
Abstract
Amplitude integrated EEG (aEEG) is increasingly utilized in preterm infants. The aim of the study was to evaluate whether semiquantitative visual assessment of aEEG background during the first 72 hours of life is associated with long-term outcome in a group of premature infants born less than 28 weeks’ gestation. Infants were prospectively enrolled and monitored in the first 72 hours after birth. aEEG was classified daily according to background activity, appearance of cyclical activity and presence of seizures activity. Log-rank and multivariable cox analysis were used to explore associations of background aEEG activity with short and long-term outcome. Overall, 51 infants were enrolled into the study. Depressed aEEG background on the third day of life was associated with poor outcome (P = .028). Similarly, absence of cycling on the third day of life was associated with death or poor outcome (P = .004 and .012, respectively). In different multivariable models adjusted for gestational age, severe intraventricular hemorrhage or use of sedative medication, neither background nor cycling activities were associated with outcome. Depressed aEEG background and absence of aEEG cycling on the third day of life are associated with poor outcome in univariable analysis. Although continuous aEEG monitoring of premature infants can provide real-time assessment of cerebral function, its use as a predictive tool for long-term outcome using visual analysis requires caution as its predictive power is not greater than that of gestational age or intraventricular hemorrhage.
Despite a decreasing incidence of severe intraventricular hemorrhage and periventricular leukomalacia, premature infants’ brain injury and resultant cognitive impairment still occurs from putative mechanisms such as inflammation, oxidative stress and impaired maturation connectivity. 1,2
Cerebral activity assessment with conventional electroencephalography (EEG) is a powerful tool in assessing the well-being and neurodevelopmental outcome in preterm infants. Two decades ago Marret et al 3 noted on a large cohort of 417 premature infants that those with increased abnormal background EEG were more likely to die. Also, Hayakawa et al 4 showed on a cohort of 101 premature infants that those having serial EEG recording with persistently depressed or dysmature background activity were more likely to be diagnosed with cognitive impairment later in life. As the implementation of a conventional EEG service in most neonatal units is challenging, many centers began exploring limited channels EEG modalities of which amplitude integrated EEG (aEEG) is the most extensively studied as it allows for continuous assessment of cerebral activity soon after birth with a minimal disturbance for the extremely premature infant. Normal maturation of aEEG background patterns in preterm infants throughout gestational age evolving from a predominant discontinuous background to a predominant continuous background at term with an evolving cyclical activity has been described 5 -9 and correlated with conventional EEG. 10 Also, associations were suggested between depressed aEEG activity and acute events (ie, intraventricular hemorrhage, 11,12 sepsis, 13 and acute respiratory acidosis 14 ), sedation 15,16 as well as short- 11,17,18 and long-term outcome. 19 -22
We hypothesized that aEEG indices soon after birth are related to outcome in premature infants.
The aim of this study was to correlate a daily semiquantitative visual background aEEG analysis during the first 72 hours of life with outcome in premature infants.
Methods
This was a prospective study. Included in the study were infants born 28 weeks’ gestation or less between July 2008 and December 2010. Infants were included if their mothers had a first trimester ultrasound examination and there was more no more than 1-week difference between it and dating by last menstrual period. Infants with significant congenital and chromosomal anomalies were not included in the study.
aEEG Monitoring
aEEG was recorded using the CFM 6000 recorder (CFM 6000, Olympic Medicals, Natus, Seattle, WA). In this method, EEG signals are derived from 2 parietal cup electrodes situated on P3 and P4 with a reference Pz electrode. Original EEG signals are asymmetrically filtered (<2 and >15 Hz), rectified and smoothened. The signal is then compressed to a rate of 6 cm/h and displayed on a semilogarithmic scale. 23,24 The original 1 channel EEG tracing is available for online and retrospective review.
As per NICU protocol, aEEG monitoring is initiated as soon as possible after admission to the NICU. Parents whose infants’ recordings were initiated in the first day of life and had at least 6 hours of recording during the first day of life were invited to join the study. Recruited infants were monitored at least up to their third day of life (or until death if occurred before).
