
Abstract
Background:
Call is among the most challenging aspects of radiology residency, fostering both knowledge development and decision-making under pressure. As imaging volumes have increased, call conditions have evolved. However, little is currently known about the variability in call structures among institutions. This study explores the perceptions of resident call across Canadian radiology programs.
Methods:
A 28-question, bilingual, anonymous survey was distributed to all Canadian radiology residents via the Canadian Association of Radiologists (CAR) and institutional representatives of the CAR Resident and Fellow Section (RFS). Anonymous data was collected including demographic information, sleep habits, staff supervision, interactions with referring physicians, and wellness.
Results:
Our survey was open from Sept 1, 2024, to Feb 28, 2025. Altogether, 112 residents responded from all training levels and programs, with 71.4% completing it in English and 28.6% in French. Most PGY-2 residents reported 8 to 11 call shifts in the preceding 8 weeks, compared to 4 to 7 shifts among PGY-3 to PGY-5. Close to half of residents reported that they did not sleep at all on call. Among those who did, 70.3% of them reported moderately insufficient sleep. Interactions with referring physicians were poor, with 49.2% of residents rating their experiences as unsatisfactory or very unsatisfactory. Lower call satisfaction was significantly associated with greater call volume and reduced sleep.
Conclusions:
Canadian radiology residents reported high call volumes, limited rest, and challenging interactions with referring physicians, all of which were linked to lower satisfaction and well-being. These findings highlight opportunities to optimize call structures, strengthen supervision, and improve resident wellness.
Introduction
Call represents one of the most challenging aspects of radiology residency in Canada. On call, residents’ knowledge and efficiency are put to the test; they develop autonomy through management-defining decisions made under time pressure and limited, if any, supervision. As imaging volumes have surged, call conditions have also changed resulting in increased call cases, increased advanced modality studies (ie, CT, MRI), and longer call hours. Fatigue secondary to such conditions may impact resident performance and lead to reduced quality reports. 1
Residency programs and their affiliated academic hospital centers are faced with the challenge of balancing resident call exposure, rotation attendance, adequate call-coverage, and resident wellness. For example, residents performing less call may improve their rotation attendance and wellness but may lack on-call learning opportunities. Those with frequent call may be deprived of day-time teaching and rotation-exposure, and may be more predisposed to burnout. 2 On a provincial level, certain residency associations have attempted to palliate the burden of call by adopting policies that limit call hours, protect time off from rotations, and enforce rest time between shifts.3-10 On a local level, programs use a pyramidal call system to allow residents to gradually adapt to call conditions, but have variable avenues of support once independent call has begun and have widely different call structures. 11 Although call conditions have seemingly become more difficult, there is little data on the current climate of call as experienced by radiology residents.
The current study seeks to identify the perceptions of call by residents in Canadian radiology programs by surveying Canadian radiology residents. The specific objectives of the survey study include the following: (1) to explore the satisfaction and well-being experienced by radiology residents on-call, (2) to investigate factors that may influence their experiences, and (3) to explore how the on-call experience can be improved from a trainee perspective. We hypothesize that radiology residents’ on-call satisfaction is influenced by workload, sleep quality, quality of supervision, and interaction with referring physicians. We hypothesize that on-call satisfaction is associated with improved resident well-being.
Methods
After a thorough literature review, we designed a 28-item questionnaire exploring call perception among radiology residents. The study was then piloted among the Canadian Association of Radiologists Resident and Fellow Section (CAR-RFS) institutional representatives for feedback. The most updated version was then revised by a collaborator from the Centre de pédagogie appliquée aux sciences de la santé at Université de Montréal. After obtaining institutional ethics approval, the online bilingual, anonymous survey was distributed to Canadian radiology residency programs via email by the CAR and individual CAR-RFS members. The survey remained open from Sept. 1, 2024, to February 28, 2025.
