
Abstract
Background/Objectives:
Acute head trauma (AHT) is a common reason for pediatric emergency department (ED) visits, although most cases do not result in clinically important traumatic brain injury (ciTBI). Clinical decision rules such as PECARN can help identify children at risk for ciTBI and guide the need for cranial computed tomography (CT). Despite this, CT appears frequently overused, raising ongoing concerns about radiation exposure, resource utilization, and clinical yield. This study evaluated after-hours CT utilization patterns and diagnostic yield for pediatric head trauma at a tertiary care centre.
Methods:
We conducted a retrospective review of after-hours non-contrast cranial CT examinations for pediatric (<16 years) head trauma performed between January 2020 and February 2024. Data extracted included presence of skull fracture and/or intracranial injury (ICI; bleed, contusion, or combination), radiation dose, and follow-up imaging. Patients were grouped by age (<2 and ≥2 years).
Results:
Among 361 children (median age 6 years; 150 females), 267 examinations (74%) were normal, with no evidence of skull fracture (79.8%) or acute ICI (83.9%). Only 29 cases (8%) underwent follow-up imaging. Children <2 years (n = 97) demonstrated higher rates of positive findings: 34% (33/97) had skull fractures and 24.7% (24/97) had ICI.
Conclusion:
In this cohort of after-hours ED-initiated cranial CT examinations, most studies did not demonstrate acute traumatic findings, particularly in children ≥2 years. Imaging of younger children had a comparatively higher diagnostic yield. These findings describe institutional CT utilization patterns and may inform future quality improvement initiatives and local imaging pathways.
Introduction
Acute head trauma (AHT) is a common reason for pediatric emergency department (ED) visits, accounting for over 800 000 presentations annually across North America. 1 AHT can result in skull fractures and traumatic brain injuries (TBIs), which are a leading cause of morbidity and mortality in children. 2 Most TBIs are classified as mild (90%), defined by a Glasgow Coma Scale (GCS) score of 13 to 15 within 30 minutes post-injury; fewer than 10% demonstrate intracranial injury (ICI) on imaging, and 0.5% require neurosurgical intervention.3,4
Young children are particularly vulnerable to TBI due to anatomical and physiological factors, including a larger head-to-body ratio, thinner skull, soft and compliant sutures, weaker neck muscles, and less myelinated brain tissue.5-7 Timely recognition of clinically important TBI (ciTBI; defined within the Pediatric Emergency Care Applied Research Network [PECARN] framework as injury resulting in death, neurosurgical intervention, intubation >24 hours, or hospital admission ≥2 nights due to TBI) is critical in this population to prevent long-term neurodevelopmental sequelae.8-10
Non-contrast cranial computed tomography (CT) is the first-line imaging modality for evaluating AHT and identifying ICIs such as subdural hematoma, epidural hematoma, and cerebral contusion. 11 Although CT is always indicated in moderate to severe TBI (GCS <13), its use in mild TBI should be guided by validated clinical decision rules such as the PECARN algorithm. 10 Importantly, PECARN identifies risk of ciTBI rather than isolated radiographic abnormalities. 10 Given the risks of radiation-induced malignancy, potential need for sedation, and unnecessary resource utilization, CT imaging must be used judiciously in this population.12-14 Despite readily available decision algorithms, CT imaging rates for mild TBI vary widely worldwide (15%-70%), with an estimated overuse rate of 27%.15-18
At our institution, imaging decisions for pediatric head trauma are guided by PECARN and Canadian Assessment of Tomography for Childhood Head Injury (CATCH2) criteria in conjunction with clinical judgement.10,19 Comparative studies indicate that PECARN demonstrates higher sensitivity and slightly better specificity than CATCH2, particularly in children <2 years.10,20 According to PECARN, CT is always indicated for children with a GCS of ≤14 at 2 hours post-injury, reflecting a 4.3% to 4.4% risk of ciTBI. 10 The challenge arises in children classified as intermediate risk by PECARN (GCS of 15 with additional risk factors), who have a low likelihood of ciTBI, estimated at approximately 0.9%. 21 In these cases, management may involve either observation or CT imaging, depending on various clinical factors such as symptom progression, clinician judgement, parental preference, and the challenges of observational assessment in infants. 10
Despite these rules, no formal clinical pathway exists at our centre to advise on the use of CT for low-to-intermediate risk of ciTBI. There was a perceived accumulation of CT imaging performed after hours at our centre, prompting interest in better characterizing institutional imaging patterns and diagnostic yield. Understanding local utilization patterns may help guide future quality improvement efforts and standardization initiatives.