aEEG Analysis
Tracings were evaluated by 1 researcher (JR), blinded to any clinical information, using a visual semiquantitative aEEG analysis according to Olischar et al criteria. 5 Thus, each 10- minute aEEG epoch was initially classified into 8 different background patterns (continuous, high discontinuous, low discontinuous, burst suppression, low voltage, isoelectric, seizure activity, and artifacts) (Figure 1). For each day of life, the percentage of time spent in each aEEG background category was calculated excluding time of seizure, artifact activity (ie, impedance>10 kOhms or disconnected electrodes) and the unrecorded time during the first day of life. Percentage of depressed background activity was calculated as the summation of the daily percentage of low discontinuous, burst suppression or isoelectric background and dichotomized into 2 groups by the 75th centile for gestational age (over 70% for 24-25 weeks’ gestational age and 60% for 26-27 weeks’ gestational age). 5
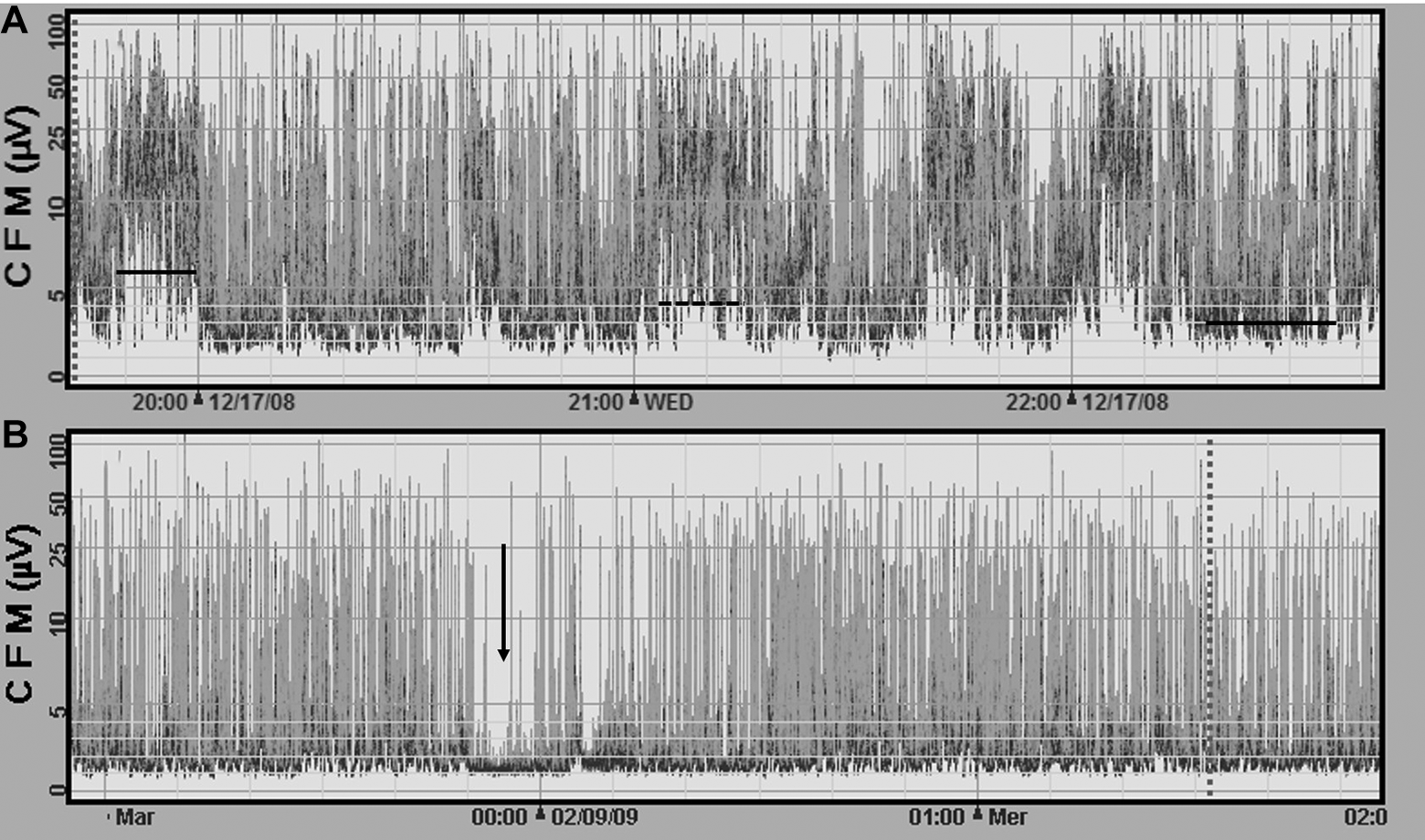
Examples of aEEG recordings with different background activity. (A) Infant born at 26 weeks’ gestation on his first day of life demonstrating continuous activity: left bar, discontinuous high activity: middle dashed line, low discontinuous: right bar. Cycling is also apparent as the wave like pattern of the lower border of the tracing formed by the alternation between the different background patterns. (B) Infant born at 27 weeks’ gestation at his 1st day of life demonstrating mainly burst suppression activity with a short 10-minute isoelectric segment (vertical arrow). No cycling pattern is perceived in this example.
