessed using the GMFCS. Of the 29 children, 6 (20.7%) were classified as GMFCS I, 2 (6.9%) as GMFCS II, 1 (3.4%) as GMFCS III, 4 (13.8%) as GMFCS IV, and 11 (37.9%) as GMFCS V. The assessment of GMFCS was challenging in 5 children (17.2%) because of insufficient caregiver information.
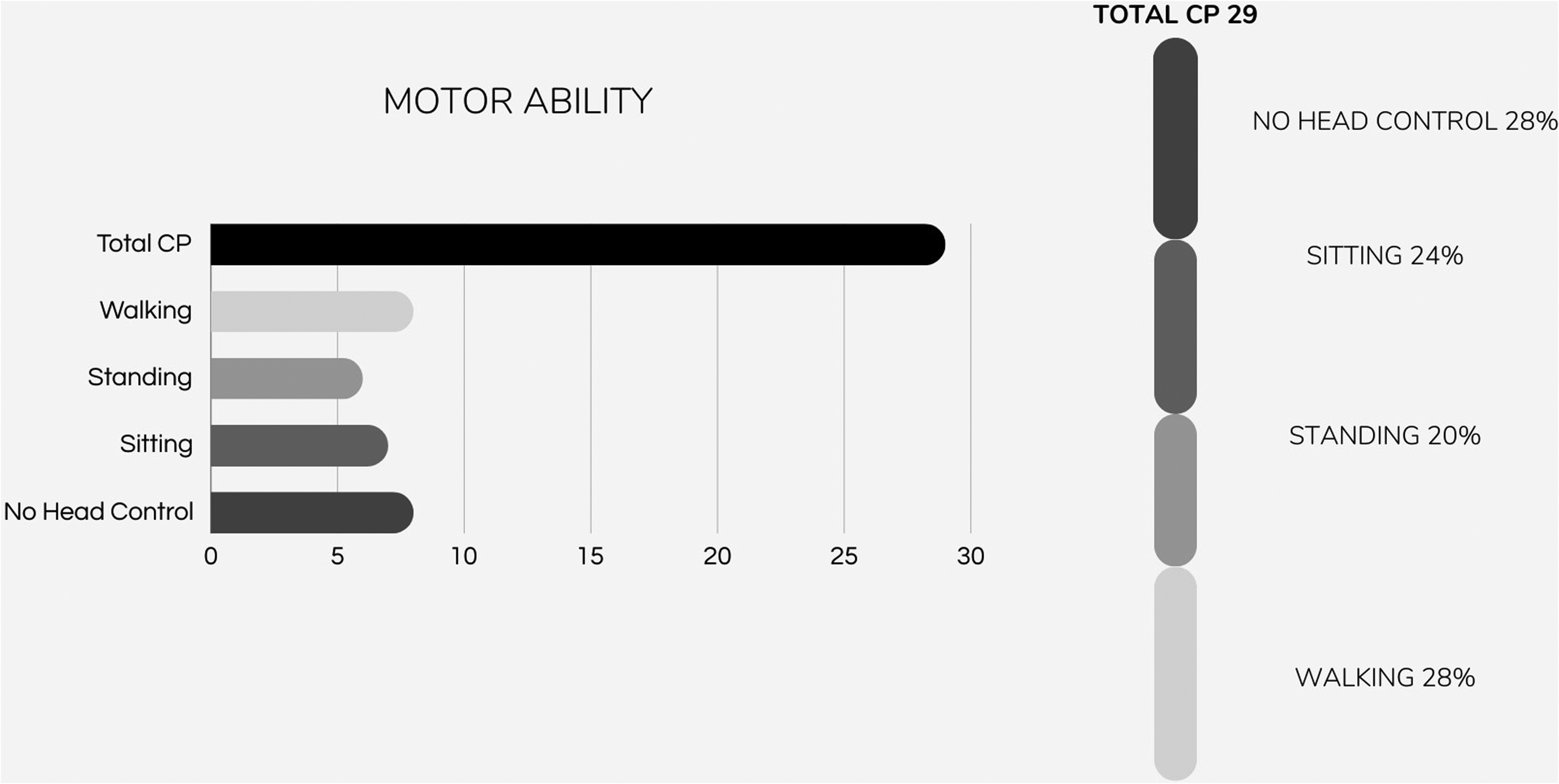
Summary of the motor abilities in the sample of children with cerebral palsy. Among the 29 children with cerebral palsy, 28% had no head control, 24% achieved sitting, 20% were able to stand, and 28% were able to walk. This highlights the variation in motor function across the group.
