
Abstract
Plasticity of language function after brain damage can depend on maturation of the brain. Children with left-hemisphere perinatal (n = 7) or childhood stroke (n = 5) and 12 controls were investigated using functional magnetic resonance imaging. The verb generation and the sentence comprehension tasks were employed to activate the expressive and receptive language areas, respectively. Weighted laterality indices were calculated and correlated with results assessed by neuropsychological test battery. Compared to controls, children with childhood stroke showed significantly lower mean scores for the expressive (P < .05) and receptive (P = .05) language tests. On functional magnetic resonance imaging they showed left-side cortical activation, as did controls. Perinatal stroke patients showed atypical right-side or bilateral language lateralization during both tasks. Negative correlation for stroke patients was found between scores for expressive language tests and laterality index during the verb generation task. (Re)organization of language function differs in children with perinatal and childhood stroke and correlates with neurocognitive performance.
Keywords
Cognitive functions in early childhood develop in the context of complex adaptive processes determined by genetic and environmental factors. 1,2 Healthy newborns have no dominance in language perception and expression, which start to develop from the third month of age. 3 Language lateralization in the left hemisphere is mostly completed by the age of 5 years; 4 however, there is evidence that lateralization deepens throughout childhood long into adolescence. 1,5
Perinatal and childhood stroke occurs most often in the territory of the brain supplied by the middle cerebral artery 6 –8 and can therefore devastate classical language areas in the left frontal and temporal lobes. 9–10
Brain damage after perinatal stroke may cause compensatory (re)organization of the language network. 11 –14 After damage of both cortical and subcortical structures, 14 other areas in the brain take over the functions of the damaged area. In children with stroke, the remarkable plasticity of the developing brain in cognitive functions has been well documented 13,15,16 and these children usually have normal IQ in early school age 6,15 and a normal language with compensatory reorganization of the language network. 11 –14 However, neurocognitive development of children with congenital unilateral brain lesion is different compared to healthy children, 17 and initial subtle delays or difficulties may gradually develop into significant cognitive problems during the school years. 17 –19
Plasticity after brain damage can depend on the maturation of the brain and can be different in children with perinatal and childhood stroke. Previous functional magnetic resonance imaging (MRI) studies have shown that early left-side subcortical damage resulted in dramatic right hemisphere reorganization of language function, 11,14,20 whereas others have found less striking contralateral reorganization following lesions with a later onset. 10,12,13,21
There are only a few studies showing the effect of brain maturation on language lateralization and cognitive development in children after stroke. 13,21 Therefore, the aim of our study was to ascertain lateralization patterns of language function in children with perinatal and childhood stroke in comparison to healthy children and to identify how changes in the organization of language function correlate with results of neurocognitive performance.
Material and Methods
Patients
Twelve children with stroke (6 girls, 6 boys, age range 6.3-13.8 years) and 12 age-matched healthy controls (7 girls, 5 boys, age range 8.4-13.9 years; Table 1) without contraindications for MRI were investigated using functional MRI and the neuropsychological test battery NEPSY for cognitive examination.
Individual Patient Information: Demographic and Neurological Characteristics, Weighted Mean Laterality Index Values in Brodmann Areas 44 + 45 and Brodmann Area 22 During the Verb Generation (VG) and the Sentence Comprehension (SC) Tasks, and NEPSY Scores in Patients and Controls.
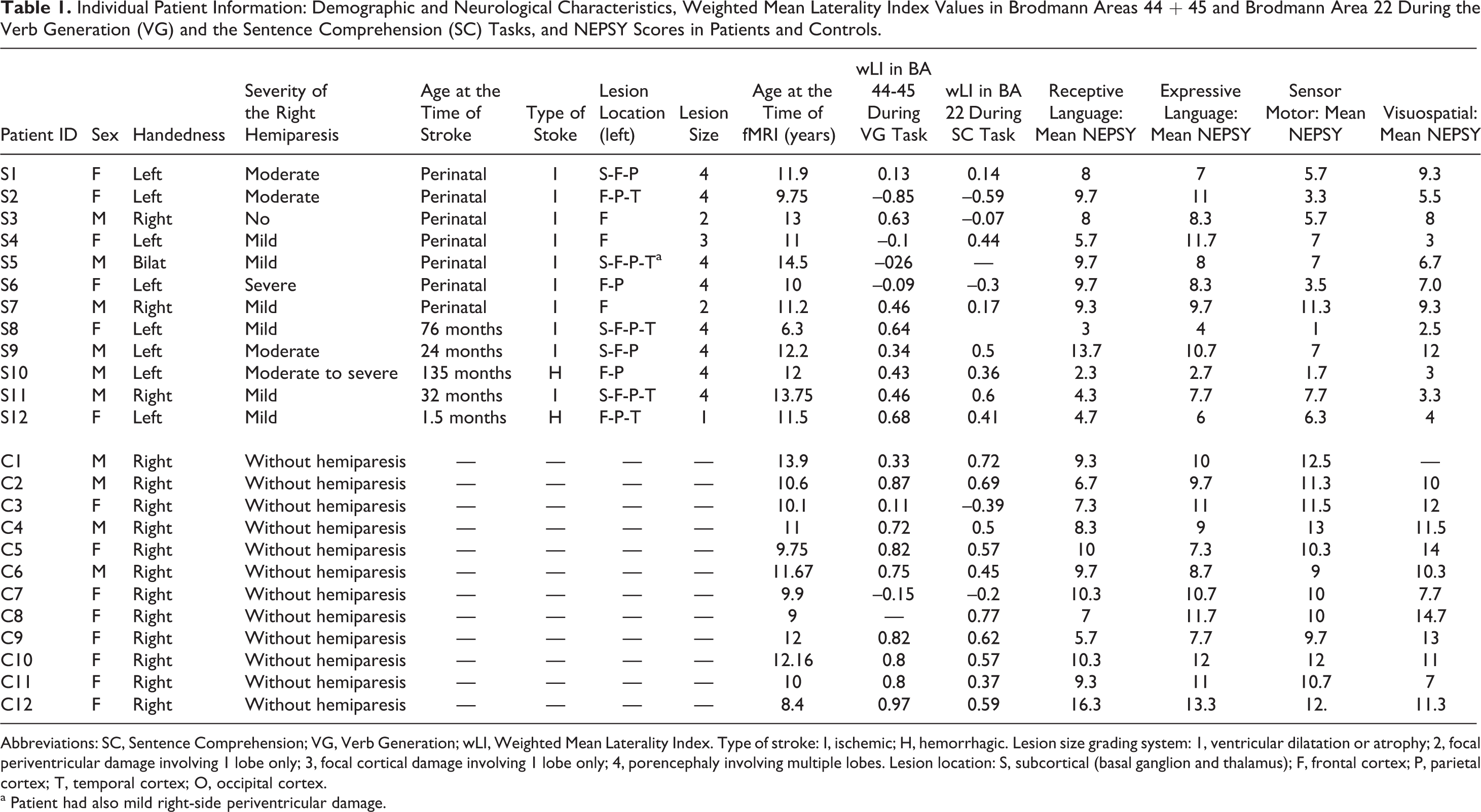
