
Abstract
Growing public awareness of genetic research, increased availability of genetic testing options, and the recent arrival of several gene-targeted therapies have combined to make genetic testing a topic of interest within many disease communities, including muscular dystrophies. We sought to investigate the genetic information received, the genetic services provided, the genetic information and services of interest to young adults with muscular dystrophy, and to identify existing gaps in the delivery of genetic information and services. Young adults with muscular dystrophy were surveyed about their interests and experiences in receiving genetic information/testing. Surveys were completed by 226 young adults with muscular dystrophy (150 male, 72 female; mean age = 21.6 years, range = 16-25 years) from Canada and the United States. Approximately 60% or less of respondents felt knowledgeable about genetic topics, including inheritance and reproductive options. Only 28% of respondents had previously met with a genetic counselor and 60% of respondents wanted to obtain more information. Findings highlight gaps between the receipt of and interest in genetic information.
Muscular dystrophy is etiologically a heterogeneous group of hereditary neuromuscular conditions characterized by progressive muscle destruction and weakness. Muscular dystrophy varies widely in terms of the specific muscles and organs impacted, age of symptom onset, and rate of disease progression.1,2
Young adults with muscular dystrophy are at a critical stage in their health care journey. At this time, young adults with muscular dystrophy are encouraged to assume greater responsibility for their care and to consider their future, including postsecondary education, employment, independent living, participation in social activities, dating, intimacy, sexuality, and family planning. 3 To plan for the future, young adults with muscular dystrophy need the relevant information and support. An important source of this information is through genetic testing to determine the etiology of their condition, and counseling to interpret the information obtained and the impact this information may have on the patient's future.4–6
With the emergence of disease-modifying treatments and increased life spans, muscular dystrophies, including Duchenne muscular dystrophy, are no longer solely childhood conditions. 7 Duchenne muscular dystrophy transition care guidelines recommend that young adults should be provided with medical facts about their reproductive life. 3 These guidelines further recommend that genetic counseling be provided to review Duchenne muscular dystrophy inheritance and implications on family planning. 3 These recommendations are relevant not only to young adults with Duchenne muscular dystrophy but any form of muscular dystrophy. Even with these recommendations, little is known about young adults with muscular dystrophy's interest in or experiences with genetic counseling and parenthood.
A 2018 Muscular Dystrophy Association survey reported that individuals with neuromuscular conditions and their caregivers were highly interested in receiving genetic testing. 4 However, findings indicated there were barriers to accessing genetic testing, including a lack of understanding about the potential benefits and associated costs. 4 Further, 29% of respondents did not feel informed about genetic testing, particularly those diagnosed more than 10 years in the past, those considered low income, and those without a college education. 4
Genetic counselors are well positioned to provide information about the genetic etiology and inheritance of muscular dystrophy, current or emerging therapies, and genetic testing options and their associated benefits, risks, and limitations. Genetic counselors can provide psychological support and facilitate decision making, which may be helpful for young adults navigating the transition to adulthood and the adult health care system.
Growing public awareness of genetic research, increased availability of genetic testing options, and the recent arrival of several gene-targeted therapies have combined to make genetic testing a topic of interest within many disease communities, including muscular dystrophy.8-10 However, beyond the Muscular Dystrophy Association report, there is a paucity of research investigating the experiences and attitudes of individuals with muscular dystrophy outside of Duchenne muscular dystrophy. 11 Thus, the objective of this study was to examine what genetic information and genetic services have been received and what genetic information/services are of interest to young adults with muscular dystrophy, and to identify existing gaps in the delivery of such information and services.
Patients and Methods
Study Design
The study followed a cross-sectional survey study design. The purposefully developed 47-item electronic survey asked young adults with muscular dystrophy about their interests and experiences in receiving genetic information relevant to their condition through closed (ie, multiple choice and Likert scales) and open-ended questions. Survey questions explored respondents’ demographics (eg, gender, age, location, schooling, household incomes, muscle diagnosis, age at diagnosis, and age at disclosure of diagnosis); receipt, self-reported knowledge, and perceived importance of and interest in receiving genetic information (eg, etiology of muscular dystrophy, potential/future genetic therapies, chance of having a child with muscular dystrophy, and genetic testing options for muscular dystrophy before or during pregnancy); and access to genetic counseling. The full survey is available as Supplementary Materials 1 and 2. This research was approved by research ethics boards at the Hospital for Sick Children (1000077815), Holland Bloorview Kids Rehabilitation Hospital (0465), and the University of Toronto (00041862).
Participants
Participants were purposively recruited through neuromuscular disease patient registries (ie, Muscular Dystrophy Association, The Duchenne Registry, and Muscular Dystrophy Canada) or snowball sampling through social media advertisements.
Inclusion criteria were as follows: (1) 16-25 years of age, (2) self-reported muscular dystrophy diagnosis, and (3) resides in Canada or the United States.
Data Analysis
Closed-ended survey questions were analyzed descriptively (eg, frequencies). Open-ended questions (to provide additional context to closed-ended responses) were analyzed using conceptual content analysis. 12 Responses were analyzed independently by two authors (LH and LM) and similar responses were combined into categories to determine common terms within the data. Discrepancies were discussed by LH, LM, and KA until consensus was reached.
Kruskal-Wallis rank-sum tests examined whether the level of self-reported knowledge on genetic topics differed between individuals who had met with a genetic counselor and those who had not, or between individuals who have a family member affected by the same type of muscular dystrophy and those who do not.