This study aims to characterize after-hours non-contrast cranial CT utilization for pediatric head trauma at our institution and describe the radiographic diagnostic yield (fracture and ICI detection) of these studies. This study was not designed to determine ciTBI rates or assess PECARN adherence. By examining imaging findings and age-stratified results, this work seeks to provide baseline data that may inform future institutional discussions regarding imaging pathways and resource utilization.
Material and Methods
This single-centre, retrospective cohort study was conducted following approval by the institutional research ethics board, with a waiver of informed consent.
Study Population and Data Collection
A retrospective review of all after-hours non-contrast head CT examinations and associated imaging requisitions performed at a tertiary pediatric referral and trauma centre between January 2020 and February 2024 was undertaken using Enterprise Imaging (version 8.3.2.050) Picture Archive and Communication System (PACS). Only patients who underwent CT for acute traumatic head injury were included. Studies performed for non-traumatic indications including isolated symptoms such as dizziness, nausea, headaches, or irritability without a preceding traumatic event were excluded.
After-Hours Coverage
The after-hours period was defined as imaging performed on weekends or between 17:00 and 8:00 on weekdays, consistent with prior literature. 22
CT Protocol
All non-contrast head CT examinations were performed using a Canon Aquilion Prime scanner (2017) at 100 kV with age-based tube current selections. Standard 2D multiplanar (sagittal, coronal, and axial) 3 mm brain and bone reconstructions, and 3D volumetric bony reconstructions were completed by CT technologists at the time of examinations and available for review within PACS. Full imaging protocols are detailed in Supplemental Appendix A.
Image Review and Data Collection
All CT examinations were interpreted and reported near the time of examination by one of 9 staff pediatric radiologists at IWK Health, including 3 radiologists with additional fellowship training in neuroradiology. Radiologists had varying levels of experience in pediatric imaging.
Radiology reports were retrieved from PACS. Medical records were reviewed for cases with positive findings. Data extracted included:
Patient demographics (age at examination, sex)
Mechanism of injury
Presence/absence of skull fracture
Presence/absence of ICI (defined as bleed and/or contusion)
Dose length product (DLP; mGy cm)
Presence/absence of follow-up imaging (≤7 days after initial study) and imaging type (CT or MRI) for further characterization of injuries or unexpected progression of symptoms
Earliest documented GCS score (either from trauma survey or initial ED assessment; grouped as >14 or ≤14, as per PECARN criteria) 10
Statistical Analysis
Statistical analyses were performed using Microsoft Excel (2024). Continuous variables are reported as median and interquartile range (IQR). Categorical data are reported as n/N (%).
Z-tests were conducted to compare the proportion of fractures and ICIs between children <2 years versus ≥2 years. All tests were done using the pooled proportion method to calculate the standard error. The significance level (α) was set at .05. 95% confidence intervals (CIs) were calculated using Wilson score method for binomial proportions. Multivariable analysis was not performed due to limited clinical variables.
Results
Descriptive Statistics and CT Findings Summary
A total of 361 after-hours non-contrast CT head examinations met inclusion criteria. The median age was 6.0 years (IQR, 2.0-13.0), with 211 males (58.5%) and 150 females (41.6%; Table 1). Ninety-seven children (26.9%) were <2 years, and 264 (73.1%) were ≥2 years.
Descriptive Statistics and CT Scan Findings for All Patients.