All individuals enrolled in a Canadian radiology residency program and part of the call pool (ie, doing independent call as of Sept. 1, 2024) were included in the study. Residents who had not yet started radiology call (ie, PGY-1 radiology residents on off-service rotations) were excluded. The 28-item anonymous, self-reported, electronic survey included questions regarding: demographics (ie, year of residency, name of institution), call workload, sleep quality and quantity, staff supervision, interactions with requesting physicians, and wellness. Wellness questions were based on The World Health Organization-Five Well-Being Index (WHO-5). 12 Residents could optionally fill out an open-ended question at the end of the survey asking for recommendations to improve call conditions. The complete survey can be found under Supplemental Materials.
Descriptive analyses were performed on demographic data, which were stratified by academic year and time interval. Categorical and continuous variables were assessed using Fisher’s exact test and Mann-Whitney U test, respectively. Questions about call perception and satisfaction were evaluated using Likert scale and parametric analysis were performed by ANOVA. Statistical analyses were performed using SPSS, using a two-sided P < .05 as an indicator of statistical significance.
Results
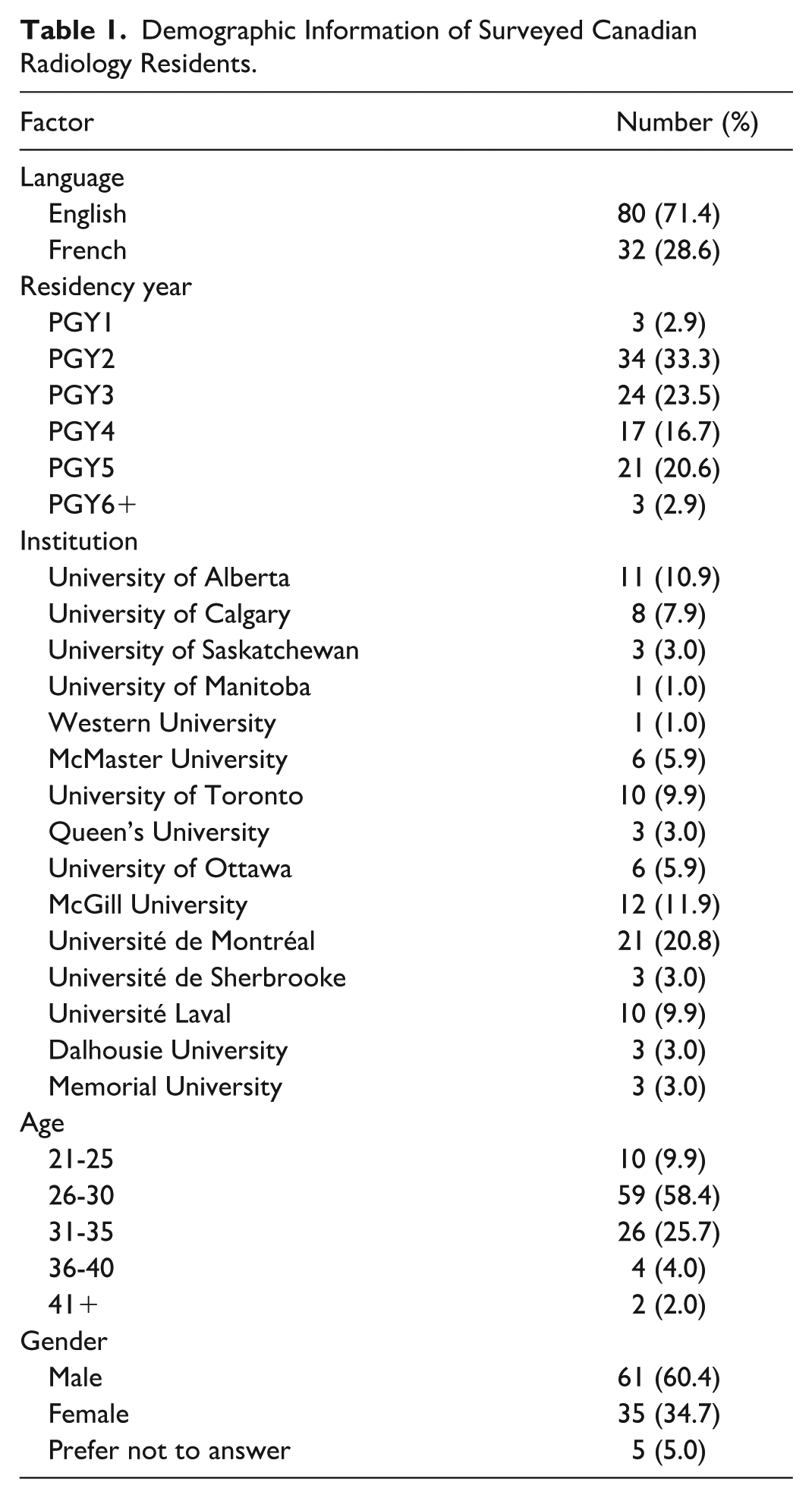
A total of 112 Canadian radiology residents completed the survey, with 71.4% responding in English and 28.6% in French (Table 1). Respondents represented all training years, with the largest proportions from PGY-2 (33.3%) and PGY-3 (23.5%). Three respondents (2.9%) were PGY-1 residents and were excluded from the further analysis. Gender distribution was balanced across respondents, and all 16 Canadian residency programs were represented.
