
Abstract
This guideline presents Part V of the Canadian Association of Radiologists (CAR) Practice Guidelines on Breast Imaging and Intervention and addresses image-guided breast intervention and biopsy procedures. This guideline provides comprehensive recommendations for stereotactic-, tomosynthesis-, ultrasound-, and MRI-guided biopsy, as well as preoperative localization and post-procedural management. Key areas include indications and contraindications, biopsy device and needle selection, tissue marker placement, documentation, radiologic–pathologic correlation, quality assurance, and personnel qualifications. Emphasis is placed on minimally invasive, image-guided procedures as the standard of care for diagnosing palpable and nonpalpable breast lesions. This guideline is intended to be used in conjunction with the other components of the CAR Breast Practice Guidelines series, which together replace the 2016 CAR Breast guidelines and reflect the current evidence base and clinical landscape in Canadian breast imaging. While outlining best practices and minimum standards, this guideline acknowledges variability in patient needs, lesion characteristics, and institutional resources, with ultimate responsibility for procedural decision-making residing with the supervising radiologist.
Preamble
The practice guidelines of the Canadian Association of Radiologists (CAR) are not rules, but are guidelines that attempt to define principles of practice that should generally produce radiological care. The radiologist and medical physicist may modify an existing practice guideline as determined by the individual patient and available resources. Adherence to CAR practice guidelines may not ensure a successful outcome in every situation. The practice guidelines should not be deemed inclusive of all proper methods of care or exclusive of other methods of care reasonably directed to obtaining the same results. The practice guidelines are not intended to establish a legal standard of care or conduct, and deviation from a practice guideline does not, in and of itself, indicate or imply that such medical practice is below an acceptable level of care. The ultimate judgment regarding the propriety of any specific procedure or course of conduct must be made by the physician and medical physicist in light of all circumstances presented by the individual situation.
Introduction
The
Together, these documents replace the previous 2016 consolidated guidelines to reflect the current evidence base and clinical landscape in Canadian breast imaging, and complement the recently published Breast Disease Imaging Referral Guidelines, which provide guidance on the most appropriate breast imaging test for a given indication or patient population. 5
These guidelines aim to provide radiologists, technologists, and other allied staff with a consensus-based approach to performing and interpreting breast imaging. These recommendations align with those published by the Canadian and American Cancer Societies, the National Comprehensive Cancer Network, and the American College of Radiology. While the guidelines serve as an educational tool and outline best practices and minimum requirements, the Working Group acknowledges that alternative actions may be appropriate depending on available resources, patient factors, technological advances, and evolving medical knowledge.
Ultimately, the supervising radiologist is responsible for determining the most appropriate examination or intervention for each patient.
Overview: Breast Intervention
Breast interventional procedures may be diagnostic, therapeutic, or both. Diagnostic procedures include but are not limited to pre-surgical localization, fine needle aspiration (FNAB) biopsy, spring-loaded core needle biopsy (CNB), and vacuum-assisted breast biopsy (VAB). Diagnostic/therapeutic procedures include cyst aspiration and abscess drainage. Minimally invasive image-guided biopsy is the most common method for diagnosing both palpable and non-palpable breast lesions. This type of biopsy offers similar accuracy to surgical biopsy, along with several advantages: it is more convenient for patients, less costly, associated with lower morbidity, better cosmetic results, and a lower complication rate. 6
Image guidance should be used for biopsy of both palpable and non-palpable masses provided that the masses are visualized. Palpation guidance is only necessary if the lesion is not seen by any imaging method. The shortest distance from the skin to the lesion should be used when possible. Image guided percutaneous biopsy is superior to open surgical biopsy for several reasons, including increased accuracy, decreased cost and wait times, and decreased surgical morbidity and cosmetic deformity.
The first section of this guideline details general pre-procedure information applicable to interventions regardless of imaging modality, including indications and contraindications, equipment selection, and documentation. Subsequent sections cover technical and procedural details specific to procedures separated by imaging modality or technique. The final section covers post-procedure considerations applicable to all modalities.