Four logistic regression models were fitted to analyze the relationship between participant characteristics and whether an individual reported having received information about each of the four genetic topics of interest (ie, etiology of muscular dystrophy, potential/future genetic therapies, muscular dystrophy inheritance, and genetic testing before/during a pregnancy). Participant characteristics included in the models were annual household income, country of residence (USA or Canada), age when first told about the muscular dystrophy diagnosis, muscular dystrophy diagnosis types (Duchenne muscular dystrophy and Becker muscular dystrophy, and other muscular dystrophy diagnoses). Only surveys containing all fields of interest were included in the models.
Results
A total of 270 surveys were completed. Forty-four surveys were excluded because respondents did not have muscular dystrophy diagnoses (n = 22) and because the required questions for inferential statistics were not completed (n = 22). A total of 226 surveys were included in the analyzed sample.
Participant characteristics are described in Table 1. The mean age of participants was 21.6 years. Age at diagnosis and age diagnosis was disclosed varied slightly with a mean difference 0.94 years (range = 0-14 years). Most participants reported they were not biological parents of any children at the time of survey completion (n = 158, 74%); of those individuals, 47% (n = 74) reported they wanted to be biological parents. Twenty percent of participants (n = 42) reported having other family members affected by the same type of muscular dystrophy.
Participant Characteristics.
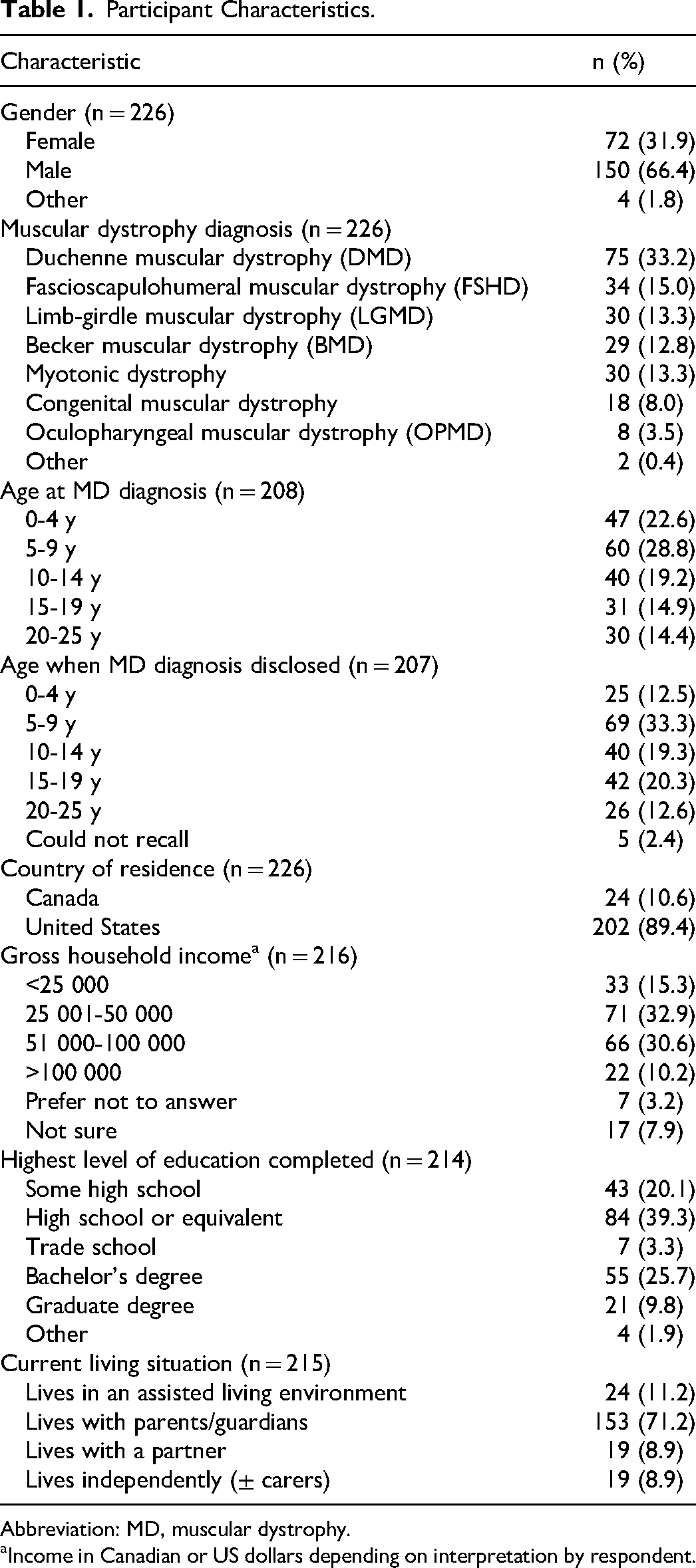
Abbreviation: MD, muscular dystrophy.
Income in Canadian or US dollars depending on interpretation by respondent.
Self-Reported Knowledge About Genetic Topics
Participants (n = 226) self-reported their knowledge on muscular dystrophy–related genetic topics (Figure 1). More than half of participants felt sufficiently informed about their disease etiology (63.3%, n = 143) and potential/future genetic therapy treatment options (52.2%, n = 118). However, fewer participants felt they were well informed about the mode of inheritance (45.6%, n = 103) or their reproductive options (44.2%, n = 100). Furthermore, participants’ self-reported knowledge on genetic topics was not impacted by having met with a genetic counselor (P value range = .48-.92) or having a family member affected by muscular dystrophy (P value range = .22-.99).