Demographic Information of Surveyed Canadian Radiology Residents.
Call volume varied widely across training levels and programs, with most residents completing 10 or 11 call shifts in the last 8 weeks (Figure 1). Most PGY-2 residents reported completing between 8 and 11 call shifts in the 8 weeks preceding survey completion, while PGY-3 to PGY-5 residents reported fewer call shifts (generally between 4 and 7). More senior residents (PGY-5+) reported <4 shifts during the same time. Overnight call was the predominant structure, though access to a post-call day was inconsistent between programs.
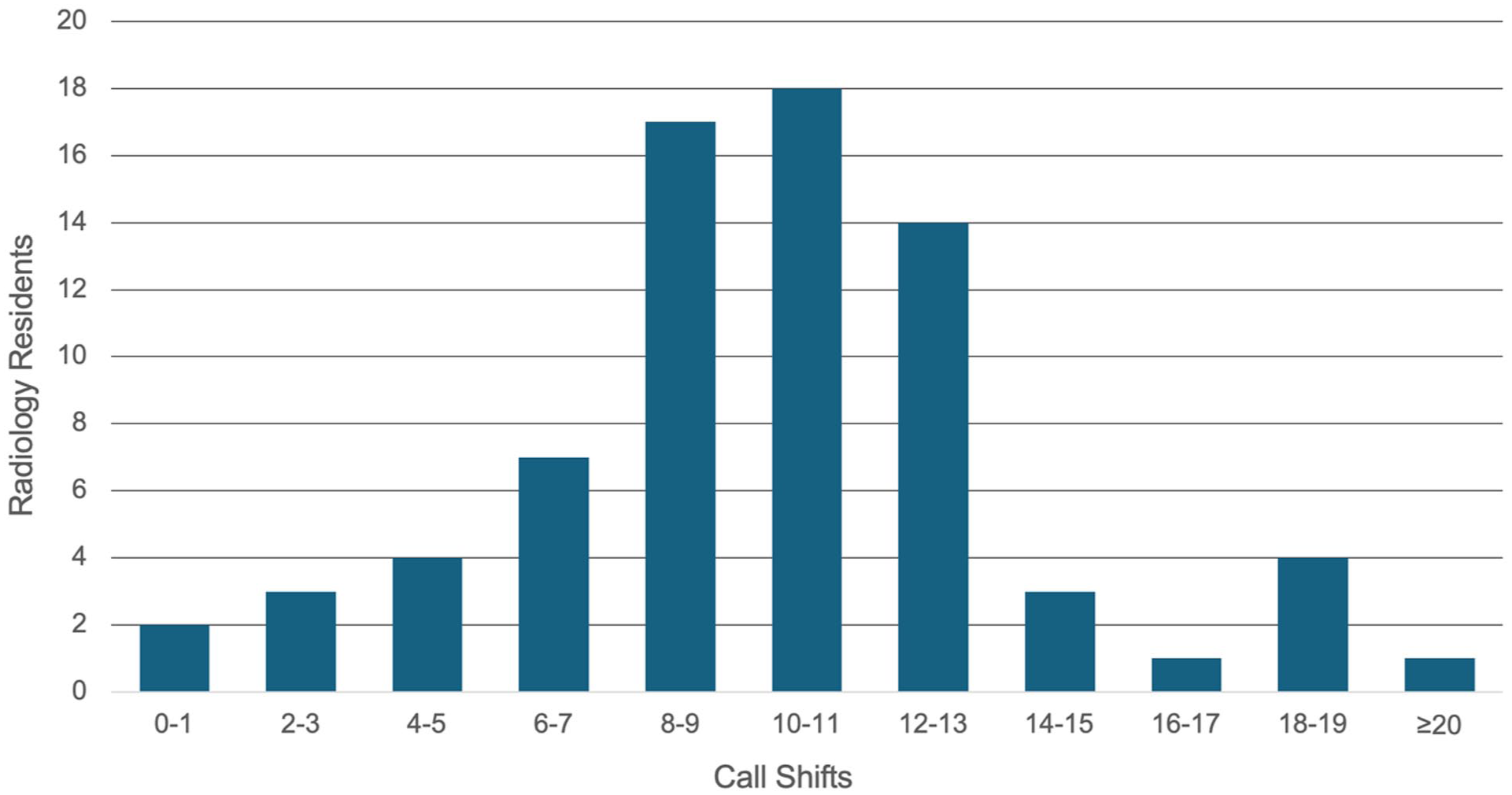