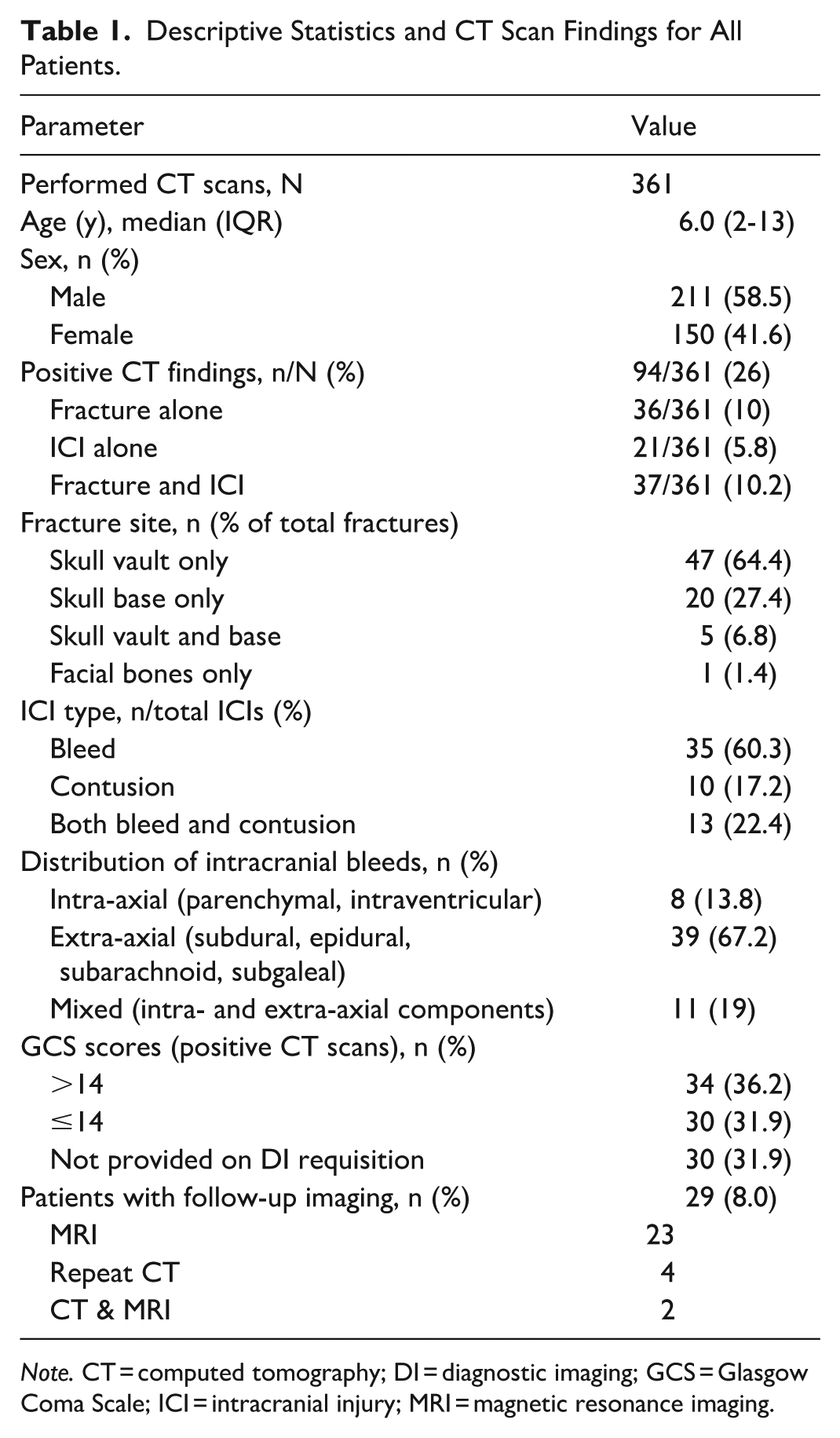
Note. CT = computed tomography; DI = diagnostic imaging; GCS = Glasgow Coma Scale; ICI = intracranial injury; MRI = magnetic resonance imaging.
Average DLP (mGy cm) increased with age according to protocol: 0-2 years = 542.07, 3-5 years = 652.59, 6-12 years = 775.20, 13-16 years = 1032.82 (Supplemental Appendix A). A summary of CT findings is presented in Table 1 and Figures 1 and 2.