Abbreviations: SC, Sentence Comprehension; VG, Verb Generation; wLI, Weighted Mean Laterality Index. Type of stroke: I, ischemic; H, hemorrhagic. Lesion size grading system: 1, ventricular dilatation or atrophy; 2, focal periventricular damage involving 1 lobe only; 3, focal cortical damage involving 1 lobe only; 4, porencephaly involving multiple lobes. Lesion location: S, subcortical (basal ganglion and thalamus); F, frontal cortex; P, parietal cortex; T, temporal cortex; O, occipital cortex.
a Patient had also mild right-side periventricular damage.
All stroke patients had unilateral left-hemisphere stroke: perinatal stroke in 7 (3 boys and 4 girls) and childhood stroke in 5 patients (3 boys and 2 girls). Eight children were left-handed and 4 were right-handed (3 with mild hemiparesis and 1 without paresis). At the time of the functional MRI investigation there was no age difference between children with perinatal stroke (mean age (95%CI) 11.6 (10.1-13.2) years) or childhood stroke (11.2 (7.6-14.7) years) and controls (10.7 (9.7-11.7) years). Median age (min-max) at the onset of childhood stroke was 32 months (1.5 months-135 months).
Patients were identified, using the Estonian Pediatric Stroke Database, on the basis of an epidemiological study (1995-2006). They were considered for participation if They had documented left-hemisphere perinatal or childhood stroke They were between the ages of 6 and 14 years Stroke was sustained more than 1 year before functional MRI and neurocognitive testing They were fluent in the Estonian language Their hearing was normal
All patients had ischemic or hemorrhagic stroke in origin and the lesion’s size of the stroke was graded according to modified version of Westmacott et al 18 (Table 1). All children with perinatal stroke had ischemic genesis of stroke 22 but in patients with childhood stroke 3 were of ischemic and 2 were of hemorrhagic origin. Two children with childhood stroke had seizures: 1 with ischemic stroke and the other with hemorrhagic stroke. Stroke patients had a history of normal first-year cognitive development, and their psychometric intelligence quotient according to the Kaufman Assessment Battery for Children was higher than 80. All children attended a normal school and class appropriate for their age.
Stroke patients born before 36 weeks of gestation, infants with presumed perinatal stroke, and children with other documented diseases involving the central nervous system (eg, severe birth asphyxia, kernicterus, encephalitis, mitocondrial disease, tumor, and postictal hemiparesis) were excluded from the study.
Controls
The control group consisted of 12 age-matched healthy children (5 boys, 7 girls) from regular public schools in Tartu (Table 1). Control children were right-handed native Estonian speakers, with normal hearing, without neurological diseases or psychiatric disorders; they were not taking medications affecting the central nervous system and had no past or current cognitive deficits.
Neuropsychological Assessment
All children were individually tested with the Developmental Neuropsychological Assessment battery NEPSY 23 (Table 1), which was used for assessment of neuropsychological development in previous studies and was adapted to the Estonian language by Kolk and Talvik. 17 The comprehensive neuropsychological battery consists of the receptive and productive language subtests, as well as of the subtests of visuospatial, sensorimotor, executive functions, attention, and memory. Normal values of test scores are 10 ± 3. Neurocognitive testing was performed within 1 month before or after the functional MRI investigation in control children and 1 day before or after functional MRI in stroke patients. The data of the Developmental Neuropsychological Assessment battery tests conducted by the neuropsychologist were not available for the neuroradiologist or the physicist during analysis of the functional MRI investigation.
MRI
Image Acquisition
Anatomical and functional images were obtained on a 1.5 T magnetic resonance scanner Magnetom Symphony (Siemens Medical Systems, Erlangen, Germany). Axial fluid-attenuated inversion recovery images and high-resolution anatomical T1-weighted 3D images (176 sagittal images, matrix 224 × 256, voxel size 1 × 1 × 1 mm3) were obtained first. For functional imaging Echo Planar Imaging (EPI) sequences (time of repetition (TR) = 4030 ms, time to echo (TE) = 50 ms, 36 axial slices, thickness 3 mm, a gap of 0.75 mm between neighboring slices for decreasing cross-talk between slices, matrix 64 × 64, voxel size 3 × 3 × 3.75 mm3) were used. The whole brain including the cerebellum was covered.
