
Abstract
Pediatric stroke is caused by a blockage or a rupture of the blood vessels in the brain and differs from adult stroke in clinical presentation, etiology, risk factors, and outcomes. 1 More than half of all strokes in children are arterial ischemic strokes (AIS), making up 70% of all ischemic strokes in children. 1 Arterial ischemic stroke is due to an interruption of blood flow to the brain, in an arterial distribution secondary to the occlusion of the cerebral arteries. 2 Arterial ischemic stroke presents as a focal neurologic deficit in 61% of cases. 3 There are important differences in etiology and outcome based on child's age at stroke onset, which is typically categorized into neonatal stroke (from 28 weeks’ gestation to 28 postnatal days of life) or childhood stroke (from 28 postnatal days to 18 years of age). 4
Cognition and language development is often negatively affected by arterial ischemic stroke. When most domains of language are considered (including phonology, semantics, syntax, discourse and literacy), children with strokes during the neonatal period up to the first year of life have worse language outcomes, compared to childhood stroke. 5 An inverted U–shaped trajectory for outcomes following stroke based on age of injury has also been reported by some, whereby the youngest children are worse affected, children aged 2-6 years of age report the best outcomes and older children have increasingly worse outcomes with older age. 6 Another U-shaped curve is recorded in a large retrospective 2-year, follow-up study conducted by Felling and colleagues (2020), which found young infants—specifically those aged 28 days up to 1 year at stroke onset—had the worse outcomes of all children. 7 Language outcomes for children sustaining neonatal strokes in either hemisphere are similar, 8 whereas in childhood stroke, language impairments after left hemisphere damage are reportedly similar to adults. 9 Younger age at stroke (before first year of life) was also found to be a predictor of worse cognitive outcomes,10,11 particularly when response inhibition, divided attention, switching, sustained attention, and other executive function (spared in verbal fluency and design fluency 5 ) evaluations are considered.12–14 Similar to language, the effect of lesion laterality on cognitive outcomes has proven inconsistent. 13 Risk factors for worse cognitive outcome include larger lesion volume, 12 infarcts affecting cortical and subcortical regions, 10 and infarcts involving both small and large vessel territories. 7
Research concerning the effects of specific demographic and psychosocial factors on cognitive and behavioral outcomes in pediatric stroke is emerging. 15 Environmental factors such as family functioning 15 and socioeconomic status16,17 have been found to affect social and neurologic outcomes in children following stroke. However, an unexplored area that remains is the sociolinguistic factor of bilingualism. Bilinguals, or individuals who are learning and using 2 or more languages, make up an estimated half of the world's population. 18 Although a prior belief was that learning 2 languages would have a negative impact on development, recent research demonstrates that neurotypical monolingual and bilingual children reach the developmental milestones of language and cognition at the same pace. 19 Moreover, it has been proposed that a bilingual environment might afford certain benefits cognitively and linguistically. 20 According to the Bilingual Cognitive Advantage hypothesis, the mental exercise related to using 2 languages (e.g., activating the appropriate language and switching between languages) can positively affect nonlinguistic cognitive functions. 21 Recent meta-analyses support the existence of a bilingual advantage in the executive functions of neurotypical pediatric populations. 22 Childhood bilingualism is also associated with linguistic advantages. Specifically, considering metalinguistic abilities, bilinguals consistently outperform their monolingual peers. 23 Bilingualism may also facilitate language production skills, such as novel word learning in bilingual school-aged children. 24 Although there is an ongoing debate about the existence of the bilingual advantage, the current work intends to move beyond the dichotomy of “advantage” vs “no advantage” and focus on how bilingual exposure may interact with (cognitive and/or language) development in populations with neurologic deficits, such as children with arterial ischemic stroke.
Bilingualism has been evaluated in adults with stroke, with mixed results. Alladi and colleagues 25 identified bilingualism as an independent predictor of poststroke cognitive impairment, as they reported better cognitive outcomes for bilinguals (higher proportion of “normal” cognition) over monolinguals. Hope et al 26 found that lesion damage to language-related regions of the brain was associated to language skills in both monolingual and bilingual groups, but the lesion-deficit association was more consistently recorded in the bilingual group. Predictions from prognostic models using monolingual lesion-behavior data did not suit bilingual patients, as language outcomes tended to be poorer in the bilinguals than predicted by the monolingual model. 26 Although in principle, monolingual models should not be used for bilinguals, as they are expected to have different processing skills. 27
Here, we investigate language and cognitive development following ischemic stroke in children with bilingual and monolingual exposure across age at stroke onset groupings. This is important, as speaking 2 languages at home and having low English-proficiency parents are associated with adverse child health outcomes 28 ; limited English-proficiency pediatric patients also experienced care-related disparities associated to their language use. 29 Research concerning bilingual exposure in the pediatric stroke population and guidelines available to clinicians are scarce. Thus far, the only study that examined bilingual pediatric stroke participants, with the sample including 5 of 6 children raised in a bilingual environment, did not include a control group of monolinguals. 30 In this primarily bilingual sample, Francois et al 30 found that left perinatal stroke patients showed larger right lateralized structural and functional connectivity of the dorsal language pathway, which was associated with better language outcomes. To date, we are not aware of any studies with an explicit focus on bilingual exposure and stroke outcomes in children.
The Current Study
The specific objective of this study is to evaluate poststroke language and cognitive outcomes of children with monolingual and bilingual exposure across 3 stroke-onset groups, using the Pediatric Stroke Outcome Measure (PSOM). Given that bilingual exposure during childhood is not associated with any known negative outcomes in terms of linguistic and cognitive development in neurotypical children, we hypothesized that bilingual exposure in pediatric stroke patients would likewise not have any negative consequences. We predicted that the Pediatric Stroke Outcome Measure follow-up scores of bilingual children would likely be comparable to the scores of their monolingual peers. Further, considering the cognitive and linguistic advantages observed in bilinguals, it is a possibility that bilingual patients would outperform their monolingual peers in certain Pediatric Stroke Outcome Measure subscales (e.g., language and cognitive/behavioral subscales). However, this could be only the case if the stroke occurred outside of the neonatal period (from 28 days of birth onward), 11 as only beyond this time frame would this allow for sufficient bilingual exposure pre- and poststroke.