It is recommended that all personnel involved in interventional procedures adhere to the requirements listed for the relevant modality in earlier sections of these guidelines (eg, for stereotactic-guided interventions, that radiologists and technologists meet the requirements detailed in the mammography section of the guideline). 1
General Guidance for Interventional Procedures
Indications and Contraindications
The decision to perform an interventional procedure should conform to the general principles noted in the preceding section. For a summary of indications and contraindications by imaging modality, please see Table 1.
Indications and Contraindications for Image-Guided Procedures, by Modality.

Pre-Procedure Preparation
Discuss the benefits, limitations, and risks of the procedure with the patient.
A thorough clinical history must be obtained, focusing on the use of antiplatelet or anticoagulant medications. Clinically significant bleeding is rare in patients following core needle breast biopsy,7,8 For standardized protocols on managing these patients and addressing periprocedural bleeding complications, refer to the CAR/CAIR
Obtain informed consent.
Prepare the breast, procedure field, and physician conducting the procedure according to infection control principles.
Obtain scout imaging (stereotactic- and tomosynthesis-guided).
Position the unaffected breast out of field for unilateral biopsies (MRI-guided).
For bilateral biopsies, compress both breasts using open coils with bilateral lateral access (MRI-guided)
Place a fiducial marker within grid for localization (MRI-guided).
Equipment
Modality-Specific Equipment
For recommendations associated with mammographic, ultrasound, and MRI equipment, please refer to other sections of these guidelines, relevant to the modality in question.1-4
Biopsy Devices and Sampling
Spring-loaded needle systems typically provide adequate samples for diagnosis.
14-gauge and larger needles are recommended for spring-loaded devices.
Vacuum-assisted core-needle biopsy systems are also suitable for ultrasound-guided procedures.
Other biopsy systems may be used under ultrasound guidance.
Accurate targeting and sampling are crucial for diagnostic success.
Biopsy-Needle Selection
Several needle biopsy devices are available for stereotactic-guided procedures, including automated core needles, vacuum-assisted devices, and other tissue biopsy systems. The choice of biopsy device depends on the type of lesion as well as the operator’s experience. MRI-guided biopsy is almost exclusively vacuum-assisted, whereas all types of needles are used for ultrasound guided procedures. Stereotactic or tomosynthesis-guided biopsies can be performed with spring-loaded and vacuum-assisted needles; VAB is preferred as it can yield larger, more accurate samples while minimizing patient discomfort and procedure time.
Vacuum-assisted devices of 11-gauge and larger have been shown to be most effective in the biopsy of microcalcifications, under stereotactic, tomosynthesis, or ultrasound guidance. 10 VAB is also indicated for architectural distortion without a mass. If a finding is visible and accessible on ultrasound, ultrasound-guided biopsy is preferable for patient comfort and to limit radiation dose. Due to the location of the biopsy target or body habitus of the patient, some patients may require a smaller-gauge vacuum-assisted device.
Fourteen-gauge needles are often recommended for ultrasound-guided core biopsy due to the quality of the sample. However, selection of a different needle size or semi-automatic needle may be dependent on lesion location and size. Co-axial technique may be helpful for sampling difficult to access lesions or lesions in dense tissue.
In the case of lesions located very close to vital structures, including axillary structures, initial biopsy may be performed with a small gauge or non-advancing core needle. A fine needle may also be a last resort in order to avoid trauma to surrounding structures. FNAB is accepted for axillary node biopsy; however, core biopsy is preferred when safe to do so, as core biopsy is more likely to yield a diagnostic sample.
Biopsy Markers
Biopsy markers are used to ensure accurate identification of lesions during follow-up or subsequent localization. 11 Breast biopsy markers help to confirm the agreement between radiologic and pathologic findings, especially when the pathology result is benign. They also serve to establish this concordance for suspicious lesions seen on one imaging technique but biopsied using another. Marker placement can help identify the correct lesion location when visibility is challenging, such as with small lesions or in patients receiving neoadjuvant chemotherapy where the target lesion may disappear during treatment.
