
Abstract
We describe a series of 7 toddler-aged children with iron deficiency anemia from excessive cow's milk consumption who presented with cerebral venous sinus thrombosis and no other identifiable risk factors for thrombosis. The deep venous system was involved in 6 patients, 6 had venous infarcts, and 5 have significant neurocognitive sequelae.
Keywords
Consumption of more than 17 ounces (500 mL) of cow's milk per day is a predictor of iron deficiency anemia (IDA) in young children. 1 The iron content of cow's milk is low, and absorption of iron is inhibited by the calcium and protein components found in cow's milk. In addition, cow's milk–induced enterocolitis can lead to significant intestinal blood loss in some children. Iron deficiency anemia peaks in toddlers 2 and is associated with cognitive sequelae. In the United States, 7.1% of children aged 1-5 years are iron deficient, and 1.1% have iron deficiency anemia. 3
Cerebral venous sinus thrombosis in children with excessive cow's milk intake and iron deficiency anemia has been reported in case reports and small case series (Table 1).4-12 Most of these reports describe reassuring outcomes following cerebral venous sinus thrombosis, although mild motor sequelae and seizures have been reported.5,7 In adults, anemia is a known risk factor for cerebral venous sinus thrombosis, with a stronger association in men than women, 13 and it is also a risk factor for poor outcome following cerebral venous sinus thrombosis. 14
Previous Reports of Children With Excessive Cow's Milk Intake, Anemia, and CVST.
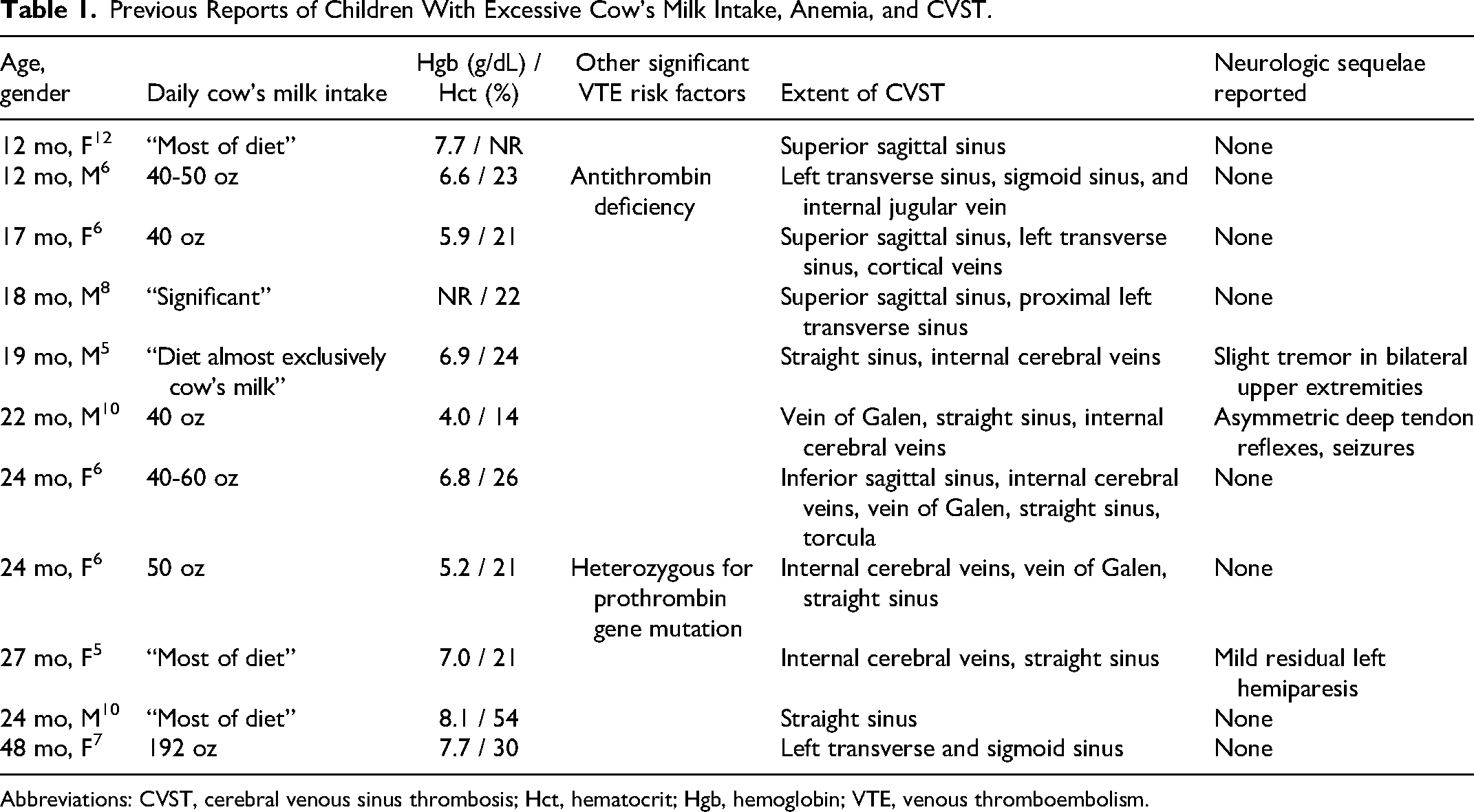
Abbreviations: CVST, cerebral venous sinus thrombosis; Hct, hematocrit; Hgb, hemoglobin; VTE, venous thromboembolism.