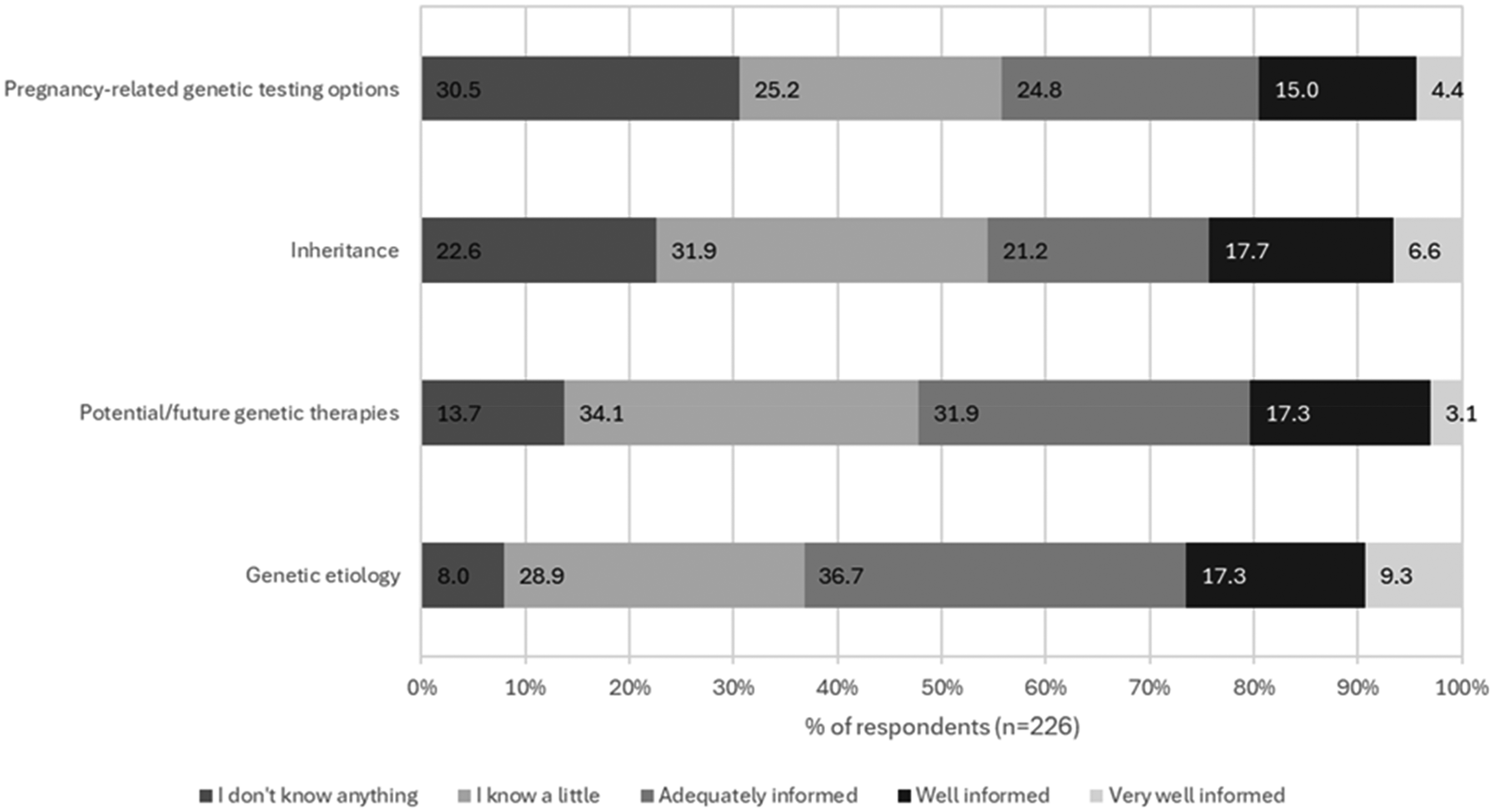
Self-reported knowledge about genetic topics.
Experiences Receiving Genetic Information
Participants reported the information they have received and the sources from which they accessed this information (summarized in Table 2). Common sources of information were respondents’ parents, various medical professionals, and Internet searches. Thirty-one (14%) respondents had not received any information about the genetic topics.
Sources for Receiving Genetic Information by Information Type and Source.
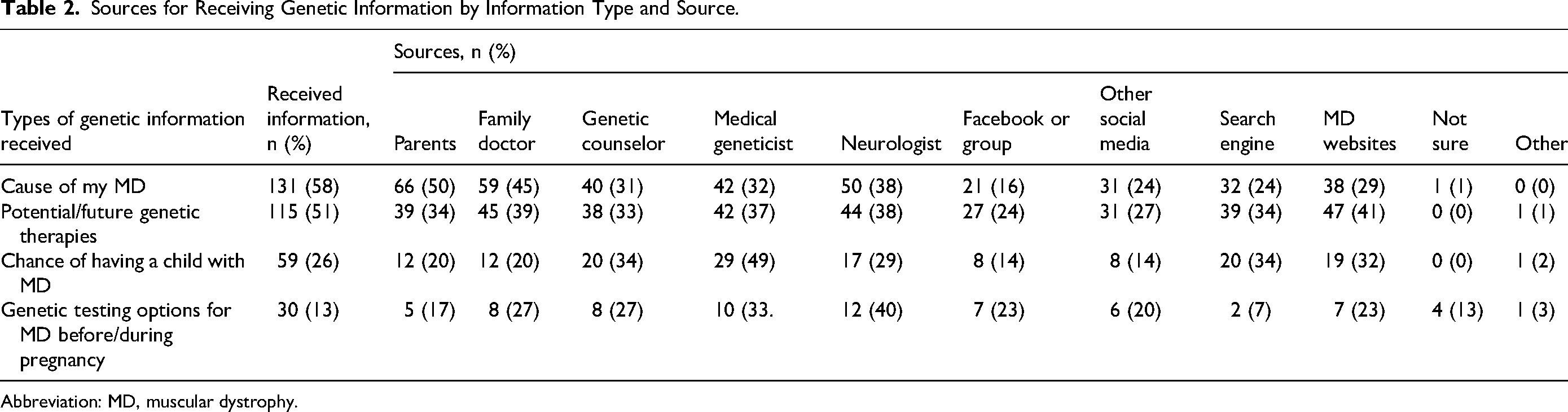
Abbreviation: MD, muscular dystrophy.