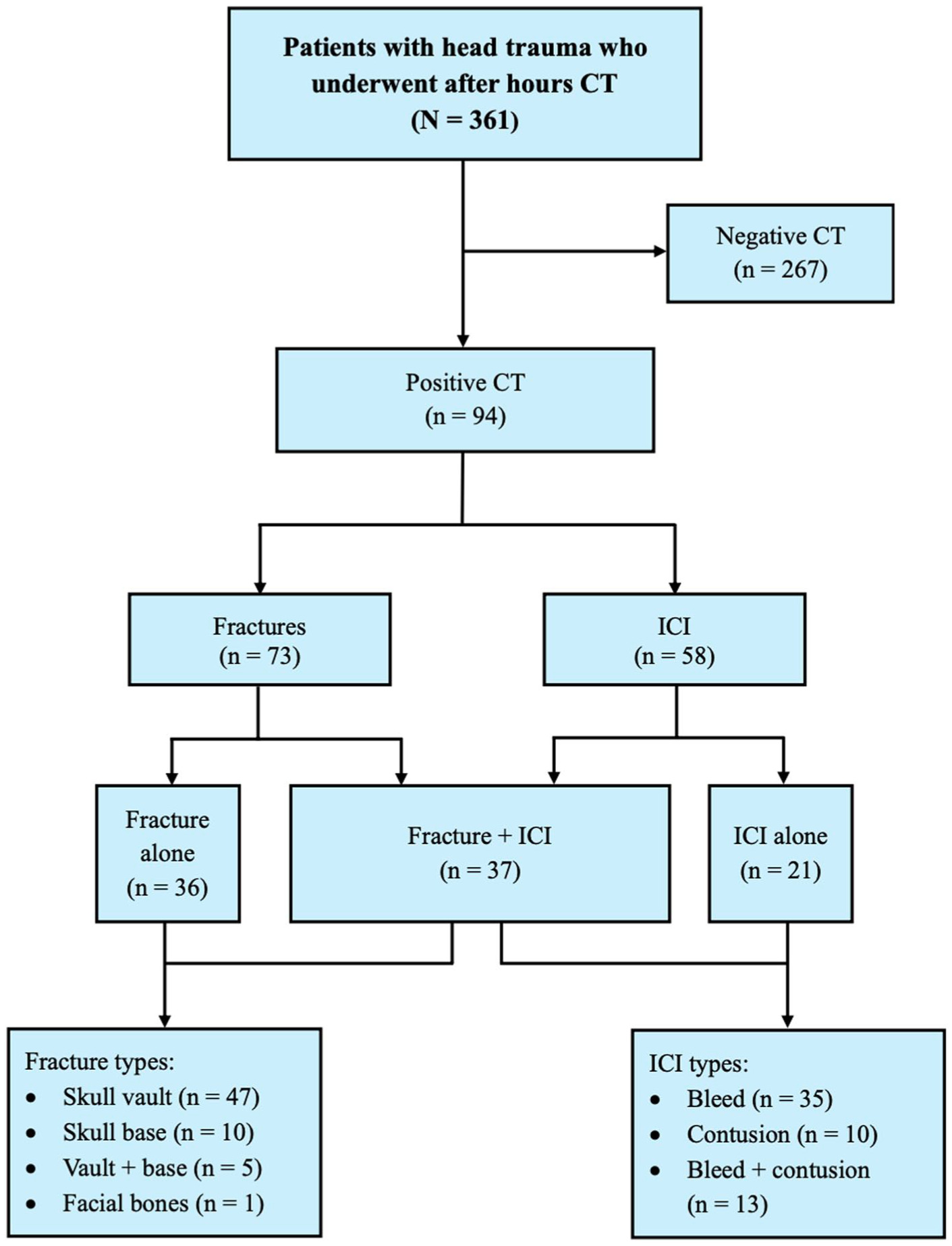
Study flow diagram.
