
Abstract
It was recently postulated that because increased genetic load and increased parental age are both purportedly associated with the risk to develop an autism spectrum disorder, there must be a linkage between increasing genetic load and increasing parental age in autism spectrum disorder pathogenesis. The present study examined the hypothesis that if increased genetic load from increasing paternal age is important to autism spectrum disorder pathogenesis, then there should be a significant relationship between increasing parental age and increasing autism spectrum disorder phenotypic severity. Outpatient clinical records were retrospectively examined to identify a consecutive cohort of subjects diagnosed with an autism spectrum disorder (n = 351). Increasing autism spectrum disorder phenotypic severity was found not to be associated with increasing maternal/paternal age. The present study failed to support the hypothesis that increasing parental age was associated with increasing autism spectrum disorder phenotypic severity, but future studies should examine the relationship between genetic mutations in subjects diagnosed with an autism spectrum disorder and increasing parental age.
Autism spectrum disorder is a neurodevelopmental disorder that is characterized by qualitative impairments in social interaction, qualitative impairments in communication, and restricted and stereotyped patterns of behavior, interests, and activities. 1 Although an autism spectrum disorder diagnosis is defined by these 3 core features, recent investigations have described many health, physical, or behavioral comorbid conditions consistently associated with an autism spectrum disorder such as gastrointestinal disturbances, incontinence, sleep problems, eating disorders, behavioral problems, and sensory processing issues. 2
In order to explain the etiologic basis of autism spectrum disorder, a recent hypothesis was postulated that the increase in mutation rates seen in some studies of subjects diagnosed with an autism spectrum disorder and the increased rate of de novo mutations observed by some studies in older fathers might make paternal age a factor in autism spectrum disorder pathogenesis. 3 In support of their hypothesis, these investigators conducted a study of genomewide mutation rates by sequencing the entire genomes of 78 Icelandic parent-offspring trios at high coverage. These investigators reported that in their samples, with an average father’s age of 29.7 years, the average de novo mutation rate is 1.20 × 10–8 per nucleotide per generation. According to the investigators, most notably, the diversity in mutation rate of single-nucleotide polymorphisms is dominated by the age of the father at conception of the child, and the paternal age effect is an increase of about 2 mutations per year of age. In addition, these investigators described observing dispersion in the number of maternal de novo mutations, and that the recombination rate is higher for women than men. The children of older mothers have more maternal recombinations than those of young mothers; however, men transmit a much higher number of mutations to their children than do women.
In support of increasing parental age as a risk factor for an autism spectrum disorder diagnosis, investigators conducted a case-control study of parental age and the risk of the offspring being diagnosed with an autism spectrum disorder in a Finnish national birth cohort. 4 These investigators used conditional logistic regression models to observe that advanced paternal age (39-49 years) was associated with childhood autism in offspring, whereas advanced maternal age was associated with both Asperger syndrome and pervasive developmental disorder in offspring ≥ 35 and ≥ 40 years, respectively. Similarly, other investigators conducted a cohort study of children to evaluate the possible association between parental age and autism spectrum disorder in Denmark. 5 These investigators observed that both maternal and paternal age were associated with a greater risk of autism spectrum disorder in the offspring.
Overall, as described by investigators, because increased genetic load and increased parental age are both purportedly associated with the risk to develop a variety of clinical neuropsychiatric disorders such as an autism spectrum disorder, there must be a linkage between increasing genetic load and increasing parental age in autism spectrum disorder pathogenesis. 6 In light of this theory, we hypothesized that if increased genetic load from increasing paternal age is important to autism spectrum disorder pathogenesis, then there should be a significant relationship between increasing parental age and increasing autism spectrum disorder phenotypic severity of subjects diagnosed with an autism spectrum disorder.
Methods
Study Subjects
The present study examined a consecutive qualifying cohort of subjects diagnosed with an autism spectrum disorder (n = 351) who were recruited from retrospective examination of medical charts of patients presenting for outpatient genetic consultations at the ASD Centers, LLC. All of the study subjects were previously diagnosed with Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria autism or autism spectrum disorder by a trained professional.
