
Abstract
We report a case series of children with childhood apraxia of speech, by describing behavioral and white matter microstructural changes following 2 different treatment approaches.
Five children with childhood apraxia of speech were assigned to a motor speech treatment (PROMPT) and 5 to a language, nonspeech oral motor treatment. Speech assessment and brain MRI were performed pre- and post-treatment. The ventral (tongue/larynx) and dorsal (lips) corticobulbar tracts were reconstructed in each subject. Mean fractional anisotropy and mean diffusivity were extracted. The hand corticospinal tract was assessed as a control pathway. In both groups speech improvements paralleled changes in the left ventral corticobulbar tract fractional anisotropy. The PROMPT treated group also showed fractional anisotropy increase and mean diffusivity decrease in the left dorsal corticobulbar tract. No changes were detected in the hand tract. Our results may provide preliminary support to the possible neurobiologic effect of a multimodal speech motor treatment in childhood apraxia of speech.
Keywords
Idiopathic childhood apraxia of speech is a neurologic childhood disorder in which the precision and consistency of movements underlying speech are impaired, in the absence of neuromuscular deficits. Childhood apraxia of speech is usually interpreted as a motor speech disorder, whose core deficit involves the planning and/or programming of the spatiotemporal parameters of speech movement sequences. 1
The majority of children with idiopathic childhood apraxia of speech presents with normal structural brain magnetic resonance imaging (MRI), 2,3 suggesting that brain abnormalities might be too subtle to be detected by conventional MRI, 2,4 but possibly could be revealed by the use of advanced brain imaging techniques. Fiori et al 5 assessed whole brain connectivity in Italian children with childhood apraxia of speech and found significant alterations of inter- and intra-hemispheric connections of bilateral brain regions, correlating with a set of clinical speech measures. This is consistent with the finding of a bilateral reduction of premotor cortex connectivity in adults with acquired apraxia of speech compared with patients who did not develop apraxia, thus suggesting that unilateral abnormalities might be insufficient to determine apraxia. 6 In a sample of children with developmental speech disorders, Morgan and Webster 7 suggested that altered connectivity of the left corticobulbar tract may be a neural marker of developmental speech disorders, whereas no abnormalities were detected in classical language tracts (such as the arcuate fasciculus).
Diffusion MRI allows exploration of brain connectivity through the assessment of the neural microstructural organization of white matter fiber tracts. 8 Not only does this help to understand the neurobiological underpinnings of neurologic disorders, but it also allows for the exploration of brain neuroplastic processes, including the modifications observed during development or those associated with learning or disease. 9 As such, changes in diffusion MRI parameters can be observed, for example, in the motor pathway following motor training, 10,11 suggesting that diffusion MRI can capture treatment related structural brain plasticity. 12 Although several intervention approaches have been successfully used in children with childhood apraxia of speech, 13 only 1 study has shown treatment-related brain modifications, namely, in the volume of the left posterior superior temporal gyrus, as assessed by MRI morphometry. 14 No studies have explored the effects of any intervention on brain connectivity.
In the present exploratory case series study, we evaluated treatment related changes in structural connectivity in a sample of children with childhood apraxia of speech. As in Kadis et al, 14 for this purpose, we applied PROMPTs for Restructuring Oral Muscular Phonetic Targets (PROMPT) treatment, a multimodal intervention for speech and language disorders focused on speech motor control. Its rationale is based on the assumption that speech motor learning and control require a systematic processing and integration of auditory, tactile, kinesthetic, proprioceptive and visual information. 15,16 Recently, a randomized controlled trial (RCT) has demonstrated the effectiveness of PROMPT in treating children with severe speech motor delay. 17
The aims of the present study were to evaluate in Italian children with childhood apraxia of speech treatment–dependent (1) behavioral changes and (2) structural brain plasticity. We hypothesized that the PROMPT speech motor treatment, which systematically integrates tactile-kinesthetic inputs, would induce specific clinical and MRI-detectable effects in children with childhood apraxia of speech. Given the complexity of the neural mechanisms underlying childhood apraxia of speech, for this study we focused on the final motor pathway, that is, the corticobulbar tracts for lips, tongue, and larynx, which have been hypothesized to be involved in speech and oromotor performance in other speech motor disorders. 18 Pre- and post-treatment behavioral and diffusion MRI data were analyzed to identify possible treatment-induced changes in speech measures and tract-based analysis of the oromotor specific tracts.
Methods
Participants
Ten children with ascertained idiopathic childhood apraxia of speech were selected for the current study from a larger sample referred to Stella Maris Scientific Institute for a suspected motor speech disorder. The diagnosis of childhood apraxia of speech was carried out by a multidisciplinary team in accordance with the 3 American Speech-Language-Hearing Association consensus criteria (ASHA, 2007) 1 and with any combination of at least 5 of the 10 Strand speech features detectable across 3 contexts that varied in difficulty 19 -21 (see Supplementary Table S1 for a description of the individual profiles). The 3 ASHA consensus criteria are as follows: (1) inconsistent errors on consonants and vowels during repeated productions of syllables or words, (2) lengthened and disrupted coarticulatory transitions between sounds and syllables, and (3) inappropriate prosody in the realization of lexical or phrasal stress. The Strand’s 10-point checklist of speech features includes difficulty achieving initial articulatory configurations or transitionary movement gestures, syllable segregation, lexical stress errors or equal stress, vowel or consonant errors including distorted substitutions, groping (articulatory searching prior to phonating), intrusive schwa, voicing errors, slow rate, slow diadochokinetic rate, and increased difficulty with multisyllabic words. The identification of the diagnostic features was based on formal testing and on perceptual analysis of video-recorded speech samples by 2 independent observers (AC, BF). As part of the clinical diagnostic protocol, all children underwent a comprehensive neurologic, genetic, behavioral, and metabolic assessment, as well as conventional brain MRI with spectroscopy, which included the study of a white matter and a gray matter volume for each subject.