Markers can migrate, and in those cases, either the remaining lesion or other landmarks can be used for localization if necessary. The type of marker selected should be based on its required visibility on a particular imaging modality (eg, ultrasound or MRI) or a nickel-free option if the patient has an allergy.
Indications
Placement of a radiologically- or ultrasound-visible clip/marker or carbon-marking at the time of biopsy is essential recommended in the following situations:
Lesions difficult to identify at follow-up or subsequent localization.
Complete or near-complete removal at sampling.
Modifications to the lesion post-biopsy (eg, small, solid intracystic lesions).
Lesions with ambiguous distribution or morphology (eg, multiple lesions).
Lesions that will potentially be treated with neoadjuvant chemotherapy.
Lesions biopsied under MRI guidance.
Lesions that may be confused with adjacent lesions.
Ultrasound-, stereotactic-, and tomosynthesis-guided biopsies for MRI-detected lesions require a marker, to ensure correlation.
Clinical Practice Recommendations
Avoid leaving suspicious microcalcifications intentionally as markers, as this may lead to under-sampling.
Use different-shaped clips for multiple placements in the same breast.
Post-biopsy mammograms are recommended when a marker is left in place (CC and lateral views).
Include comments on the marker’s positioning relative to the lesion in the report.
Limited post-biopsy unenhanced MRI views can be used in addition to mammography after ultrasound guided biopsy of MRI-detected lesion if there is doubt the lesions correlation.
Be aware of potential marker migration or misplacement following biopsy.
A patient declining a clip or tissue marker is not an absolute contraindication for continuing with the biopsy.
Documentation
A permanent record of interventional procedures should be documented in a retrievable image storage format. Specific details of documentation vary with the type of procedure performed. Retention of procedure imaging should be compliant with federal and provincial policies, with local health care facility procedures, and with clinical need.
Reporting should be in accordance with the CAR Standard for the Communication of Diagnostic Imaging Findings. 12 Permanent records of image-guided breast interventions should be documented in retrievable image storage format. For image labeling requirements and recommended report inclusions, please see Table 2.
Documentation of Image-Guided Interventions.

Stereotactic and Tomosynthesis-Guided Biopsies
Stereotactic-guided breast biopsies are appropriate for most lesions visible on mammograms, including microcalcifications, masses, asymmetries, and architectural distortions. When available, stereotactic guidance is preferred over grid-type mammographic guidance because it is more accurate for the calculation of the Z position of a lesion, is faster, and requires less radiation.
Digital breast tomosynthesis (DBT) guidance can be utilized for findings suitable for the stereotactic technique, as described above. If lesions are visible only or more clearly on DBT compared to 2D mammography, a DBT-guided percutaneous biopsy is preferred, if available.
Specifications of the Procedure
Lesion Targeting and Documentation
The physician performing/supervising the procedure targets the lesion.
Document needle positioning with paired pre-fire stereotactic images or DBT image.
Obtain post-fire imaging at the proceduralist’s discretion.
For non-fire mode, capture paired stereotactic or DBT images with the needle in final pre-biopsy position.
Biopsy and Verification
VAB is preferred over spring-loaded devices.
A needle gauge of 12 or larger is recommended except in specific scenarios that may necessitate a smaller gauge.
For microcalcifications, obtain magnified specimen radiograph to verify adequate sampling.
Place tissue marker post-biopsy, especially for potentially obscured lesions or multiple biopsies, with imaging to document placement.
Use markers with different characteristics for multiple lesions.
Ultrasound-Guided Procedures
Ultrasound guidance can be used when a lesion (usually a mass or lymph node) is visualized on ultrasound. Prior to the performance of any ultrasound-guided percutaneous procedure, the finding should be reassessed. The primary advantage of ultrasound-guided procedures is real-time confirmation of target sampling. Other advantages include accessibility, cost-effectiveness, and lack of patient exposure to radiation or contrast.