Methods
Patients
Patients enrolled in the Hospital for Sick Children (SickKids; Toronto, Canada) Stroke Registry between January 1, 2008, and December 1, 2019, were considered for the study if they were first-ever arterial ischemic stroke patients aged 0-17 years at stroke. Exclusion criteria included presumed perinatal arterial ischemic stroke; multiple diagnoses of stroke (e.g., stroke recurrence or different stroke types followed by arterial ischemic stroke); prior diagnosis of select neurologic comorbidities (trisomy 21, nonverbal autism); and fewer than 2 Pediatric Stroke Outcome Measure evaluation scores available poststroke.
Language information and outcome measure data were retrieved from the SickKids Stroke Registry. First and second language (and other languages, if applicable) and any described use or exposure were abstracted from the stroke and neuropsychological clinic visit notes and medical charts. As no measure of language proficiency was available in the charts, proficiency was not considered. The monolingual group was composed of children who were exposed to one language only from birth. The bilingual group was defined by concurrent learning or exposure to at least 2 languages (e.g., one heritage/home language and one societal language). Given the sociocultural context of Canada, bilingual children would have had exposure to English (and/or less commonly, French) from birth, while another language may be either simultaneously exposed, as in the case of a heritage language or sequentially exposed, later with formal schooling (usually at age 4 years for the start of preschool). Children who began to learn a second language in school settings, a typical experience for sequential bilinguals, and children who were exposed to more than 2 languages (multilingual children) were both subsumed within the bilingual group. Given that both simultaneous and sequential bilinguals have been associated with cognitive and linguistic advantages, both types of bilinguals were grouped together for analysis.31,32
Previous literature evaluating outcomes using the Pediatric Stroke Outcome Measure indicated that emerging deficits were more common in recovery patterns of children younger than 1 year at stroke onset. 7 Felling and colleagues (2020) found that in their multivariate analysis, only infants 28 days to 1 year at stroke onset were predictive of worse overall Pediatric Stroke Outcome Measure outcomes. Further lending support for dividing the childhood stroke group, language and cognitive Pediatric Stroke Outcome Measure outcomes also showed similar differences, whereas the sensorimotor domains were less sensitive to age at stroke onset. 7 Although various research use differing groupings based on age, patients in this sample were stratified into 3 “age at stroke onset” groups motivated by the recovery patterns in studies also using the Pediatric Stroke Outcome Measure. These were neonates, <28 days; first-year, 28 days to 12 months; and childhood, 13 months to 18 years. Using Kruskal-Wallis test, our preliminary analyses evaluating this grouping also corroborated these differences using the Pediatric Stroke Outcome Measure, H(2) = 12.15, P < .002, indicating a significant difference between the 3 groups.
Pediatric Stroke Outcome Measure
The Pediatric Stroke Outcome Measure is a standardized, structured pediatric neurologic examination composed of 115 test items and summarized into 5 subscales; Right Sensorimotor, Left Sensorimotor, Language Production, Language Comprehension, and Cognitive/Behavioral subscales.33, 34 Each Pediatric Stroke Outcome Measure subscale is scored on a range from 0 (no deficit), 0.5 (mild deficit), 1 (moderate deficit), to 2 (severe deficit), with a total Pediatric Stroke Outcome Measure out of 10, considering the sum of all 5 subscales. A greater score is indicative of worse outcome. The Pediatric Stroke Outcome Measure takes into consideration the administering neurologist's observations (partially based on age-appropriate language and cognitive tasks), parent report and medical chart information (e.g., clinic notes, neuropsychological assessment—including standardized language and cognition measures).
Currently, the Pediatric Stroke Outcome Measure is the only available standardized neurologic examination of outcome specific to the pediatric stroke population. 33 The Pediatric Stroke Outcome Measure's construct validity and reliability have been established against standardized neuropsychological measures, evaluating the content or domains matched to each subscale. 33 Performances on the language production subscale were significantly correlated to standardized assessments of verbal fluency, expressive vocabulary, and parental reports of functional communication. Performances on the language comprehension subscale were correlated to standardized measures of receptive vocabulary and parental reports of functional communication. The above subscales were not correlated with verbal IQ, suggesting that the Pediatric Stroke Outcome Measure language subscales do not evaluate general cognitive functioning but the language domains. The performance on the cognitive/behavioral subscale was found to be significantly associated with standardized measures of overall intellectual ability, verbal reasoning, perceptual reasoning, mental manipulation of information, visuomotor processing speed, parent-reported executive function, behavior regulation, social skills, and functional independence at home. 33 It is noted that given the differences in the way these tests are measured, the Pediatric Stroke Outcome Measure represents an effective screening tool and is ideal for use in outcome-related research,7,33,35 although neuropsychological measures allow for more detailed evaluations, though not as well positioned to be administered on a larger scale.
Pediatric Stroke Outcome Measure scores used in the current study were collected at hospital discharge and in the follow-up clinics at regularly scheduled intervals, in keeping with the hospital's neurology program. These were on average at 3-6 months and 12 months poststroke, then at 1-2-year intervals after the first year up to 18 years of age, when children were transitioned to adult care. In our current sample, a minimum of 2 test time points of the Pediatric Stroke Outcome Measure were necessary and ranged up to 10 time points for all patients; follow-up was at minimum 2 months poststroke, up to a maximum of 10 years poststroke based on the scheduled clinic visits. The statistical analysis accounted for the variability in the follow-up intervals, given that some patients were not always available as scheduled (because of distance from hospital and other commitments).
Statistical Analysis
Anonymized data are available openly at https://doi.org/10.5683/SP2/E3ECVD and were analyzed in Jamovi (version 1.6.6, The jamovi project, 2020, https://www.jamovi.org/). Growth curve modeling, a mixed effects model including time point (month at test from stroke onset) as a predictor was used to analyze the relationship between language group and outcome.36,37 In our analyses, we focused on the cognitive/behavioral, language production (i.e., language expression), and language comprehension (i.e., language reception) Pediatric Stroke Outcome Measure subscales. A Combined Language subscale was calculated through sum of the scores from the language production and comprehension subscales. We fit linear mixed models for each Pediatric Stroke Outcome Measure subscale as outcome variables, using time point (month at test from stroke onset), language group (monolingual, bilingual), age at stroke onset (neonate, first-year, childhood), sex (female, male), laterality (right, left, bilateral), and its interaction as fixed effects, with participant as random effect (see Supplementary Materials for full models and additional results related to sex and laterality, which are generally in line with findings reported in previous literature).