Additional inclusion criteria were the presence of nonverbal IQ within the normal range at standardized tests of intelligence (WPPSI-III or the WISC-IV performance scales depending on the child’s age) and normal structural brain MRI and magnetic resonance spectroscopy at 1.5-tesla (T) GE Scanner. Exclusion criteria were the presence of orofacial structural abnormalities, known pathologies of neurologic, neurometabolic, and genetic etiologies; audiological deficits; epilepsy; or behavioral and social-relational disorders (ie, autism spectrum disorder).
The final sample included 10 subjects (9 male and 1 female), all right-handed and monolingual Italian speakers, with a mean age of 6.3±1.4 years. Five children were assigned to PROMPT treatment (PROMPT-t) and 5 to a treatment protocol that targeted language and nonspeech oral movements (LNSOM-t). The mean age of the PROMPT-t group was 5.9 (SD 1.35) at enrolment, whereas the mean age of the LNSOM-t was 6.5 (SD 1.1). The 2 groups did not differ significantly in age at baseline (P > .2).
Experimental Design
Children assignment to the PROMPT-t group was based on a pragmatic approach and depended on the availability of a PROMPT trained speech-language pathologist, who could deliver therapy at estimated fidelity levels 22 in the child environment, whilst the children assigned to the other group underwent treatment according to the routine clinical speech and language care. Baseline evaluation (T0) included brain MRI with diffusion MRI and a comprehensive speech motor assessment and was repeated at T1, within 2 weeks from the end of the treatment, which consisted of 50 sessions. Changes of clinical measures between T1 and T0 were considered as the primary outcome measures and diffusion MRI changes between T1 and T0 as possible underlying biological markers.
MRI Investigation
MRI data were acquired using a 1.5-T MRI scanner (Signa Horizon 1.5; GE, Milwaukee, WI). High-resolution structural images were acquired using an isotropic 3D T1-weighted FSPGR sequence. Diffusion MRI data were acquired along 30 directions (b = 1000 s/mm2). One volume with a b-value at zero was also acquired. Diffusion MRI data were preprocessed using tools available in FSL. 23 Preprocessing included brain extraction with manual corrections as required, as well as correction for head motion and eddy current distortions. 24 Maps of fractional anisotropy and mean diffusivity were calculated using MRtrix. 25 The single-fiber response function was estimated from the diffusion images using the “Tournier” algorithm implemented in MRtrix, and fiber orientation distributions were calculated using constrained spherical deconvolution. 25
Diffusion and structural images were coregistered using boundary-based registration. 26 To generate the corticobulbar tracts of interest, 2 regions of interest were outlined in the T1-weighted FSPGR as spherical seed regions for tractography (7 mm radius). The regions on each hemisphere were identified as described in Liégeois 18 by selecting 2 seeding regions of interest ventral to hand representation area (hand knob), which have been reported to correspond to the lips (dorsal corticobulbar tract) and larynx/tongue (ventral corticobulbar tract) representation in the motor cortex. 18,27 A third seeding “hand knob” region of interest was also placed to reconstruct the control tract (hand tract) for the analysis. To define an inclusion region of interest in the pons, a track density image (TDI) 28 was generated from the whole brain tractogram. A region of interest was placed on the TDI between transverse pontine fibers and middle cerebellar peduncle. A pediatric neuroradiologist (RP) and a child neurologist (SF), who agreed on region of interest placement, were blinded to treatment groups.
Tracts were generated using probabilistic tractography by seeding from the 7-mm seed spheres described above (dorsal corticobulbar, ventral corticobulbar, and hand tract), with the pons region of interest as a waypoint. The maximum number of generated streamlines was set to 10 000. An automatic cleaning procedure for excluding false-positive streamlines was applied, whereby isolated streamlines were removed. A streamline-count image was created from tractograms, and voxels containing a value of 1 (ie, a single streamline) were regarded as exclusion regions. Streamlines passing through these voxels were removed. Efficacy of this process was assessed visually. In order to verify the trajectories, tracts were checked by a pediatric neuroradiologist (RP) and a child neurologist (SF), still blinded to treatment groups. Mean fractional anisotropy (FA) and mean diffusivity (MD) were calculated for each reconstructed tract (dorsal corticobulbar, ventral corticobulbar, and hand tract). Examples of the generated tracts in children with childhood apraxia of speech are shown in Figure 1.