Distribution of number of call shifts among surveyed Canadian radiology residents in the past 8 weeks.
The volume of cases seen per call also varied depending on weekday or weekend shifts (Figure 2), with most residents submitting over 90 preliminary reports on an average weekend shift. As expected, CT was the predominant modality read on call, while responsibilities pertaining to other modalities were inconsistent between programs. For example, not all programs read MRI on call. With respect to ultrasounds, most residents submitted <10 preliminary reports during a typical call shift. On the weekend, a few (22.2%) centers reported between 10 and 19 ultrasound studies. Some residents cited availability of ultrasound technologists on call, while for others, residents themselves were responsible for performing the ultrasounds.
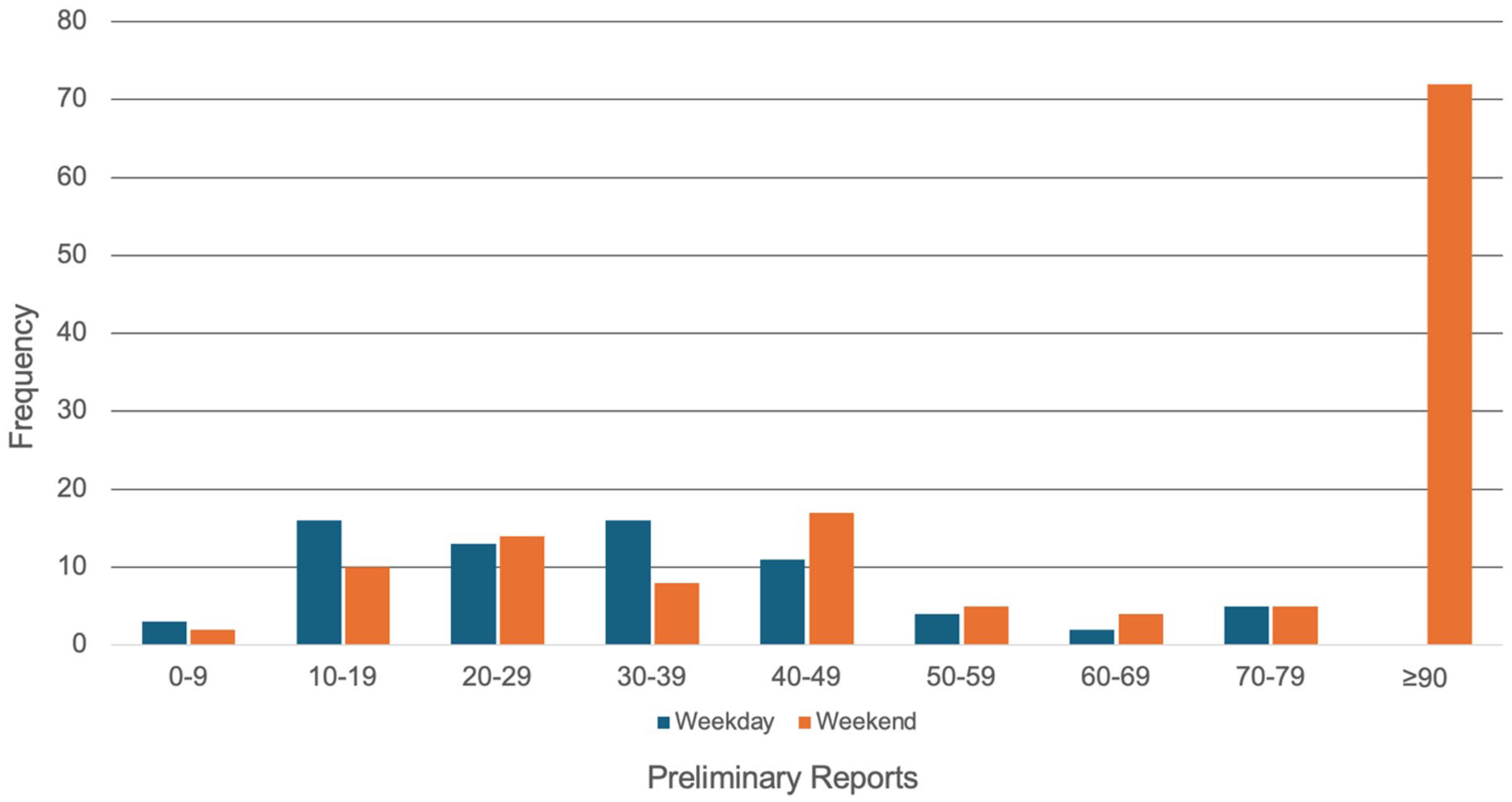
Number of preliminary reports submitted during weekday and weekend shifts, on average, in the past 8 weeks.
Most residents described case volume on call as unmanageable or very unmanageable (62.4%; Figure 3). Difficulty managing case volume slightly decreased with more advanced residency level. In stratified analyses, 100.0%, 74.2%, and 70.8% of PGY-2, PGY-3, and PGY-4 residents, respectively, rated call volume as unmanageable or very unmanageable, whereas only 33.3% of PGY-5 residents found case volume unmanageable or very unmanageable.