The median (min-max) interval between stroke and functional MRI assessment was 10.2 years (1-11.2) for childhood stroke and 11.6 years (9.8-14) for perinatal stroke. According to the MRI investigation, all stroke patients had a lesion in the area of the left middle cerebral artery but the size and location of the lesions varied among the patients. In the neonatal stroke group, 3 patients had cortical/subcortical damage, 1 of them had also damage in the basal ganglia, and 4 patients had periventricular white matter injury. Three patients with childhood stroke sustained cortical/subcortical damage, 2 of them had lesions remote from the cortical grey matter in deep brain structures (basal ganglia, thalamus), and 2 had periventricular white matter injury. There were no statistical differences in the number of cases with periventricular white matter injury among the perinatal or childhood stroke patients.
The Functional MRI Scanning Paradigm
The subjects in this study completed 2 language tasks with auditory presentation which has been shown to produce more reliable language lateralization function than visual presentation. 5,9,24 Also the young age of some of the subjects precluded the use of printed word prompts. Prior to entering the scanner, the children were trained to perform the tasks using different sets of words and sentences. The subject was instructed to think and comply with the task during the study silently to minimize the motion artifacts associated with speech. The tasks were recorded in a male voice. In a periodic block design 5 blocks of study and control tasks were used. In each block 30-second periods of the language task were interleaved with 30-second periods of the control task while children performed finger tapping. After the study the subject was asked about words and sentences to verify how he or she had heard them.
During the control block the subject was instructed to tap sequentially the fingers to the thumb, the rate of sequential tapping was self-paced. The control task was designed to control for the auditory prompt used in the task, to distract the subject from task compliance during the control period, to provide observable confirmation of compliance with the task, and to provide activation of motor strip as reference data for each subject.
The verb generation task to activate expressive language area in the frontal lobe was based on the task described for functional MRI by Benson et al 25 and used for children. 5,9,20,26 The task involves presentation of a series of concrete nouns for which subjects are required to name an action associated with each. For example, if the noun “ball” is presented, the subject might generate verbs like “throw,” “kick,” or “hit.”
A second task was the sentence comprehension task to activate the receptive language areas in the temporal lobe. 24,27 Upon hearing a sentence, the subject was asked to silently decide if it was right or wrong (“the bird is singing vs the bird is barking”). The ratio of the right to the wrong sentences was 7:1.
Both tasks were performed by all children. In case initial evaluation of the functional MRI investigation on the workstation of the MRI scanner showed bilateral activation, at least 1 extra attempt was made to ensure correctness of the data. The initial study group included 27 children (13 controls and 14 stroke patients); however, 1 control subject and 2 stroke patients were excluded from the study because they were not able to perform either of the functional MRI tasks after several attempts. Thus, the total success rate for the verb generation task was 85% (23/27) and for the sentence comprehension task was 81% (22/27).
Twelve control subjects and 12 stroke patients who completed at least 1 technically acceptable functional MRI task were included in the study. One girl in the control group was unable to comply with the requirements of the functional MRI scans during the verb generation task as she was too anxious, but she was able to perform the sentence comprehension task. One girl with childhood stroke (age 6.3 years) and 1 boy with perinatal stoke (14 years) were excluded from the final analysis of the sentence comprehension task due to short attention spans and motion artifacts.
Postprocessing of the Functional MRI Data
The first results were visualized on the workstation of the MRI scanner using the software Syngo MR A30 (Siemens Medical Systems). Image analysis was performed using the Statistical Parametrical Mapping software (Wellcome Trust Centre for Neuroimaging, University College, London, UK) based on MATLAB (Math Works, Natick, MA, USA). The resulting t-maps for each subject were analyzed within the Brodmann areas 44 + 45 (frontal lobe) and Brodmann areas 22 (temporal lobe) as defined by the MRIcro templates. The weighted mean laterality indices were calculated using combined bootstrap/histogram analysis by Wilke and Schmithorst. 28 A positive weighted mean laterality index value indicates left hemisphere lateralization and a negative value indicates right lateralization. Values close to zero (ie, weighted mean laterality index –0.2 … 0.2) show bilateral activation. 5,21
Statistical Analysis
Additional statistical evaluation was performed with the statistical package SAS version 9.1 (SAS Institute Inc, Cary, NC). Prior to further analysis the normality of the data was evaluated using the Kolmogorov–Smirnov criterion. The nonparametric Mann–Whitney U-test and the Wilcoxon test were employed to compare the laterality indices and the Developmental Neuropsychological Assessment battery test results for the study groups. Spearman’s and Pearson’s correlation coefficients were used to analyze correlations. To examine the association between the variables, simple linear regression was used. Values are given as means with the 95% confidence interval. All P values are 2-sided. The accepted level for statistical significance was P < .05.
Statement on Ethics
This study was approved by the Ethics Review Committee on Human Research, University of Tartu. Informed consent for participation in the study was obtained from the parents of the patients.
Results
Neurocognitive Performance in Children With Stroke
Children with stroke showed significantly lower mean scores for expressive language (P < .05), for sensorimotor function (P < .001), and for visuospatial function (P < .01) compared to controls (Table 2). Children with childhood stroke had significantly lower mean scores for the expressive (P < .05) and receptive language (P = .05) subtests compared to controls. At the same time, patients with perinatal stroke showed no significant differences both for expressive and receptive language compared to controls. However, children with perinatal or childhood stroke showed significantly lower mean scores for the sensorimotor (P < .01) and visuospatial function tests (P < .05) compared to control children, without significant differences between the stroke groups.