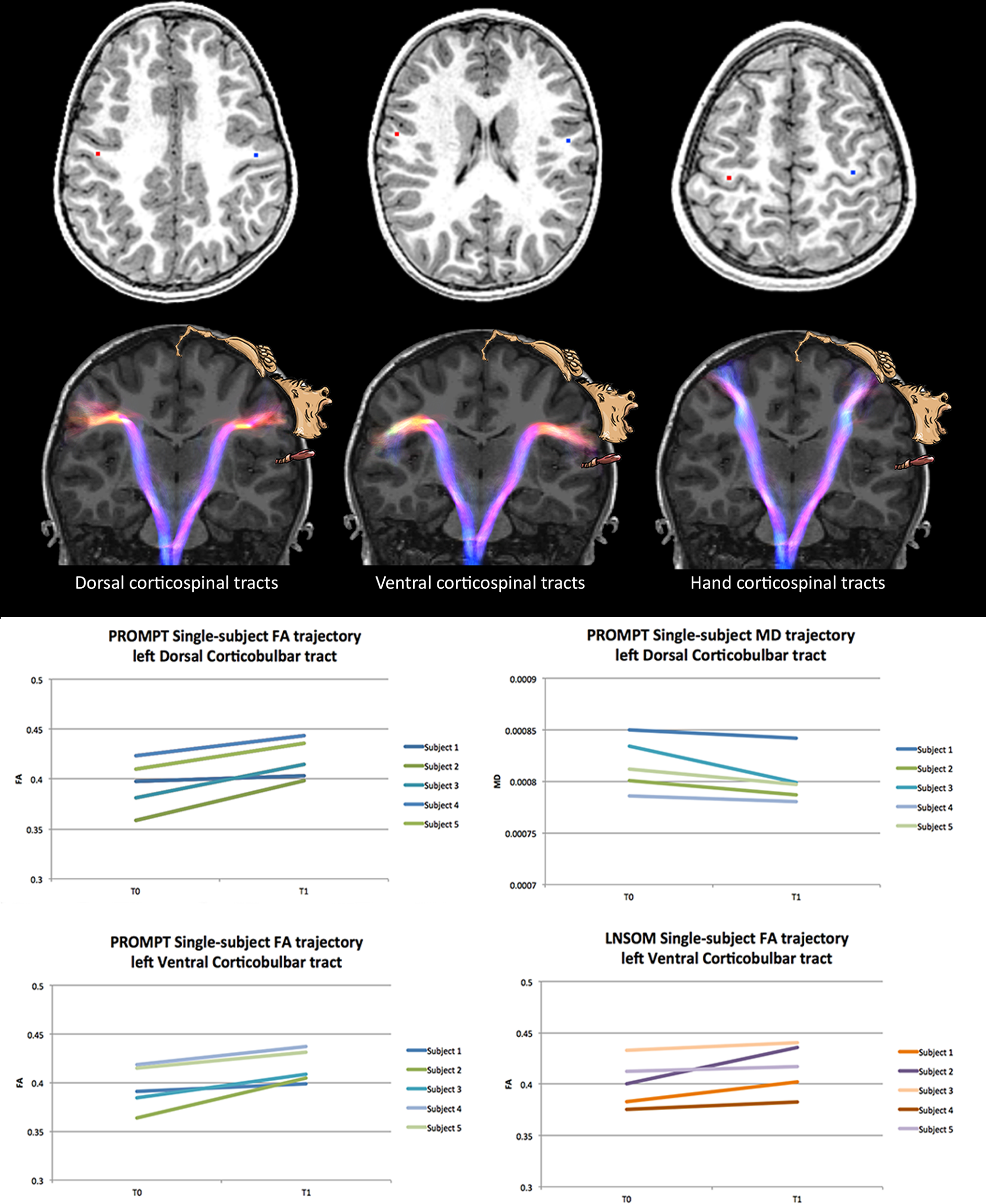
Top row: Identified center (red and blue dots) of the hemispheric spherical seed regions for tractography (7-mm radius), respectively, for dorsal corticobulbar, ventral corticobulbar, and hand tracts (left to right). Middle row: Reconstructed bundles for dorsal corticobulbar, ventral corticobulbar, and hand tracts (left to right). Bundles are overlaid on T1-weighted images. The color of the tracts refers to the fiber orientation according to original tractogram (red: left-right; blue: top-bottom or vice versa). Motor homunculus is schematically represented according to Penfield and Boldrey (Penfield, 1937). Figures are representative of the global origin, shape, and orientation of the reconstructed bundles, irrespective of the cropping of the anatomical slice. Bottom rows: Single-subject trajectories of diffusion MRI metrics for significant changes in both treatment groups. Subjects are identified by colors consistent with Figure 2. FA, fractional anisotropy; LNSOM, Language and Non-Speech Oral Motor; MD, mean diffusivity; PROMPT, PROMPTs for Restructuring Oral Muscular Phonetic Targets.
Nonverbal and Verbal Motor Skills and Speech Assessment
All children were assessed with the Verbal Motor Production Assessment for Children (VMPAC).
The VMPAC is a tool for the assessment of verbal motor skills in children. The items are grouped into 5 areas: Global Motor Control, Focal Oromotor Control, Sequencing, Connected Speech and Language Control, and Speech Characteristics. In Global Motor Control, the structural and neuromuscular integrity of the orofacial district, tone, and strength are assessed. Focal oromotor control is the area in which motor control in speech and nonspeech movements is assessed according to a developmental hierarchical model of speech motor control. 29 Focal oromotor control is evaluated in movements requiring control of jaw, labial-facial musculature, and tongue on only one of the 3 planes of movements (vertical, horizontal, and anterior-posterior) that define the functional space in which speech movements are executed. In the sequencing area, the VMPAC assesses the child’s ability to learn and control nonspeech as well as speech sequences across several repetitions of the same targets. In Connected Speech and Language Control the quality of motor control is evaluated during the production of phrases in a picture description task. This area allows for the evaluation of movement patterns that occur during language production and of the interactions between language complexity and the increase of motor load in longer units. Speech characteristics is an area in which the management of voice parameters, speech rate, prosody, and resonance are taken into consideration.