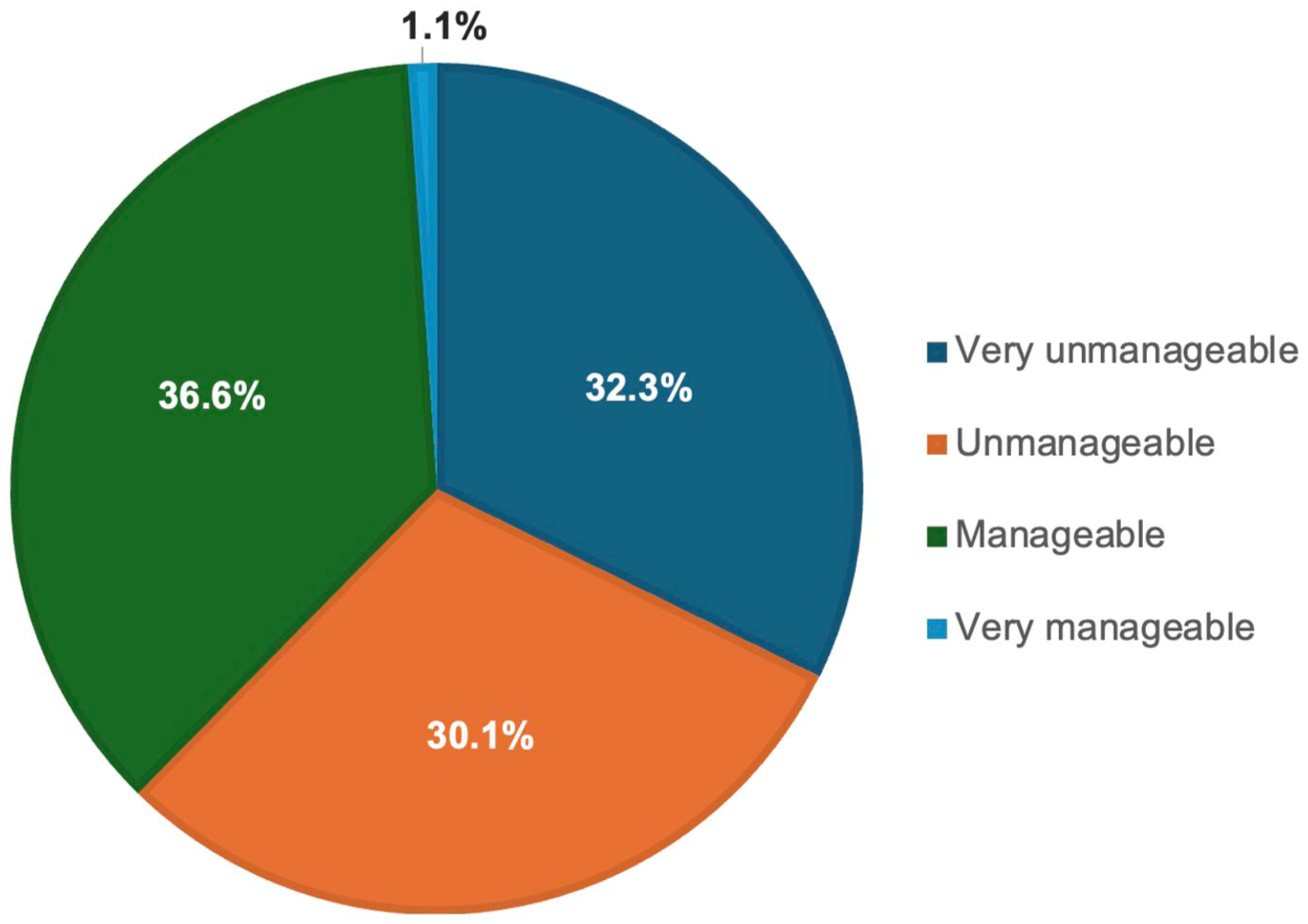
Resident perception of call volume during each call shift over the past 8 weeks.
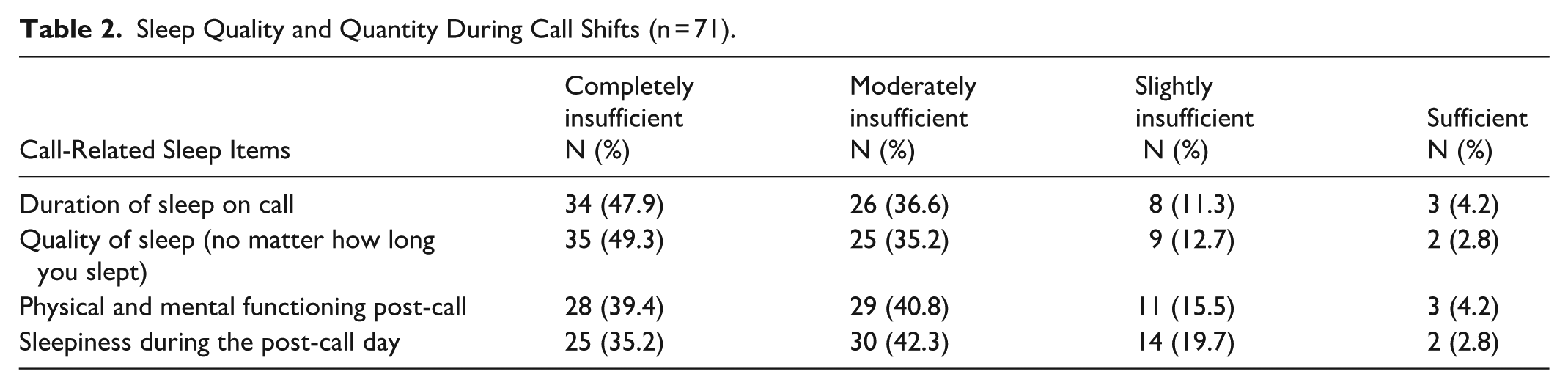
Approximately half (47.9%) of residents reported that they did not sleep at all on call (Table 2), deviating from the norm. Among those who did, 70.3% of them reported moderately insufficient sleep. Quality of rest post-call varied significantly by program. 80.2% of residents indicated moderate-to-severe decreased functioning post-call. Residents also reported that fatigue negatively impacted both clinical decision-making and learning efficiency.