Clinical Evaluation
At the time of their initial clinical presentation, the subjects examined in the present study had extensive medical histories taken by trained healthcare professionals. Information collected on each of the subjects included: subject’s age at initial clinical evaluation, gender (male or female), autism spectrum disorder classification (any type of developmental regression after birth or no developmental regression after birth), parental age at subject’s birth (maternal and paternal), and a parent/guardian completed Autism Treatment Evaluation Checklist at initial clinical evaluation.
The Autism Treatment Evaluation Checklist quantitatively evaluates overall skills in a number of areas in subjects diagnosed with an autism spectrum disorder, including subscales in the areas of speech/language/communication, sociability, sensory/cognitive awareness, and health/physical/behavior. The Autism Treatment Evaluation Checklist was used to measure the phenotypic severity of subjects diagnosed with an autism spectrum disorder by measuring autism spectrum disorder severity (ie, the greater the autism spectrum disorder phenotypic severity, the greater the Autism Treatment Evaluation Checklist severity score).
Statistical Evaluation
In order to evaluate the effects of parental age on the phenotypic severity of subjects diagnosed with an autism spectrum disorder, the statistical package in SAS version 9.1 was utilized. The regression procedure was used to construct a statistical model in SAS to evaluate the relationship between maternal age and paternal age at the time of a subject’s birth and total Autism Treatment Evaluation Checklist and Autism Treatment Evaluation Checklist subscale scores. The subject’s age at the time of initial clinical presentation when the Autism Treatment Evaluation Checklist was completed was entered into the model as a covariable. The null hypothesis was that maternal or paternal ages at the time of a subject’s birth would not be related to total Autism Treatment Evaluation Checklist or Autism Treatment Evaluation Checklist subscale scores. As an additional positive control analysis, the regression procedure was used to construct a statistical model in SAS to evaluate the relationship between the subject’s age at the time of initial clinical presentation when the Autism Treatment Evaluation Checklist was completed and total Autism Treatment Evaluation Checklist and Autism Treatment Evaluation Checklist subscale scores. It was a priori hypothesized that the speech/language/communication Autism Treatment Evaluation Checklist subscale should significantly improve with increasing age of the subject diagnosed with an autism spectrum disorder at initial clinical presentation. This is because investigators previously reported that subjects diagnosed with an autism spectrum disorder were observed to have changes in communication reflected by acquisition of language as a function of age. 7 The null hypothesis was that the subject’s age at initial clinical presentation would not be related to total Autism Treatment Evaluation Checklist or Autism Treatment Evaluation Checklist subscale scores. In all statistical tests conducted, a 2-sided P value <.05 was considered statistically significant.
Results
Table 1 summarizes the overall demographic information on the cohort (n = 351) examined in the present study. It was observed that males predominated in the cohort examined with a male-female ratio of 4.6:1. It addition, it was observed that subjects diagnosed with an autism spectrum disorder that experienced any type of developmental regression following birth (52%) slightly predominated over subjects diagnosed with an autism spectrum disorder that did not experience any type of developmental regression following birth (48%).
An Overview of the Study Cohort (n = 351) Examined.