In addition to the above analysis, presence of seizure activity (defined as a sudden rise of the aEEG pattern with a concomitant evolving repetitive spike or sharp wave pattern lasting for at least 10 seconds) 12 and cyclicity (smooth sinusoidal pattern, mostly in the lower border of the aEEG tracing 12 [Figure 1]), were noted.
As aEEG recording is a common practice in the authors’ unit, attending physicians had access to monitors at all time. None of the infants recruited received anticonvulsant medication during the first 3 days of life.
aEEG Assessment Reliability
Interrater reliability was assessed by a random reevaluation by 2 of the authors (RJ and SE) of a 1-hour recording from 45 different infants. Intraclass correlation coefficient for depressed background activity was 0.977 (CI: 0.959-0.987).
Clinical Data Collection
All data were prospectively collected. These data included demographic information, intrapartum history (presentation, mode of delivery), infant’s perinatal course (Apgar score, cord pH, base excess), birth weight, gestation age at birth, medications and clinical diagnoses.
Cerebral ultrasound scans were performed (as per the study protocol) on the first and third days of life, at 1 week of age, 30 and 34 weeks’ corrected gestation age.
Neurodevelopmental Outcome
Families were contacted at the age of 24 months for a follow up visit. General physical examination was performed, together with the Bayley-III Screening Test 25 and the Amiel-Tison Neurological Evaluation Tool. 26 Outcome was dichotomized as good or poor for the short and long-term outcomes. Being alive at discharge was considered as good short-term outcome, while for long-term outcome, a composite good outcome was considered as survival with a normal physical examination with no sensory impairment, no at-risk categories on the Bayley Screening Test and no severe classification in the Amiel-Tison evaluation. Death, blindness, deafness, 1 or more at-risk scores on the Bayley Screening Test or severe classification in the Amiel-Tison evaluation were considered a composite poor long-term outcome.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences (IBM SPSS version 21). Continuous data are presented as mean ± standard deviation (SD) and assessed by t-test or Mann–Whitney test. Categorical data are presented as proportions and compared by chi-square or Fisher’s exact tests.
Log-rank survival analysis was used to examine associations between aEEG indices and death before discharge or poor outcome in the first, second and third days of life. Log-rank analysis was also used to examine the associations between poor outcome and neonatal clinical characteristics either known to affect neurodevelopmental outcome or suspected to act as a confounding variable. For each significant association between aEEG and outcome a multivariable cox regression was performed. Due to the sample size, each model included a maximum of 3 covariates. A probability value of <.05 was considered statistically significant.
Results
During the study period 142 infants were born at 28 weeks’ gestation or less, 14 parents declined participation, in 23 infants gestational age was not reliable, 44 infants were not monitored in the first 72 hours of life either due to unavailability of the monitor 5 were not approached, 1 infant had congenital anomaly and 1 was recruited to another study. Of the 54 families that consented to participate in the study, 3 were excluded due to unreliable gestational age and thus the final cohort consisted of 51 infants. aEEG recordings were started at a median age of 3 hours 31 minutes (range 25 minutes to 17 hours 16 minutes). All but 2 infants’ recordings started prior to 10 hours of age. Clinical characteristics of the recruited infants with its comparison to the nonrecruited are presented in Table 1. The only differences that were found between the 2 groups were a lower prevalence of Bedouin-Muslim ethnicity in the recruited group (49% vs 66%, P = .049) and, within survivors, 3 infants in the recruited group that were diagnosed with grade 3 retinopathy of prematurity as compared to none in the none recruited group.
Neonatal Characteristics and Comparison With Infants Born in the Same Period and Not Included in the Study.
