
Abstract
Balamuthia mandrillaris granulomatous amebic encephalitis is a rare disease that is associated with a high rate of mortality. Delays in diagnosis and treatment are common because of limited information on the organism in addition to its nonspecific clinical presentation. Prior reports have demonstrated that the encephalitis presents as multifocal lesions throughout the central nervous system with enhancement and edema. Here we report a case involving a 4-year-old previously healthy female child with a novel pathologic presentation of B mandrillaris infection, including vasculitis involving multiple large intracranial vessels as well as inflammation of multiple cranial nerves. The infection was ultimately fatal despite early diagnosis and initiation of targeted treatment.
Keywords
Balamuthia mandrillaris is a free-living ameba found in the environment that can rarely lead to a highly fatal encephalitis in both immunocompromised and immunocompetent hosts. B mandrillaris has only been reported as a cause of encephalitis in around 200 patients, 1 and is associated with a dismal mortality rate. 2 Because it is a rare infection, its pathogenesis is poorly understood, and its treatment has been challenging. It is believed to be acquired from the dirt through inhalation, and it infects the brain through hematogenous spread. 3 Dissemination along nerve fibers from the periphery to the brain has also been proposed. 4 The ameba uses multiple mechanisms to evade host immune responses, including suppression of cytotoxic T cells, and overexpression of immune factors by the host to increase blood-brain barrier permeability. 5 Once in the central nervous system, B mandrillaris employs metalloproteinases, phospholipase A2, and phospholipase D to facilitate the destruction and then engulfment of host cells.6,7 Clinical manifestation of this infection can be variable. Initial symptoms are often fever, headache, vomiting, and lethargy, which progress to include serious neurologic symptoms such as encephalopathy, seizures, and weakness. 2 Neuroimaging typically demonstrates multifocal lesions of enhancement and associated edema. 2 Treatment usually involves administration of multiple antimicrobials with in vitro activity against B mandrillaris. Often patients are treated with as many as 5 medications, and still have poor survival outcomes. 2 Here, we present the case of a young child who presented with acute onset hemiparesis and found to have developed a multifocal central nervous system vasculitis and encephalitis. To our knowledge, this represents the first report of B mandrillaris infection presenting as a central nervous system vasculitis.
Case Description
A 4-year-old previously healthy female child presented with acute onset of left facial droop, dysarthria, and left-sided hemiparesis. About 3 weeks before presentation, the patient had mild upper respiratory tract symptoms, intermittent headache, and fever up to 102°F. There had been no recent travel, no toxic exposures, and no known exposure to sick contacts. There was no personal or family history of autoimmune conditions, hypercoagulable states, sickle cell trait or disease, stroke, or epilepsy.
Brain magnetic resonance imaging (MRI) on day 1 of hospitalization showed diffusion restriction in the right caudate, putamen, corona radiata, and left putamen consistent with acute ischemia as well as an atrophic-appearing left basal ganglia (Figure 1). Vessel imaging showed bilateral mid-distal MCA and basilar artery stenosis with vessel wall contrast enhancement suggestive of vasculitis (Figure 2). There were chronic changes of periventricular T2 hyperintensities bilaterally. Notably, there was leptomeningeal enhancement bilaterally and questionable diffuse enhancement of bilateral cranial nerves (Figure 3).