Specifications of the Procedure
Needle Positioning and Approach
Perform the procedure under real-time imaging guidance, using a high-frequency linear transducer.
The long axis of the needle should be visible along the long axis of the transducer.
Keep the needle relatively parallel to the chest wall and transducer face.
Choose an insertion point balancing a parallel approach and minimal tissue traversal.
Maintain greater parallelism for devices with a throw. Taking a parallel approach improves the visibility of the needle during the procedure.
Image Documentation
Prior to sampling, obtain images of the target lesion or area of interest. These images should not include the needle.
When markers or non-wire localization devices are placed, obtain imaging that documents the marker or device
For core needle biopsies (CNB), fine needle aspirations (FNA), and wire localizations: Capture an image showing the needle traversing the lesion May capture 2 orthogonal images of the needle through the lesion instead of a single image
For vacuum-assisted biopsies and cyst aspirations: Take lengthwise images of the needle and lesion before sampling/aspiration Image the area after sampling/aspiration to document any residual lesion.
MRI-Guided Biopsies
Image-guided CNB under MRI guidance has decreased both the number of benign surgical biopsies and the number of surgical procedures needed to treat breast cancer.13,14
Facilities performing breast MRI should have the ability to perform correlation with mammography, MRI-directed breast ultrasound, and MRI-guided interventions. If MRI-guided biopsy is not offered at the facility performing the breast MRI, a referral arrangement should be established with a cooperating facility to provide these services without the need to repeat the MRI examination.
Specifications of the Procedure
Initial Imaging and Targeting
Perform a 3-plane localizer sequence.
Obtain pre-contrast T1-weighted images to confirm adequate positioning.
Administer contrast and perform post-contrast T1-weighted imaging.
Create subtraction images if needed for subtle findings.
Use manual targeting (paper method) or computer-aided evaluation (CAE) systems.
Calculate and note skin entry coordinates and target depth.
Lesion Targeting and Documentation
Move the patient table out of MR scanner bore.
Place biopsy guidance sheath with obturator to calculated depth.
Confirm accurate placement with sagittal and axial imaging.
Adjust targeting if necessary.
Biopsy and Verification
Vacuum-assisted biopsy (VAB) is preferred for MRI-detected lesions. A needle gauge of 12 or larger is recommended.
Avoid 14-gauge spring-loaded core biopsy due to insufficient sampling.
Obtain sufficient samples depending on lesion size, device gauge, and clinical scenario, to get accurate diagnosis.
Place tissue marker post-biopsy, obtain a mammogram to document marker position.
Additional Considerations
Approximately 10% of lesions may not persist; recommend 6-month follow-up if not seen on MRI.
MRI-detected lesions are often small with high incidence of atypia.
MRI-guided biopsies have a higher underestimation rate compared to stereotactic biopsies.
Precision in targeting is crucial, especially considering the lesion position relative to grid.
Technical Guidelines
Imaging Protocol
Examinations should be performed with a dedicated open interventional MRI coil equipped with a localization device.
Spatial resolution should be high enough to identify the target(s) of interest.
Images need to be obtained quickly to ensure visualization of the finding prior to contrast washout.
The resolution may not match that of a diagnostic protocol, due to the goal being target identification rather than detection and characterization.
Faster sequence acquisition should be used to minimize overall procedure time, reducing patient discomfort and motion.
Perform simultaneous bilateral imaging when findings in each breast are being biopsied concurrently.
Image Enhancement Techniques
Slice thickness and in-plane spatial resolution should be similar to adequately visualizing the finding
Consider using fat suppression and subtraction imaging to identify the target finding. Note that subtraction may cause misregistration due to patient motion.
Motion-correction software can help reduce subtraction artifacts.
Contrast Administration
Gadolinium contrast is generally necessary to identify the target lesion.
Use standard dose of 0.1 mmol/kg as a bolus.