Logistic regression analysis (Supplementary Material 1) showed that holding all other predictor variables constant, participants with Duchenne muscular dystrophy or Becker muscular dystrophy were more likely to have received information about future genetic therapies compared to those with other types of muscular dystrophy (OR = 1.96, 95% CI = 1.05-3.70). No other predictor variables tested in the model met the threshold for statistical significance for any of the genetic topics.
Participants seeking genetic information (n = 45) identified barriers, including psychological barriers like feeling hopelessness or fear (20%, n = 9); physical limitations (eg, poor mobility), logistical barriers (eg, lack of time or opportunity), or economic barriers (eg, lack of financial resources to support access to counseling or treatment; 31%, n = 14); information being restricted by caregivers or health care providers (11%, n = 5); not understanding the information or being unable to identify trustworthy sources (24%, n = 11); and a belief that medical knowledge about muscular dystrophy–related genetic topics is limited (13%, n = 6).
Interest in Receiving Genetic Information
More than half (64%, n = 143) of participants believed it is important to receive genetic information about the cause of their muscular dystrophy, 41% (n = 92) of participants believed it is important to receive information about their chance of having a child with muscular dystrophy, and 19% (n = 42) of participants believed it is important to receive information about genetic testing options for muscular dystrophy related to a pregnancy. On the other hand, 15% (n = 35) of participants were not interested in receiving any information about any of the aforementioned topics. Respondents indicated the best ages (median age response) to receive genetic information about their muscular dystrophy (described in Table 3).
Median Age in Years to Receive Genetic Information.
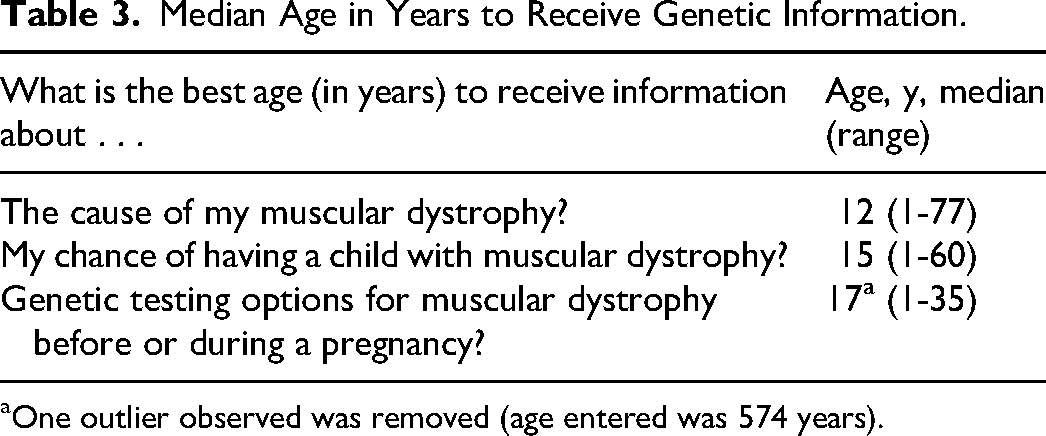
One outlier observed was removed (age entered was 574 years).
Participants wished to know more about potential/future genetic therapies related to their form of muscular dystrophy (57%, n = 128); the cause of their muscular dystrophy (46%, n = 105); chances of having a child with muscular dystrophy (34%, n = 76); pregnancy-related genetic testing options (24%, n = 54); sex, intimacy, or social life living with muscular dystrophy (1.3%, n = 3); and clinical trials (1.3%, n = 3).
One participant expressed frustration at the lack of progress in treatment for their form of muscular dystrophy, reporting that “I was told 15 years ago there would be treatments available by now. Then [sic] CRISPR would be a game changer. Science just leaves [facioscapulohumeral muscular dystrophy] on the back burner while they treat cancer and COVID” (20-year-old female participant with facioscapulohumeral muscular dystrophy).
Respondents believed that the following facts were the most important for them to know about their condition: information about treatments, cures, and ways to optimize health while living with muscular dystrophy (35%, n = 78); prognosis of their muscular dystrophy and impacts on daily life (21%, n = 47); possible physical or psychological issues that may arise (17%, n = 38); inheritance and prevention of recurrence of their muscular dystrophy (7%, n = 15); education about the cause of muscular dystrophy (7%, n = 15); how to access information using the Internet or social media (3%, n = 6); and how to access care (3%, n = 6). Several respondents emphasized the importance of honest communication about their condition (4%, n = 8). Further, several participants expressed doubts about the genetic etiology of muscular dystrophy saying, “Maybe it's because of my poor living habits” (24-year-old male participant with facioscapulohumeral muscular dystrophy) and “I don't think muscular dystrophy is genetically related. Either fetal nutrition or acquired causes” (21-year-old female participant with facioscapulohumeral muscular dystrophy).