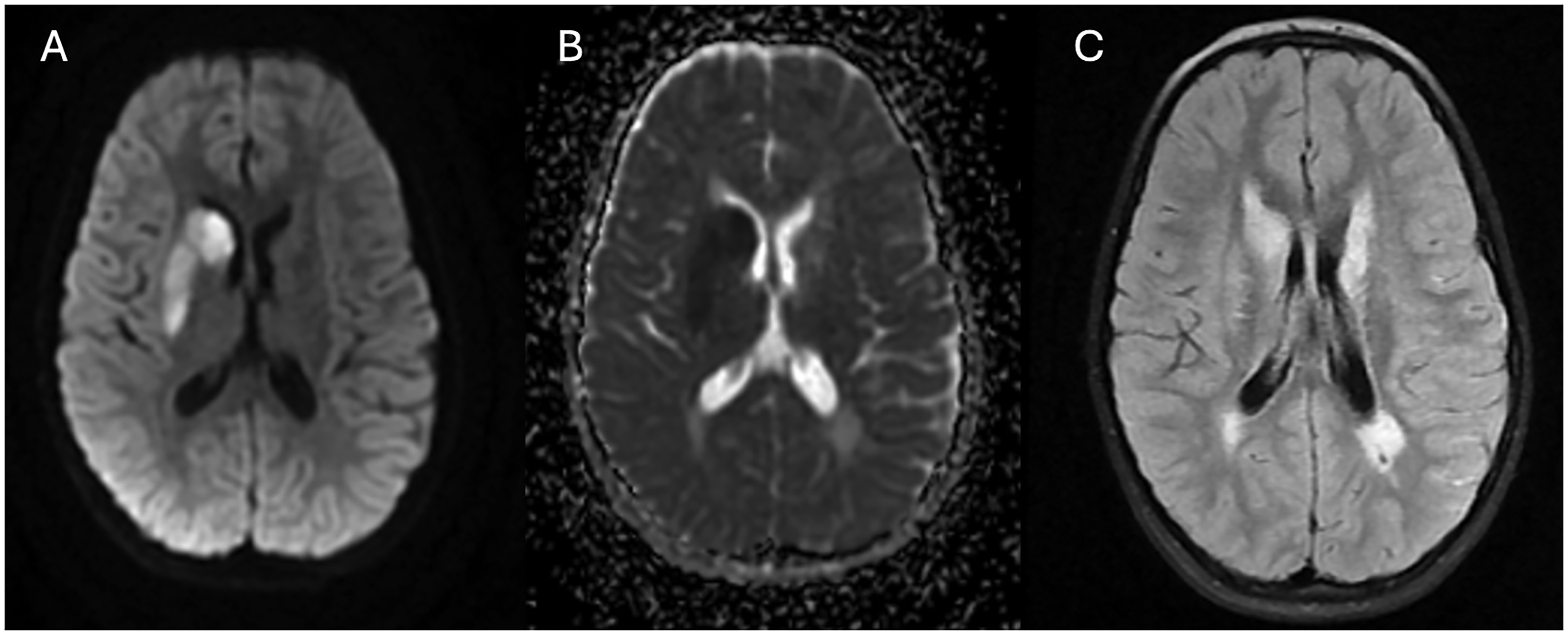
Neuroimaging findings of recurrent ischemic strokes in a patient with Balamuthia mandrillaris. Magnetic resonance imaging (MRI) of brain on day 1 of hospitalization showed (A) diffusion restriction in the right caudate, putamen, corona radiata, and left putamen (B) with associated ADC correlate consistent with acute ischemia as well as an atrophic-appearing left basal ganglia. (C) In addition, there are chronic changes of periventricular T2 hyperintensities bilaterally. ADC, apparent diffusion coefficient.
