
Abstract
Background:
Perinatal stroke is a leading cause of hemiparetic cerebral palsy and lifelong disability. Neurodevelopmental outcomes are difficult to predict and markers of long-term poor outcome continue to be investigated. Deceleration in growth of head circumference has been associated with worse developmental outcomes in neonatal brain injury. We hypothesized that perinatal stroke would result in decreased rates of head growth during childhood that would be associated with worse developmental outcomes.
Methods:
Patients with magnetic resonance imaging (MRI)–confirmed neonatal arterial ischemic stroke and arterial presumed perinatal ischemic stroke were identified from a population-based research cohort (Alberta Perinatal Stroke Project). Demographics and occipital-frontal circumference data were collected from medical records. Head growth was compared to typically developing control charts using a 2-tailed t test. The Fisher exact test was used to examine associations between Pediatric Stroke Outcome Measures (PSOM) scores and occipital-frontal head circumference.
Results:
Three hundred fifteen occipital-frontal head circumference measurements were collected from 102 patients (48 female, 54 male), over a median of 3.2 years (standard deviation = 5.18, range = 0-18.3). After 3 months for female patients and 1 year for male patients, occipital-frontal head circumference deviated and remained below normal growth trajectories (P < .05) with a large effect size (Cohen d >0.8). Poor outcome (PSOM ≥ 1) was associated with smaller occipital-frontal head circumference (P < .05).
Conclusion:
Head growth deceleration is observed in children with perinatal arterial ischemic stroke and is associated with poor outcome. Head circumference may be a tool to alert clinicians to the potential of abnormal neurologic outcome.
Perinatal stroke causes hemiparetic cerebral palsy and other neurologic morbidities for millions of children worldwide. 1,2 The specific, focal vascular syndromes that result in perinatal stroke injuries are well defined by neuroimaging. 3,4 Arterial ischemic strokes are most common, resulting from occlusion of any of the cerebral arterial territories, and frequently the middle cerebral artery. These and other perinatal stroke lesions can result in a large area of injury with resultant encephalomalacia and volume loss in the weeks following injury. 5,6 Loss in brain volume has been shown to predict decreased occipital-frontal head circumference. 7,8 However, the effects of perinatal stroke on longer-term head growth during development are unstudied.
As a focal injury of defined timing in an otherwise healthy brain, perinatal stroke is an appealing human model of developmental plasticity. Neuroimaging and other brain mapping techniques are informing increasingly sophisticated models of functional development following early unilateral injury. This is most defined in the motor system where engagement of the contralesional hemisphere appears to be a major determinant of clinical function. Substantial evidence of such alterations in motor cortex and corticospinal tract organization 9 has more recently been complemented by more diffuse alterations in the contralesional hemisphere including sensory networks, 5,6 myelination, 10 cerebellum, and thalamus. 11 Such models carry translational significance, informing targets for noninvasive neuromodulation trials that are now demonstrating evidence of efficacy. 10 Despite these advances in perinatal stroke research, overall brain growth following perinatal stroke has not been evaluated.
Occipital-frontal head circumference is the standard clinical measure of head growth in the newborn, infant, and child, and is an economical, simple surrogate marker of brain growth. 12 Microcephaly is defined as an occipital-frontal head circumference below 2 standard deviations from the mean. 13 Acquired microcephaly, or the long-term deceleration of occipital-frontal head circumference growth from a normal range to below the second percentile, 14 is associated with poor neurologic development across a wide variety of conditions. 12,14 Microcephaly has also been associated with worse developmental outcome for neonatal intensive care unit survivors 12 and diminished intellectual development in children. 14 Occipital-frontal head circumference has some ability to predict neurodevelopmental outcome in preterm infants with brain injury. 7 Despite a high risk of evolving adverse developmental outcomes, occipital-frontal head circumference growth trajectories have not been described in perinatal stroke survivors.
We conducted a population-based, retrospective cohort study to evaluate longitudinal head growth in children with perinatal stroke, hypothesizing that head growth rates are reduced as compared to established norms. We further aimed to determine if smaller head circumference was associated with worse developmental outcomes.