Mean Values of the Cognitive Function Tests (95% Confidence Interval) According to the Developmental Neuropsychological Assessment Battery in Stroke Patients and Controls.
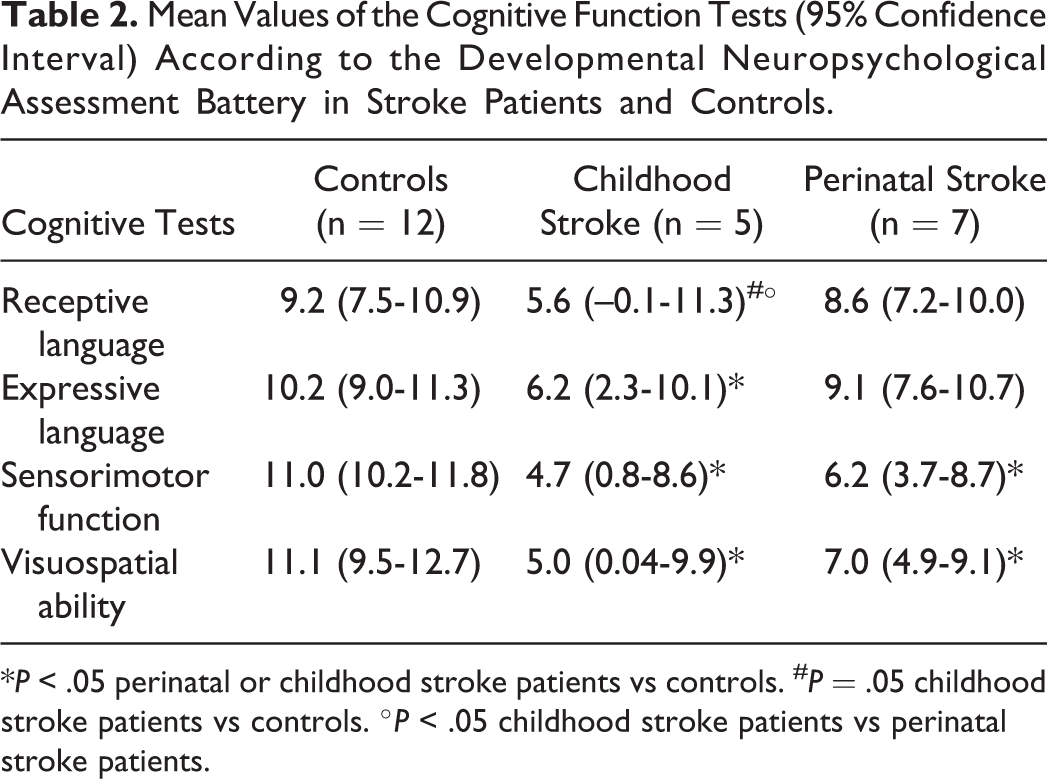
*P < .05 perinatal or childhood stroke patients vs controls. # P = .05 childhood stroke patients vs controls. °P < .05 childhood stroke patients vs perinatal stroke patients.
The Effect of Left-Hemisphere Stroke on Language Lateralization
In children with stroke (the whole group) mean weighted mean laterality index in Brodmann areas 44 + 45 during the verb generation task and in Brodmann area 22 during the sentence comprehension task was significantly different from that of controls (P < .05). In perinatal stroke patients mean weighted mean laterality index in Brodmann areas 44 + 45 in the frontal lobe during the verb generation task and within Brodmann area 22 in the temporal lobe during the sentence comprehension task was significantly lower (P < .05) compared to control children and language function localized in the right hemisphere. However, there were no differences in mean weighted mean laterality index between childhood stroke patients and controls (Table 3). Significant differences (P < .05) in weighted mean laterality index were found between the perinatal and the childhood stroke groups in Brodmann area 22 during the sentence comprehension task; a similar trend (P = .06) was also noted in Brodmann areas 44+45 during the verb generation task.
Mean (95% Confidence Interval) Values of Weighted Mean Laterality Indices in Brodmann Area 22 and Brodmann Area 44+45 During the Verb Generation and the Sentence Comprehension Tasks in Patients and Controls.
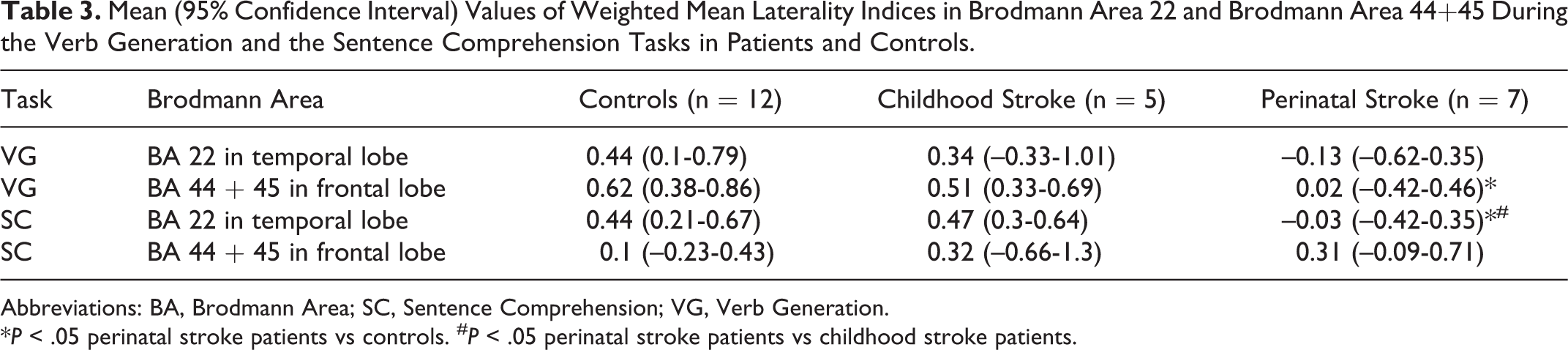
Abbreviations: BA, Brodmann Area; SC, Sentence Comprehension; VG, Verb Generation.