The research team lacked expertise in orthopedics and physiatry, so clinical diagnoses of osteotendinous comorbidities were only assessed in specific cases. Most children with high suspicion of these comorbidities were referred for further evaluation. A comprehensive assessment showed that 5 children (17.2%) had postural asymmetry, primarily because of scoliosis, whereas 2 children (6.9%) had clinical signs of hip dislocation, both of whom had severe physical disabilities.
Pain was assessed using the r-FLACC Scale for children with disabilities, based on observations and caregiver reports. Only 6 children were assessed for pain, 20.7% of whom exhibited pain. Three children showed minimal pain, 2 moderate, and 1 severe.
Diagnostic and Treatment Recommendations
Of the 29 participants, 11 (37.9%) were advised to start pharmacologic therapy, and 14 (48.3%) were recommended for further diagnostic evaluation including EEG (6), MRI (3), pelvic radiographs (4), and blood tests (3). Rehabilitation therapies were recommended for 13 children (44.8%), particularly those not currently engaged in structured therapy.
Discussion
Comorbidities in Children With Cerebral Palsy
In our cohort, a significant challenge in the care of children with cerebral palsy in this resource-limited setting was the detection and monitoring of comorbidities. As illustrated in Table 1, in this population sample, children with cerebral palsy show a greater degree of verbal and motor impairment and an elevated risk of developing comorbidities in comparison to the findings reported in the literature concerning children from high-income countries.
Comparison of Different CP Comorbidities Between the Literature Data From HICs and the Study Sample.
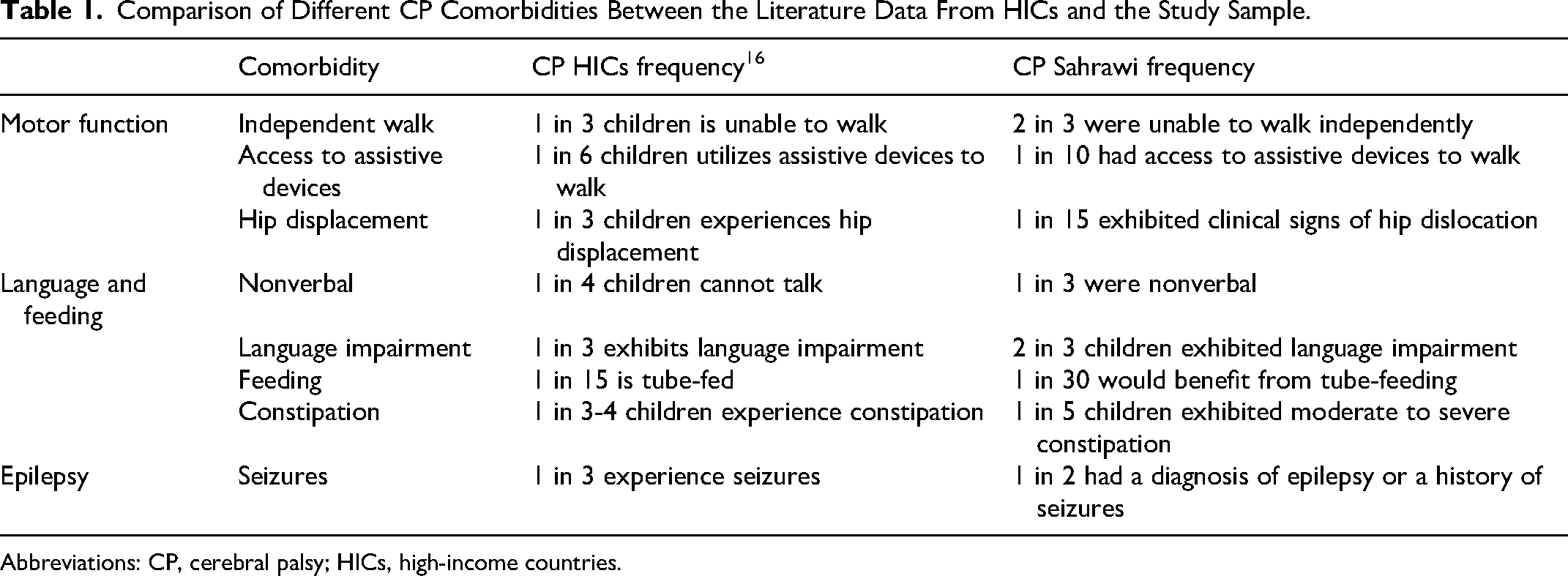
Abbreviations: CP, cerebral palsy; HICs, high-income countries.