Methods
Population
Participants were identified through the Alberta Perinatal Stroke Project, a population-based research cohort. 4 Inclusion criteria were age 0-18 years, a magnetic resonance imaging (MRI)–confirmed, unilateral arterial perinatal stroke, either neonatal arterial ischemic stroke or arterial presumed perinatal ischemic stroke, defined according to established imaging-based criteria, 15 and available Pediatric Stroke Outcome Measure (PSOM) scores. Children with systemic conditions or additional neurologic conditions not attributable to stroke were excluded.
Head Growth
All available occipital-frontal head circumference measurements from birth were collected from the medical record, sex-segregated, and arranged in increasing order from birth to 18 years. All values were then assigned to a representative age using the criteria of birth to 6 months by 2-week intervals, 6 months to 2 years using 1-month intervals, and 2 years to 18 years using 6-month intervals. These ages reflect those used in the data provided by Roche et al 15 for healthy American children, which functions as our comparative data. As per the interquartile range (IQR) technique for outlier removal, any values >(1.5 × IQR) + 75th percentile or <25th percentile – (1.5 × IQR) were excluded. 16
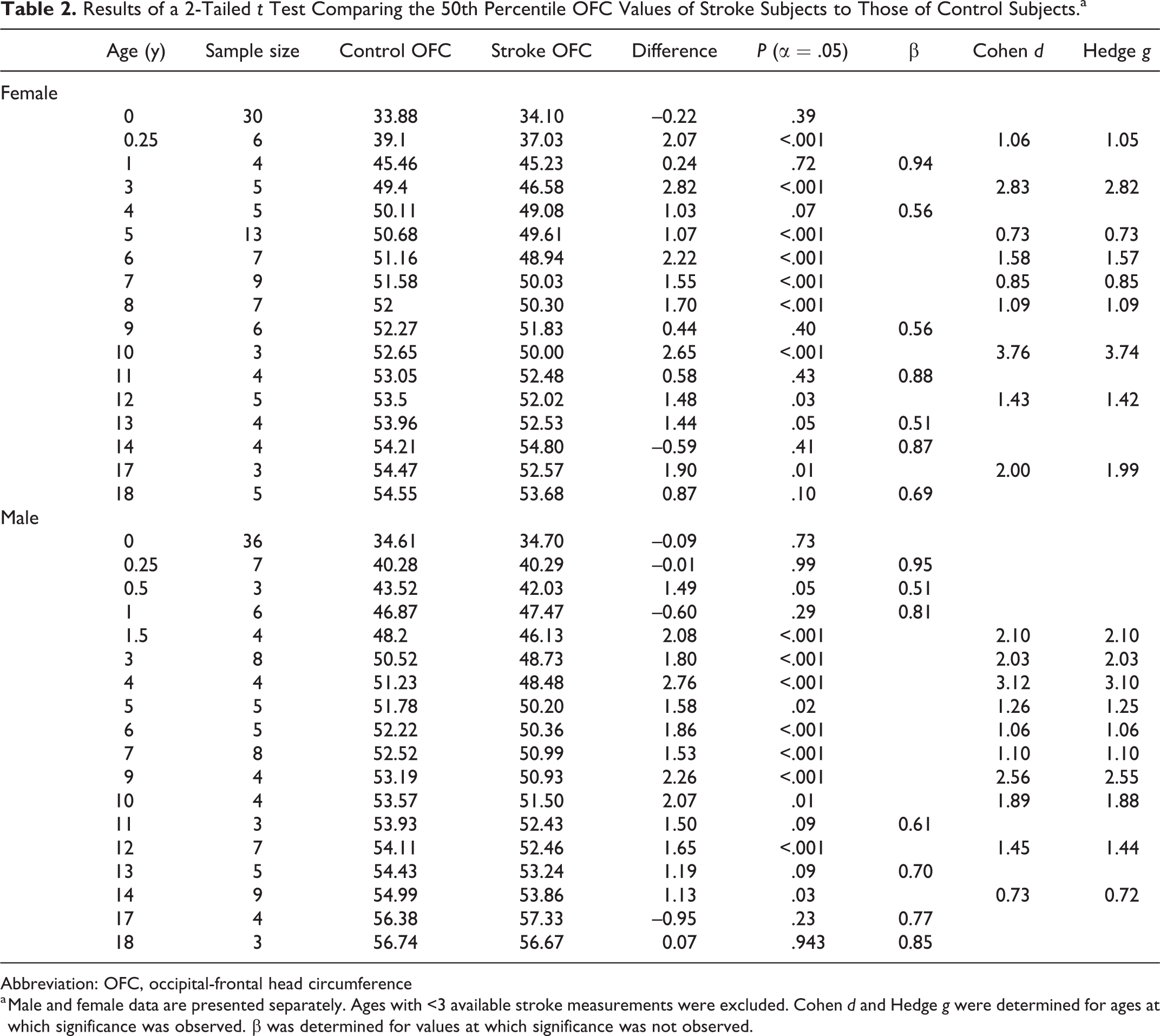
Normalcy was confirmed for the data in each age interval, as ages with <3 data or extensive kurtosis were omitted. A 2-tailed t test was then applied; means from each age interval were compared with data from Roche et al. 15 To account for the potential influences of a limited sample, we calculated β at each age of apparent insignificance (Table 2). Cohen d, Hedge g, and type II error were also determined.
Analysis of Head Growth