Experience Meeting With a Genetic Counselor
Sixty-four participants (28%) reported having met with a genetic counselor, with the mean age at first meeting being 13 ± 6 years old (out of 39 responses). Eleven participants (28%) were less than 12 years of age when they first met with a genetic counselor.
Participants reported speaking about information related to inheritance of muscular dystrophy (26%, n = 11), their genetic cause of muscular dystrophy (40%, n = 7), and treatment options/disease management (16%, n = 7). Two respondents (5%) described receiving support from the genetic counselor: “The genetic counselor communicated with me in detail, understood my condition and psychological condition, gave me some treatment methods, and encouraged me to actively cooperate with the treatment” (20-year-old female participant with myotonic dystrophy).
Participants described varying experiences related to receiving genetic counseling. Participants with positive experiences felt that the genetic counseling session increased their understanding of their neuromuscular condition (36%, n = 13), and felt the counselor was empathic and developed a good relationship with them (8%, n = 3). For example, “[The genetic counselor] explained my etiology and treatment suggestions to me in detail, and he [sic] could contact him at any time if I had any needs” (24-year-old male participant with limb girdle muscular dystrophy). Two respondents (6%) felt their experience with genetic counseling and testing was not positive. One respondent reported, “I did whole exome sequencing twice. Both opened a pandora's box of mutations that no one could really interpret so it just added more fear” (20-year-old female participant with facioscapulohumeral muscular dystrophy).
Experiences and Attitudes Relating to Genetic Testing
Genetic testing was performed in 69% (n = 156) of participants; however, only 47% (n = 107) received a confirmed diagnosis from the genetic test results. Reasons reported for not having received genetic testing included never being offered testing (35%, n = 18), cost (25%, n = 13), living far from testing site (25%, n = 13), not wanting genetic testing (12%, n = 6), and a sibling had already received genetic testing (n = 1, 0.6%). Approximately 60% (n = 29) of those who had not had genetic testing indicated they would be interested in learning more about genetic testing for muscular dystrophy.
Participants were conflicted on whether there were advantages and disadvantages associated with genetic testing for muscular dystrophy. The distribution of responses is displayed in Figure 2.
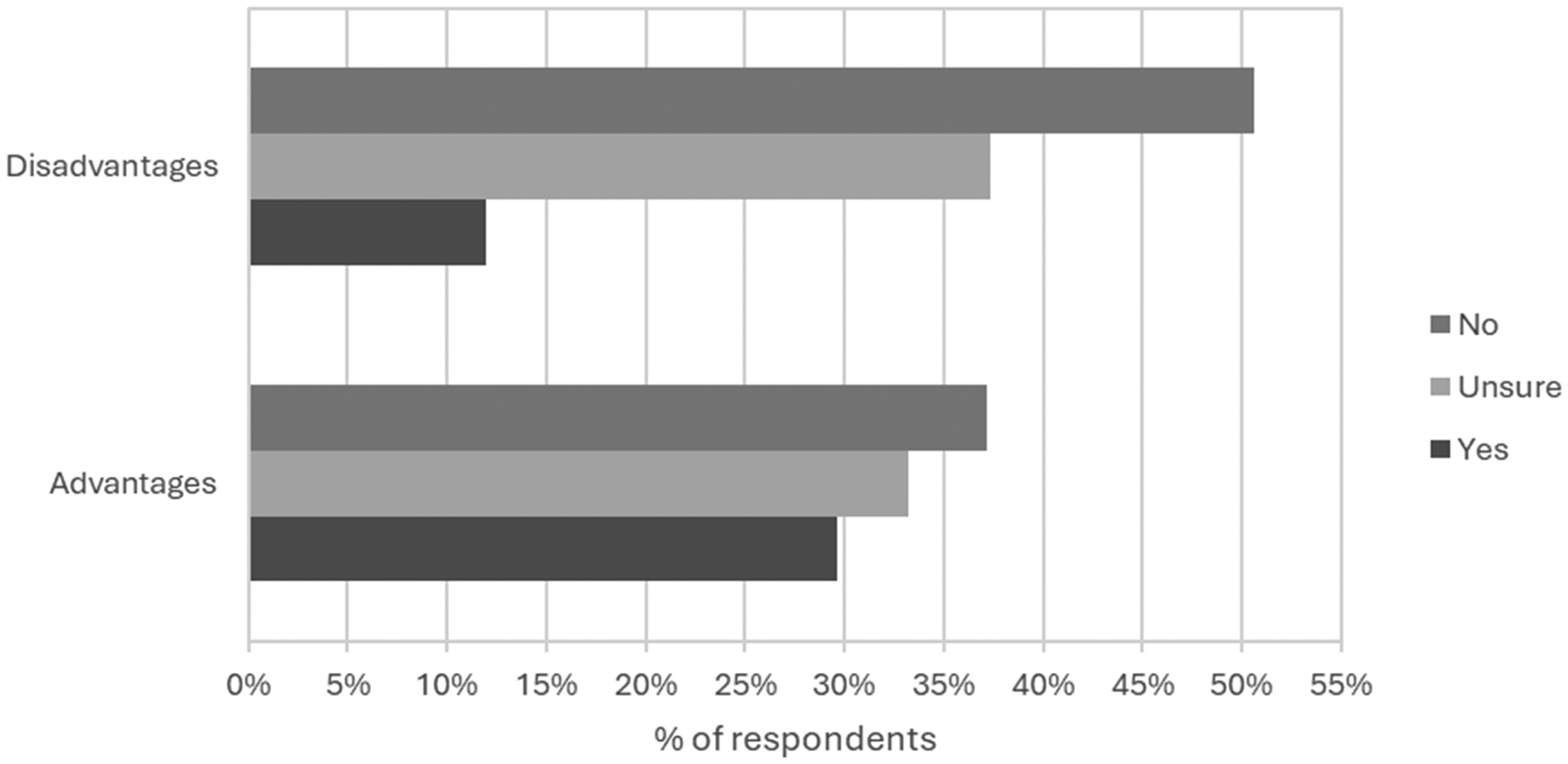
Frequency of respondents’ beliefs about there being advantages and disadvantages to genetic testing.