Follow with at least 10 mL saline flush.
Scan Timing
For optimal lesion visibility, capture images before contrast washout.
For single postcontrast scans, complete within 4 minutes of bolus injection.
Investigation of Nipple Discharge Using Galactography
Galactography or ductography may be used as an alternative to MRI for the investigation of pathologic nipple discharge, when MRI is not available or contraindicated. Ductography is minimally invasive, may be uncomfortable, and can be time-consuming. The procedure is technically challenging. The rate of incomplete or failed ductograms may be as high as 15% to 23%. 15
Ductography is performed with a 30-gauge blunt-tipped straight or angled cannula gently inserted into the orifice of the discharging duct. 1 to 3 mL of nonionic iodinated contrast medium is slowly administered through the cannula, and 2 orthogonal views are obtained, with additional views obtained as necessary.
The discharge must be present on the day of ductography so that a cannula can be placed in the correct duct. Failure to cannulate the discharging duct may lead to a false negative result.
Ductography is not recommended in lactating women or patients with active mastitis. Known hypersensitivity to iodinated contrast agents is a relative contraindication. A negative ductogram does not reliably exclude an underlying cancer or high-risk lesion, with the false-negative rate reported to be as high as 20% to 30%. 16
Post-Procedure Follow-Up
Post-Procedure Care
Compress the biopsy site, skin entry site, and needle path until hemostasis is achieved. Compression time varies based on patient factors and extent of bleeding. Note: Absence of external bleeding doesn’t guarantee internal hemostasis.
Post-biopsy mammogram, to assess residual calcifications and to check clip placement (if used).
Additional views may be necessary to visualize the tissue marker.
Include DBT images for DBT-only visible findings.
Report should state marker position relative to the biopsy site.
Monitor and document any delayed complications; record any treatments administered.
Submission of Pathology Specimen(s)
Submitting a specimen for histopathology is a request for a consultant opinion. For this opinion to be effective, accurate identification and good preservation of the specimen are essential. Providing good clinical details is vital as the histopathological findings are interpreted in the clinical context.
The requisition should be properly filled out with the following information:
Patient complete name, age, date of birth, and collection date
Clinical history
Side and source of tissue
Number of needle core biopsies submitted
Specimen containers should be labeled completely with patient information, collection site, date, and physician’s name. When multiple specimens are to be examined and diagnosed individually, each specimen must be submitted in a separate container completely labeled as indicated above.
Specimens should be placed in buffered formalin within approximately 10 minutes of their removal from the patient. Increased cold ischemic time will interfere with the assessment and staining of the tissues. The volume of formalin is ideally 20 times that of the specimen, but for very large specimens this may be reduced to ten times the volume of the specimen. Very small specimens should be placed in formalin almost immediately (within 1 or 2 minutes depending on the size); otherwise marked drying artifacts will occur. Larger specimens with a high fat content, which float, may be covered within a few layers of paper towels to allow formalin to reach the upper surface of the specimen. The container obviously must be able to accommodate the specimen plus many times its volume in formalin. The specimens should fit through the opening of the container with ease.
Radiologic-Pathologic Correlation
Ideally, the physician who performed the procedure should determine the concordance between pathology results and imaging findings.17,18 If that physician is not available a designated physician may determine concordance to facilitate timely management of the patient. Radiologic-pathologic correlation is crucial due to potentially higher upgrade rates and false-negatives.19-21 Technical constraints inherent to MRI can make determination of radiologic-pathologic concordance challenging because there is not confirmatory method to verify adequate sampling.
Following receipt of the pathology report, an addendum to the biopsy report should be produced by the radiologist in charge of the biopsy or by his/her assigned proxy when required to expedite results. This addendum should include the radiologist’s opinion on radiologic-pathologic concordance or discordance as well as a suggestion for the appropriate management follow-up, such as the need for further imaging, imaging follow-up, repeat biopsy or surgical consultation.
Discussion with the pathologist is strongly encouraged when determining appropriate management for patients with questionable radiology-pathology concordance.