Occipital-frontal head circumference data were used to generate sex-specific head circumference plots from ages 0 to 18 years. Fiftieth percentile stroke occipital-frontal head circumference was determined using available data in each age interval (Table 2). Data provided by Roche et al 15 were used to generate the control plots. Trajectories were plotted in R and stroke trajectories were smoothened using LOESS. Standard error was determined for each age-specific 50th percentile stroke occipital-frontal head circumference value (Figure 1).
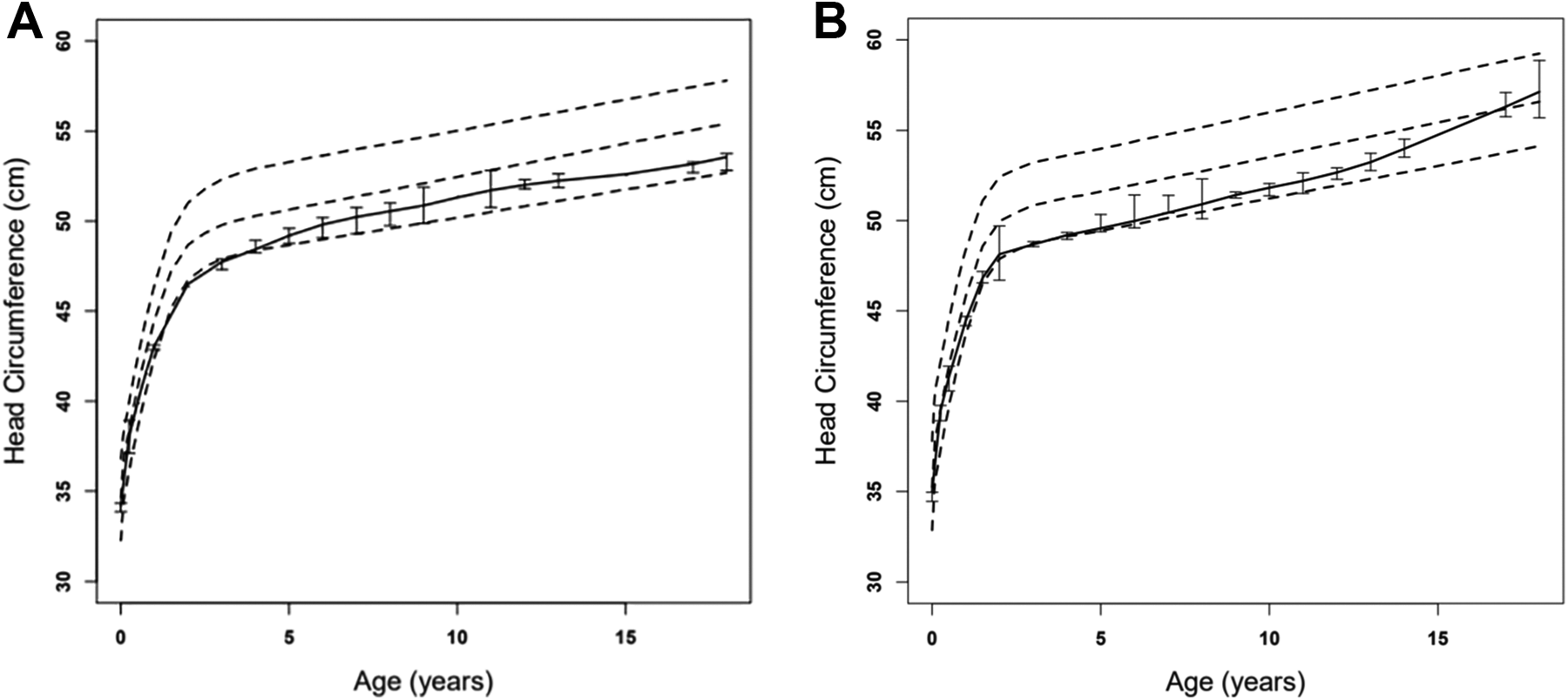
OFC growth trajectories of (A) female and (B) male stroke patients and healthy controls: the solid line represents the 50th percentile for stroke patients and the hashed lines represent the 5th, 50th, and 95th percentile for healthy controls. Bars represent standard error. OFC, occipital-frontal head circumference.
Outcomes
The PSOM is an objective outcome measure that examines neurologic deficit and function on a 10-point deficit scale. 17 For each subject with both occipital-frontal head circumference and PSOM data, the most recent occipital-frontal head circumference measurement was assigned a percentile based on the standards provided by Roche et al. 15 For the analysis of outcome, data from male and female patients were pooled. Fisher exact test was used to determine if <50th percentile occipital-frontal head circumference was more frequently observed in subjects with PSOM ≥1, compared to subjects with PSOM = 0, and whether microcephaly was more frequently observed in subjects with PSOM ≥1. A Student t test was used to compare the average PSOM of children with occipital-frontal head circumference within 1 standard deviation (SD) of the mean to the average PSOM of children whose occipital-frontal head circumference was at least 2 SD less than the mean.