Here, we report only models relevant to our hypothesis. These models include time point (month at test from stroke onset; each child was evaluated at multiple time points after stroke onset, up to 10 years), language group (monolingual vs bilingual status), age at stroke (neonate, first-year, childhood), and its interactions. The time point variable was assigned a specified loading in the model, based on the month after stroke at test, and was also used as a random variable when fit improved. All models included participant as random effect. Maximum likelihood method of estimation was used, and model fit was evaluated using Akaike information criterion and Bayesian information criterion values. Statistical analyses and reporting have been done in consultation with an institutional statistician.
Results
Study Cohort
A total of 253 children with arterial ischemic stroke met our inclusion and exclusion criteria. Of these patients, 3 additional patients were excluded because of chart unavailability; 13 deceased patients had residual data in the registry and were excluded. The final study sample totaled 237 children. The demographic and stroke characteristics of all children are available in Table 1. The sample consisted of monolingual (n = 111) and bilingual patients (n = 126). This distribution is in line with Statistics Canada's (2016) reports of 4 in 10 households speaking more than one language at home, with this proportion increasing for larger metropolitan areas. 38 Although the language group distribution is fairly comparable in the neonate and first-year age at stroke groups, the childhood group had more monolinguals than bilinguals. Also, the first-year group had the smallest number of patients (only 14% of the whole sample) compared to the other groups. Socioeconomic status (SES) was available for a subset of the sample and was evaluated by calculating a composite SES score based on annual income and parents’ highest level of education. A Mann-Whitney test found no difference between monolinguals and bilinguals in socioeconomic status (U = 867.50, P = .65). More details on the languages used by the bilinguals and stroke type are available in the supplementary materials.
Patient Demographicsa and Stroke Characteristics for Monolingual and Bilingual Participants.
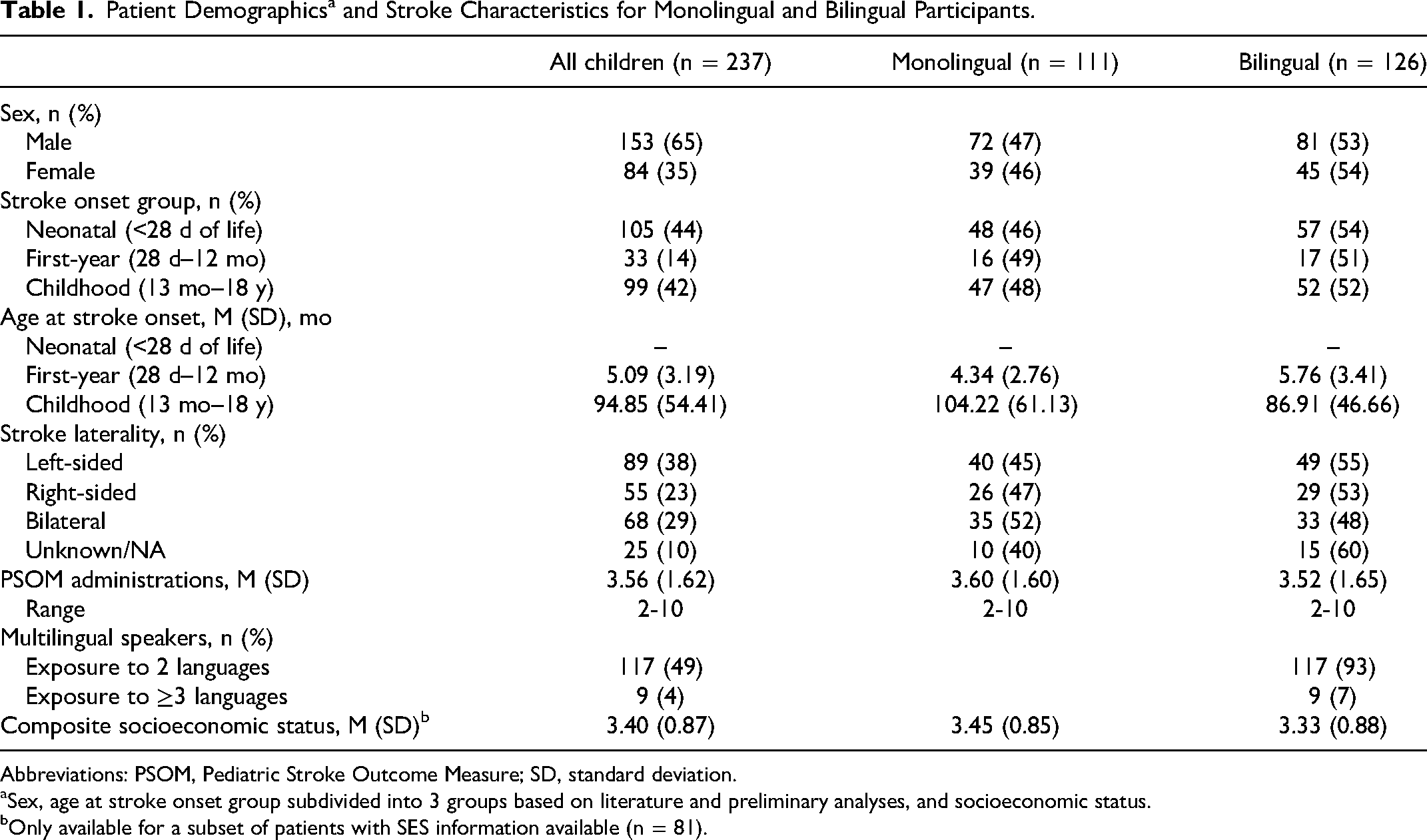
Abbreviations: PSOM, Pediatric Stroke Outcome Measure; SD, standard deviation.
Sex, age at stroke onset group subdivided into 3 groups based on literature and preliminary analyses, and socioeconomic status.
Only available for a subset of patients with SES information available (n = 81).
Cognitive/behavioral subscale.