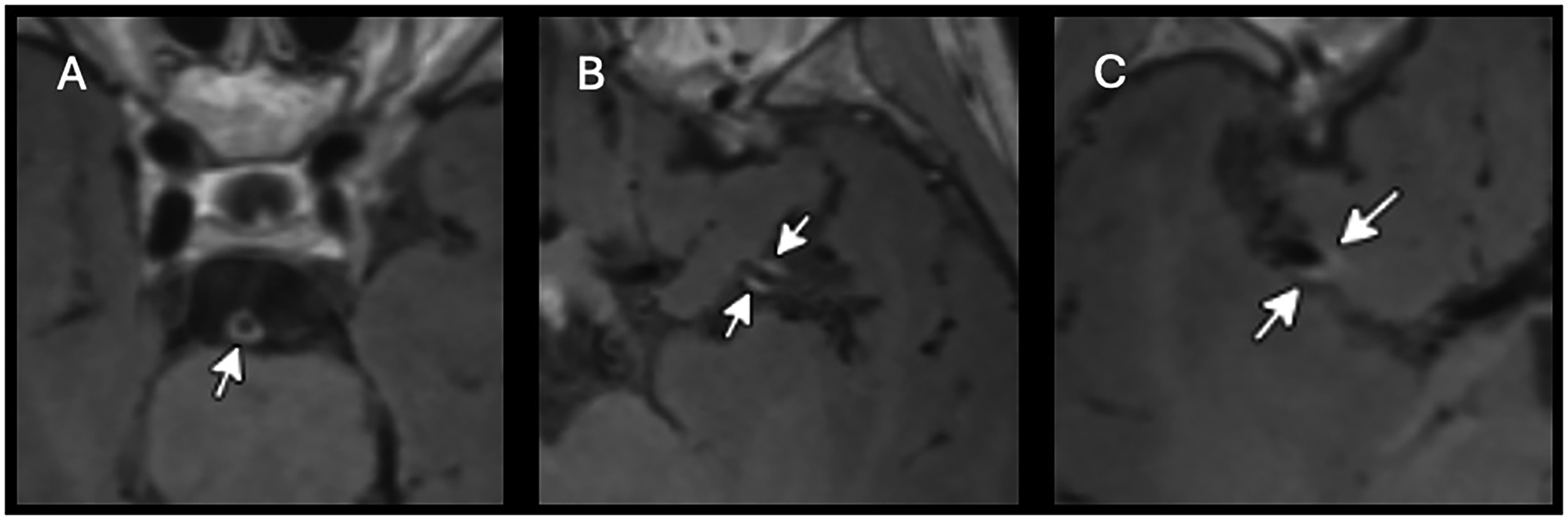
Neuroimaging findings of central nervous system vasculitis in a patient with Balamuthia mandrillaris. Magnetic resonance imaging (MRI) of brain with and without contrast with double inversion recovery (black blood sequence) demonstrated multifocal enhancement of the cerebral large arteries, including (A) basilar artery, (B) left middle cerebral artery, and (C) right middle cerebral artery.
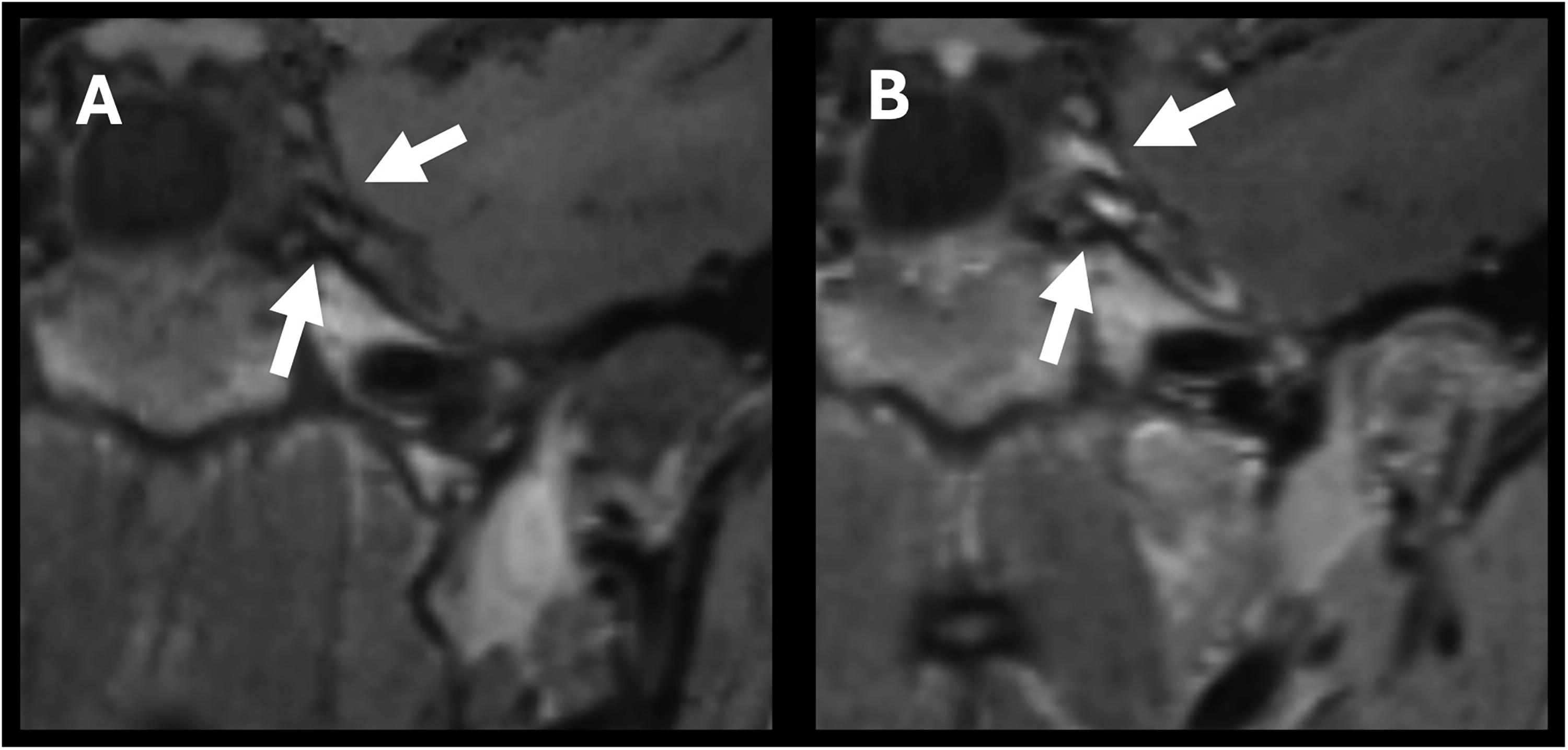
Neuroimaging findings of cranial nerve enhancement in a patient with Balamuthia mandrillaris. (A) Precontrast and (B) postcontrast magnetic resonance imaging (MRI) of brain demonstrated contrast enhancement of cranial nerves.
Initial cerebrospinal fluid studies were notable for lymphocytic pleocytosis, low glucose and elevated protein levels, and presence of oligoclonal bands. Initial testing for common infectious organisms for meningitis and encephalitis were negative, although Karius testing and cerebrospinal fluid metagenomics panel were pending.
Laboratory work was unremarkable, including autoimmune studies and hypercoagulable studies. Echocardiogram and transcranial Dopplers were unremarkable. Computed tomography (CT) of the chest and abdomen/pelvis showed no abnormalities