Motor Function and Mobility
Literature indicates that approximately one-third of children with cerebral palsy are unable to walk, with key risk factors including 4-limb involvement, intellectual disability, epilepsy, and vision impairment. 20
In the present study, 21 children (72.4%) were unable to walk independently. Although studies have indicated that 1 in 6 children with cerebral palsy use assistive devices, 20 of the 6 children (20.7%) who could have benefited, only 3 (10.3%) had access to assistive devices. Furthermore, although approximately 50% of children with cerebral palsy are able to walk independently, 20 only 8 children (27.6%) in our cohort achieved this level of mobility.
Hip displacement and postural abnormalities are frequently observed in children diagnosed with cerebral palsy, with approximately one-third of affected children developing hip displacement, and 10% progressing to dislocation without proper surveillance. 20 In the present cohort, 2 children (6.9%) exhibited clinical signs of hip dislocation, both of whom had severe physical disabilities. Silent subluxation frequently remains undetected until it causes pain and functional impairment, exacerbating postural issues such as scoliosis. 21 Furthermore, postural asymmetry, predominantly attributable to scoliosis, was observed in 5 children (17.2%) in the present study. Consequently, the implementation of systematic screening programs, exemplified by the Australian Hip Surveillance Guidelines 22 and the Swedish CPUP Follow-Up Programme, 23 is emphasized to facilitate early detection and multidisciplinary care, thereby preventing progression through timely interventions. 21
Language Impairments and Feeding Difficulties
Communication difficulties are a common occurrence in children with cerebral palsy. Approximately 1 in 4 have challenges in verbal communication and 1 in 3 exhibit language impairments. 20 In the present cohort, 24 children (83%) had language impairment, with 10 children (34.5%) having articulation difficulties and 11 children (37.9%) being nonverbal.
Feeding difficulties and gastrointestinal issues, including oropharyngeal dysfunction, gastroesophageal disease, and constipation, frequently accompany cerebral palsy. In our study, 6 children (21%) were observed eating in inappropriate positions, such as on their parents’ arms or legs. EDACS scoring revealed that 1 child presented an inability to eat or drink safely, and tube feeding would have been required (score 5), 2 had significant safety concerns (score 4), and 2 had minimal to no feeding difficulties. The literature shows that children with cerebral palsy are more likely to experience feeding issues by 6 months of age, and 1 in 15 required tube feeding.
Malnutrition and growth failure are linked to feeding difficulties in cerebral palsy, and these issues contribute to reduced cerebral and immune function, delayed growth, and increased respiratory complications. 24 The ability to feed orally requires mature sucking skills and the coordination of sucking, breathing, and swallowing, which are often impaired in children with cerebral palsy, especially those with severe forms (GMFCS IV or V).25,26 In our cohort, 19 children (65.5%) showed signs of dysphagia, with 14 children (48%) exhibiting clinical features of severe cerebral palsy (GMFCS IV or V).
Estimates suggest that between one-third and one-quarter of children with cerebral palsy experience constipation. 20 In our sample, 6 children (20.7%) exhibited moderate to severe constipation.
Epilepsy
Epilepsy is a common comorbidity in cerebral palsy, affecting approximately 1 in 4 children, with up to 1 in 3 experiencing seizures at some point. 20 Its reported prevalence ranges from 15% and 60%, with most cases emerging within the first 4-5 years of life. In our sample, 16 children (55%) had a diagnosis of epilepsy or a history of seizures.
Existing literature indicates a correlation between epilepsy and the severity of cerebral palsy, with epilepsy being most prevalent in individuals with tetraplegia (50%-94%), frequently observed in those with hemiplegia (33%-50%), and less common in those with diplegia and ataxic cerebral palsy (16%-27%). 24 However, no significant correlation was observed between epilepsy and cerebral palsy severity in our cohort, although our small sample size limits statistical power and should be considered when interpreting results.
Diagnosis
This study highlights the diagnostic challenges faced in the Sahrawi refugee camps. The high prevalence of perinatal distress and early-life infections aligns with findings from other low- and middle-income countries, 3 emphasizing the impact of limited prenatal and perinatal care on cerebral palsy development. The study found profound motor impairments, with only 27.6% of children achieving independent walking, and prevalent language impairments and feeding difficulties, underscoring the need for early interventions.