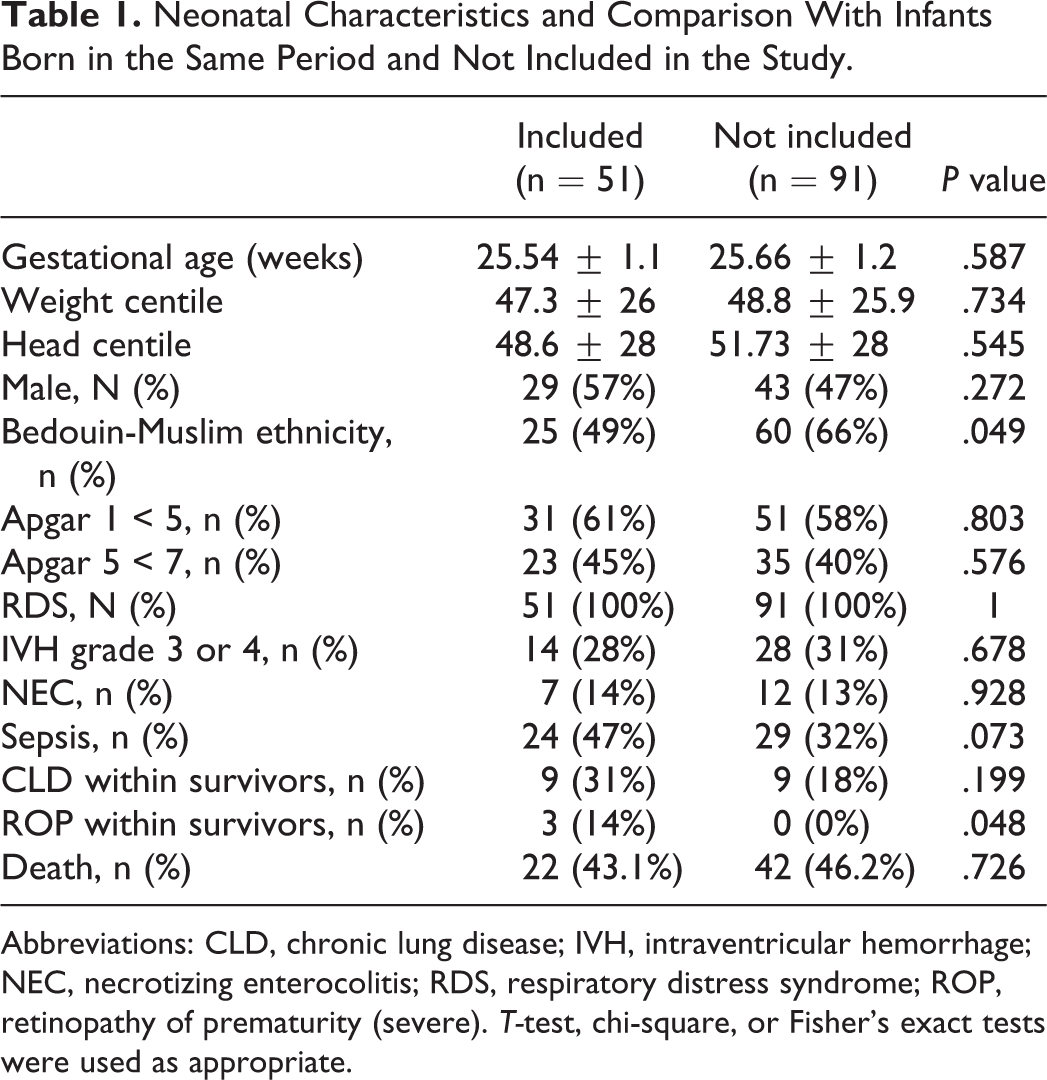
Abbreviations: CLD, chronic lung disease; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; RDS, respiratory distress syndrome; ROP, retinopathy of prematurity (severe). T-test, chi-square, or Fisher’s exact tests were used as appropriate.
Outcome
Overall 29 infants survived to discharge, of them, 25 (86%) were contacted at a mean age of 2.2 ± 0.22 years and assessed with the Amiel-Tison Neurological Evaluation Tool. Nineteen completed the Bayley-III Screening Test (6 did not complete the test due to lack of cooperation). The active medical files of the 4 children for whom contact was lost revealed that at 5 to 7 years of age, none had cerebral palsy or a noted developmental delay.
Of the 25 infants assessed with the Amiel-Tison neurological assessment 6 infants fitted the severe classification and of the 19 infants assessed with the Bayley-III Screening Test, 10 were found at risk in the cognitive category, 2 infants in the receptive language category, 4 in the expressive language category, 5 in the fine motor category and 7 infants were found at risk in the gross motor category. One infant was found at risk in all categories. Nine infants were categorized as having good outcome.
Death or poor outcome (Table 2) were significantly associated with gestational age, severe intraventricular hemorrhage in the first 3 days of life, need for sedation in the second or third day of life and necrotizing enterocolitis.
Association of Main Neonatal Clinical Conditions With Outcome.