Regular Radiology-Pathology Breast Biopsy Correlation rounds are recommended as a method to facilitate case review and determination of concordance between imaging findings and biopsy results.
Management Recommendations
In cases of insufficient sampling, repeat biopsy should be recommended, preferably using a method that achieves a larger sample size than that of the original biopsy.
Additional Considerations for MRI
There is a higher upgrade rate for MRI-detected high-risk lesions compared to mammography or ultrasound.23-27
For concordant benign findings, further intervention or excision is not usually required. Consider short-term follow-up with diagnostic breast MRI at 6 months due to challenges in determining concordance.
Preoperative Localization
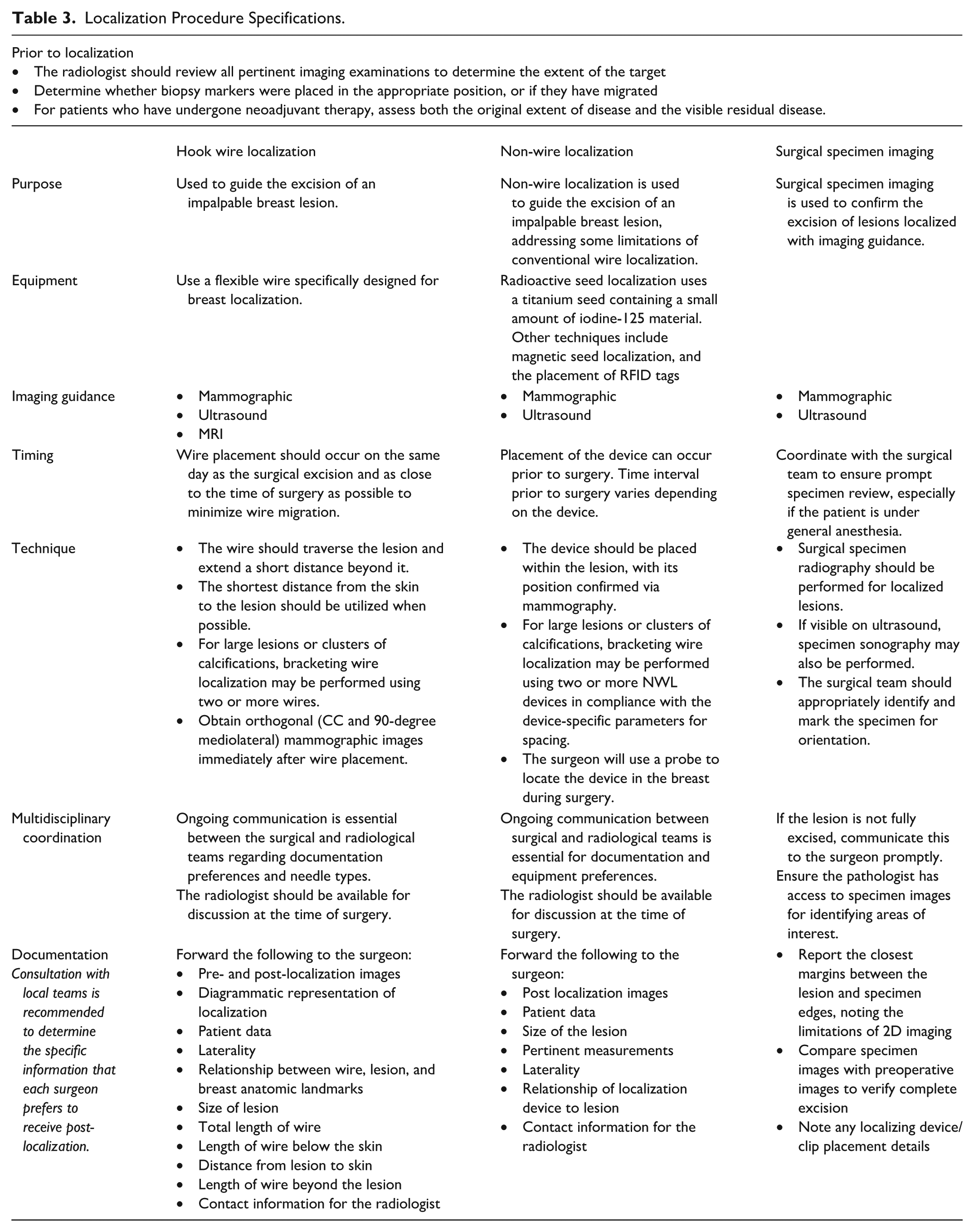
Preoperative image-guided localization has become an essential component in the management of nonpalpable breast abnormalities prior to surgical excision. This approach has evolved into the standard of care, providing surgeons with guidance to ensure successful removal of target tissue. The technique of preoperative localization through image-guided wire placement, which was pioneered in the 1970s, continues to be a reliable and safe method for breast lesion localization.