*P < .05 perinatal stroke patients vs controls. # P < .05 perinatal stroke patients vs childhood stroke patients.
All childhood stroke patients showed left-side activation both after the verb generation and sentence comprehension tasks (Tables 4 and 5). Among the children with perinatal stroke 5/7 (71%) showed atypical right-side or bilateral (weighted mean laterality index 0 ± 0.2) activation in Brodmann areas 44 + 45 after the verb generation task and 5/6 (83%) in Brodmann area 22 after the sentence comprehension task. Among the controls 9/11 (82%) showed left-side activation after the verb generation task and 10/12 (83%) showed left-side activation after the sentence comprehension task.
Hemispheric Lateralization With Weighted Mean Laterality Index of Language Activation in Brodmann Areas 44 + 45 During the Verb Generation Task.
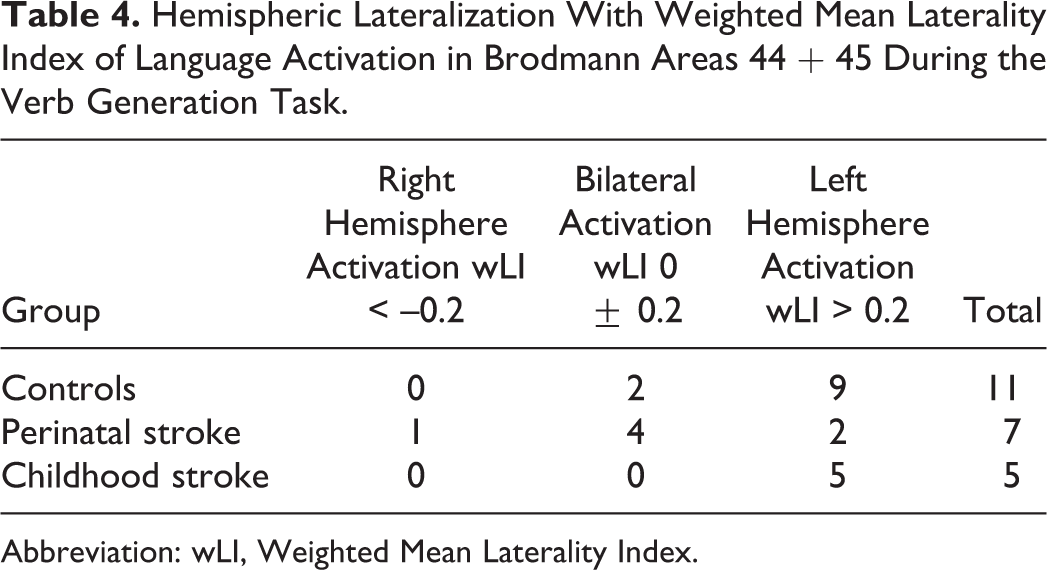
Abbreviation: wLI, Weighted Mean Laterality Index.
Hemispheric Lateralization With Weighted Mean Laterality Index of Activation in Brodmann Area 22 During the Sentence Comprehension Task.
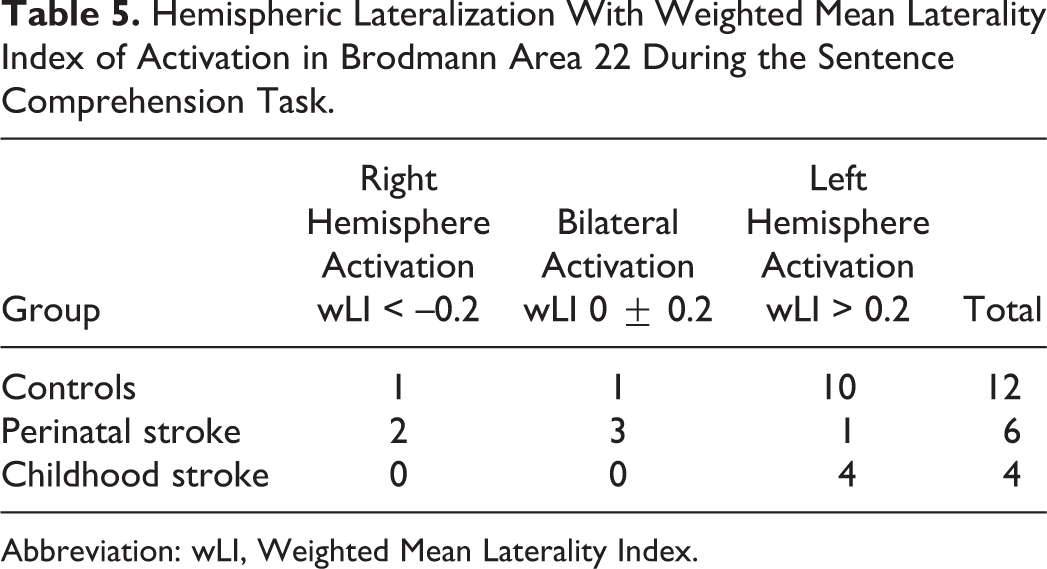
Abbreviation: wLI, Weighted Mean Laterality Index.