or signs of vasculitis. EEG showed left occipital and right parieto-temporal sharp waves suggesting increased risk for seizures. The patient experienced a generalized tonic-clonic seizure on day 23.
Repeat brain MRI on day 3 showed the left putamen lesion was now ring-enhancing with a necrotizing-like appearance and newer small subcortical infarcts (Figure 4). Repeat cerebrospinal fluid studies showed worsening lymphocytic pleocytosis, hypoglycorrhachia, and increasing protein levels. Lip and salivary gland biopsy was pursued to identify potential sarcoidosis, which was negative.
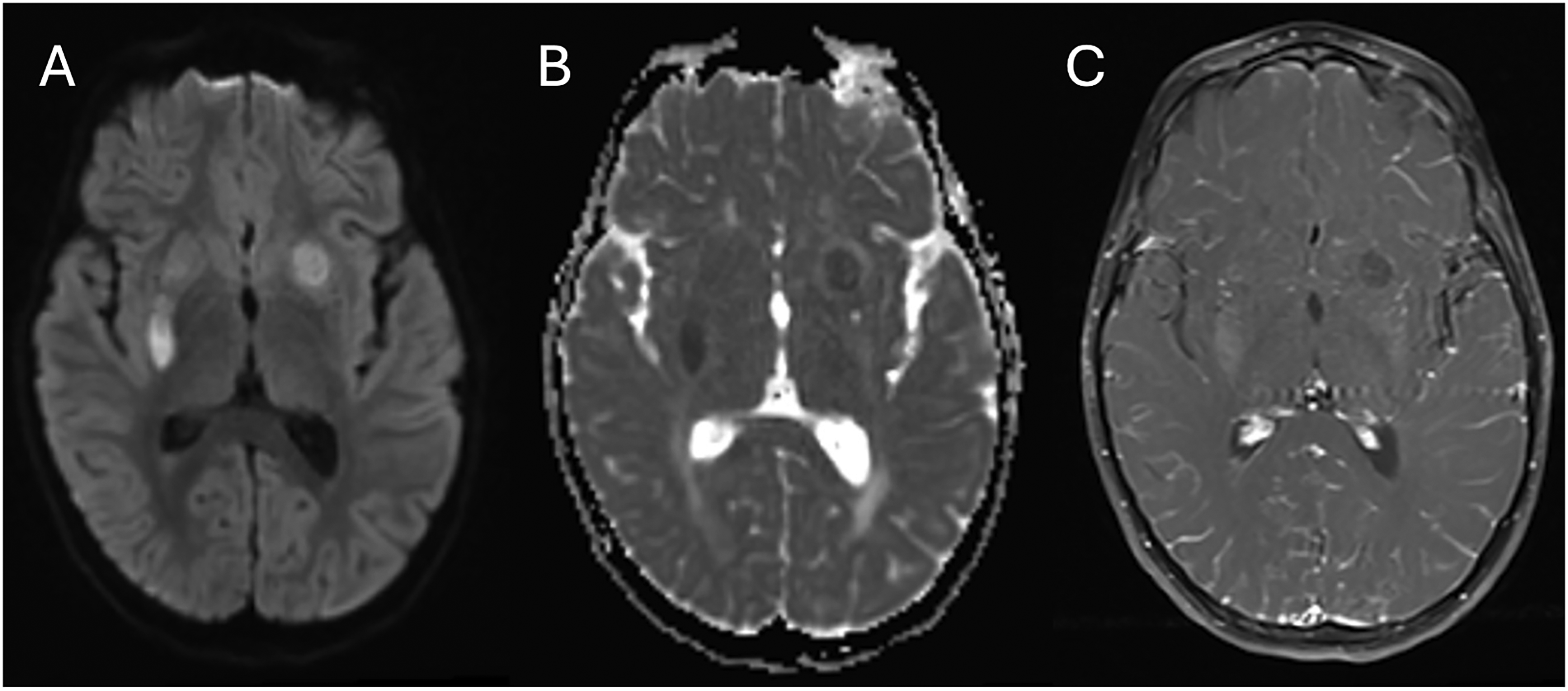
Neuroimaging findings of ring-enhancing lesion in a patient with Balamuthia mandrillaris. Repeat magnetic resonance imaging (MRI) of brain on day 3 of hospitalization demonstrated both that the left putamen lesion now is ring-enhancing (not shown) with central necrosis and there were newer small subcortical infarcts with (A) DWI sequence, (B) ADC sequence, and (C) T1 postcontrast sequence. ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging.
Karius testing from day 1 was reported on day 12 and demonstrated a positive result for B mandrillaris, which was further confirmed by cerebrospinal fluid polymerase chain reaction (PCR) test at the Centers for Disease Control and Prevention (CDC). Treatment was immediately initiated, which included fluconazole, azithromycin, and trimethoprim/sulfamethoxazole (Bactrim) on day 12, then adding flucytosine and miltefosine on day 13. Simultaneously, the process for institutional review board and CDC approval was initiated for an investigational new drug application for nitroxoline, a now out-of-use antibiotic previously used for urinary tract infection. This drug has had anecdotal success in treatment of Balamuthia encephalitis. This was started on day 27 of hospitalization.
On day 26 of hospitalization, repeat brain MRI was markedly improved, with decreased contrast enhancement, no evidence of abscess or ring-enhancing lesions, resolved restricted diffusion, stable right greater than left basal ganglia encephalomalacia, and improved residual vasogenic edema. Patient's clinical status remained stable although she was still endorsing mild headaches and cyclical fevers twice per day. On her discharge neurologic examination, she had no overt facial asymmetry, and full motor strength except for 4+/5 left grip strength and left knee extension, possibly limited by cooperation. She was discharged to home on day 42 on multidrug therapy.