The following advantages to genetic testing for muscular dystrophy were provided: clarifies inheritance/risk to family members (25%, n = 14), informs clinical management and targeted therapies (30%, n = 17), informs prognosis and plans for the future (23%, n = 13), and identifies a specific cause for symptoms (35%, n = 20). One participant described the biggest advantage as “Having more data for researchers. Not much for person other than they know for sure what they have” (24-year-old male participant with Duchenne muscular dystrophy).
Disadvantages of genetic testing as perceived by participants included feelings of sadness or depression in response to the testing results (18%, n = 2). Additionally, one participant wrote that “the positive test for facioscapulohumeral muscular dystrophy led my Dr. to quit looking for other diagnosis for my problems which hindered my treatment. Just because you have FSHD doesn't mean you don't have other more pressing health issues” (20-year-old female participant with facioscapulohumeral muscular dystrophy).
Discussion
There is a paucity of literature describing if and how genetic counseling services are used by young adults with muscular dystrophy, which genetic topics are of interest, and barriers to receiving information or testing. Beyond the 2018 Muscular Dystrophy Association report mentioned previously, very little research to date has investigated the experiences of individuals with muscular dystrophy other than Duchenne muscular dystrophy. 4 By inviting individuals with all forms of muscular dystrophy to participate, this study serves to amplify the voices of a wider range of young adults with muscular dystrophy. This study contributes findings that address these gaps in the literature.
Experiences with and Interest in Receiving Genetic Information
Genetic topics of interest to young adults with muscular dystrophy included the etiology of their muscular dystrophy, potential genetic therapies to treat their muscular dystrophy, and for a minority, their recurrence risk and reproductive options. Participants emphasized the importance of knowing the prognosis of their condition and how it may impact their daily lives. These findings were consistent with the literature that describes the interest young people with genetic conditions have in receiving more information about the biological cause of their conditions and the impact on their daily lives.13,14 Evidence from the Duchenne muscular dystrophy literature suggests that some parents may be unwilling to discuss life span or the progressive nature of the condition with their affected child.8,14-16 Knowing this, it is important that members of the health care team are prepared to have or facilitate discussions about the patients’ life span and long-term prognosis with the patients, their parents and other family members, with the patients’ permission. Of note, many participants did not have specific questions about the genetics of their condition, suggesting the importance of clinicians being proactive in creating a safe space for the discussion of genetic topics.
Participants preferred to receive information about specific genetic topics at different ages, suggesting that individuals may benefit from multiple conversations about genetic information throughout adolescence and transition to adulthood. Studies exploring the communication of genetic information within families have shown that ongoing communication with children about their genetic diagnosis and its implications improves psychological outcomes and understanding of the condition.8,9 Specifically, Gallo et al 9 recommended which genetic concepts may become important to a child/adolescent at different developmental stages. For instance, it was noted that school-aged children were more concerned about the implications of a genetic condition for themselves and other family members, whereas adolescents were interested in information about their own reproductive risks. Findings from the current study support these recommendations, in particular that young people with genetic conditions preferred to receive information about the cause of their muscular dystrophy at 12 years old, and reproductive risks and related testing options later, at 15 and 17 years old.
Notable differences between young adults with muscular dystrophy's previous receipt of and interest in receiving genetic information were observed. Particularly, only 26% of participants reported having received information about their chance of having a child with muscular dystrophy, whereas 41% indicated that it was important to receive this information. Similarly across all topics, a greater number of participants indicated the importance of receiving information about each genetic topic (ie, etiology of muscular dystrophy, potential future genetic therapies, genetic testing options during pregnancy) than had actually received these types of information. These findings suggest that the genetic information received by young adults with muscular dystrophy and the current rates of receiving genetic counseling are insufficient. These findings highlight the need for genetic counseling throughout adolescence and transition to adulthood.
To further explore young people's experiences with obtaining knowledge and experiences with receiving genetic information, it was important to consider where this population had received information about genetic topics. Parents and family doctors were common sources of information about the cause of muscular dystrophy; however, parents were not common sources of information about inheritance or pregnancy-related genetic testing options. These findings are consistent with the literature stating that adolescents with genetic conditions often rely on parents as primary sources for genetic information on certain topics; however, they may feel uncomfortable discussing reproductive risks.10,13,17 Clinicians may also be reluctant to initiate conversations about sexual and reproductive health with young people living with chronic conditions because of awkwardness, interference from parents, lack of knowledge, or belief that the information is not relevant.18-21 These results emphasize the importance of ensuring parents and clinicians with a limited expertise in genetics and reproductive health are equipped with evidence-based information about these topics.