Results
Occipital-Frontal Head Circumference
Three hundred fifteen occipital-frontal head circumference measurements were collected from 102 patients (145 from 48 female patients, and 170 from 54 male patients). The mean age of last measurement was 7.8 years for female patients (range: 0-18.0 years) and 7.0 years for male patients (range: 0-18.3 years). Following outlier removal, 137 measurements remained for female patients and 158 measurements remained for male patients. On average, 2.77 occipital-frontal head circumference measurements were available for female patients (SD = 1.88) and 3.15 measurements were available for male patients (SD = 1.51) (Table 1). In male and female patients, mean stroke occipital-frontal head circumference was significantly smaller than mean control occipital-frontal head circumference at most ages past birth (P < .05) (Figure 1). This difference was first observed at 3 months for female patients and 1 year for male patients. A large effect size was observed for most ages at which significance was demonstrated (Cohen d > 0.8, Hedge g >0.8) (Table 2). The average value of β was 0.73 (Table 2). As is the case for nonstroke patients, occipital-frontal head circumference for stroke patients rapidly increases in the first few years of life, then continues to grow at a slower rate (Figure 1). The stroke curves follow the control curves closely before flattening out below the 50th percentile (Figure 1). The incidence of microcephaly in stroke patients was 20.1% in female patients and 18.5% in male patients. This difference was not significant (P > .05).
Patient Demographics.

Abbreviations: NPV, negative predictive value; OFC, occipital-frontal head circumference; PPV, positive predictive value; PSOM, Pediatric Stroke Outcome Measures; SD, standard deviation.