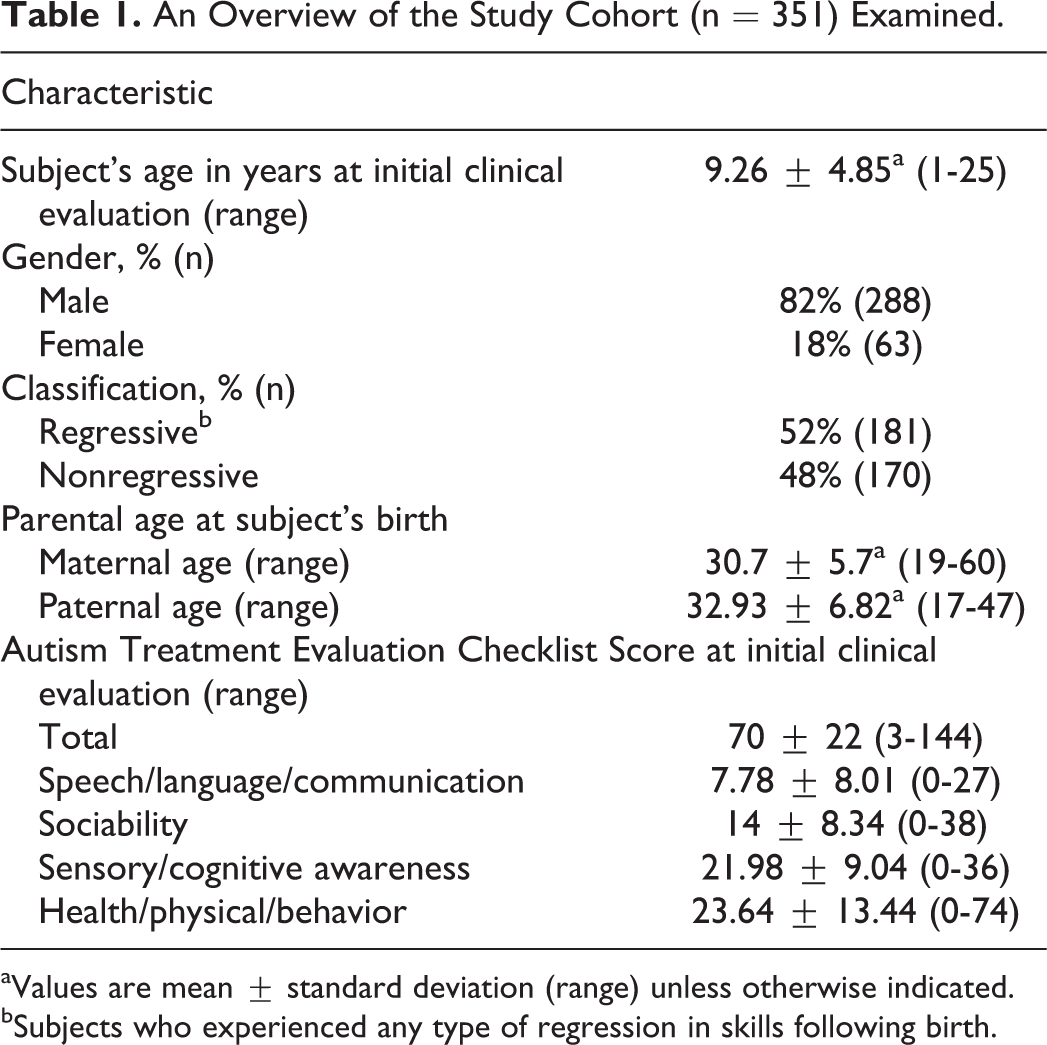
aValues are mean ± standard deviation (range) unless otherwise indicated.
bSubjects who experienced any type of regression in skills following birth.
Tables 2 and 3 evaluate the relationship between autism spectrum disorder phenotype measured using the Autism Treatment Evaluation Checklist and maternal and paternal age, respectively. Overall, it was observed that no significant relationships were observed between increasing autism spectrum disorder phenotypic severity and increasing maternal or paternal age, except for a significant inverse relationship between increasing maternal age and decreasing autism spectrum disorder phenotypic severity for the Autism Treatment Evaluation Checklist subscale of sociability (ie, older maternal age was associated with improved sociability).
A Summary of the Relationship Between Maternal Age at the Time of Subject’s Birth and ATEC Scores.