We modeled cognitive development as predicted by language group, age at stroke group, and its interaction, with the time point variable added in as an additional fixed variable and random slope (along with participant) to increase model fit. Although language group was nonsignificant, age at stroke was a significant predictor of cognitive/behavioral Pediatric Stroke Outcome Measure scores, such that Pediatric Stroke Outcome Measure was seen to increase incrementally, with an older age at stroke indicating a worse outcome: the neonatal group had the lowest Pediatric Stroke Outcome Measure scores, whereas the childhood group had the highest Pediatric Stroke Outcome Measure scores (Table 2; Figure 1).
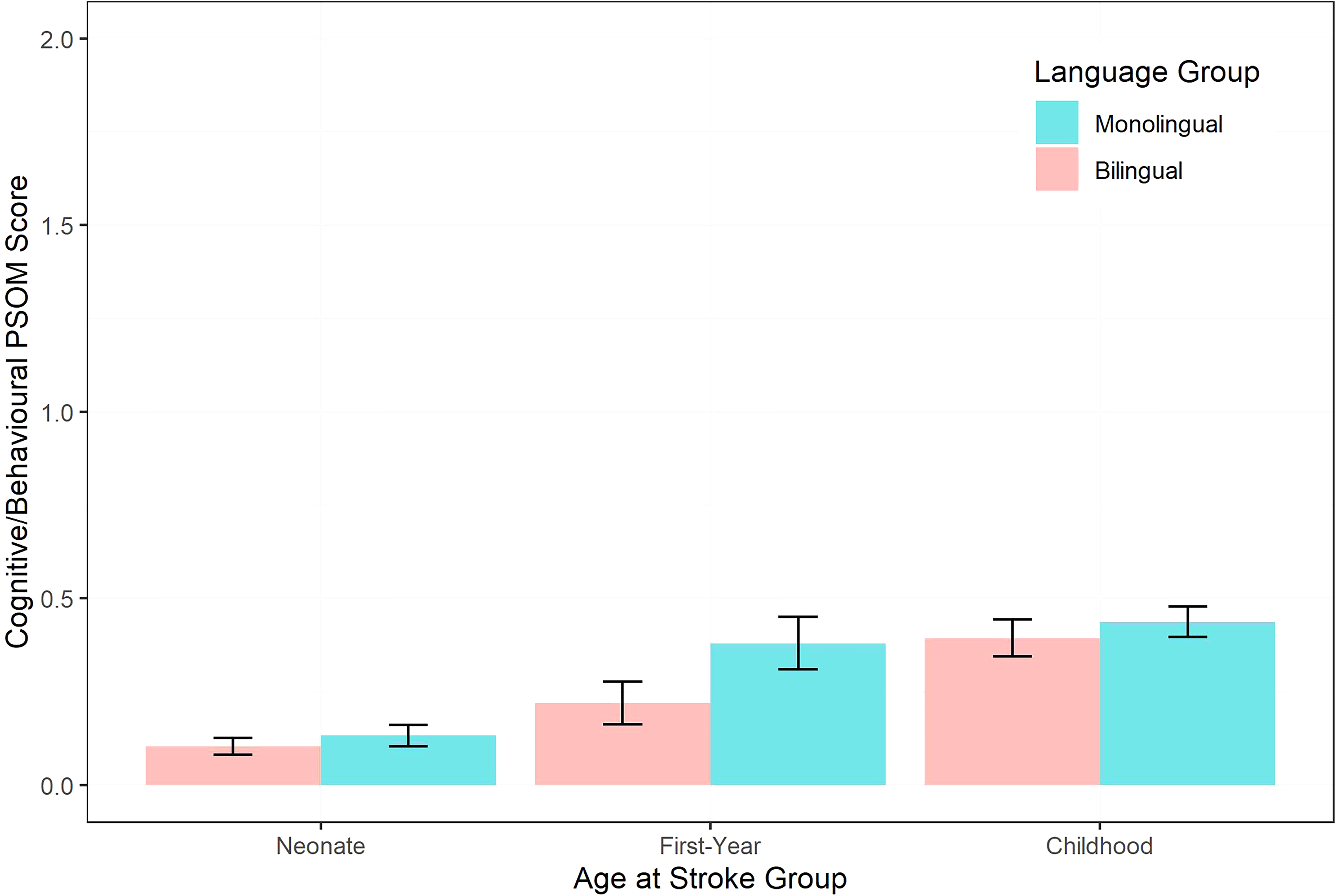
Plot of cognitive/behavioral PSOM by age at stroke group and language group over multiple assessments poststroke within a 10-year period. A higher PSOM score is indicative of a worse outcome. PSOM, Pediatric Stroke Outcome Measure.