Speech and language were evaluated according to the procedure described in Chilosi et al, 3 which included the following speech measures: evaluation of phonetic inventory, assignment of an intelligibility score (by 2 independent observers blinded to the assigned treatment group), word accuracy scored as the percentage of consonants correct in a picture-naming task; inconsistency of lexical productions after 2 presentations of the same naming task; diadochokinesis rate and accuracy assessed by a maximum performance task (fast repetition for 20 seconds of 2 and 3 syllable nonwords).
Intervention
Each therapy session delivered to the children in both groups lasted 45 minutes. The 10 children received a full cycle of therapy that included 50 sessions, with a frequency of 2 sessions per week over a period ranging from 6 to 10 months (a cycle was considered as concluded for a child when 50 sessions were completed).
PROMPT Treatment
The PROMPT-treated children received individual treatment sessions by a speech-language therapist (SLT). Regarding speech motor goals, a PROMPT session includes a short blocked prepractice followed by randomized practice in which the syllables, words, and phrases are produced within a communicative context in play. Speech motor goals are, as soon as possible, integrated in goals for language and functional communication. During a PROMPT session, tactile-kinesthetic-proprioceptive inputs are consistently provided in order to shape speech movements, to give information on sequencing and timing, and to introduce constraints for reduction of the degrees of freedom at the articulators’ level in favor of accuracy of movements. During the blocked practice session, each target word or phrase was repeated consecutively 5-6 times. In the randomized practice, the speech targets were embedded in 2 to 3 activities (structured play, such as board or card games, constructive play, play-dough, bowling), which allowed for at least 20 repetitions per target per session. For each child, a lexicon of 20 words reflecting the individual speech motor goals was selected and used in interactive activities. These words could be embedded in meaningful phrases, whose length and complexity depended on the overall level of language demonstrated by the child.
LNSOM Treatment
The treatment program included nonspeech oral motor training, but also articulation and language, though from a different perspective. None of the SLTs who treated the children of the control group were PROMPT trained. The therapy delivered to the LNSOM-t group consisted of a linguistic and articulatory approach that included auditory discrimination of phonemic categories at the syllable and word level and nonspeech oral motor exercises (ie, exercises for blow, labial, and lingual movements). Receptive and expressive lexicon and morphosyntax were targeted depending on the children’s linguistic profile. The selection of the speech sounds to be targeted was based on developmental rather than motor criteria and aimed at the best possible acoustic accuracy of speech sounds in accordance with the order of phonetic acquisition by typically developing children.
Statistical Analyses
At T0 and T1, respectively, differences in age, VMPAC scores, and diffusion metrics on each side of the brain between the PROMPT-t and LNSOM-t subjects were examined by a Mann-Whitney U test in view of the small number of subjects included in the present analysis.
VMPAC results were converted into percentages of correct responses for each area (global motor control, focal oromotor control, sequencing, connected speech and language control, and speech characteristics), which were separately entered in the analysis.
In order to evaluate possible behavioral and neurobiologic effects of PROMPT treatment, VMPAC data, mean fractional anisotropy, and mean diffusivity of each tract (dorsal, ventral, or hand corticobulbar tract) in both groups were compared by Wilcoxon paired test and also estimating bootstrap median difference and its 95% confidence interval. Despite the fact that almost all of the analyzed variables showed a symmetric distribution, nonparametric analyses, and bootstrap estimates were used in view of the limited sample size. Effect size was calculated for any results with P < .1. A P value ≤.05 was considered for statistical significance. Statistical analyses were performed using Stata 14 and R version 3.3.3.
Results
Participants
Ten children were enrolled in the study (5 each for PROMPT-t and LNSOM-t groups). The mean interval between the 2 assessments in the PROMPT-t group was 7.4 months (SD = 0.7; range 6-8) and in the LNSOM-t group was 7.8 months (SD = 1.6; range 7-10).
As shown in Table 1, at T0 VMPAC percentage scores and speech measures did not differ between the 2 groups. Post-treatment (T1) comparisons between groups on the same measures revealed significantly better performances by the PROMPT-t children in VMPAC Connected Speech and Language Control and in the percentage of correct consonants in words.
Participants’ Clinical T0 and T1 Characteristics and Comparisons Between Groups.