Methods
We performed a retrospective study of all children seen at Seattle Children's Hospital between January 2009 and March 2023 with cerebral venous sinus thrombosis, iron deficiency anemia, and no other identified risk factors for thrombosis. Charts and imaging reports of patients identified using diagnostic codes for cerebral venous sinus thrombosis were reviewed to confirm diagnosis. Chart review was used to extract data about clinical presentation, neuroimaging, and outcome. The study was approved by the Seattle Children's institutional review board.
Results
Seven children (15, 17, 33, and 42 months old boys, and 18, 24, and 38 months old girls) had cerebral venous sinus thrombosis, iron deficiency anemia, and apart from some degree of dehydration at presentation, likely due to the cerebral venous sinus thrombosis, no other significant cerebral venous sinus thrombosis risk factors (Table 2). Four had symptoms of viral upper respiratory tract infection within the 2 weeks preceding presentation. All were initially suspected of having viral gastroenteritis as they presented with recurrent emesis and malaise. Two had breath-holding spells at presentation.
Patients With CVST Due to Iron Deficiency Anemia.
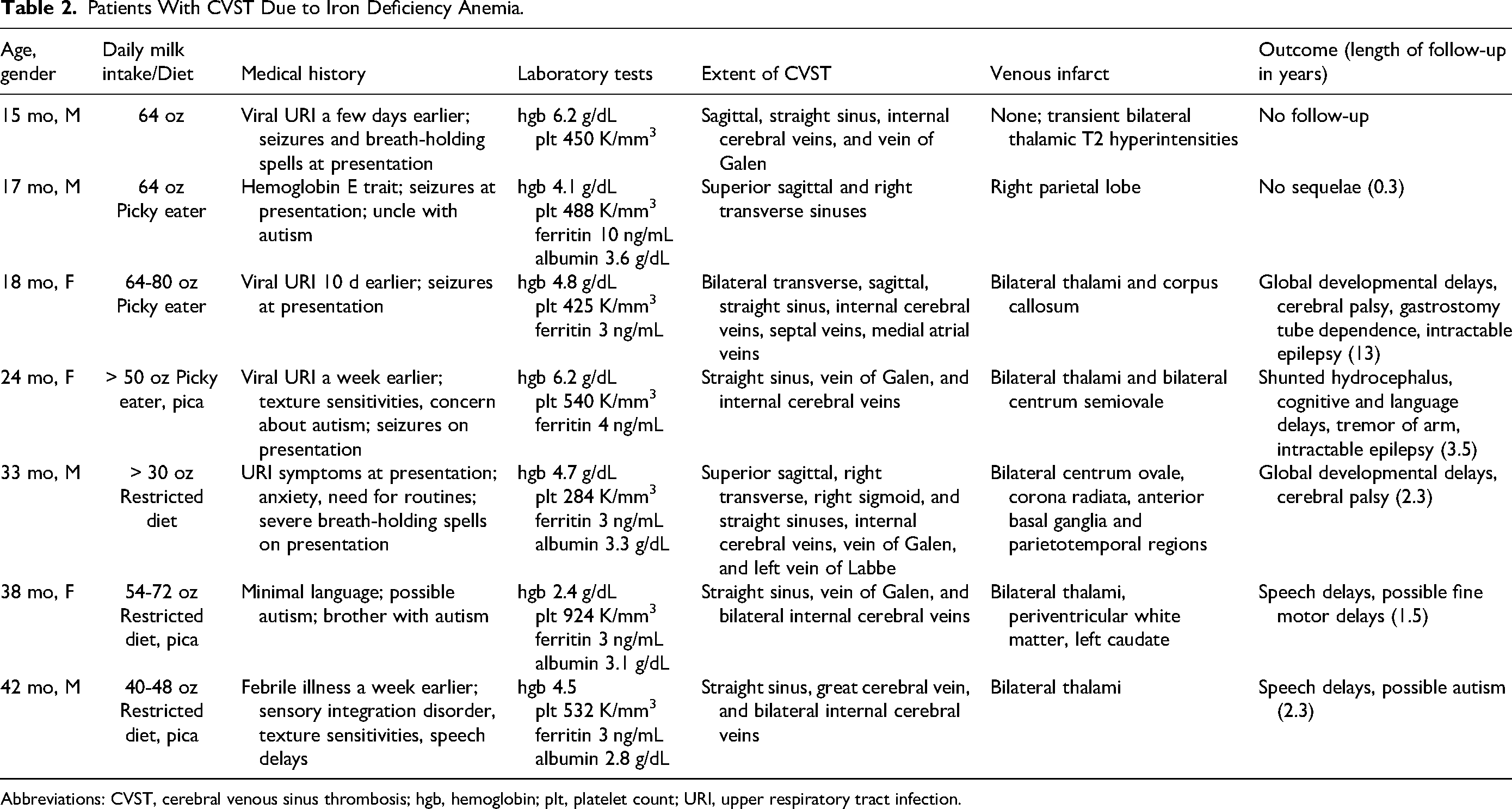
Abbreviations: CVST, cerebral venous sinus thrombosis; hgb, hemoglobin; plt, platelet count; URI, upper respiratory tract infection.