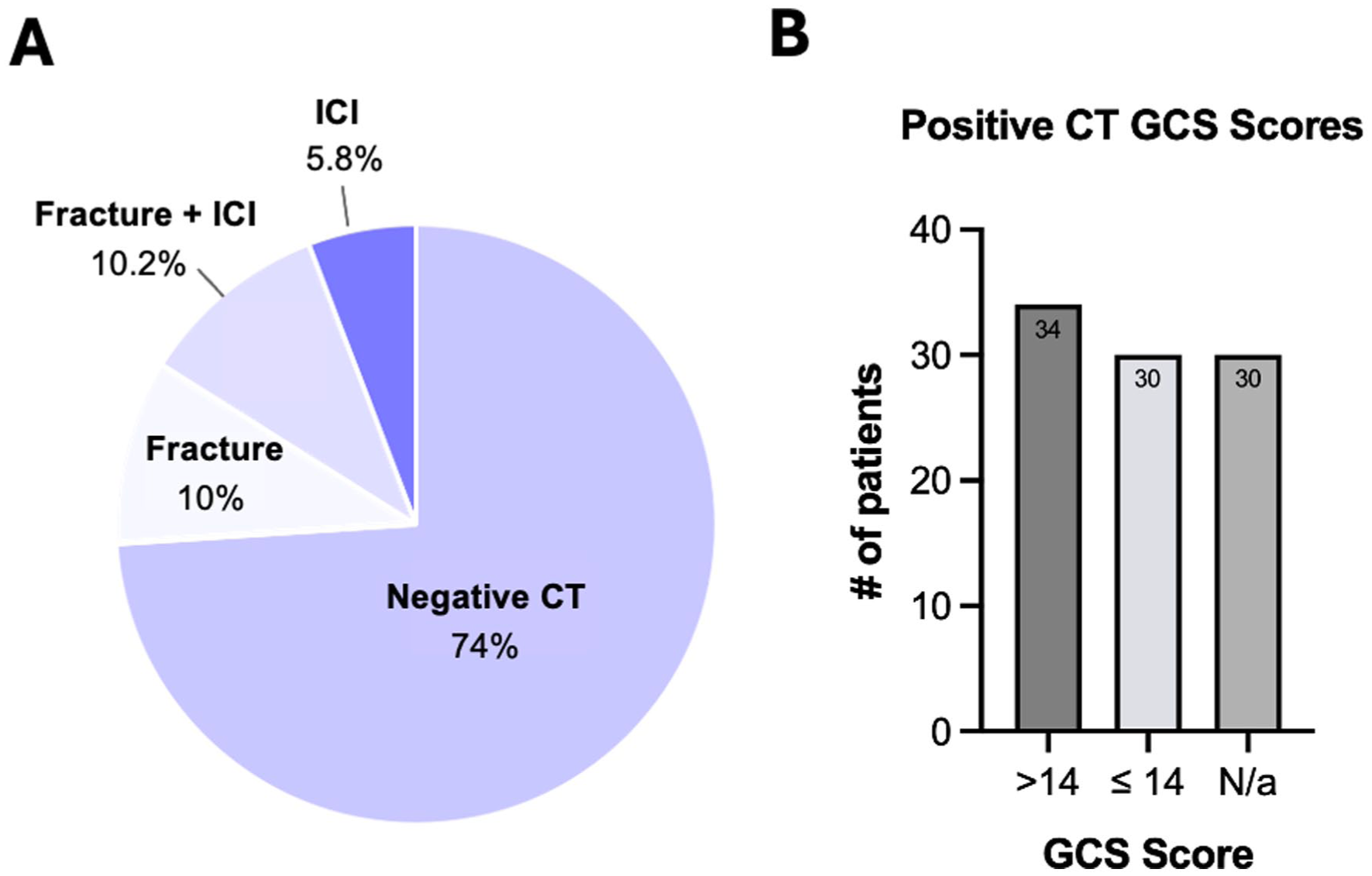
CT findings and Glasgow Coma Scale distribution among patients with positive neuroimaging. (A) Distribution of CT scan results for the entire cohort (N = 361). Most children (n = 267) had a normal CT. Among abnormal scans (n = 94), the most common findings were combined fracture and intracranial injury, followed by isolated fracture, and isolated intracranial injury. (B) GCS scores among patients with positive CT findings (fracture and/or intracranial injury). Patients were categorized as having GCS >14 (minor head trauma), GCS ≤14 (moderate-severe head injury), or unavailable scores. These categories correspond to PECARN risk stratification pathways and illustrate where patients with radiographic findings would fall within the clinical decision algorithm.