Summary of Results From Growth Curve Models Predicting the Fixed Effects of Time Point, Language Group, Age at Stroke Group and Its Interaction on Various PSOM Subscalesa
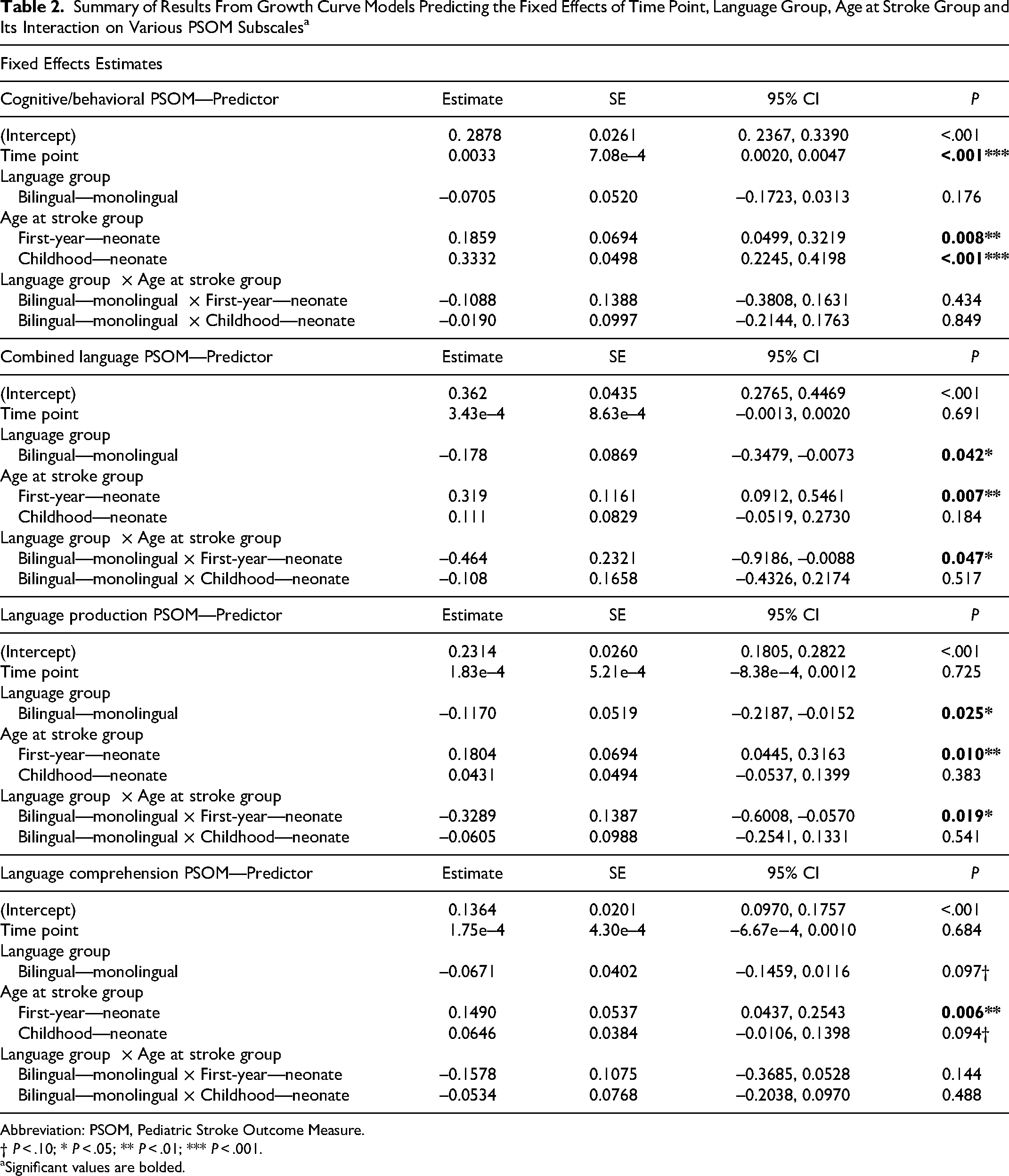
Abbreviation: PSOM, Pediatric Stroke Outcome Measure.
† P < .10; * P < .05; ** P < .01; *** P < .001.
Significant values are bolded.
Using growth curve modeling (Figure 2A), we visualized significant trajectory differences for cognitive/behavioral Pediatric Stroke Outcome Measure scores over time by age at stroke onset groups. We observed patterns of increases over time for children if they had a stroke in their first year and to a lesser extent for neonates but a fairly steady outcome for childhood strokes. In Figure 2B, although no significant differences between language groups emerged, visually monolinguals trajectories mirror those seen in Figure 2A whereas no differences can be seen among bilinguals by age at stroke group.
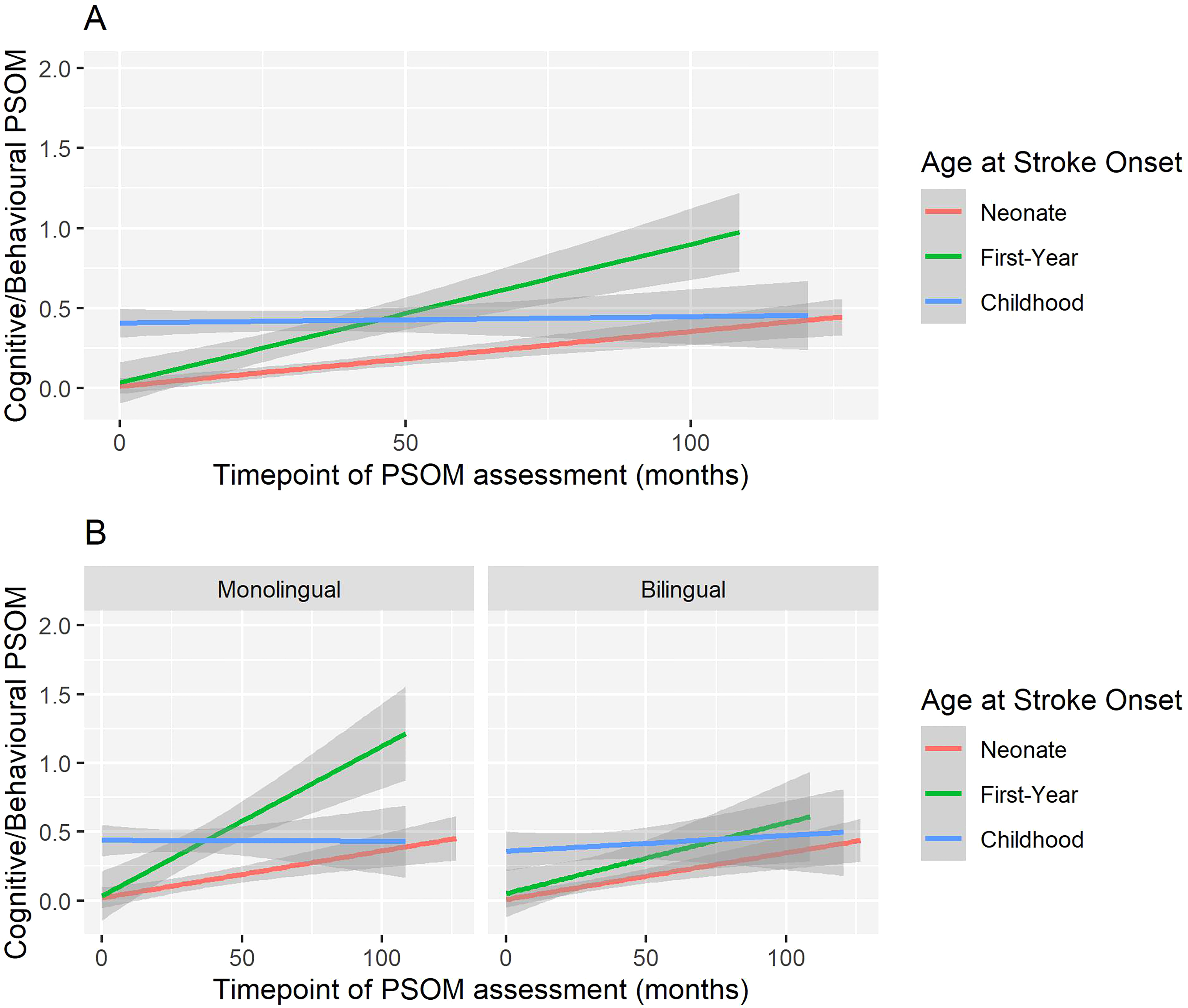
(A) Growth curves for cognitive/behavioral PSOM trajectories over time by age at stroke onset. (B) Growth curves for cognitive/behavioral PSOM trajectories over time by age at stroke onset for monolingual and bilinguals independently. The gray overlay indicates standard error. A higher PSOM score equates to a worse outcome. PSOM, Pediatric Stroke Outcome Measure.