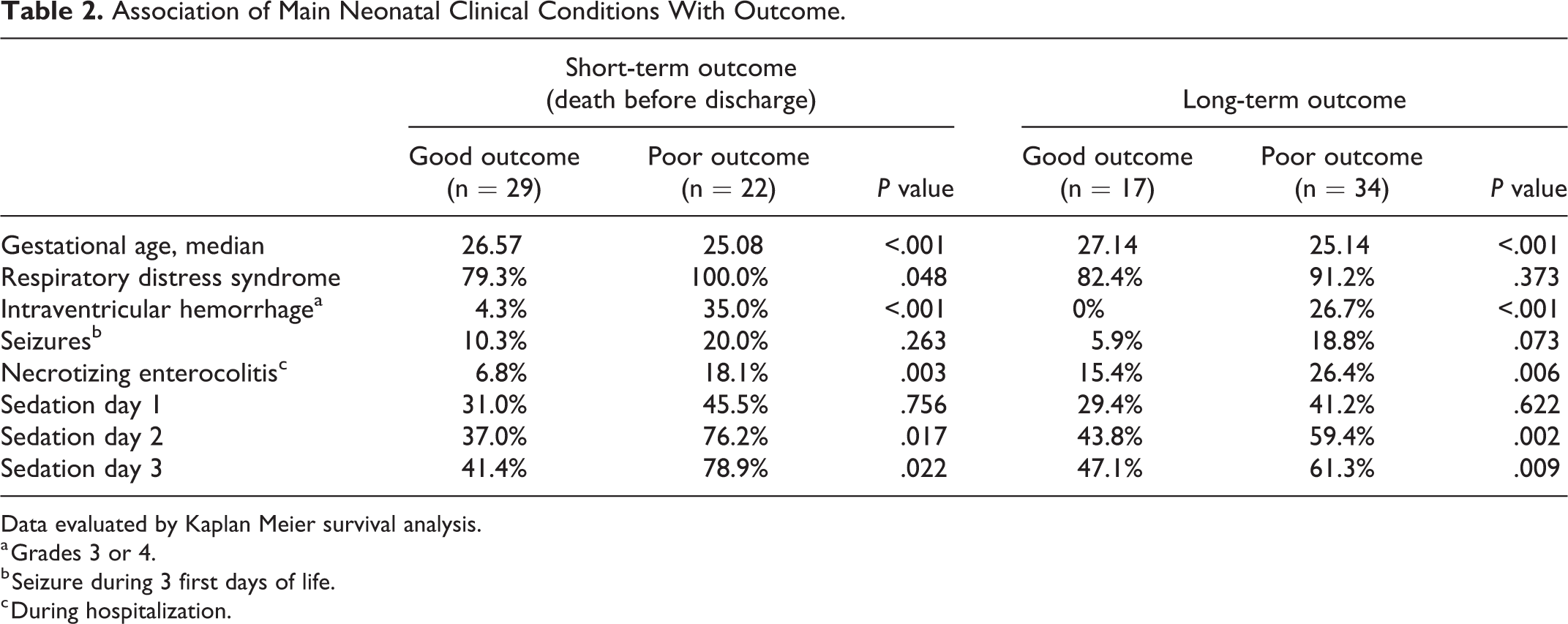
Data evaluated by Kaplan Meier survival analysis.
a Grades 3 or 4.
b Seizure during 3 first days of life.
c During hospitalization.
EEG and Gestational Age
Using simple linear regression, the percentage of time spent with a depressed aEEG background pattern was inversely proportional to gestational age (day 1: beta: –0.071, P < .001, R 2: 0.23; day 2: beta: –0.56, P = .015, R 2: 0.12; day 3: beta: –0.027, P = .004, R 2: 0.17).
Associations of aEEG with Outcome
Depressed aEEG background (over the 75th centile per gestational age) was more prevalent in infants who died before discharge or with poor long-term outcome. Only on the third day of life this association was significant for infants with poor long-term outcome (41 vs 65%, P = .039). Similarly, absence of cycling was significantly associated with death before discharge or poor long-term outcome only on the third day of life (31 vs 74%, P = .004 and 35 vs 50%, P = .012, respectively) (Table 3).
Association of aEEG attributes With Short- and Long-Term Outcome.