The patient returned to the hospital 4 days later with worsening fevers, headache, photophobia, nausea, vomiting, and diarrhea. Repeat MRI demonstrated significant progression of patient's encephalitis with (1) nodular enhancement and thickening along the entire ventricular system with development of hydrocephalus, (2) new enhancing lesions in the midbrain, (3) enhancement of multiple cranial nerves, and (4) increased size of prior enhancing lesions in the basal ganglia and temporal and parietal lobe white matter with worsening vasogenic edema.
During this hospitalization, the patient required ventriculostomy placement to treat the hydrocephalus, and the antimicrobial regimen was continued. The patient became progressively encephalopathic and was transitioned to comfort-focused care 2 weeks into this hospitalization. The patient died due to respiratory compromise 57 days from the initial presenting symptoms.
Discussion
B mandrillaris encephalitis can affect both immunocompromised and immunocompetent patients with high rates of mortality. Our limited understanding of the pathogenesis and clinical presentation of this organism leads to delays in diagnosis and treatment. In the rare case that the organism is identified early enough, current treatments are still largely inadequate because of an incomplete understanding of the pathophysiology of this pathogen. 1 As it is a rare cause of encephalitis, increased reporting, and evaluation of B mandrillaris encephalitis is critical. This report describes the case of a 4-year-old child who developed novel neuroimaging findings of B mandrillaris central nervous system vasculitis and encephalitis.
A novel aspect of this patient's presentation was the extensive central nervous system vasculitis evident on neuroimaging early in the disease course. To our knowledge, this is the first case demonstrating central nervous system vasculitis as the presenting pathology for B mandrillaris infection. There was multifocal enhancement of the vessel walls of bilateral middle cerebral arteries and the basilar artery with associated stenosis. This impressive vasculitis initially prompted a high suspicion for a rheumatologic etiology such as primary central nervous system angiitis, and high-dose steroids were considered. Fortunately, steroids were not started until results from infection studies had arrived. Treatment with steroids presumably would have hampered the patient's ability to mount an immune response to the infection.
Another compelling aspect of the patient's neuroimaging is that there was leptomeningeal enhancement and diffuse enhancement of bilateral cranial nerves, which prompted additional evaluation for neurosarcoidosis. These neuroimaging findings have not been commonly described for B mandrillaris as other findings such as acute ischemia, hemorrhagic lesions, and ring-enhancing lesions 2 that were also present for this patient. The patient's neuroimaging was also quite unique in that there was chronic-appearing extensive small vessel white matter hyperintensities that were aged to be present for years despite the patient's young age and no prior health issues. Although the clinical presentation appeared acute, there may have been a chronic disease process present that may either have predisposed the patient to this infection or perhaps was the infection itself that was latent for months to years.
Despite extensive encephalitis and vasculitis throughout multiple large central nervous system vessels, the patient surprisingly presented with minimal neurologic symptoms out of proportion to the cerebrospinal fluid findings and neuroimaging. This suggests that the patient presented early in the disease course. The patient was treated with fluconazole, azithromycin, trimethoprim/sulfamethoxazole, miltefosine, and nitroxoline. There was initially a stabilization of the patient's neuroimaging and improvement in the patient's symptoms. Unfortunately, the patient's encephalitis rapidly progressed, and the patient succumbed to this infection just 2 months from initial presentation. Other studies have anecdotally suggested that early diagnosis and treatment of B mandrillaris is a critical feature to improve survival. 2 Our case underscores the urgent need for the development of more rapid diagnostics and more effective treatments for B mandrillaris encephalitis.
Conclusion
B mandrillaris infection causes a rare and deadly encephalitis because of its aggressive nature and is often not identified until postmortem because of delays in diagnosis and treatment. B mandrillaris was diagnosed early in the clinical course and treated early with a multidrug regimen including nitroxoline. Despite early diagnosis and initiation of a multidrug regimen, the patient did not respond adequately to treatment and the infection rapidly became fatal. This case of a young previously healthy child was novel in its findings of central nervous system vasculitis and cranial neuropathy as early signs of infection. Given the severity of this disease, there is a dire need to develop more effective treatments.
Footnotes
Author Contributions
JA and KP drafted the manuscript. JA generated the figures. JA, TK, and KP reviewed the manuscript. JA and KP performededits based on peer review comments.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.