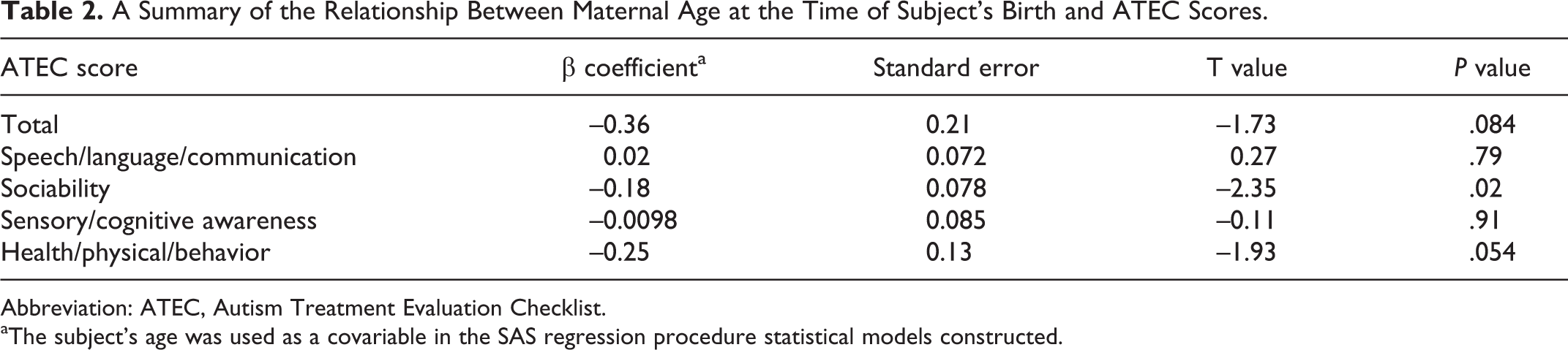
Abbreviation: ATEC, Autism Treatment Evaluation Checklist.
aThe subject’s age was used as a covariable in the SAS regression procedure statistical models constructed.
A Summary of the Relationship Between Paternal Age at the Time of Subject’s Birth and ATEC Scores.
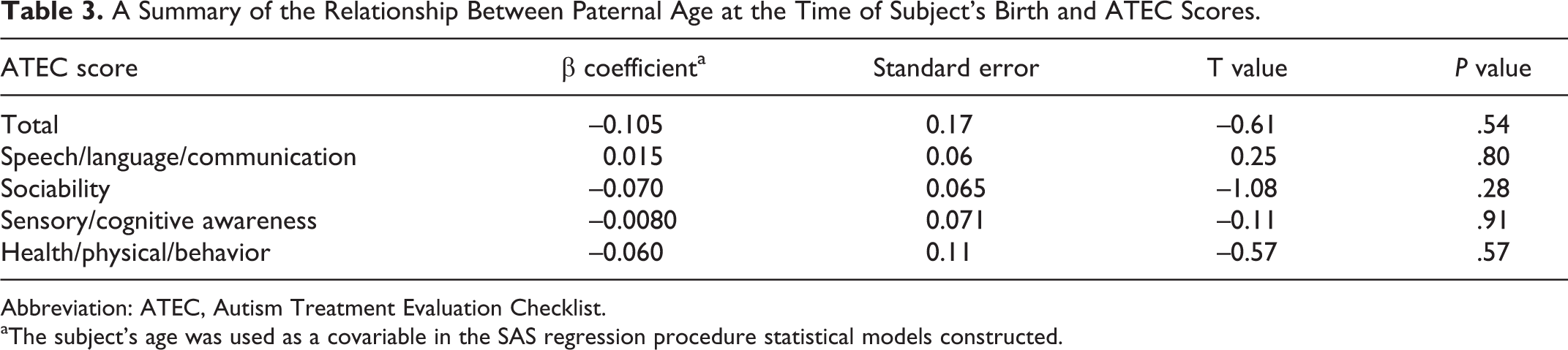
Abbreviation: ATEC, Autism Treatment Evaluation Checklist.
aThe subject’s age was used as a covariable in the SAS regression procedure statistical models constructed.
Table 4 evaluates the relationship between autism spectrum disorder phenotypic severity measured using the Autism Treatment Evaluation Checklist and the age of subjects diagnosed with an autism spectrum disorder. Overall, it was observed that total Autism Treatment Evaluation Checklist scores trended to improve with increasing subject’s age at initial clinical presentation. Among the various Autism Treatment Evaluation Checklist subscales, as was a priori predicted, it was observed that speech/language/communication Autism Treatment Evaluation Checklist subscale significantly improved with increasing subject’s age at initial clinical presentation.
A Summary of the Relationship Between Subject’s Age at the Initial Clinical ATEC Evaluation and ATEC Scores.