Lateralization of Activation and Location of Stroke
All 5 children with childhood stroke (3 with cortical/subcortical lesions and 2 with periventricular damage [PVI]) showed left-side activation both during the verb generation and sentence comprehension tasks. Of the 3 perinatal stroke patients with large cortical/subcortical lesions, 1 child had bilateral and another had right-side activation both during the sentence comprehension and verb generation tasks. One child showed bilateral activation during the verb generation task and right-side activation during the sentence comprehension task. Among the 4 perinatal stroke children with periventricular white matter injury, 2 showed right-side, 1 left-side, and 1 bilateral activation after the verb generation task, and 2 showed bilateral, 1 right-side, and 1 left-side hemisphere lateralization after the sentence comprehension task.
In stroke patients negative correlation was found between mean score for the cognitive expressive language tests by the Developmental Neuropsychological Assessment battery and weighted mean laterality index within Brodmann areas 44 + 45 (Spearman’s correlation coefficient r = –.6, P = .036 and Pearson’s correlation coefficient r = –.55, P = .062) (Figure 1). Correlation between scores for the receptive language test by the Developmental Neuropsychological Assessment battery and weighted mean laterality index in Brodmann area 22 during the SC task was not significant (Spearman’s correlation coefficient r = –.42, P = .22, Pearson’s correlation coefficient r = –.37, P = .29). Children with perinatal stroke showed a trend for correlation between score for the receptive language test and weighted mean laterality index in Brodmann areas 22 after the sentence comprehension task (Spearman’s correlation coefficient r = –.8, P = .059, Pearson’s correlation coefficient r = –.79, P = .06), as well as between score for the expressive language test and Weighted Mean Laterality Index in Brodmann areas 44 + 45 (Spearman’s correlation coefficient r = –.5, P = .25; Pearson’s correlation coefficient r = –.47, P = .29).
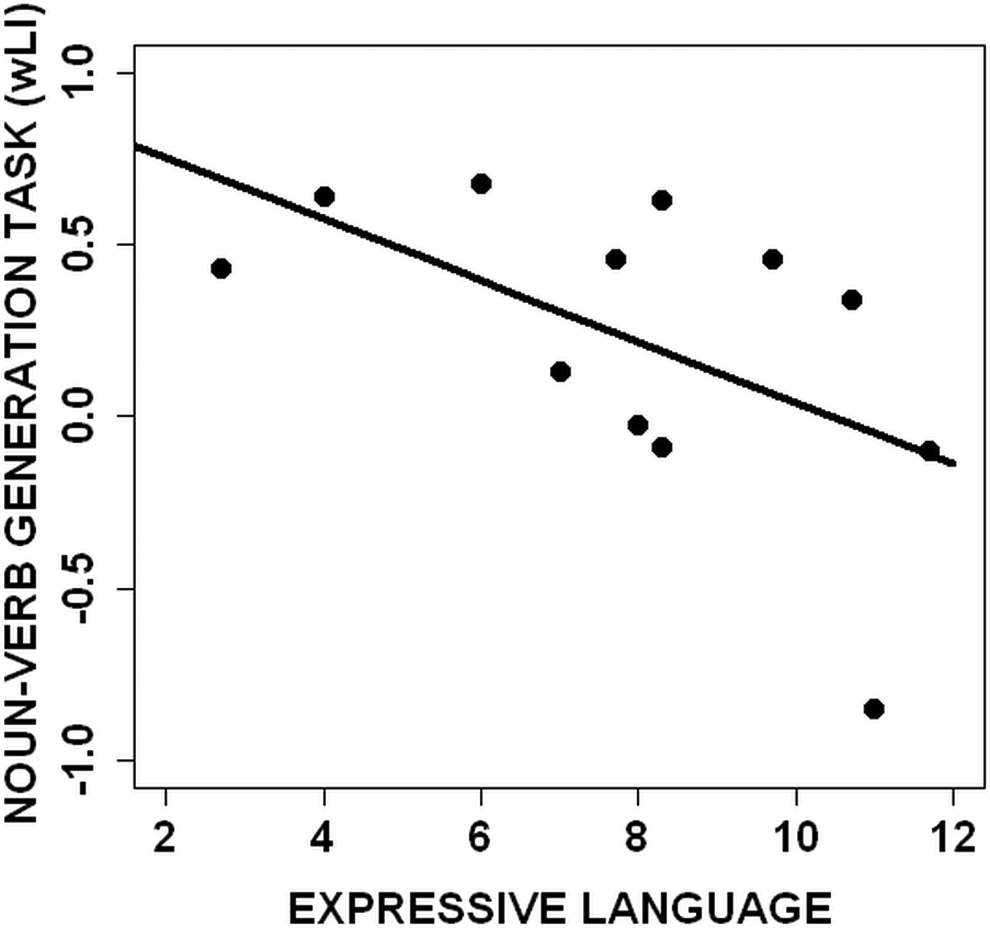
Scatterplot of scores with regression line for cognitive expressive language and Weighted Mean Laterality Index (wLI) within Brodmann area (BA) 44 + 45 during the verb generation task (r = –.55, P = .062).