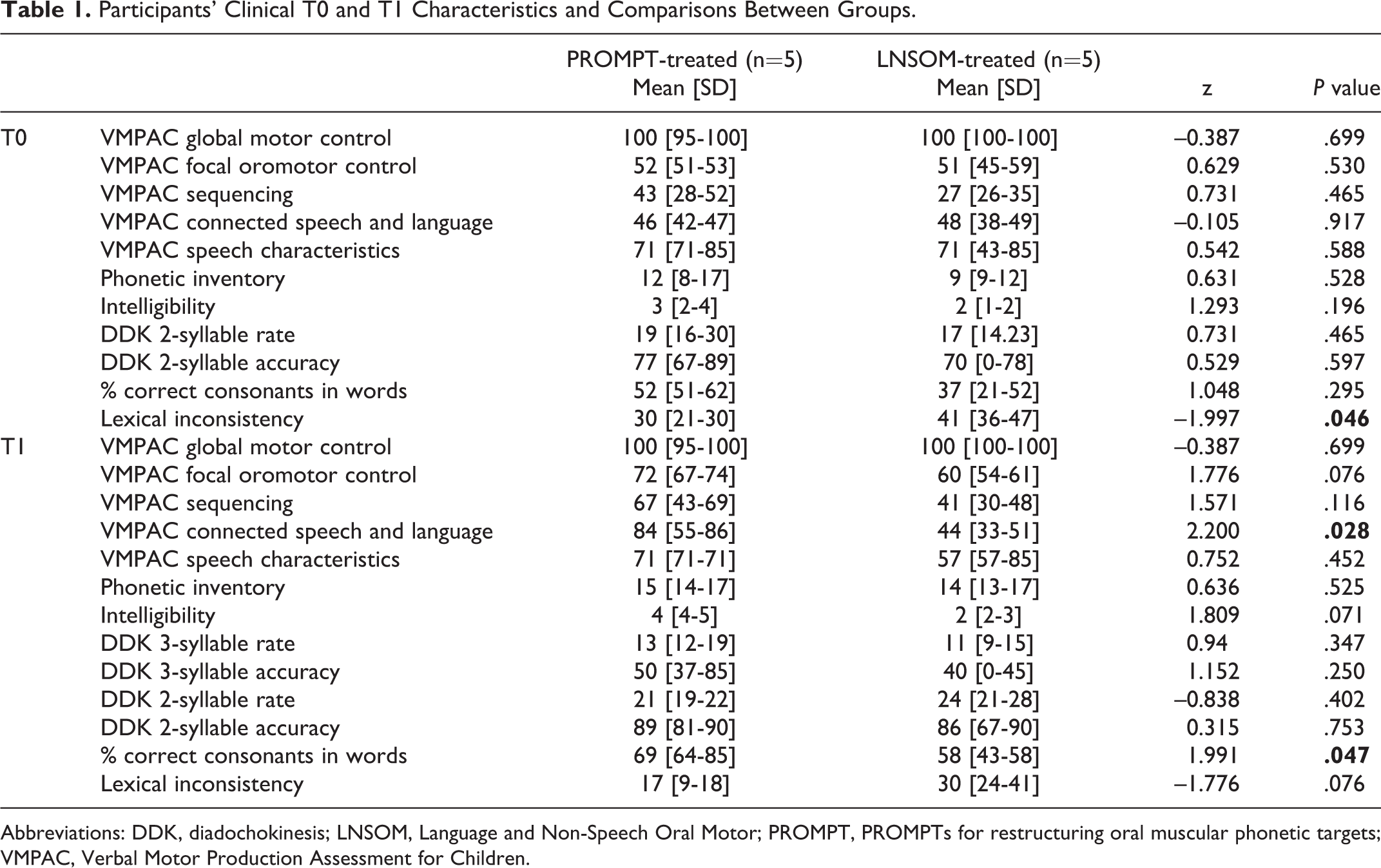
Abbreviations: DDK, diadochokinesis; LNSOM, Language and Non-Speech Oral Motor; PROMPT, PROMPTs for restructuring oral muscular phonetic targets; VMPAC, Verbal Motor Production Assessment for Children.
Post-treatment Behavioral Changes Within the PROMPT- and the LNSOM-Treated Groups
Wilcoxon test revealed differences between T0 and T1 for some of the VMPAC areas in the PROMPT-t group, but no statistically significant differences in the LNSOM-t group (Table 2, Figure 2). In particular, the VMPAC Sequencing and Connected Speech and Language scores improved significantly in the PROMPT-t group (P = .039 and P = .043, respectively), resulting in a large effect size (effect size = 1.19 and 1.64, respectively). Increase of Focal Oromotor Control score approached significance in the PROMPT-t group (P = .057).
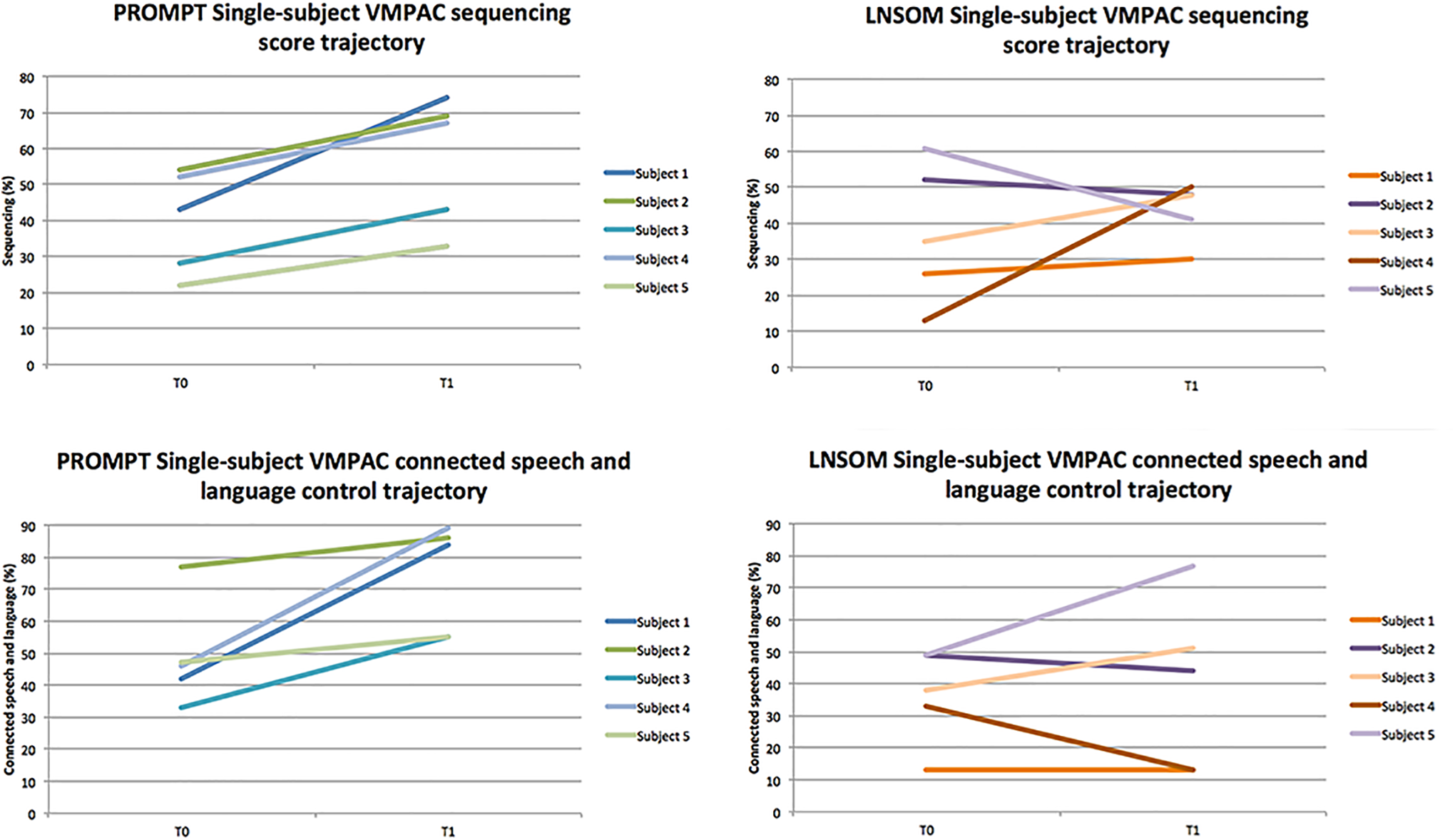