Sleep Quality and Quantity During Call Shifts (n = 71).
Most residents reported that direct staff supervision was available by phone (85.3%) but rarely in person (12.7%). Perceived adequacy of supervisions improved with training level; 40.9% of PGY-2s rated supervision as “insufficient” or “poor” compared to 28.5% PGY-3s, and <15% PGY4+. Most (72.2%) respondents felt staff backup was sufficient for safe patient care, though this varied depending on the attending on-call.
Residents’ perceptions of their interactions ranged from “authoritative” to “collaborative.” Overall satisfaction with referring physician interactions was low, with 49.2% of respondents rating their experiences as unsatisfactory or very unsatisfactory. Qualitative data revealed that interactions were more positive when radiology residents were treated as consultants rather than as “service providers.”
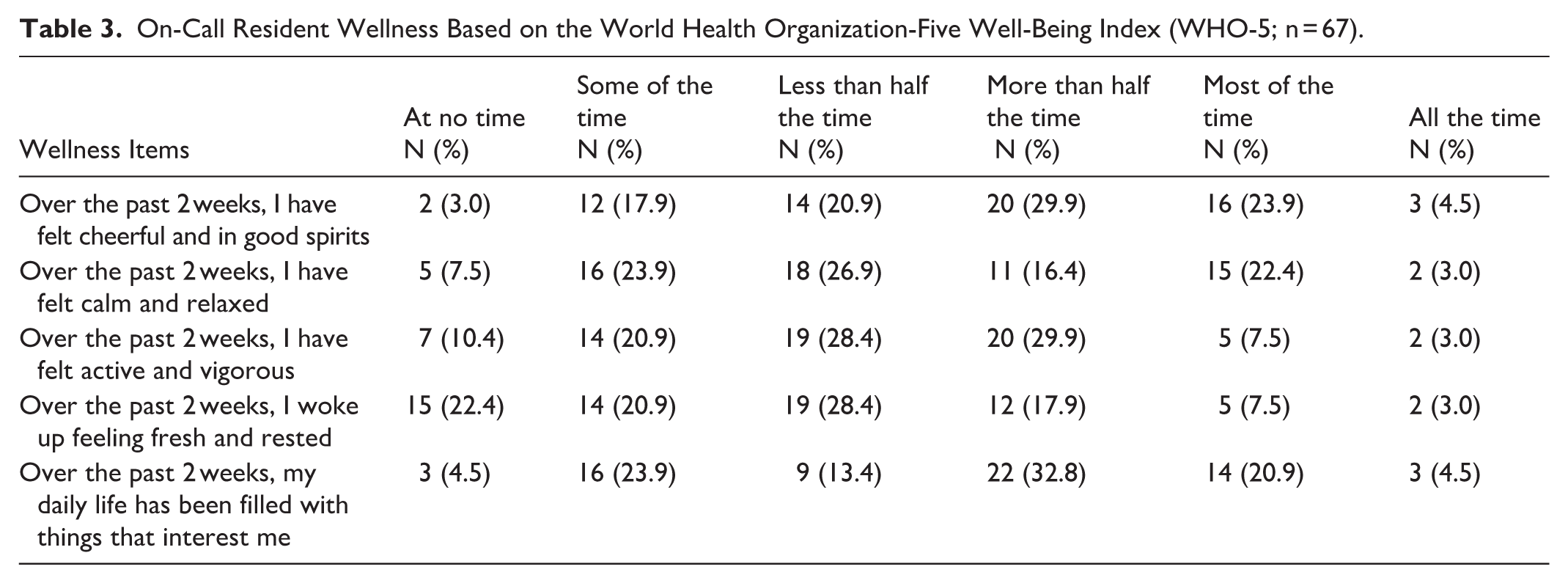
Mean call satisfaction decreased with higher call volumes and poorer sleep quality (P < .05). For instance, residents reporting little to no sleep on call – a deviation from the norm – consistently reported lower satisfaction. Self-reported wellness varied, with over half of residents having reported being cheerful or in good spirits majority of the time (Table 3). On the other hand, 71.7% of residents reported waking up feeling fresh and rested less than half of the time with 22.4% of residents responding at no time. Wellness questions also indicated that many residents felt stressed and exhausted during call-heavy periods.