A correlation was found between visuospatial test scores and weighted mean laterality index in Brodmann areas 44 + 45 during the verb generation task (Spearman’s correlation coefficient r = 0.81, P = .02; Pearson’s correlation coefficient r = –.58, P = .17) but not in Brodmann areas 22 during the sentence comprehension ask in perinatal stroke patients. There was no correlation between weighted mean laterality index during the language tasks and neurocognitive score for language, sensorimotor, or visuospatial function in children with childhood stroke.
Language Lateralization, Neurocognitive Performance and Age at the Onset of Stroke
No correlation was found between weighted mean laterality index and age of the children during the functional MRI investigation for controls. Although there were no differences in weighted mean laterality index during the verb generation or sentence comprehension task between patients of different ages at the onset of stroke, children with the onset of stroke after the age of 2 years (n = 3) had significantly (P < .05) lower mean (95% CI) scores for the receptive language test by the Developmental Neuropsychological Assessment battery, 3.2 (0.7-5.8), compared to children with the onset of stroke before the age of 2 years (n = 9), 8.7 (6.7-10.7). A similar difference was found for the expressive language tests, with significantly lower scores for children with the onset of stroke after the age of 2 years, 4.78 (0-11.2) compared to children with the onset of stroke before the age of 2 years, 8.96 (7.5-10.4).
Discussion
The results of the present study suggest that patients with left hemisphere stroke have a different functional MRI language activation pattern depending on age at the onset of stroke. Differences in cortical activation were associated with the neurocognitive performance of the receptive and expressive language tests. According to functional MRI, children with perinatal stroke had right-side or bilateral cortical organization of language function, but there were no significant differences in the scores for the expressive and receptive language test compared to controls. However, all patients with childhood stroke showed lateralization of language function in the left hemisphere and significantly lower mean language test scores. The different pattern of (re)organization of the language network may significantly affect further development of language in children with childhood and perinatal stroke. In healthy right-handed adults, the left hemisphere is dominant for language function and right hemispheric dominance for language is rare. 10 Our data for 8- to 14-year-old healthy right-handed children revealed left hemisphere lateralization of expressive language function after the verb generation task in 82% and of receptive function after the sentence comprehension task in 83%, which is consistent with previous studies reporting that lateralization deepens throughout childhood long into adolescence. 1,5
The degree of lateralization, measured by weighted mean laterality index, increases with age, suggesting that specialization of the left hemisphere for language processing continues to increase during childhood. 5 It is hypothesized that there is a “dormant circuitry” available for language function that is inhibited in the nondominant hemisphere of healthy children but which may be turned on (or activated) when primary regions in the dominant hemisphere become unavailable to exert inhibition, as in the case of perinatal stroke. 20 Atypical activation after brain lesions are found in areas that were active at an earlier stage of development and may have been inhibited in the process of learning and development. Therefore, reactivation of the bilateral network in the case of damage in the young brain leads to possibilities of compensating for losses in functionality. 13 Age at the onset of stroke has a significant impact on the brain capacity for plasticity to compensate for damage. Significantly higher mean scores for the expressive and receptive language tests were found in patients with perinatal stroke but not in patients with childhood stroke. Neonates may have better abilities, compared to older children, to compensate for brain damage and this plasticity probably persists also in early childhood. Children who sustained stroke before the age of 2 showed significantly better performance in the language tests compared to children with the onset of stroke after the age of 2 years. According to earlier studies by Lenneberg, 29 children who developed brain damage before the age of 2 can achieve normal language development irrespective of the side of the damage (the so-called equipotentiality hypothesis), whereas later onset of damage leads to more persistent verbal impairment.
We found correlation between lateralization of language control and neurocognitive performance after left-side stroke. Better results in the receptive and expressive language tests were shown by children who demonstrated a shift of language activation to the right hemisphere. Patients with high mean language test scores had atypical lateralization of the language network in the homotopic areas of the right hemisphere, indicating brain plasticity. Children between ages 8 to 18 years (mean 12 years) with lesions in the frontal and temporal lobes tended to perform the vocabulary test better and had higher IQ with atypical language lateralization in the right. 12
Plasticity is an intrinsic property of the brain throughout the life span, that enables modification of function and structure of the brain in response to environmental demands. 2 However, the mechanisms of plasticity may vary with age. 2,30 Patients with an arterio-venous malformation affecting the left perisylvian region recruited the right hemisphere into the language processing network during early development, presumably in response to congenitally aberrant circulation. This early right hemisphere recruitment in arterio-venous malformation patients exceeded a similar process in the brain of stroke patients whose left cortical language network was impaired in adulthood. 10 Children with perinatal stroke in our study showed atypical bilateral or right-side lateralization of language activation. Contrary to this, older children with stroke showed no ability to change the cortical activation pattern both for receptive and expressive language and were worse in the performance of the language tests compared to the perinatal stroke group. Although children with early childhood stroke before the age of 2 years did not show a shift of language network function to the right, they had significantly better results in the language tests compared to those with the onset of stroke after the age of 2 years.