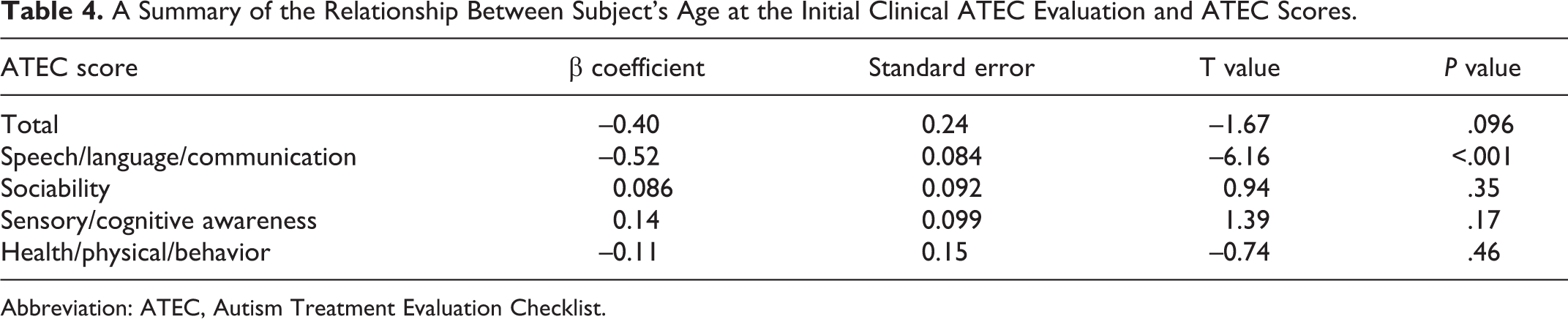
Abbreviation: ATEC, Autism Treatment Evaluation Checklist.
Discussion
The present study, utilizing a novel method to evaluate the potential relationship between increasing paternal age and increasing autism spectrum disorder phenotypic severity, failed to find a significant relationship. In contrast to the potential hypothesized relationship between increasing parental age and increasing autism spectrum disorder phenotypic severity, it was observed that there was a significant inverse relationship between maternal age and autism spectrum disorder phenotypic severity for the Autism Treatment Evaluation Checklist sociability subscale. Consistent with the a priori hypothesized relationship between increasing subject’s age at initial clinical presentation and Autism Treatment Evaluation Checklist scores, particularly relating to speech/language/communication skills, it was observed that increasing subject age at initial clinical presentation was significantly correlated with improved speech/language/communication subscale scores. Overall, it is apparent that our observations provide important insights into the apparent lack of a relationship between increasing parental age and increasing autism spectrum disorder phenotypic severity.
In further considering the biological plausibility of the results observed in the present study, a recent study specifically aimed to address whether paternal age impacted the burden of structural genomic deletions and duplications in copy number variation burden in a large population from the Netherlands (n = 6773). 6 These investigators observed no evidence to support the effect of paternal age on copy number variation load in the offspring, and their results were also negative for global measures as well as several proxies for de novo copy number variation events. These investigators concluded that their results strongly suggest that the level of global copy number variation burden is not influenced by increased paternal age. In addition, these investigators suggested that it remains possible that local genomic effects may exist for specific phenotypes, but their study indicates that global copy number variation burden and increased father’s age may be independent disease risk factors. In addition, other investigators recently evaluated the role of de novo mutations in subjects diagnosed with an autism spectrum disorder by sequencing the exomes of autism spectrum disorder cases and their parents (n = 175 trios). 8 Fewer than half the cases (46.3%) carry missense or nonsense de novo variants, and the overall rate of mutation is only modestly higher than the expected rate. These investigators determined that there is a small increase in the rate of de novo events, which, when taken together with their protein interaction results, are consistent with an important but limited role for de novo point mutations in subjects diagnosed with an autism spectrum disorder. Similar results have been documented for de novo copy number variations. Overall, the investigators concluded that genetic models incorporating the investigator’s data indicate that most of the observed de novo events are unconnected to autism spectrum disorder; those that do confer risk are distributed across many genes and incompletely penetrant (ie, not necessarily sufficient for disease). Furthermore, with respect to the relationship between increasing paternal age as a risk factor for an autism spectrum disorder described in the aforementioned studies from Finland and Denmark, 4,5 a recent cohort study on children diagnosed with an autism spectrum disorder in the US state of New Jersey failed to find a significant relationship between increasing maternal or paternal ages and the risk of an autism spectrum disorder diagnosis. 9 This observation is consistent with the no-effect relationship observed in the present study, also on US children.