Six patients had full laboratory testing for the most common inherited thrombophilias identified in pediatric venous thromboembolism: Factor V Leiden, prothrombin gene mutation, protein C activity, free protein S antigen, and antithrombin activity. One had a more limited thrombophilia evaluation, with only protein C activity, free protein S antigen, and antithrombin activity. Six of the 7 patients had also had an antiphospholipid panel performed. None of the patients had any positive thrombophilia testing. None had a documented central nervous system infection or cerebrovascular abnormalities. One patient had a history of hemoglobin E trait, which is not associated with risk for thrombosis.
Milk intake ranged from 30 to 80 oz/d. Hemoglobin at presentation ranged from 2.4 to 6.2 (median 4.7) g/dL, platelet count 284 to 924 (median 488) K/mm3, ferritin from 3 to 10 (median 3) ng/mL, and albumin 2.8 to 3.6 (median 3.2) g/dL. The deep venous system was involved in 6 patients, including straight sinus and bilateral internal cerebral vein involvement. Six patients suffered venous infarcts, including thalamic infarcts and deep white matter infarcts (Figure 1). Venous stroke was present in 86% (6/7) of children with cerebral venous sinus thrombosis due to isolated iron deficiency anemia, in contrast to 28% (45/158) of the entire cerebral venous sinus thrombosis cohort.
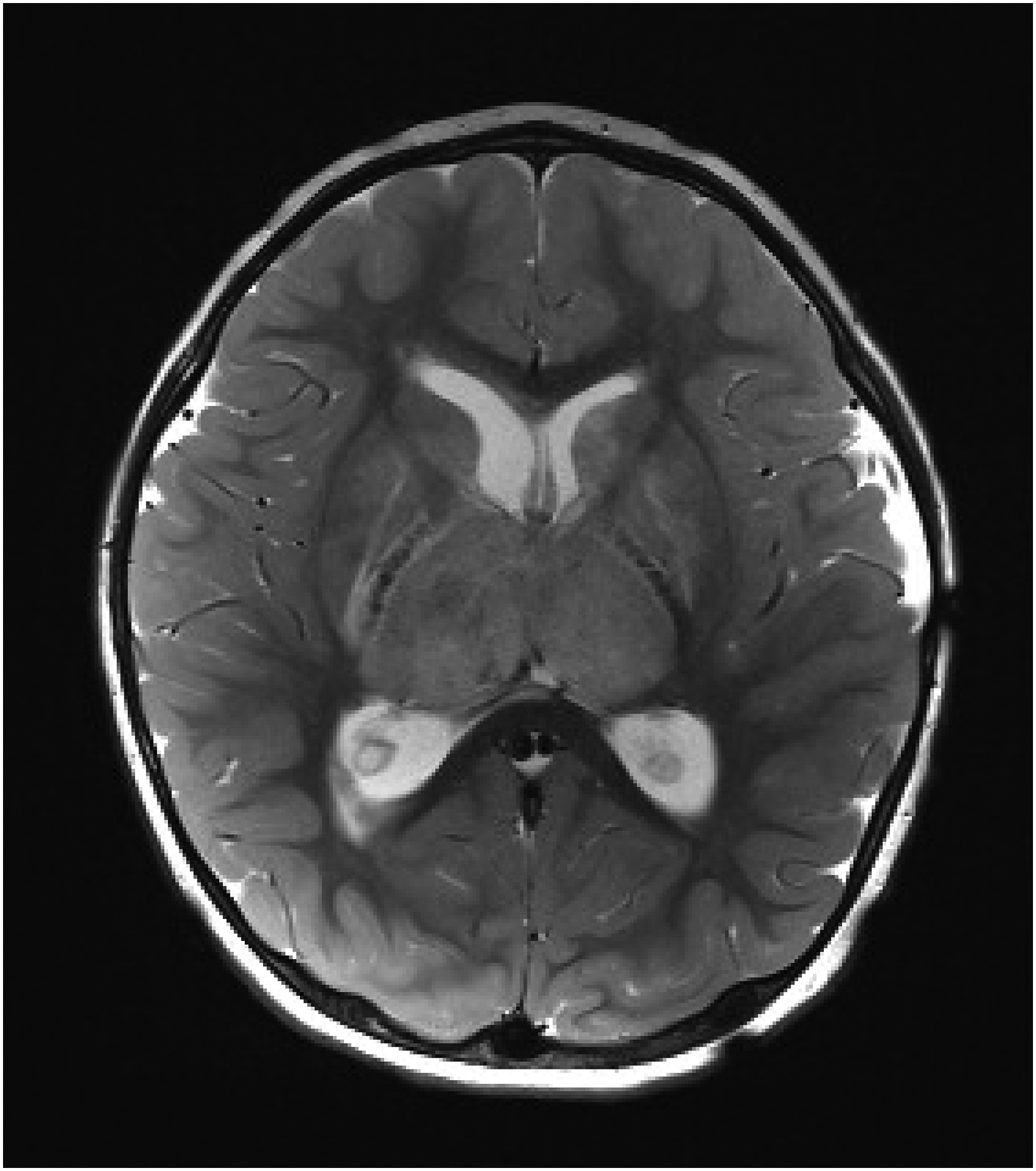
Axial T2-weighted magnetic resonance imaging (MRI) scan from a 24-month-old female with iron deficiency anemia and cerebral venous sinus thrombosis showing edema due to venous infarcts of the right greater than left thalami and obstructive hydrocephalus at the level of the third ventricle secondary to thalamic swelling.
All 7 of the children with cerebral venous sinus thrombosis had a very limited diet. The 4 oldest children all had behavioral and developmental concerns other than a limited diet, including sensory integration disorder in 1 patient, and autism in 2 patients. All but the 15-month-old and 17-month-old required rehabilitation services and have significant neurocognitive sequelae, including cerebral palsy in 4 patients, refractory epilepsy in 2 patients, and cognitive and/or language delays in 5 patients (Table 2).
Discussion
An association between iron deficiency anemia and cerebral venous sinus thrombosis has been described, but the pathophysiology of thrombus formation and propagation in iron deficiency is not well understood. 15 One factor often cited is the development of thrombocytosis in the iron-deficient state, because low iron levels bias the commitment of progenitor cells in the bone marrow toward the platelet precursor cells, the megakaryocytes. 