Overall, 267 CT scans (74%) demonstrated no acute findings. Most children were negative for fracture (n = 288, 79.8%) and acute ICI (n = 303, 83.9%). Among abnormal studies (n = 94), there were 73 (36 isolated) fractures, 58 (21 isolated) ICIs, and 37 combined fractures and ICIs (Figure 2A). Of all ICIs, there were 35 bleeds (60.3%), 10 contusions (17.2%), and 13 combined bleeds and contusions (22.4%; Table 1). Of all intracranial bleeds, 39 (67.2%) were extra-axial (subdural, epidural, subarachnoid, or subgaleal). Most fractures involved the skull vault alone (n = 47; 64.4%). Follow-up imaging was uncommon (n = 29; 8%).
Among children with positive CT findings, earliest documented GCS scores were reviewed as GCS is a key variable within PECARN ciTBI risk stratification. Thirty-four (36.2%) had a GCS >14, 30 (31.9%) had a GCS ≤14, consistent with moderate or severe TBI, and 30 (31.9%) lacked clearly documented GCS associated with the ED visit (Table 1, Figure 2B).
Descriptive Statistics and CT Findings Summary for Children <2 Years
Ninety-seven examinations were performed in children <2 years (42.3% female). Fracture and ICI rates in this group were 34% and 24.7%, respectively (Table 2). Five patients (5.2%) underwent additional imaging.
Descriptive Statistics and CT Scan Findings for Patients <2 Years of Age.
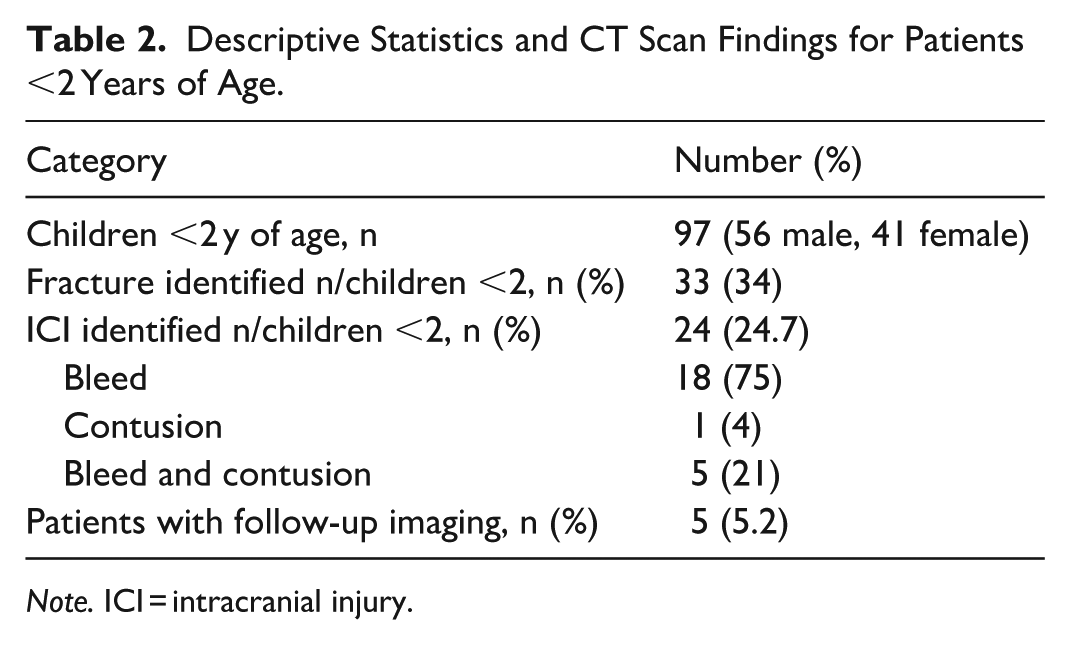
Note. ICI = intracranial injury.
Comparison of Abnormal CT Findings by Age Group
Fractures were significantly more common among children <2 years (34%, 95% CI 25.4%-43.8%) compared with older children (15.2%, 95% CI 11.3%-20.2%; P < .001; Table 3). Intracranial injury was also more common in children <2 years (24.7%, 95% CI 17.3%-34.0%) compared with children ≥2 years (12.9%, 95% CI 9.4%-17.5%; P = .007; Table 3).