Several functional MRI studies have shown that early subcortical damage resulted in dramatic right hemisphere reorganization of language function. 11,15,20 In the perinatal stroke group 20 functional MRI cortical activation patterns for language production were shifted to the right-side inferior and middle frontal gyri. At the same time, these activated cortical areas represented an almost mirror image of left frontal lobe activation for this task seen in the control group. However, some degree of activation was evident in the left frontal lobe as 2 of the 10 patients had left-hemispheric dominance. 20 According to our data, 2 of the 7 patients with perinatal stroke after the verb generation task and 1 of the 6 patients after the sentence comprehension task showed left hemisphere lateralization of language function which was associated with worse performance in all language skills. As in our study, less striking contralateral reorganization followed lesions after a later onset. 10,12 Thus, right-side activation of language function is associated with better performance in language skills. A study of older children after cerebrovascular accidents showed right-side activation and better performance in linguistic tasks with increasing lateralization in the left hemisphere. 13,21
Some authors have reported that the neurocognitive impairment of pediatric stroke patients does not depend on the hemispheric location or size of lesion but rather on the age of the child at the time of damage 17 or gender. 18 In perinatal stroke patients the size of lesion does not appear to affect the interhemispheric distribution of activation. 20 Both cortical/subcortical and periventricular lesions of the left hemisphere result in a significant shift of expressive language toward the right hemisphere. However, in older children with cerebrovascular damage higher right-hemisphere activation did not correlate with size of damage; also correlation between different language performances seems to be independent of the size and location of damage. 21 Our findings confirm this: both periventricular and large cortical/subcortical damage shifted language function to the right in patients with perinatal but not with childhood stroke.
Considering the relatively well-preserved language functions, performance in the visuospatial and sensorimotor tasks by patients after perinatal stroke was lower; this is an important finding of our study. Thus, the ability of the brain to compensate for damage is different, which could be ascribed to selective plasticity in different cognitive functions, as is also shown in studies of early hypoxic-ischemic injury in early childhood. 31 Patients with early left-hemispheric lesions have been reported to show spared language functions (which are mediated by the right hemisphere) but they exhibit deficits in visuospatial functions. 15,32 Earlier, the “crowding hypothesis” has explained these deficits by neuronal scarcity in the right hemisphere for fulfilling the functions inherent of the right hemisphere. Patients with early left-hemisphere lesions and right hemispheric language production were impaired in visuospatial functions in comparison not only to normal controls but also to patients without right hemispheric language preference. 15,16,32 We showed that children with left-hemisphere perinatal or childhood stroke had deficit in visuospatial function irrespective of language dominance. Hence there should exist an explanation other than “overcrowding” to explain low visuospatial function both in perinatal and childhood stroke patients.
Limitations
The present study has some limitations. First, the number of patients in the study is somewhat low, especially in the group of childhood stroke. The small size of the study group can limit the statistical power and generalizability of the study results. The data about the effect of age on language outcome are controversial and need further research in children with childhood stroke. Although the size and localization of damage varied both in the neonatal and childhood stroke groups, there were no statistical differences in the localization of damage. More thorough studies are required to clarify the effect of maturity of the brain on the recovery of cognitive functions and on the laterality of language function in stroke patients.
A second limitation of the study is that girls prevail in the control group. Girls mature more rapidly in verbal abilities compared to boys; 33 however, we found no gender-related differences in language skills to account for differences between the perinatal and the childhood stroke groups.
When studying the issue of reproducibility in individual subjects, Rutten et al found that combined task analysis is more reliable compared to individual task analysis. 34 Two different tasks (verb generation and sentence comprehension) were used to identify the laterality of language in our study. The verb generation as the verb producing task has a superior ability of hemispheric dominance assessment 25,34 and yields results concordant with the Wada test also for atypical dominance. 35
A third limitation of the study is as the Brodmann areas 22 and 44 + 45 were masked, possible additional language activation areas were not identified. However, the aim of the study was to identify the laterality of language function and to compare it with cognitive function, but not to identify all additional areas where language is (re)organized.
Conclusions
(Re)organization of language function after left-hemisphere stroke differs in children with perinatal and childhood stroke and correlates with neurocognitive performance. The plasticity process and recovery in the language domain depend on the time of focal brain damage being more effective in perinatal than in childhood stroke patients.
The selective ability of the brain to compensate for functions in the damaged area is probably manifested in the case of the language preferred in younger ages compared to other cognitive functions like visuospatial function.
Footnotes
Acknowledgments
The work was done at Tartu University Hospital. The authors thank all the patients and parents for contribution. We are indebted to Ms Pille Kool for the help with the study’s statistical analysis. The article was previously submitted to the journal Stroke in December 2012. The material was previously presented (oral presentations) at the 11th International Congress of European Society of Magnetic Resonance in Neuropediatrics in Amsterdam in 2011 and at the 16th Nordic Congress of Cerebrovascular Diseases in Tallinn 2011.
Author Contributions
PI was responsible for the design of the project, performed data analysis, communicated with the ethical committee, prepared the patients for functional magnetic resonance imaging, performed functional magnetic resonance imaging studies, performed the statistical analysis, and wrote the first and final drafts of the article. TT performed functional magnetic resonance imaging studies and wrote the first and final drafts of the article. JK analyzed the functional magnetic resonance imaging studies and corrected the final draft of the article. RL collected the stroke patients, prepared the patients for functional magnetic resonance imaging and neurocognitive studies, and corrected the final draft of the article. MK performed the neurocognitive studies. KK analyzed the functional magnetic resonance imaging studies and corrected the final draft of the article. AK collected the stroke patients, prepared the patients for functional magnetic resonance imaging and neurocognitive studies, and corrected the final draft of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was partly financed by the Estonian Science Foundation (GARLA 6627, 9016, 5462) and by targeted financing TARLA 7695, 0475 and DARLA 3144.
Ethical Approval
Ethical approval was provided by the Ethics Review Committee on Human Research of the University of Tartu, protocol number 170/T-17 from 28.04.2008, consisting of Andres Soosaar, Arvo Tikk, Eve-Merike Sooväli, Riina Kallikorm, Oivi Uibo, Kaja Kasterpõld-Tõrs, Kristi Lõuk, Lembit Allikmets, Vallo Olle, Naatan Haamer, Maire Link, Elin Org, and Aime Keis.