Results of a 2-Tailed t Test Comparing the 50th Percentile OFC Values of Stroke Subjects to Those of Control Subjects.a
Abbreviation: OFC, occipital-frontal head circumference
a Male and female data are presented separately. Ages with <3 available stroke measurements were excluded. Cohen d and Hedge g were determined for ages at which significance was observed. β was determined for values at which significance was not observed.
PSOM Outcomes
PSOM scores were available for 101 patients (53 male, 48 female) with available occipital-frontal head circumference data (Table 1). Eighty-seven percent of stroke patients with <50th percentile occipital-frontal head circumference had abnormal outcomes (PSOM ≥ 1) compared with 52% of patients with ≥50th percentile occipital-frontal head circumference (P = .004). Significantly more stroke patients with microcephaly (defined as occipital-frontal head circumference ≥2 SD below the mean) had PSOM ≥1 (89%) compared with nonmicrocephalic patients (36%) (P < .05). The average PSOM of children with occipital-frontal head circumference within 1 SD of the mean was 1.45. This value was significantly lower than the average PSOM of children with occipital-frontal head circumference at least 2 SD less than the mean (5.43). Lastly, the abilities of microcephaly to predict abnormal PSOM, as indicated by positive predictive value, and normocephaly to predict normal PSOM, as indicated by negative predictive value, were 90.0% and 33.3%, respectively (Table 1).
Discussion
Occipital-Frontal Head Circumference Trajectories
This study is the first to describe the trajectory of head circumference in patients with perinatal stroke. Our data demonstrate that focal brain injury secondary to stroke is associated with smaller head circumference, as the mean head circumference was smaller than expected beginning at 1 year for male patients and 3 months of age for female patients (Figure 1). The occipital-frontal head circumference is significantly smaller in stroke survivors at most ages after birth (Table 2, Figure 1). Occipital-frontal head circumference is normal in early infancy but deviates soon after, remaining significantly smaller than the norm throughout childhood and adolescence. A significant association between lower occipital-frontal head circumference and general estimates of poor outcome (P < .05) suggests clinical relevance.
These results are consistent with existing literature on occipital-frontal head circumference in high-risk pediatric populations. Decreased occipital-frontal head circumference is frequently associated with brain injury as well as more diffuse neurodevelopmental conditions. Microcephaly is seen in 17% of patients with ataxia-telangiectasia. 18 Children are also reported to have smaller occipital-frontal head circumference following severe TBI with increased intracranial hypertension, 19 and 37% of patients have <10th percentile occipital-frontal head circumference following the onset of infantile spasms. 20 In girls with classic Rett syndrome, a severe neurodevelopmental disorder, occipital-frontal head circumference is reported at least ∼2 SD below the mean. 21 As perinatal stroke is a focal brain injury that occurs in a crucial time in neurodevelopment, it is unsurprising that survivors present with smaller occipital-frontal head circumference.
Emerging hemiparetic cerebral palsy may alert clinicians to order imaging and raise the suspicion of perinatal stroke. Our findings suggest that patients with lower occipital-frontal head circumference may also be at higher risk of developmental difficulties and might require close neurodevelopmental follow-up. We examined arterial presumed perinatal ischemic stroke and neonatal arterial ischemic stroke patients collectively as the 2 diseases differ only in timing of clinical presentation. 22 Although neonatal arterial ischemic stroke patients present most commonly with seizures in the first days of life, arterial presumed perinatal ischemic stroke patients are asymptomatic until 4-6 months postpartum. 23 After 4-6 months, motor asymmetry or early hand preference becomes evident. 23 We demonstrate that the initial time point at which smaller occipital-frontal head circumference is observed precedes or is concurrent with these symptoms. Occipital-frontal head circumference should be monitored in all infants and is another potential biomarker of perinatal stroke outcome.