On-Call Resident Wellness Based on the World Health Organization-Five Well-Being Index (WHO-5; n = 67).
Discussion
This national survey highlights important systemic challenges faced by Canadian radiology residents during call. Residents reported variable experiences across institutions and training levels, with high call volume, limited sleep, and variable supervision emerging as significant contributors to reduced well-being and call satisfaction. These findings align with prior reports linking fatigue and increased workload to decreased diagnostic accuracy and burnout among radiology trainees.1,13
Call volume was a central source of dissatisfaction, with most respondents describing case volume as unmanageable or very unmanageable. Overall, as post-graduate year increased, residents found call volume to be slightly more manageable. However, a significant number of residents still found call volume difficult to manage despite being quite advanced in their training, with 70.8% of PGY-4 residents and 33.3% of PGY-5 residents describing case volume as unmanageable or very unmanageable.
Interactions with referring physicians also represented a major source of dissatisfaction. Over one-third of residents described these interactions as poor or unsatisfactory, echoing prior studies that suggest radiologists are often viewed as peripheral rather than central to patient care. A recurring suggestion in our survey was increased awareness among referring clinicians on call conditions, the role of imaging, and application of imaging appropriateness criteria. This raises broader questions about the culture of interdisciplinary communication in academic hospitals and its impact on resident learning and professional identity. 14
Supervision was another key area of concern. While staff radiologists were generally available by phone in case the resident had a question, in-person support was limited. This may reflect increasing workload pressures on staff, but it also highlights discordance between the goals of resident autonomy and patient safety. 15 A minority of Canadian centers have staff correcting resident reports over 24 hours. Among residents who did not have 24-hour corrections, multiple comments expressed interest in increased evening support and the implementation of 24-hour coverage. Routine phone corrections were a point of concern. Residents cited that phone corrections often would begin after the end of their call shift. On the other hand, other comments mentioned that the interruption of reading from phone corrections during the call shift was incompatible with the continuous high volume of cases. Programs must carefully balance these priorities, particularly for junior residents who are newly transitioning to independent call.
Resident wellness and sleep are imperative for efficient and safe performance on call. Call satisfaction appeared to relate to workload and rest, with higher call volumes and poorer sleep associated with lower mean satisfaction scores. Wellness responses indicated that many residents experienced fatigue and reduced energy during call-heavy periods.
These findings add to the limited literature on the Canadian radiology resident call experience and provide a descriptive overview of current conditions across programs.16,17 They also highlight the need for systemic strategies to reduce resident fatigue – whether through optimized call schedules, protected time off for rest and recovery, or increased staff support overnight.
Conclusion
To the best of our knowledge, this national survey is the first of its kind to provide a comprehensive overview of Canadian radiology residents’ experiences with call. Residents reported high call volumes, insufficient supervision, and frequent fatigue, all of which were associated with lower satisfaction and well-being. Interactions with referring physicians also represented a key challenge. These findings highlight opportunities for programs and national organizations to optimize call structures, support resident well-being, and strengthen supervision models.
Supplemental Material
sj-pdf-1-caj-10.1177_08465371251407871 – Supplemental material for Perceptions of Call by Canadian Radiology Residents: A National Survey
Supplemental material, sj-pdf-1-caj-10.1177_08465371251407871 for Perceptions of Call by Canadian Radiology Residents: A National Survey by Claudia Deyirmendjian, Neel P. Mistry, Ha Le, Pamela Boustros and Michael N. Patlas in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
We would like to thank Mr. Robert Gagnon of the Centre de pédagogie appliquée aux sciences de la santé at Université de Montreal, for revising the call questionnaire.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Canadian Association of Radiologists Resident and Fellow Section (RFS).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Michael N. Patlas is the Editor-in-Chief of the CARJ and the senior author of this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.