Single-subject trajectories of VMPAC significant changes in the PROMPT-t subjects, compared to LNSOM-t trajectories. Subjects are identified by colors consistently with Figure 1.
For the speech measures (Table 2), PROMPT-t children showed statistically significant improvement of intelligibility (P = .039), diadochokinesis 3 syllable accuracy (P = .043), and percentage of consonants correct in words (P = .042). LNSOM-t group showed improvement in phonetic inventory (P = .041) and diadochokinesis 2 syllable rate (P = .042).
T0 and T1 Diffusion MRI Metrics, VMPAC, and Speech Scores in Each Treatment Group Along With Median Differences and 95% Confidence Interval Obtained From Bootstrap Estimate.
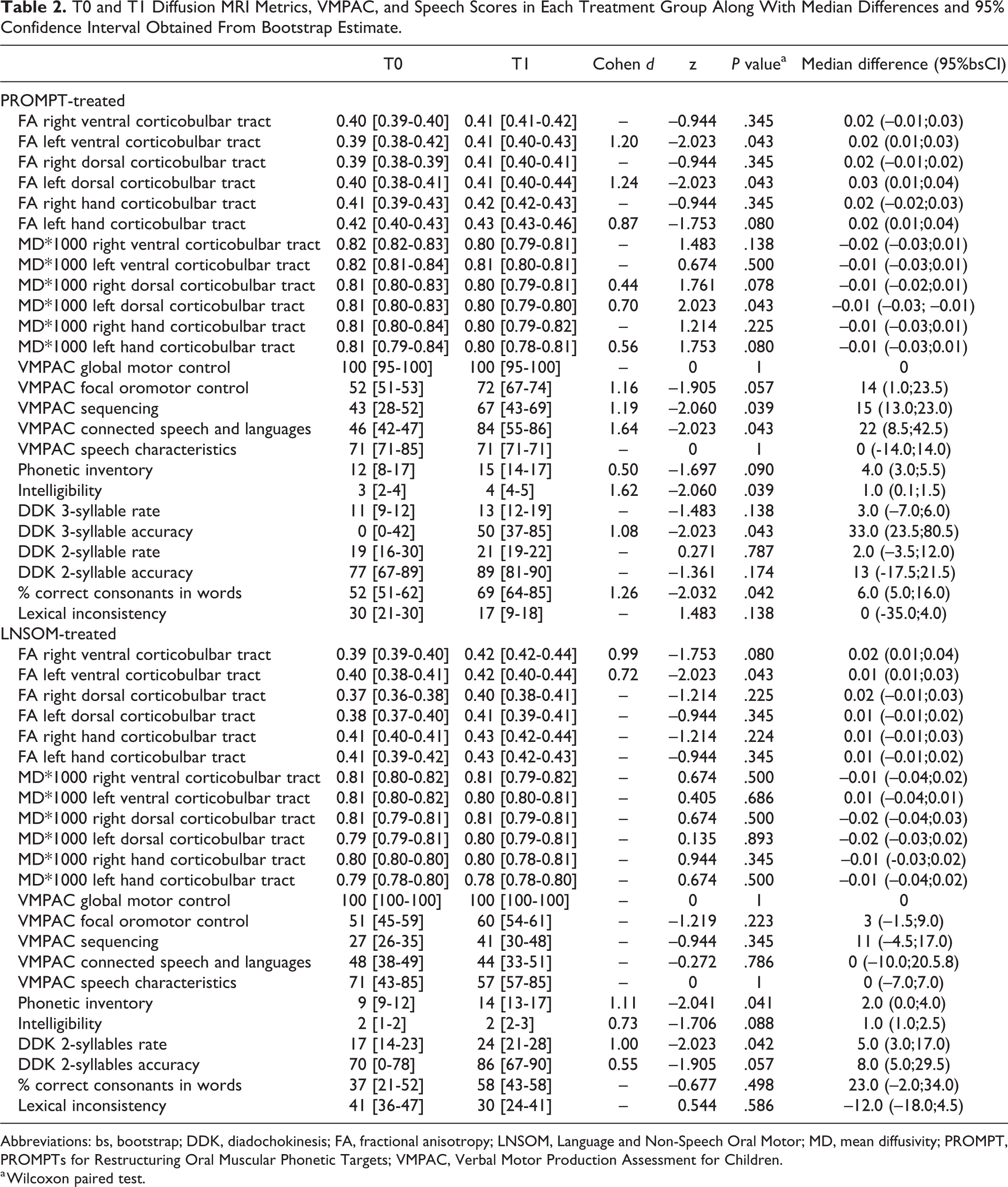
Abbreviations: bs, bootstrap; DDK, diadochokinesis; FA, fractional anisotropy; LNSOM, Language and Non-Speech Oral Motor; MD, mean diffusivity; PROMPT, PROMPTs for Restructuring Oral Muscular Phonetic Targets; VMPAC, Verbal Motor Production Assessment for Children.