16 Only 1 of the patients in our study had a significantly elevated platelet count, suggesting this mechanism did not play a significant role. There are studies of platelet aggregation in children with iron deficiency anemia with conflicting results, with one showing increased response to ADP and collagen 17 and a more recent study that does not confirm these findings. 18 A study in premenopausal women showed the opposite effect, with lower platelet reactivity and adhesion under flow while iron deficient compared with the iron replete state. 19 Iron deficiency causes defects in the red cell membrane and decreased red cell deformability, which leads to abberant shear stress and vascular damage, which could also be an important contributor to thrombosis risk. 20
Patients in our study also had hypoalbuminemia at presentation, which could be due to protein loss in the gastrointestinal tract because of subclinical enterocolitis associated with cow's milk. Enterocolitis, along with the relatively low free water content of cow's milk compared with other fluids, could also predispose to thrombosis because of an inability to compensate during dehydrating events such as diarrhea or vomiting.
Our study suggests cerebral venous sinus thrombosis associated with excessive cow's milk intake may be a more severe form of cerebral venous sinus thrombosis that often involves the deep venous system. Unlike previous reports, most patients in our study had significant neurocognitive sequelae. The poor outcomes in the patients in our study were attributable to cerebral venous sinus thrombosis as opposed to other direct central nervous system injury, and severe iron deficiency due to excessive cow's milk intake was the only significant provoking factor identified. In the United States, whole cow's milk is typically introduced into the diet at 12 months of age, with a recommended limit of 16-24 ounces per day. Young children with high cow's milk intake, particularly those with poor intake of iron-containing solid foods, or atypical development should be screened early for iron deficiency. Delayed diagnosis of cerebral venous sinus thrombosis due to presentation with nonspecific symptoms similar to those of gastroenteritis likely contributed to the poor outcomes in our study. There should be a high index of suspicion for cerebral venous sinus thrombosis in toddlers with severe cow's milk anemia presenting with recurrent emesis and malaise.
Footnotes
Author Contributions
The authors contributed equally in concept design, data analysis, and drafting of the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Seattle Children's Institutional Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.