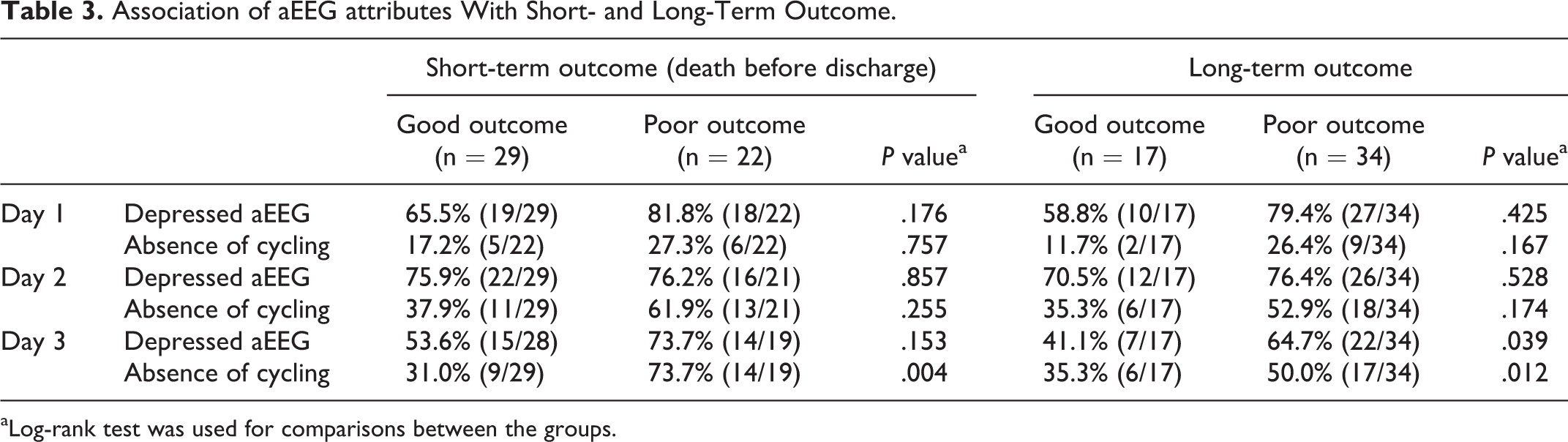
aLog-rank test was used for comparisons between the groups.
Due to the relatively small sample size, 2 multivariable models were designed in relation to the third day of life for each aEEG attributes (background or cycling). Models were adjusted for gestational age and either for severe intraventricular hemorrhage or sedation. In these models, while gestational age, sedation and intraventricular hemorrhage were significant predictors of outcome in nearly all models, depressed background activity and absence of cycling were not found to be independently associated with outcome (Table 4).
Associations of aEEG attributes at the Third Day of Life With Death and Long-Term Outcome (Multivariable Models).
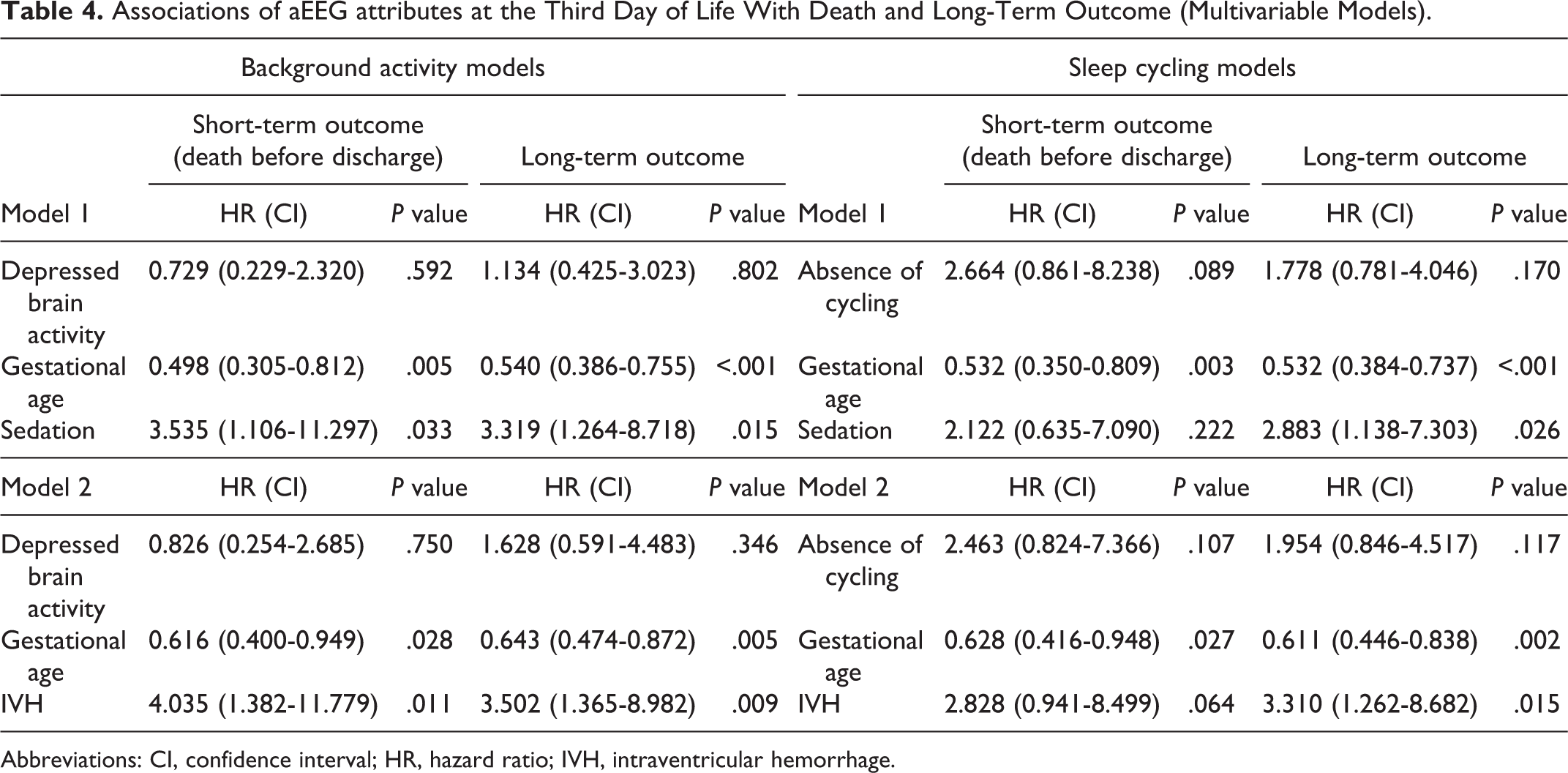
Abbreviations: CI, confidence interval; HR, hazard ratio; IVH, intraventricular hemorrhage.
Discussion
In this prospective study, poor outcome of infants born before 28 weeks’ gestation was associated with aEEG depressed background and absence of cycling in the third day of life. In multivariable models that included gestational age, intraventricular hemorrhage and need for sedation, neither absence of cycling nor depressed background activity were found to be independent predictors of outcome.
Several studies in the last 3 decades assessed the correlation between early aEEG background or cycling phenomenon with long and short-term outcome in premature infants. These studies differed in inclusion criteria, use of sedation, aEEG devices, the aEEG time interval used, the timing of aEEG, the aEEG classification used 5,7,12 and type and age of outcome. Two seminal studies were published by Hellstrom-Westas et al, the first in 1991 27 evaluating 31 infants born less than 33 weeks’ gestation and the second in 2001 11 evaluating 64 babies less than 33 weeks’ gestation with severe intraventricular hemorrhage (grade 3 or 4). The authors reported in both that the presence of cycling and higher percentage of a pattern corresponding to high discontinuity (ie, minimum activity higher than 3 micV) in the first week of life was associated with good outcome. In the latter study, a manual count of burst per minute was performed and a burst density of 130 bursts per hour proved to be the best cut off differentiating between good and poor outcome. Mortality in these studies (35 and 42% in the early and later study respectively), was similar to ours. Several years later, Bowen et al, 17 in the first study using a digital aEEG monitor, employed a classification similar to ours. They