It is also important to consider for the hypothesis tested in the present study that there should be a linkage between increasing genetic load and increasing parental age in autism spectrum disorder pathogenesis. 6 The observation that increasing parental age is associated with increased single-nucleotide mutations does not directly translate into changes of copy number variations in subjects. These 2 types of genetic changes are distinct from one another. Namely, single-nucleotide mutations involve single base pairs in the genome, whereas copy number variations involve large swaths of the genome (ie, multiple large sequences of genes) either being deleted or repeated.
Furthermore, it is interesting to hypothesize that because copy number variations are based on an analysis of the frequency of observing specific single-nucleotide polymorphisms at specific intervals in the genome 10 that if increasing parental age increases the frequency of single-nucleotide mutations, it is possible that increasing parental age may generate apparent changes in copy number variations that are not genuinely present in a person’s genome. As a corollary to this, if increased parental age is associated with an autism spectrum disorder diagnosis, it would further complicate any attempts to evaluate true differences in the frequency of copy number variations among subjects diagnosed with an autism spectrum disorder in comparison to neurotypical controls. This would occur because increased parental age among subjects diagnosed with an autism spectrum disorder should be associated with an increased frequency of single-nucleotide mutations in these subjects, and increased single-nucleotide mutations should increase the frequency of screening identified copy number variations among subjects diagnosed with an autism spectrum disorder relative to neurotypical controls with younger parental age, decreased single-nucleotide mutations, and a lower frequency of screening-identified copy number variations. If this phenomenon is true, then the small increase in copy number variations observed in some studies of subjects diagnosed with an autism spectrum disorder in comparison to neurotypical controls may simply be due to false positives generated by their higher frequency of single-nucleotide mutations, possibly related to the older ages of their fathers.
Finally, the theory that mutations generate sequence diversity and provide a substrate for selection, and as a result the rate of de novo mutations is therefore of major importance to evolution, 3 is well accepted. However, it is entirely a different case to suggest that the increasing rate of de novo mutations associated with increasing paternal age is a causal factor in autism spectrum disorder pathogenesis. This is so because whatever de novo mutations occur with increasing parental age, they should occur in a random fashion throughout the entire genome. In order to be of importance to autism spectrum disorder pathogenesis, presumably, the mutations would have to occur in specific genes at specific locations. Additionally, if genetic mutations do result in individuals diagnosed with an autism spectrum disorder phenotype, selective pressure would probably strongly select against such individuals, because they are less likely to thrive and are less likely to produce offspring.
Strengths and Limitations
A significant strength of the present study was its overall study design using a large retrospective consecutive cohort of subjects professionally diagnosed with an autism spectrum disorder using the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria. As such, the sample examined was not influenced by investigators choosing to examine subjects diagnosed with an autism spectrum disorder with specific features that might influence the results of the study. In addition, the diagnoses were previously made by trained professionals prior to the present study using recognized criteria, so as to ensure that all the subjects examined had an autism spectrum disorder. Similarly, because the information on the subjects was collected as part of the routine clinical care, the investigators and parents that provided the information analyzed in the present were completely unaware of the methods of analyses employed in the present study. Also, the overall size and statistical model techniques employed ensured that the present study had adequate statistical power to detect significant associations between increasing parental age and autism spectrum disorder phenotypic severity. Furthermore, given the overall demographic similarities in the autism spectrum disorder cohort examined in the present study with that of other studies, the results should have applicability to other autism spectrum disorder cohorts, but we recommend that future studies should be conducted in other autism spectrum disorder cohorts to determine their consistency with our observations.