Comparison of CT Findings Across Age Groups.

Note. ICI = intracranial injury.
Discussion
This single-centre retrospective review describes after-hours non-contrast cranial CT utilization patterns for pediatric head trauma over a 4-year period at a tertiary care centre. Most examinations (74%) demonstrated no acute traumatic findings, including skull fracture or ICI. These findings highlight patterns of CT utilization and diagnostic yield within the imaged cohort and do not permit assessment of overall imaging rates, ciTBI prevalence, or decision-rule adherence.
Despite the overall low prevalence of clinically significant findings, age-related differences were notable. Children <2 years demonstrated significantly higher fracture and ICI rates compared with older children. This likely reflects anatomical vulnerability, distinct injury mechanisms in early developmental years, and limitations of clinical assessment tools, particularly in preverbal infants.5,23 In a study by Markovic et al examining CT findings in children under 3 years with mild TBI, skull fractures, and intracranial hematomas were observed in 46% and 13.8% of cases, respectively. 13 Although our ICI rates are comparable, direct comparison is limited because TBI severity was not stratified in our cohort. These factors support careful age-specific risk stratification while maintaining attention to radiation stewardship.
Radiation Risk
Radiation exposure from CT remains a significant concern in pediatric imaging. A recent large population-based study further demonstrated an association between pediatric and adolescent exposure to ionizing radiation and increased risk of hematologic malignancy. 24
In our cohort, mean DLP values exceeded international and provincial pediatric Diagnostic Reference Levels (DRLs) by approximately 20% to 50% across age groups. 25 Our provincial DRLs are 404.1, 574.6, 729.3, and 871.9 for children aged <1, 1-5, 6-10, and 11-15 years, respectively. These findings suggest potential opportunity for protocol optimization and equipment updating or replacement, while preserving diagnostic image quality.
Although younger children have a higher risk of both skull fracture and ICI, alternative imaging modalities should be readily considered when appropriate. For example, in young children with an open fontanelle, formal diagnostic cranial ultrasound or point-of-care ultrasound (POCUS) provide radiation-free options.
Future Directions: Point-of-Care Ultrasound
POCUS has emerged as a promising tool for ED physicians in the initial evaluation of skull head trauma, particularly for the detection of skull fractures prior to CT. 26 POCUS demonstrates high sensitivity (91%) and specificity (96%) for detecting skull fractures. 26 When a fracture is identified, subsequent CT may be appropriate in high-risk patients, as 25% to 55% of infants and young children with skull fractures have associated intracranial hemorrhage.23,27 However, most hemorrhages are small and rarely require neurosurgical intervention. 23
POCUS may therefore serve as a radiation-free alternative to immediate CT in carefully selected lower-risk patients, particularly in tertiary pediatric centres with ultrasound expertise. In our study, some ED records indicated POCUS was occasionally used prior to CT; however, these studies are not archived at our institution, precluding evaluation of POCUS findings or their influence on subsequent imaging decisions. Prospective studies are needed to assess the reliability of POCUS in routine practice and to define its optimal integration into pediatric head trauma pathways.
Resource Stewardship and After-Hours Imaging
CT overuse not only exposes children to unnecessary imaging risks but also burdens the healthcare system, particularly when many scans occur after-hours. 28 Staffing demands for safely imaging young children, especially during off-hours, create further operational challenges.
Imaging decisions during after-hours periods may be influenced by contextual factors. Increased CT utilization is likely multifactorial: higher acuity presentations outside regular business hours, reduced ED observation capacity, limited availability of senior clinical support, and operational pressures may all contribute.29-32 Prior literature suggests that a substantial proportion (70%) of ED CT examinations are performed after-hours and that nighttime arrival may be associated with increased imaging utilization. 33
Barriers to observation are more pronounced after-hours, including difficulty assessing alertness in tired children, parental preference, and concerns regarding follow-up reliability. 32 One study found that after-hours arrival (10 PM to 6 AM) was associated with increased CT utilization in head-injured children. 29
Observation Interval
Short periods of ED observation have been proposed as a safe and effective strategy to reduce unnecessary CT use in children with minor head trauma, in alignment with the PECARN guidelines. 10 A United States study from Arora et al found that observation in intermediate-risk children reduced CT use without affecting clinical outcomes or length of stay. 1 A German study from Schmittenbecher et al reported CT use in only 13.4% of pediatric TBI cases across all severities when an observation-first approach was implemented. 34 These findings support initial observation as a safe, cost-effective alternative to immediate CT in appropriately selected children.