assessed 2-hour periods of aEEG recordings during the first 3 days of life in 64 infants less than 29 weeks’ gestation and found that infants who died or had severe intraventricular hemorrhage were less likely to demonstrate cycling and more likely to have a low discontinuous pattern of aEEG. In 2011 El-Dib et al 28 and Klebermass et al 21 published 2 independent studies on the association of aEEG patterns in premature infants and outcome. The first 28 used the Burdjalov score 7 on 70 infants born less than 34 weeks’ gestation and reported that a dysmature score (less than 2 weeks of the expected gestational age) at 1 week of age, but not during the first 2 days of life correlated to abnormal neurodevelopment at the age of 4 months. The second, 21 the largest study to date with 143 neonates less than 30 weeks’ gestational age, reported on weekly 4 hours aEEG recording. In this study, a lower aEEG score and absence of cycling at the first week of life were found to be predictive of long-term outcome. Wikstrom et al 19 in 2012, added to the visual assessment of background activity and cycling a computerized assessment of interburst interval. Similar to the study of Hellstrom-Westas et al, 11 where bursts per hours were manually counted, they reported in a multivariable analysis (adjusted for gestational age), that a 10% increase in the interburst interval percentage during 1 hour of aEEG increased the odds of a worse outcome by 2.2. This concept is attractive as it is related to developmental neurobiology, bursts being considered important for brain wiring during development 29,30 and thus could be expected to demonstrate a predictable pattern of impaired maturation that can be assessed using quantitative aEEG analysis. In another study with a large sample size (n = 139) of infants born between 27 and 32 weeks’ gestation, 20 aEEG was recorded for different time periods within the first 3 days of life. Both a lower Burdjalov score 7 and a lower background severity score were shown in a multivariable analysis to be correlated to abnormal outcome at 18 months corrected age. In the most recent study by Bruns et al, 22 65 infants less than 32 weeks’ gestation at birth were enrolled with a 9.2% mortality in this cohort. Infants were monitored for at least 4 hours daily in the first 3 days of life. In this study, depressed background on day 2 was associated with death before discharge. In multivariable analysis, absence of cycling and depressed background on day 3 were associated with worse mental but not psychomotor developmental index scores.