Combined language subscales.
We modeled language development as predicted by language group, age at stroke group, and its interaction, with time point variable as an additional fixed effect as it did not increase fit as random effect (only participant). Language group was significant, with better outcomes favoring bilinguals over monolinguals (P = .04; Table 2; Supplementary Materials). Additionally, one of the interaction comparisons between the age at stroke group and language group showed significance (P = .04; Table 2), with better outcomes for bilinguals in the first-year group. Differing from the age at stroke group pattern apparent in the cognitive Pediatric Stroke Outcome Measure model, a U-shaped pattern with the highest scores was observed for the first-year group.
Language comprehension subscale.
We modeled language comprehension as predicted by language group, age at stroke group and its interaction, with the time point variable as a fixed effect as model fit did not increase as a random effect (only participant). A trend for language group favored better outcomes for bilinguals over monolinguals (P = .08; Table 2; Supplementary Materials). As for age at stroke group findings, a U-shaped pattern with the highest scores was observed for the first-year group.
Language production subscale.
We modeled expressive language function as predicted by language group, age at stroke group and its interaction, with time point variable as additional fixed effect as it did not increase fit as random effect (only participant). As shown in Table 2, language group showed significantly better outcomes for bilinguals over monolinguals (P = .02), while age at stroke group also has significant differences in a U-shape pattern. Once again, the first-year group showed a significant difference between language groups such that monolinguals had worse language production outcomes than bilinguals at age 28 days to 1 year at stroke onset (Figure 3). Age at stroke group and its interaction with language group was a significant predictor of language production Pediatric Stroke Outcome Measure score (P = .01; Table 2).
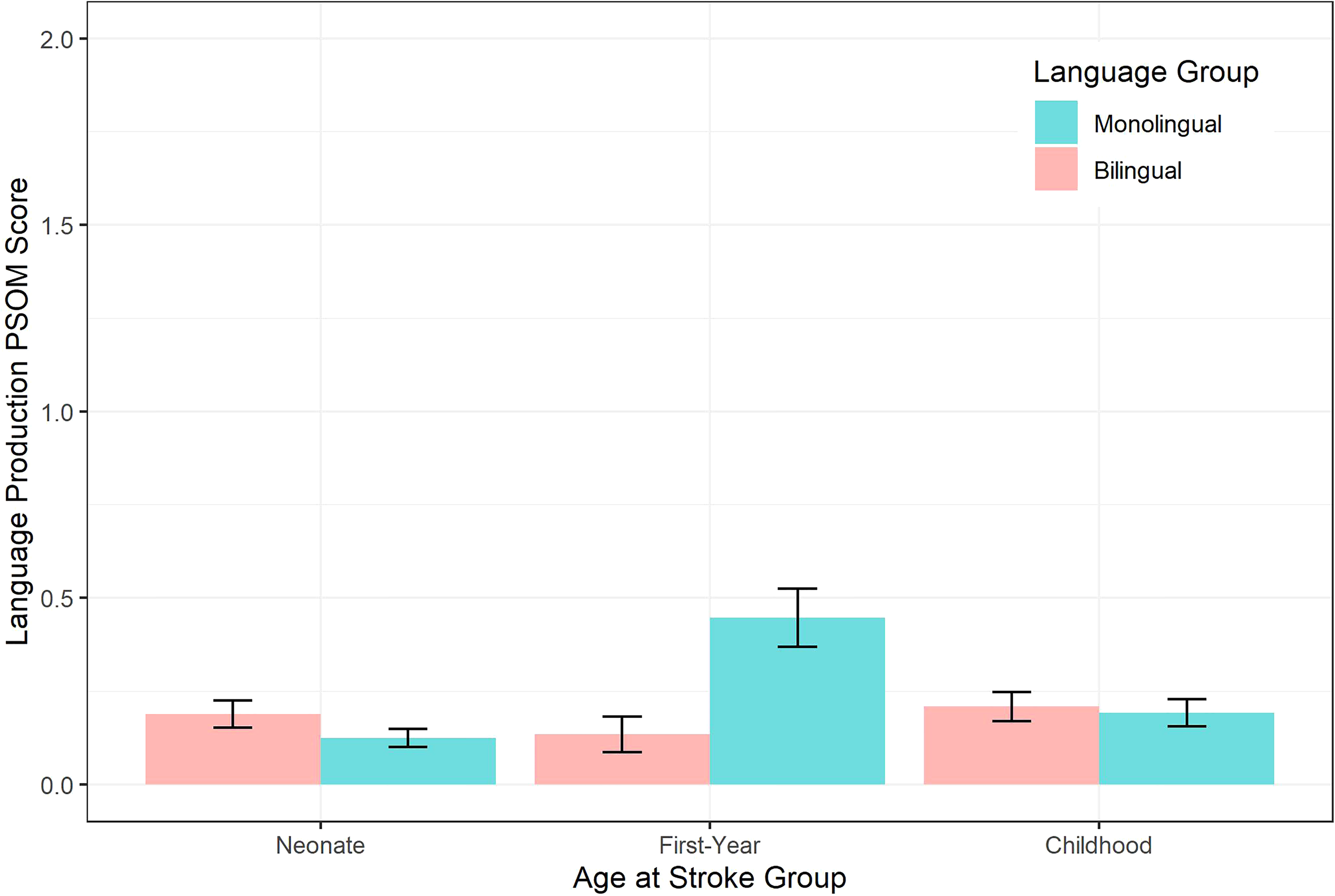
Plot of language production PSOM by age at stroke group and language group over multiple assessments poststroke within a 10-year period. A higher PSOM score is indicative of a worse outcome. PSOM, Pediatric Stroke Outcome Measure.