The absence of structured diagnostic pathways, constrained access to imaging, and a lack of specialized care providers contribute to delays in cerebral palsy diagnosis and intervention. Future efforts should focus on strengthening early screening programs, increasing access to essential medications, and expanding rehabilitation services through community-based initiatives.
Access to Treatment
Physiotherapy access in our cohort (52%) varied significantly depending on location and community involvement, leading to inconsistencies and treatment discontinuation. Compared with high-income countries, access to orthotics and assistive devices was limited. Of the 13 children who could walk without assistance, only 3 had access to aids such as a standing aid or walker, and 1 child had a wheelchair. Environmental factors in the refugee camps, including sandy terrain and uneven surfaces, further restrict mobility.
Pharmacologic treatment gaps were also evident. Literature recommends drugs like baclofen, clonidine, and gabapentin for managing dystonia and spasticity, as well as botulinum toxin injections and orthopedic surgery for severe cases.21,27 However, in the present cohort, only 1 child had undergone orthopedic surgery (tenotomy), outside the Sahrawi refugee camps as part of a solidarity mission, despite others meeting surgical indications. Pharmacologic treatments for spasticity and epilepsy were frequently unavailable or inadequate, reflecting broader health care disparities.
Access to ASMs was limited. Although ASMs are standard for epilepsy in cerebral palsy, 20 many children faced delays in diagnosis and treatment because of limited access to hospitals, EEG diagnostics, and medications. Although most children with a confirmed epilepsy diagnosis were receiving ASMs, others with suspected seizures lacked diagnosis and treatment.
Follow-up consultations were infrequent, with some children going months or years without specialist evaluations. Medication availability was constrained, with valproic acid being the most prescribed drug, followed by lamotrigine, carbamazepine, and levetiracetam. Certain drug classes were restricted by the Algerian government and Sahrawi Arab Democratic Republic, further contributing to inequities in treatment.
Despite the small sample size, our findings underscore the urgent need for targeted health care strategies to improve outcomes for children with cerebral palsy in this setting. Further research incorporating longitudinal follow-up and broader community assessments will be essential to refine interventions and address existing gaps in care.
Limitations and Future Research Directions
The small sample size limits the generalizability of findings, and access to care may have influenced patient selection, as families with better resources were more likely to seek clinical evaluation. This suggests that children with even greater barriers to care or severe clinical features may face worse outcomes.
Data on cerebral palsy comorbidities in low- and middle-income countries are highly variable because of differences in health care resources and study methodologies, complicating comparisons. The development of systematic reviews in the future could facilitate the identification of key comorbidities and the contextualization of disparities across low- and middle-income countries. The necessity for cost-effectiveness studies is evident in order to ascertain affordable interventions that could improve the delivery of care in such settings.
Given the variability in cerebral palsy data across low- and middle-income countries, before prevention and intervention strategies can be effectively implemented, it is essential to establish a more systematic and comprehensive approach to epidemiologic data collection. A structured and widespread surveillance system, developed in accordance with local guidelines, would allow a more accurate estimation of the prevalence of cerebral palsy and associated comorbidities. This would provide a stronger basis for targeted health planning and resource allocation, ensuring that future interventions are both evidence-based and contextually appropriate.
The limited access to reliable perinatal data and the challenges of early diagnosis persist as significant issues, along with the struggle for a correct etiologic definition of cerebral palsy.
The implementation of awareness campaigns to enhance prenatal care, nutrition, and infection risk awareness is imperative. The training of local health care providers in the implementation of simple, cost-effective screening tools like the Hammersmith Infant Neurological Examination and General Movements Assessment could facilitate an early identification of cerebral palsy in high-risk infants.
Further efforts should focus on expanding diagnostic capabilities, incorporating telemedicine for remote evaluations, and increasing the availability of critical medications such as baclofen and botulinum toxin. Additionally, developing structured rehabilitation programs and piloting community-based rehabilitation initiatives could improve access to therapy for children in remote areas.
Finally, research on prevention strategies tailored to this specific setting is essential. The identification of risk factors and the implementation of targeted prenatal and perinatal interventions could help reduce cerebral palsy prevalence in refugee populations.
Conclusions
This study emphasizes the significant challenges in diagnosing, monitoring, and managing cerebral palsy and its comorbidities in resource-limited settings, such as the Sahrawi refugee camps. Gaps in access to early diagnosis, rehabilitation, spasticity management, and specialized care highlight the need for sustainable, context-specific interventions to improve outcomes for children with cerebral palsy.