Outcomes
Outcomes following perinatal stroke vary in modality and severity, but many result in life-long morbidity. 1 Multiple factors complicate outcome prediction. For example, the extent of speech deficit is difficult to ascertain before the child acquires language. 1 Likewise, the predictors of cognitive processes such as attention, cognition, inhibition, and memory are not well defined. 1 Adverse motor outcomes are common in survivors of perinatal stroke and are extensively investigated. 1,24 MRI and pathologic hand preference are valid predictors of motor outcomes, 1,24 but neither tool is fool-proof. 24 Our data suggest occipital-frontal head circumference as another modality that may help in prognostication.
Although MRI is helpful for neurodevelopmental prognostication, it lacks high sensitivity for developmental outcomes. 25 PSOM is a valid and reliable short-term marker of outcome in pediatric stroke. 17 Our results show that abnormal PSOM is more frequently observed in patients who have microcephaly or whose occipital-frontal head circumference is below the 50th percentile. We further demonstrate that average PSOM is significantly greater in patients with occipital-frontal head circumference at least 2 SD lower than the mean. Our finding that small occipital-frontal head circumference predicts mild to severe developmental impairment (positive predictive value = 90%; Table 1) suggests that it may function as an additional marker that alerts clinicians earlier to developmental delay. However, it is important to note that the absence of microcephaly does not have the same ability to predict normal outcomes, as the negative predictive value of normocephaly is 33.3% (Table 1). Ultimately, further investigation is warranted, as the extent to which PSOM predicts long-term outcomes is unknown. 26
Limitations
Perinatal stroke is often retrospectively diagnosed and presents in ∼1:2500-3000 live births. 22 Thus, although all efforts were made to obtain comprehensive data, some limitations were inevitable. Ages with <3 data or extensive kurtosis were omitted to maintain the integrity of the t test, but even so, the average age- and sex-specific sample size was 5. To account for the potential influences of a limited sample, we calculated β at each age of apparent insignificance (Table 2). The average value of β was 0.73, which gives reason to suspect that there is indeed significance at these ages. However, mean occipital-frontal head circumference appears larger in stroke patients at 3 ages where no difference was found (Table 2). These results likely reflect sampling bias, occipital-frontal head circumference is consistently lower in perinatal stroke survivors (Figure 1, Table 2). In addition, the potential for selection bias in our data cannot be excluded. Consistent data were not available for most patients after age 0, and it is possible that patients who were more severely affected are overrepresented in our charts.
Our patient population was homogenous in the sense that patients with systemic conditions or nonstroke neurologic diagnoses were excluded from the study. Height, weight, and race data were either unavailable (height and weight) or uncollected (race). However, children of all major racial-ethnic groups display similar head growth potential 27 ; our results are generalizable to patients of diverse ethnic backgrounds.
It is reasonable to speculate that infarct volume has more prognosticative potential than occipital-frontal head circumference. However, infarct volume only modestly predicts outcomes following perinatal stroke. 1 Accordingly, occipital-frontal head circumference was the focus of this study. Additional investigation is required to determine why the adverse outcomes predicted by occipital-frontal head circumference are unexplained by infarct volume. Of emerging interest is the importance of changes in the contralateral hemisphere to outcome prediction. It is now known that the 2 hemispheres differ in many aspects, including motor pathways, 28 sensory systems, 29 and thalamus. 30 In light of these discoveries, it is possible that changes in the unaffected brain are responsible for poststroke occipital-frontal head circumference growth.
Conclusion
This study demonstrates that occipital-frontal head circumference is significantly smaller following perinatal stroke, and that microcephaly may serve as an additional predictor of long-term developmental outcome. Our study contributes to the rapidly improving understanding of the chronic consequences of perinatal arterial stroke.
Footnotes
Acknowledgments
We thank the members of the Calgary Pediatric Stroke Program for their continued support of this study.
Author Contributions
AL conducted the data and statistical analysis, drafted and made all revisions to the final manuscript. AK contributed to data collection and manuscript review. AF assisted with data collection and manuscript review. AM collected the data, developed and planned the research concept, and contributed to the draft and final revisions of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent was obtained and all methods were approved by the Conjoint Health Research Ethics Board of the University of Calgary (Approval Number: REB14-2090).