Furthermore, social media platforms were the most common source of information about potential therapies; however, search engines and websites of recognized muscular dystrophy organizations were also referenced by at least 30% of respondents. These findings suggest the value of clinicians exploring a young adult with muscular dystrophy's comfort level with accessing trustworthy Internet resources and navigating the information provided, particularly because 24% of barriers identified pertained to these issues.
Barriers to Receiving Genetic Information
Participants identified several barriers faced by young adults with muscular dystrophy who wish to access genetic information. The logistical barriers identified, including cost and living far from muscular dystrophy centers, were consistent with the 2018 Muscular Dystrophy Association survey. 4 Psychological barriers to information, such as fear, have previously been described in studies with children with various types of genetic conditions.8,14 Evidence from these studies suggests that fear in children with genetic conditions was commonly related to the unknown aspects of their condition and may be associated with information being purposefully withheld by parents and/or care providers. Findings from the current study further underscored the importance of maintaining consistent open lines of communication about one's muscular dystrophy and creating space during appointments to explore fears, feelings of hopelessness, and other psychological considerations.
Results of the logistic regression suggested that one's muscular dystrophy diagnosis may be a barrier to receiving genetic information as participants with diagnoses other than Duchenne muscular dystrophy or Becker muscular dystrophy were less likely to have received information about genetic therapies. However, these findings are in line with recent advancements and availability of genetic therapies targeting mutations in the gene responsible for both Duchenne muscular dystrophy and Becker muscular dystrophy.22-24 Information about the status of ongoing genetic therapy research targeting other muscular dystrophy diagnoses may not be as easily accessible. The study findings highlight the need for ongoing development of patient-friendly resources with up-to-date information about research across a broader array of muscular dystrophy diagnoses. As therapy development is not uniform across muscular dystrophy types, it may also be useful to develop resources that explain how different gene-specific therapies may be used to treat various forms of muscular dystrophy. Such resources may stimulate discussions between patients and clinicians about the therapy landscape for the patient's specific condition.
Experiences and Attitudes Relating to Genetic Testing
Consistent with the Muscular Dystrophy Association report, the current study reported a high degree of interest in genetic testing among participants. Barriers to receiving genetic testing were consistent with those previously reported by individuals living with neuromuscular diseases. 4 Twenty-five percent of participants identified the new barrier of “living too far from a testing site.” It is possible that the uptake in remote health care provision, accelerated during the COVID-19 pandemic, may result in increased accessibility of specialized care, which may mitigate, or even remove, some of the logistical barriers reported. Furthermore, cost was identified as a barrier to genetic testing by 25% of participants. Throughout the survey, economic barriers were cited almost exclusively by participants from the United States, perhaps reflecting the differences in specialized health care service delivery models between Canada and the United States. Specifically, private insurance in the United States does not always cover genetic testing, 25 and diagnosis is based on presentation and other factors.26,27
The most prominent barrier identified was that participants were not offered genetic testing (60%). In some cases, this barrier may be attributed to health care providers who lack an understanding of the potential benefits of genetic testing. The Muscular Dystrophy Association report illustrated that both patients and clinicians may have misconceptions about the benefits, efficacy, and costs of genetic testing. 4 A common misconception of participants in the current study was that genetic testing was not beneficial in cases where a muscular dystrophy diagnosis has already been confirmed in a family member. The finding that 37% of participants did not think there were advantages to genetic testing suggest that young adults with muscular dystrophy, along with their care providers, require clearer information about the benefits and limitations of genetic testing. The possibility of uncertain results should be discussed and the patient's anticipated reactions to results should be explored.
Implications for the Role of Genetic Counselors and Future Directions
This study has identified several areas where the involvement of genetic counselors may be valuable in helping meet the needs of young adults with muscular dystrophy. Participants identified psychological barriers to receiving genetic information, including fear and feelings of hopelessness. Genetic counselors are well-poised to explore these types of psychological considerations and provide emotional support to patients and their caregivers. 28
Furthermore, genetic counselors can clarify misconceptions about genetic information and testing as they are trained to explain complex information about genetic conditions, including the benefits and limitations of genetic testing. Genetic counselors can respectfully explore diverse belief systems about causes of a genetic condition, which may allow misconceptions to be addressed.29,30 Furthermore, genetic counselors may be useful resources in cases where cost is identified as a barrier to testing by facilitating applications for health insurance coverage.
Participants identified not knowing if a resource was trustworthy as a barrier. Reviewing patient-friendly resources and providing up-to-date information about relevant clinical trials is a common component of genetic counseling sessions that would minimize this barrier.
Few survey respondents reported having met with a genetic counselor, and most of these respondents could not recall the genetic counseling topics discussed, which likely impacts participants’ self-reported knowledge on genetic topics. Because diagnosis of muscular dystrophies generally occurs at younger ages, 27 children may not be present or remember interactions at genetic counseling meetings, impacting knowledge of genetic topics. These findings suggest that the timing and frequency of genetic counseling should be carefully considered. Multiple appointments over the span of childhood and adolescence may be ideal to facilitate gradual adaptation to the condition. Survey respondents identified 12-17 years old as optimal timing to receive genetic information, which should be considered particularly as retention of information typically decreases with time since counseling 31 and it is important that adolescents with muscular dystrophy are knowledgeable about genetic information (ie, etiology of muscular dystrophy, genetic inheritance, genetic testing for pregnancy) during adolescence.