In recent years, there have been significant advancements in non-wire localization (NWL) techniques. These innovations aim to address some of the limitations associated with traditional wire localization methods, potentially enhancing patient care and streamlining clinical workflows. NWL devices lack a component external to the breast after placement (as is present with the proximal wire segment when a wire is placed). The absence of an external component in NWL offers increased patient comfort and decreased risk of displacement or transection of the localizing device compared with wires. 28 All forms of NWL typically have 2 components: a single-use sterilized device preloaded into a needle introducer and a console with a handheld probe for the detection of deployment by the radiologist and for surgical guidance by the surgeon. The localizing device may be placed at the breast lesion, adjacent to the biopsy marker (if it lies at the site of the lesion), or at the post-biopsy hematoma if the lesion itself cannot be visualized and if a biopsy marker is not present. In addition to some type-specific limitations (outlined below), NWL may be subject to imprecise positioning during placement or deployment. An important limitation of NWL is that once deployed, they currently cannot be repositioned.
Indications
Presurgical localization in the breast is useful for patients with indications including, but not limited to:
Biopsy-proven cancer
Biopsy-proven metastatic lymphadenopathy
High-risk lesions diagnosed at percutaneous biopsy
Imaging-pathological discordance at core-needle biopsy
Cases in which core-needle biopsy fails to provide a definitive histological diagnosis or is not an option
Specifications of the Procedure
The radiologist should meet the recommended qualifications and personnel requirements for each modality listed in other sections of this guideline.
See Table 3 for more information.
Localization Procedure Specifications.
2025 Guideline Development Committee
Co-Chairs
Samantha Fienberg, MD, FRCPC
Carolyn Flegg, MD, FRCPC
Committee Members
Priscila Sacilotto Crivellaro, MD, FRCPC
Rachel Fleming, MD, FRCPC
Wade Koberstein, MD, FRCPC
Anat Kornecki, MD, FRCPC
Anisa Mnyusiwalla, MD, FRCPC
Saly Zahra, MD, FRCPC
Previous Guideline Development Committees
2016 Committee
Shiela Appavoo, MD, FRCPC (Chair)
Ann Aldis, MD, FRCPC
Petrina Causer, MD, FRCPC
Pavel Crystal, MD, FRCPC
Anat Kornecki, MD, FRCPC
Yolanda Mundt, MD, FRCPC
Jean Seely, MD, FRCPC
Nancy Wadden, MD, FRCPC
2012 Committee
Shiela Appavoo, MD, FRCPC (Chair)
Ann Aldis, MD, FRCPC
Petrina Causer, MD, FRCPC
Pavel Crystal, MD, FRCPC
Benoît Mesurolle, MD, FRCPC
Yolanda Mundt, MD, FRCPC
Neety Panu, MD, FRCPC
Jean Seely, MD, FRCPC
Nancy Wadden, MD, FRCPC
Footnotes
Acknowledgements
The Working Group would like to thank the CAR members and radiologists across the country who contributed their feedback and suggestions during the revision process of this guideline.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.