Using growth curve modeling (Figure 4A), we visualized trajectory differences for language production Pediatric Stroke Outcome Measure scores over time by age at stroke onset groups. In Figure 4B, marked differences between the monolingual and bilingual trajectories, particularly for the first-year group were evident. The monolingual group showed increases over time if they had a stroke in their first year, whereas the scores for the bilingual group remained fairly steady over time.
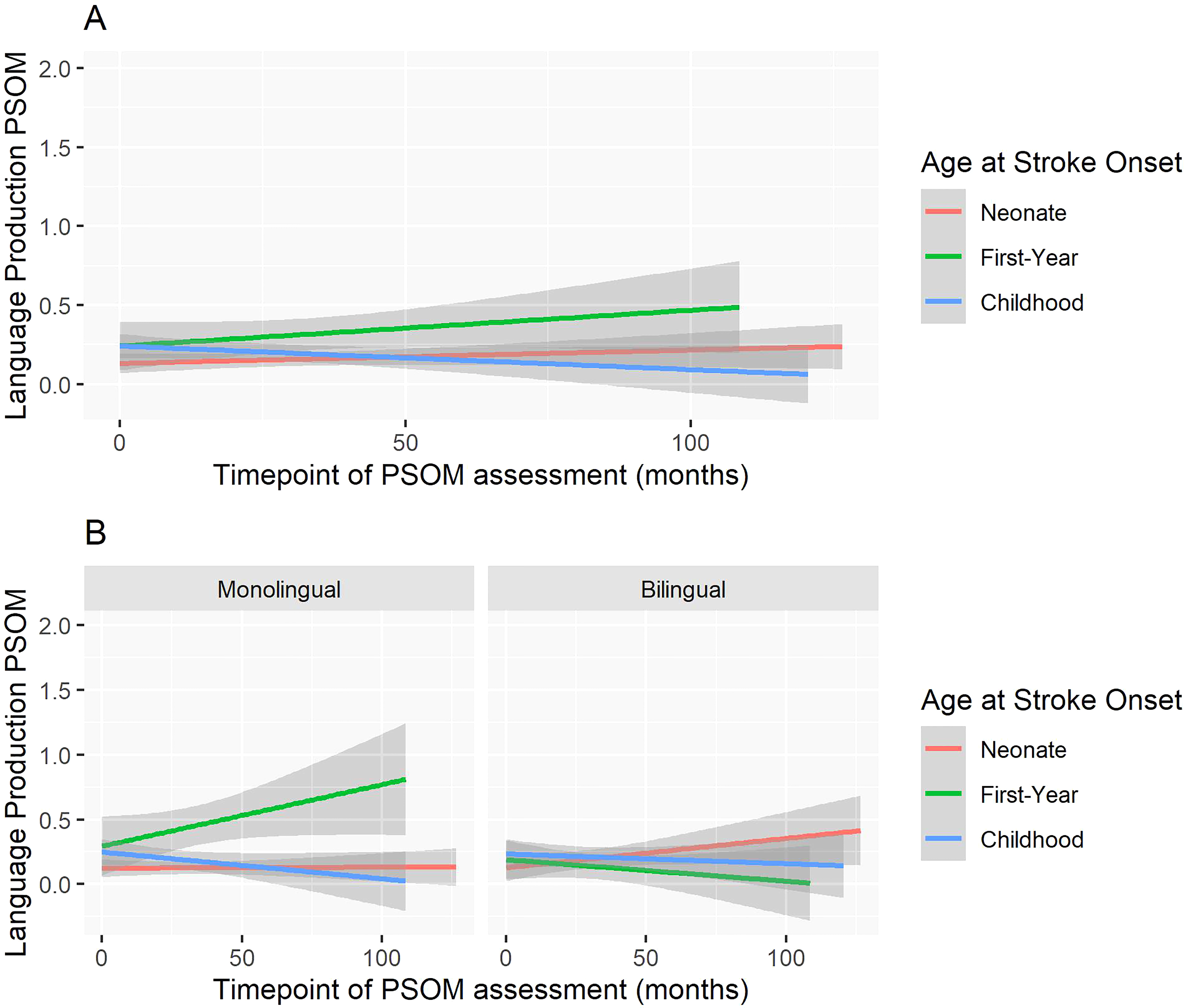
(A) Growth curves for language production PSOM trajectories over time by age at stroke onset. (B) Growth curves for language production PSOM trajectories over time by age at stroke onset for monolingual and bilinguals independently. The gray overlay indicates standard error. A higher PSOM score equates to a worse outcome. PSOM, Pediatric Stroke Outcome Measure.
Discussion
We evaluated the effects of bilingual exposure on the cognitive and linguistic development of children poststroke, using the Pediatric Stroke Outcome Measure (PSOM) administered at several time points and up to 10 years poststroke. First, we found no language group effect or interactions in the cognitive/behavioral Pediatric Stroke Outcome Measure model, suggesting that monolingual or bilingual status did not affect the cognitive/behavioral scores. Second, language group differences showed significantly better outcomes in the bilinguals in the case of language production Pediatric Stroke Outcome Measure (P = .02) and combined language Pediatric Stroke Outcome Measure (P = .04), though this was not true at all age of stroke onset groups. Better outcomes for bilinguals in the group that sustained a stroke between 1 and 12 months of age were found in both the language production Pediatric Stroke Outcome Measure model (P = .01) and the combined (production and comprehension) language Pediatric Stroke Outcome Measure (P = .04).