Despite the many differences between the studies, all have shown some association of different outcomes variables with cycling and/or background aEEG activity. Variations in the predictive values of the different studies are possibly explained by differences in gestational age criteria and varying rates of severe intraventricular hemorrhage and mortality that independently affect outcome and consequently also the predictive value of aEEG. Thus, though aEEG depression or lack of cycling are related to cerebral injury (temporary or permanent), its marginal addition in multivariable models is not always significant.
Detection of moderate to severe brain injury during the NICU hospitalization has been mainly achieved using serial bedside cerebral ultrasonography examinations which have wide variation in reported sensitivities (43-79%) albeit higher specificities (82-95%) for predicting motor outcomes. 31 Infants with poor neurodevelopmental outcome, especially those with cognitive impairment, often show no evidence of cerebral injury on sonography. Studies on brain MRI are reported to have higher sensitivities (65-100%) and specificities (55-97%) for long-term outcome of prematurely born infants, but these studies report results from term equivalent age scans, thus reflecting the entire NICU hospitalization. This study and those cited above demonstrated a significant association between early life aEEG indices with outcome. These data support the concept that much of the cerebral damage in preterm infants is already present at birth or commences very early in life. 2 As the effects of later complications such as late onset sepsis or necrotizing enterocolitis cannot be accounted for, the power of aEEG to predict outcome in premature infants can never be as strong as in term infants after a single acute insult such as HIE.
Strengths and Limitations
The strengths of this study include its prospective design and the careful gestational age verification. There was no selection bias as all preterm infants in the region are born and cared for in a single center and recruited babies mirrored the nonrecruited eligible infants. Also, unlike most of the other studies, the authors assessed an average daily aEEG recording rather than several hours of daily probing. Additionally, the aEEG analysis was performed blinded to the result of neurodevelopment outcome. The assessment of neurodevelopmental outcome was done by an independent observer (EG) unaware of the aEEG findings.
Study limitations include the high mortality rate that prevented a separate assessment of the survivors. The authors consider that using survival analysis and collapsing death and abnormal development to a single poor outcome partly dealt with this shortcoming. Also, 17% of the survivors’ outcome was derived from medical files and not direct examination, however, excluding them from the analysis did not change the results significantly. Lastly, this was a single center study, and thus the results might not be generalized to other units with different epidemiology.
Conclusion
Although the use of continuous aEEG monitoring of premature infants in the NICU is valuable for real-time assessment of cerebral function, reliance on it as a predictive tool for long-term outcome using visual analysis requires caution. Quantitative analysis can enhance the prognostic significance of early aEEG in the clinical setting if it becomes more widely available with the next generation of monitors.
Footnotes
Acknowledgments
We thank all families for their participation in the study. We would also wish to thank Lena Novack, PhD, for her help and review of the statistical analysis.
Author Contributions
JR: Contributed to the design of the study, participated in the assessment and analysis of the data, wrote the first draft of the manuscript and gave a final approval to the final version of the manuscript. SG: Contributed to the design of the study, participated in the statistical analysis of the data, critically revised the manuscript and gave a final approval to its final version. IM: Contributed to the design of the study participated in the data collection and its assessment, critically revised the manuscript and gave a final approval to its final version. AG: Contributed to the design of the study, participated in the data assessment, critically revised the manuscript and gave a final approval to its final version. EG: Contributed to the design of the study, participated in the data collection and its assessment, critically revised the manuscript and gave a final approval to its final version. ES: Conceptualized and designed the study, supervised all steps of data collection, analysis and interpretation, critically revised the manuscript and gave a final approval to its final version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the local ethic committee of Soroka Medical Center. Guardians of all infants recruited signed an informed consent form.