a Wilcoxon paired test.
Changes in Diffusion MRI Metrics After Treatment
Differences in diffusion MRI metrics were detected in the left dorsal and ventral corticobulbar tracts in the PROMPT-t group (Table 2, Figure 1). In particular, the left dorsal corticobulbar tract showed fractional anisotropy increase (P = .043) and mean diffusivity decrease (P = .043), whereas in the left ventral corticobulbar tract, the mean fractional anisotropy only increased (P = .043). Further, in the LNSOM-t group, diffusion MRI metrics differences were detected in the left ventral corticobulbar tract with fractional anisotropy increase (P = .043), but with no corresponding mean diffusivity decrease. All significant differences resulted in medium to large Cohen effect sizes (range 0.70-1.24). There were no significant differences in the hand control tracts in any group.
Discussion
The aim of the present study was twofold. First, we aimed to describe a series of cases of children with childhood apraxia of speech in order to explore the different clinical effects of PROMPT treatment compared to a routine speech and language treatment (LNSOM). Our results demonstrated no changes in any of the VMPAC areas in the LNSOM-t group, whereas in the PROMPT-t group we found significant improvements in the Sequencing and Connected Speech and Language areas of the VMPAC. These findings possibly add some evidence on the effectiveness of PROMPT in changing not only speech performances assessed at the word level 30 -34 but also in the production of longer sequences, such as in phrases. As for the other speech measures, PROMPT-t children showed a significant improvement of word and of 3-syllable diadochokinesis accuracy, as well as of the overall intelligibility of speech. The LNSOM-t group showed statistically significant improvement of phonetic inventory and of the 2 syllable diadochokinesis rate.
Second, we aimed at preliminarily identifying possible microstructural changes after PROMPT treatment in white matter corticobulbar tracts involved in oromotor control. Our results showed changes in diffusion MRI metrics, such as an increase in fractional anisotropy and a reduction in mean diffusivity, in the left dorsal corticobulbar tract, which has been previously identified as corresponding to the lips representation of the homunculus. 18
We also found fractional anisotropy increase, but not mean diffusivity decrease in the left ventral corticobulbar tract corresponding to the tongue/larynx representation, both in the PROMPT-t and LNSOM-t groups.
Although our results should be interpreted with caution because of the small sample size, they reflect more consistent changes in white matter microstructural properties, possibly because of treatment-induced neuroplasticity. Overall, these findings support the benefits of a treatment focused on speech movements in improving some of the symptoms of childhood apraxia of speech, as recommended by the ASHA Technical Report. 1 Despite the small sample, the effect size was large for all the statistically significant differences, though causal relationships should be explored on larger samples and through well-designed studies.
Treatment-Induced Plasticity in Childhood Apraxia of Speech and Mechanisms of Recovery
Clinical changes in our case series are further supported by the results of the diffusion MRI analyses. The fractional anisotropy increase in the left Dorsal and Ventral Corticobulbar tracts in the PROMPT-t group can be related to a favorable change in the microstructural properties of the explored tracts, compatible with treatment-induced plasticity. Corticobulbar tracts represent the final motor pathway and are included in the available models of speech motor control. 2,18,35 Reduction of fractional anisotropy and related increase of mean diffusivity are reported to be associated with impaired connectivity, whereas processes connected with learning can determine neuroplastic effects and have been associated with fractional anisotropy increase and mean diffusivity decrease. 5,36 -39 Our results are aligned with previous findings of the left dorsal corticobulbar tract involvement in speech production. 18 In our study, the ventral corticobulbar tract also showed some treatment induced changes in the LNSOM-t group, though limited to fractional anisotropy increase.
A possible explanation for the more substantial increase of fractional anisotropy in the dorsal corticobulbar tracts associated with lips/face compared to tongue/larynx (ventral corticobulbar tracts) could be that jaw control and labial-facial control were priority motor goals of the therapy for all the children in the PROMPT-t sample. Also, the maturation and refinement of tongue movements and its synergistic functioning within the speech motor system has been proven to require a longer time also in typically developing children. 40,41
The relationship between our results and the pathogenic network dysfunction in childhood apraxia of speech is far from clear. Considering the small number of subjects, we oriented our study toward a well-defined a priori hypothesis on corticobulbar tracts. However, it can be hypothesized that the observed results might either reflect the secondary effect of a change in higher level networks subserving speech motor control, or the effect of a direct involvement of the corticomotor tract in childhood apraxia of speech recovery.