Age at stroke onset was a predictor of stroke outcome, such that the first-year group had the highest scores in all language Pediatric Stroke Outcome Measure subscales, consistent with previous findings. 7 Similarly, Trauner and colleagues found the trajectory of language development in monolingual children after perinatal stroke is significantly altered between the first and second year of life compared to controls, such that by 2 years of age, their stroke group experienced delays in language production. 39 Although this pertains to early childhood stroke, it is possible that monolinguals of the first-year group showed similar outcomes for language expression, whereas the different outcome for bilinguals was reflective of the aforementioned linguistic advantage for bilinguals. We might also expect differences to be apparent if the stroke occurred outside of the neonatal period (past 28 days after birth), as this time frame would allow for sufficient bilingual exposure pre- and poststroke. Outperforming monolinguals, bilingual children at this age make strides in language learning and metalinguistic skills. 23 Alternatively, at follow-up Pediatric Stroke Outcome Measures, the first-year group could also be showing evidence of their language development, as they transition from a primarily home environment (where they might receive heritage language exposure) to more societal exposure to the language of assessment, English. Therefore, the difference in the language Pediatric Stroke Outcome Measure scores could equally be evidence of growth in English-language skills at this time in bilinguals (as the Pediatric Stroke Outcome Measure is administered in English), or evidence for a general advantage in language learning and metalinguistic skills in bilinguals in general, which functions as a protective factor for pediatric patients.
The lack of an effect in the cognitive/behavioral model may suggest no difference between the 2 groups; alternatively, it may stem from the sensitivity of the Pediatric Stroke Outcome Measure in detecting changes in cognition. First, at the earlier ages, it is difficult to sharply distinguish cognition and language in these stroke-onset groups as this is still evolving with maturation. Second, the agreement between normal/abnormal Pediatric Stroke Outcome Measure subscale scores was the weakest for the cognitive/behavioral subscale, compared to other Pediatric Stroke Outcome Measure subscales. 33 Finally, previous studies using the cognitive/behavioral Pediatric Stroke Outcome Measure have typically recruited older children aged 6 years and older at study. 12 In other atypically developing populations, evidence for a cognitive advantage in bilinguals has been mixed. There has been a documented bilingual cognitive advantage in inhibition and switching in pediatric traumatic brain injury 40 and in enhancing executive functioning on working memory tasks, but not mental flexibility and verbal fluency in children with epilepsy. 41 Given this, we cannot definitively disregard the effects of bilingual exposure on children's cognitive abilities. Future studies using finer-grain or more detailed cognitive measures with these populations are needed to address this question further.
This work was not without limitations. The retrospective study design has notably affected the type of data available. Given the secondary-use data, language exposure was collected based on clinic notes, as there was no way to objectively evaluate the degree of exposure, language proficiency, where the child was exposed, nor language balance in the child. This also highlights a limitation of data currently collected in clinical settings, as a more rigorous language questionnaire would have been preferable to consider language exposure on a continuum and to consider the environment of language exposure more thoroughly. Another limitation related to the sampling includes the differences in group size. The first-year age at stroke group was notably smaller than other groups. Although we maintain that our sample is representative, replicating these effects is recommended for confirmation. Another limitation regarding the data set is related to the follow-up time frame of younger patients with neonatal stroke in particular, whose data in early follow-ups may not be representative of outcome given their young age. Given the study design, we are unable to probe whether the bilingualism effect is only due to the children showing improvements in English-language learning (given that the Pediatric Stroke Outcome Measure is administered only in one language, English) or if there was a difference because of another facet of the hypothesized linguistic advantage. We also note that the performance improvement was only found in the language production Pediatric Stroke Outcome Measure and not in language comprehension Pediatric Stroke Outcome Measure; though in the combined language subscales, there was a strong trend. An additional consideration is that of socioeconomic status, as it has been known to moderate bilingual effects. Although a subset of the children did have socioeconomic status information, a large portion (66%) of the sample did not have this information available. However, of those with socioeconomic status available, no differences between language groups were noted. Similarly, we lacked data regarding the race and ethnicity of patients.
The timing of pediatric stroke during a child's development entails complex cognitive and linguistic challenges in recovery. 11 Vulnerability during “sensitive periods” of development leave children open to the risk of further disruption in development, building on previous milestones. 5 Recovery has been conceptualized as categorical change on the Pediatric Stroke Outcome Measure severity classification system over time,7,35 as assessed in the Recurrence and Recovery Questionnaire (based on the Pediatric Stroke Outcome Measure), 42 and more generally, through a restoration/restitution of function or an adaptative compensation through substitution. 43 Recovery as it relates to poststroke outcomes is predominantly used in the literature, though development is an intrinsically related concept. As such, conflation of these terms further complicates the situation of atypically developing populations. 43
Conclusion
This is the first study evaluating the effect of bilingualism on language and cognitive development poststroke. Our overall results indicate that patients from monolingual and bilingual environments follow similar development poststroke when their cognitive abilities are considered; however, bilinguals had better language outcomes compared to monolinguals for those between 1 and 12 months of age at stroke onset. Considering the limitations of the current study, more data are needed to make a more definitive conclusion about the cognitive development of monolingual and bilingual patients. Importantly, the current study did not find any negative effects of bilingual exposure on development in children poststroke.
Supplemental Material
sj-docx-1-jcn-10.1177_08830738231171466 - Supplemental material for Language and Cognitive Outcomes Following Ischemic Stroke in Children With Monolingual and Bilingual Exposure
Supplemental material, sj-docx-1-jcn-10.1177_08830738231171466 for Language and Cognitive Outcomes Following Ischemic Stroke in Children With Monolingual and Bilingual Exposure by Kai Ian Leung, Nomazulu Dlamini, Robyn Westmacott and Monika Molnar in Journal of Child Neurology
Footnotes
Author Contributions
KIL, ND, RW, and MM made substantial contributions to the conceptualization and overall design of the study. KIL collected patient data from charts and performed initial statistical analysis. KIL and MM interpreted the data and drafted initial manuscript. All authors read, revised critically for important intellectual content, and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by the Natural Sciences and Engineering Grant (RGPIN - 2019 - 06523) to MM and the Natural Sciences and Engineering Research Council - Alexander Graham Bell Canada Graduate Scholarship - Master’s to KIL.
Ethical Approval
This study was approved by the Research Ethics Board at SickKids (REB#1000067719) and consent was provided for all participants or their caregivers as part of their enrollment into the SickKids Stroke Registry.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.