In older children, short ED observation, either by a nurse or responsible, well-instructed caregivers, can safely reduce unnecessary CT use without compromising care. 32 This approach is not intended to shift workload from radiology to the already burdened ED teams, but rather to suggest that caregivers may be empowered to assume part of the observation role at home. Providing clear caregiver education on expected symptom progression, red flags warranting urgent reassessment, and reassurance regarding the typically benign nature of minor head injuries can maintain safety while conserving radiology and ED resources.
While our study did not review all ED records, a few cases noted initial observation periods among those with positive findings. These observations support continuing to encourage an observation-first strategy in children categorized as intermediate-risk children within the PECARN framework, who have an estimated 0.9% risk of ciTBI. 10
Documentation Quality as a Barrier to Guideline Implementation
Among children with positive CT findings, nearly one-third (31.9%) had a GCS ≤14, a group for whom CT imaging is unequivocally indicated according to PECARN guidelines. 10 Inclusion of these higher-acuity cases likely contributed to the observed diagnostic yield. 35
A key finding was the substantial proportion of cases with incomplete clinical documentation. Among children with positive CT findings, 31.9% lacked documented GCS scores, despite GCS being fundamental to PECARN risk stratification. 10 Incomplete documentation limits retrospective evaluation of clinical decision-making, risk stratification, and adherence to established decision rules. Furthermore, imaging guideline adherence could not be assessed, as ciTBI was not directly measured and denominator data were unavailable. Standardized documentation of decision-rule variables represents a system-level opportunity to improve risk stratification, quality assurance, and future research.
Limitations
This study has several limitations. First, its retrospective design in a single centre limits the generalizability of these findings. Second, incomplete clinical documentation, including GCS scores and specific rationale for CT referral, hindered comprehensive evaluation of guideline adherence and risk stratification. Third, because this study used PACS data, it did not capture patients managed conservatively without imaging, and injury severity cannot be reliably determined. The primary aim of this work was to describe CT utilization patterns and quantify imaging volume in this cohort rather than assess appropriateness of imaging or adherence to guidelines. Future research at our centre should include prospective studies and detailed ED chart reviews to contextualize CT use within the total population of head-injured children.
Conclusions
This study provides an objective description of CT utilization patterns in pediatric head trauma cases imaged after-hours at a single tertiary centre. Most examinations did not demonstrate acute ICI or skull fracture, particularly among children ≥2 years. Children <2 years demonstrated higher diagnostic yield, underscoring the importance of age-specific risk stratification.
While CT remains essential for detecting clinically significant injuries, these findings suggest opportunities to optimize imaging practices in pediatric head trauma through improved clinical documentation, structured observation strategies for intermediate-risk patients, and thoughtful integration of alternative imaging modalities. Future studies at our centre should incorporate total head-injured children presenting to the ED, clinical context, and outcomes to evaluate decision-making patterns and identify safe strategies for optimizing imaging while maintaining diagnostic accuracy.
Supplemental Material
sj-docx-1-caj-10.1177_08465371261435381 – Supplemental material for Cranial Computed Tomography Use in Pediatric Head Trauma: Assessing Appropriateness, Insights, and Recommendations in a Single-Centre Cohort
Supplemental material, sj-docx-1-caj-10.1177_08465371261435381 for Cranial Computed Tomography Use in Pediatric Head Trauma: Assessing Appropriateness, Insights, and Recommendations in a Single-Centre Cohort by Marley Blommers, Minwoo Park, Jessica Kimber, Mauricio Rico Quiranz, Sunaina Ramdass, Beth MacDonald, Katie Gardner, Tahani Ahmad and Mareen S. Kraus in Canadian Association of Radiologists Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.