Although barriers to accessing genetic counseling services were not collected, barriers identified in receiving genetic information (eg, limited access to a specialized treatment center, cost) may be relevant. Alternative strategies for genetic counseling services delivery, such as group counseling sessions and creation of online patient resources, have been successful in other patient populations32-34 and should be considered for adolescents with muscular dystrophy. Another alternative strategy for genetic counselors to extend the reach of their services may be to present at family conferences to promote accessibility and minimize misconceptions of genetic counseling services.
Looking ahead, there are several ways in which genetic counselors can ensure that young adults with muscular dystrophy receive the supports they need at the optimal time. First, alternative strategies for genetic counseling service delivery, including telehealth counseling sessions, group counseling sessions, and the creation/curation of online resources could fill the gaps in knowledge and interest in learning about genetic topics. Young adults with muscular dystrophy should be included in the development of these sessions and/or resources to ensure they meet their needs and are meaningful. Furthermore, the rereferral of adolescents to genetic counseling to review genetic topics that may have previously been discussed in early childhood or with their parents/caregivers should be considered. Rereferral to genetic counseling may also be indicated to explore the option of genetic testing in detail, if not previously completed. At this time, genetic counselors could address misconceptions about the benefits and limitations of genetic testing and particularly in the United States, facilitate applications for insurance coverage.
Limitations
Although this study substantially adds to both the neuromuscular and genetic counseling fields, it has some limitations. This study included only individuals who could read and write in English, which may limit the generalizability of the results. Additionally, males represent a large proportion of the study sample, likely related to the proportion of participants with Duchenne muscular dystrophy. Furthermore, this study relied on self-reported patient data, including muscular dystrophy diagnosis type and age, which could not be verified by the research team. Because of anonymous data collection, the study design did not restrict individuals from completing the electronic survey multiple times and therefore cannot exclude the possibility of duplicate records in the data set. Lastly, because recruitment was completed by self-referral from patient registries, participants may have been more informed about genetic topics and be more likely to be interested in learning more.
Conclusions
We explored the types of genetic information and services received and of interest to young adults with muscular dystrophy. Participants were highly interested in receiving information about the cause of their muscular dystrophy and potential genetic therapies to treat muscular dystrophy, with fewer participants interested in information about the chance of having a child with muscular dystrophy or pregnancy-related genetic testing options. Study findings emphasized the importance of knowing one's prognosis and the associated impact on daily life. Fewer participants reported receiving information about specific genetic topics than the number who believed the information to be important, suggesting that more genetic information should be provided. Barriers to accessing genetic information included logistical, economic, and psychological barriers, as well as barriers to understanding genetic information or identifying trustworthy sources. Study findings suggest a role for genetic counselors in addressing misconceptions relating to genetic testing, the genetic etiology of muscular dystrophy, and the impact of having a diagnosis on the patient's reproductive life, especially during adolescence and adulthood.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738251330413 - Supplemental material for Interests and Experiences of Young Adults with Muscular Dystrophy in Receiving Genetic Information
Supplemental material, sj-docx-1-jcn-10.1177_08830738251330413 for Interests and Experiences of Young Adults with Muscular Dystrophy in Receiving Genetic Information by Leah Hammond, Christina Ippolito, Kimberly Amburgey, David Chitayat, Stacy Hewson and Laura McAdam in Journal of Child Neurology
Supplemental Material
sj-pdf-2-jcn-10.1177_08830738251330413 - Supplemental material for Interests and Experiences of Young Adults with Muscular Dystrophy in Receiving Genetic Information
Supplemental material, sj-pdf-2-jcn-10.1177_08830738251330413 for Interests and Experiences of Young Adults with Muscular Dystrophy in Receiving Genetic Information by Leah Hammond, Christina Ippolito, Kimberly Amburgey, David Chitayat, Stacy Hewson and Laura McAdam in Journal of Child Neurology
Footnotes
Acknowledgements
We thank the young adults with muscular dystrophy who devoted time and effort to complete the online survey for this research study. Additionally, thank-you to the Duchenne Registry, Muscular Dystrophy Association, Muscular Dystrophy Canada, and the Hospital for Sick Children for assisting in participant recruitment and reviewing study materials. We acknowledge the contributions of Liz Mar, graphic designer with the Creative Services Studio at the Hospital for Sick Children, for their help with developing social media graphics for recruitment, and Bryan Maguire, statistician at the Hospital for Sick Children, for their support with data analysis.
Author Contributions
LH contributed to all aspects of the study, including conception and design, data collection, analysis and interpretation, and manuscript preparation and revisions. CI contributed to the interpreation of data and revised the manuscript. KA contributed to data analysis and interpretation, and manuscript revisions. DC contributed to data collection, analysis and interpretation, and revised the manuscript. SH contributed to the study design, interpretation of data, and manuscript revisions. LM contributed to all aspects of the study, including conception and design, data collection, analysis and interpretation, and manuscript preparation and revisions.
Consent to Participate
Participants provided informed consent to participate through submitting the survey.
Data Availability
Data Availability datasets generated during and/or analyzed during the current study are not publicly available as study participants did not consent to the secondary use of their data for research.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors LH, CI, SH, DC, and LM have no conflicts of interest. KA was an employee at Deep Genomics between July 2019 between April 2023 and continues in a consulting position (May 2023–present).
Ethical Considerations
This research was approved by research ethics boards at the Hospital for Sick Children (1000077815), Holland Bloorview Kids Rehabilitation Hospital (0465), and the University of Toronto (00041862).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Toronto MSc Genetic Counselling Fund and the University of Toronto Genetic Counselling Fund.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.