Future efforts should prioritize raising awareness policies by promoting maternal health care, reducing disability stigma and expanding community-based rehabilitation for children with cerebral palsy and their families. Training local health care professionals in cost-effective screening for early cerebral palsy detection and addressing comorbidities, such as malnutrition, is essential to improve outcomes and quality of life.
To address the disparity in access to specialized care, telemedicine presents a viable solution for remote consultations, second opinions, and the training of local health care providers. The integration of telemedicine with visiting multidisciplinary teams facilitates enhanced diagnostic accuracy and improved clinical decision-making, particularly in the context of imaging and complex cases.
Finally, it is essential to collaborate with local health authorities in order to reinforce the resilience of health care systems. By prioritizing training, resource allocation, and the development of structured early intervention pathways, it is possible to address the specific requirements of this population and ensure the long-term enhancement of care delivery.
By employing targeted research and locally adapted strategies, future endeavors have the potential to address existing deficiencies and enhance the quality of life for children with cerebral palsy and their families in resource-limited settings.
Supplemental Material
sj-pdf-1-jcn-10.1177_08830738251336486 - Supplemental material for Cerebral Palsy in a Rural Desert Population of Southern Algeria: A Cross-Sectional Study of Epidemiology of Comorbidities and Unmet Needs
Supplemental material, sj-pdf-1-jcn-10.1177_08830738251336486 for Cerebral Palsy in a Rural Desert Population of Southern Algeria: A Cross-Sectional Study of Epidemiology of Comorbidities and Unmet Needs by Linda Bonezzi, Ilaria Accorinti, Francesca Maria Agostina Papoff, Maria Orsi, Giacomo D’Arcangelo, Emanuele Bartolini and Roberta Battini in Journal of Child Neurology
Supplemental Material
sj-pdf-2-jcn-10.1177_08830738251336486 - Supplemental material for Cerebral Palsy in a Rural Desert Population of Southern Algeria: A Cross-Sectional Study of Epidemiology of Comorbidities and Unmet Needs
Supplemental material, sj-pdf-2-jcn-10.1177_08830738251336486 for Cerebral Palsy in a Rural Desert Population of Southern Algeria: A Cross-Sectional Study of Epidemiology of Comorbidities and Unmet Needs by Linda Bonezzi, Ilaria Accorinti, Francesca Maria Agostina Papoff, Maria Orsi, Giacomo D’Arcangelo, Emanuele Bartolini and Roberta Battini in Journal of Child Neurology
Footnotes
Acknowledgments
We would like to express our deepest gratitude to the Sahrawi population for their kindness, trust, and invaluable collaboration throughout this study. We extend our sincerest gratitude to the Sahrawi Arab Democratic Republic (SADR) for their invaluable support and assistance in facilitating our work within the refugee camps.
Furthermore, we would like to thank the entire team of physicians, health care professionals, and volunteers who were indispensable in the organization and realization of this mission. Their dedication, expertise, and commitment were crucial to the success of this project.
Finally, we acknowledge the collective efforts of all those who provided logistical, clinical, and emotional support to make this research possible.
Author Contributions
LB: Conceptualization, methodology, writing – original draft, writing – review & editing, data analysis and interpretation, visualization. IA: Conceptualization, methodology, writing – original draft, writing – review & editing, data collection, data analysis and interpretation, visualization. FMAP: Conceptualization, methodology, writing – review & editing, data collection, data interpretation. MO: Conceptualization, methodology, writing – review & editing, data collection, data interpretation. GD: Statistical analysis and interpretation of the data. EB: Methodology, conceptualization, supervision, writing – review & editing. RB: Methodology, conceptualization, supervision, writing – review & editing. All authors approved the final version of the manuscript and are accountable for all aspects of the work.
Consent to Participate
During the ambulatory visits, the purpose of the study was explained to the caregivers with the assistance of an Italian-Arabic interpreter and only the data following the obtaining of verbal consent from participants were recorded.
Consent for Publication
Informed consent to publish was provided by the participant(s) or a legally authorized representative (caregivers).
Data Availability
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethics approval for data collection was obtained from the Sahrawi Arab Democratic Republic as part of the aim of the solidarity mission of the nonprofit association Medicina e Assistenza ai Margini (MAM-Odv).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by Italian Ministry of Health RC 2024 to IRCCS Stella Maris Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.