An additional strength of the present study was that all of the subjects examined were diagnosed with an autism spectrum disorder. This ensured that factors related to study participation that may influence the selection of neurotypical controls who may or may not participate in a study did not impact the results, and further factors associated with an autism spectrum disorder diagnosis in comparison to neurotypical children were minimized because all of the subjects examined were diagnosed with an autism spectrum disorder.
Another strength of the present study was the use of parental completed Autism Treatment Evaluation Checklists to measure the clinical phenotypic severity of subjects diagnosed with an autism spectrum disorder. The Autism Treatment Evaluation Checklist is an inexpensive and accurate method to evaluate autism spectrum disorder phenotypic severity. The Autism Treatment Evaluation Checklist provides quantitative total scores and subscale scores for specific domains in autism spectrum disorder symptoms, and in recent studies was found to significantly correlate with other established quantitative measures of autism spectrum disorder phenotypic severity such as the Childhood Autism Rating Scale. 1
Among the potential limitations of the present study was that no neurotypical controls were examined. We believe it may be worthwhile to study parental ages among subjects diagnosed with an autism spectrum disorder in comparison to neurotypical controls, but the present study went further than this simple comparison to determine whether increasing parental ages were functionally important to the overall clinical symptoms of subjects diagnosed with an autism spectrum disorder. As a consequence, the present study provides important data to support the apparent lack of mechanistic relationship between increasing parental age and increasing autism spectrum disorder phenotypic severity. We recommend that future studies examine the subset of individuals diagnosed with an autism spectrum disorder and have a known genetic anomaly to evaluate the potential relationship between increasing parental age and the frequency of known genetic anomalies in subjects diagnosed with an autism spectrum disorder.
Finally, although the present study was not specifically designed to evaluate the mean maternal ages in neurotypical and subjects diagnosed with an autism spectrum disorder, it was observed that the overall mean maternal age of 30.7 years in the autism spectrum disorder cohort examined was similar to the overall mean maternal age of 29 years observed in other general population cohorts from the United States. 11 This suggests that the maternal ages for subjects diagnosed with an autism spectrum disorder in the present study were not grossly different from the general population in the United States.
Another potential limitation of the present study was that only Autism Treatment Evaluation Checklist scoring was used to measure autism spectrum disorder phenotypic severity. Despite this limitation, the Autism Treatment Evaluation Checklist has been validated in previous studies for its usefulness in quantitatively measuring autism spectrum disorder overall and specific domains phenotypic severity. In addition, the present study examined subjects diagnosed with an autism spectrum disorder under the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria, which has since the time of the execution of our study been replaced with the manual’s fifth edition (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) criteria. We recommend that future studies evaluating the potential relationship between increasing parental age and autism spectrum disorder phenotypic severity utilize other measures of autism spectrum disorder phenotypes to observe their consistency with our results.
Conclusions
The present study provides important new insights into the apparent lack of an association between increasing parental age and increasing autism spectrum disorder phenotypic severity. The results of the present study support several recent studies that have also failed to observe a significant association between increasing parental age and genetic burden as measured by copy number variations. It is apparent from the results of the present study, in conjunction with genetic observations among subjects diagnosed with an autism spectrum disorder, that most observed de novo genetic events are unconnected to an autism spectrum disorder diagnosis, and those that do confer risk are distributed across many genes and are not necessarily sufficient for disease. Future studies should further explore the potential relationship between increasing parental age and the frequency of known genetic anomalies among subjects diagnosed with an autism spectrum disorder.
Footnotes
Author Contributions
DG was the main writer and was involved in analysis of the data. BH was the main computer programmer involved in analysis of the data and drafting the manuscript. JK was involved in drafting, reviewing, and editing the manuscript. LS was involved in drafting and editing the manuscript. MG was involved in study design, analysis of the data, and drafting of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the nonprofit Institute of Chronic Illnesses, Inc, and the nonprofit CoMeD, Inc.
Ethical Approval
The present study received Institutional Review Board approval from the Liberty IRB, Inc (Deland, FL), to retrospectively review clinical data generated from patients presenting for clinical care to the ASD Centers, LLC, clinics (IRB Tracking# 12.08.0023).