Possible Role of Lateralization in Childhood Apraxia of Speech Recovery
More consistent changes were found here in the left corticobulbar tracts. This left lateralized speech motor recovery might be linked to a dysfunction mostly in the left corticobulbar tract in childhood apraxia of speech. It is of note, however, that similar findings were reported in studies involving also other types of speech sound disorders, including articulation disorder, phonological disorder, and phonological delay or inherited speech disorders. 42,43
Although our data do not allow to precisely define the biological meaning of an asymmetrical brain dysfunction in childhood apraxia of speech, they are in agreement with previous findings showing plasticity changes in the left hemisphere after treatment in childhood apraxia of speech. 14 Based on our preliminary results and on previous reports, one might speculate that the left hemisphere tracts are more responsive to plasticity than the right tracts, or, alternatively, that the left hemisphere is primarily affected and therefore the main target of recovery, or a combination of the two. 5
The hypothesis of possible unilateral atypicalities in childhood apraxia of speech is also in agreement with data on acquired adult apraxia of speech resulting from left hemispheric stroke, 44 -46 although no evidence supporting a similar organization in the developing brain has ever been demonstrated. 44
The present study provides evidence in support of the role of left dorsal and ventral corticobulbar tracts abnormalities as the target for brain plasticity induced by treatment. Compared to the only study demonstrating a neurobiological effect of a PROMPT treatment in childhood apraxia of speech, 14 our children experienced a longer treatment. According to this larger window of plasticity, it is not surprising to detect a small but likely effect in the descending corticobulbar tracts. The impact on oral motor control areas, such as the rolandic cortex, of a longer block of therapy has already been hypothesized 14 and is consistent with our findings.
Limitations
Our study has several limitations, starting from the small number of subjects, which is due to the rarity of idiopathic childhood apraxia of speech and to families’ and children’s compliance to treatment and MRI execution. For this reason, no correlation analyses between structural tract-based changes and clinical measures could be performed. Neither parameters such as the severity of the disorder, age, and sex were included as covariates in the analysis, nor was it possible to have specific age matching, which would have reduced age-related biases.
Also, because of the limited number of subjects, we focused our interest on the final motor pathway, that is, the corticobulbar tracts, because of the expected higher reproducibility of these tracts and their previously hypothesized role in speech motor disorders. 18 Other tracts such as the inferior fronto-occipital fasciculus (IFOF 47 ), or the frontal aslant tract (FAT 48,49 ), linking the supplementary motor area with the pars opercularis of the inferior frontal gyrus might also be dysfunctional in childhood apraxia of speech. A more comprehensive analysis of a wider network, including IFOF and FAT, should be performed in a larger sample, since their role has never been investigated in developmental speech motor disorders.
Furthermore, the impact of a possible maturation effect has not been controlled here and might be targeted in future studies. A larger sample would allow extending the study to a higher number of tracts and networks to disentangle the complex relationship between disease and recovery in childhood apraxia of speech.
Conclusions
The current results in our case series of children with childhood apraxia of speech show behavioral and neural structural changes induced by treatment, with more marked effects on speech motor control and related connectivity after PROMPT, compared with nonspeech oral motor and language treatment. Further studies are mandatory to confirm our preliminary results.
Supplemental Material
Supplemental Material, sj-pdf-1-jcn-10.1177_08830738211015800 - Neural Changes Induced by a Speech Motor Treatment in Childhood Apraxia of Speech: A Case Series
Supplemental Material, sj-pdf-1-jcn-10.1177_08830738211015800 for Neural Changes Induced by a Speech Motor Treatment in Childhood Apraxia of Speech: A Case Series by Simona Fiori, Kerstin Pannek, Irina Podda, Paola Cipriani, V. Lorenzoni, Beatrice Franchi, Rosa Pasquariello, Andrea Guzzetta, Giovanni Cioni and Anna Chilosi in Journal of Child Neurology
Footnotes
Acknowledgements
We acknowledge the children and families who took part in this study, the nursing staff, radiology and administrative staff in the MR Service and Laboratory at Stella Maris Scientific Institute. We acknowledge Sabrina Giannino for scoring VMPAC assessment and Olena Chorna for English revision. We also acknowledge Luca Canapicchi for drawing the homunculus in ![]() according to Penfield and Boldrey (Penfield, 1937).
according to Penfield and Boldrey (Penfield, 1937).
Author Contributions
SF, AC, IP, PC, AG, and GC contributed to study design; SF, AC, IP, PC, KP, AG, and GC drafted the manuscript. SF, AC, IP, PC, and RP contributed to data collection; and SF, AC, IP, PC, RP, and KP performed data analysis. BF contributed to clinical data collection; and VL contributed to the statistical analyses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by PROMPT Institute for Motor Speech Research Grant 2014 and by the Italian Ministry of Health (RRC-2013-2353257).
Supplemental Material
Supplemental material for this article is available online.
Ethical Approval
This study was carried out in accordance with the recommendations of the local and regional pediatric ethics committees. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics Committee of the IRCCS Fondazione Stella Maris (Number 13/2013) and of Meyer Hospital (Number 127/2018).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.