
Abstract
Purpose:
This study examines factors contributing to burnout among radiology residents through a Canadian lens and assesses strategies employed at our institution to mitigate its impact.
Methods:
This was a single-institution cross-sectional study. Four anonymous online surveys were administered through Qualtrics to PGY 2-5 radiology residents from 2021 to 2025. These surveys identified residents with burnout and distress and assessed contributing factors, suggestions for reducing burnout, and residents’ responses to implemented interventions. Interventions were employed at 2 hospitals within our institution.
Results:
The surveys had response rates of 30% (2021), 57.7% (2023), 60% (2024), and 62% (2025). 50% of pre-intervention respondents were identified as burned out. The rate reduced to 18.8% post-intervention, with results not being statistically significant (P = .167). Top factors driving burnout included time (eg, increased work hours, time constraints), extra duties (clinical and administrative), and perceived lack of radiology knowledge when dealing with complex cases. Interventions included additional daily 1-hour teaching sessions, wellness lunch rounds, debriefing sessions, transitioning from paper-based protocolling to a hybrid-electronic paper-based system, call schedule modifications, improved ergonomics, and social functions, including incorporating indoor and outdoor activities. Interventions targeting work hours were subjectively the most well-received in combating burnout.
Conclusion:
This study underscores the prevalence of burnout among radiology residents. Our institution has implemented a multi-faceted approach to address burnout within our radiology residency program.
Introduction
Burnout is characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment. Physician burnout has garnered significant attention due to its high prevalence, with nearly half of all physicians experiencing some component of burnout. 1 This issue has profound negative impacts, including poor patient care and outcomes, higher health care costs, and increased staff turnover. 1 Previous studies have demonstrated that radiologists experience notably high rates of burnout, affecting up to 85% of trainees.2,3 Compared to non-radiologists, radiologists are more likely to feel unhappy and undervalued in the workplace, particularly by leadership. 4
Further, Canadian radiology residents report higher burnout rates, particularly in the domains of emotional exhaustion and depersonalization, compared to Americans.3,5 For instance, 50.7% of Canadian radiology residents reported high emotional exhaustion compared to 37% of radiology residents working in New England.3,6 This complex issue is driven by multiple factors, including heavy workload and rising expectations, prolonged working hours, physical and social isolation, and frequent workflow interruptions.7-12 In particular, Canadian radiology trainees have cited poor work-life balance, insufficient support from radiology attendings, and dissatisfaction within their program as driving forces for burnout.5,6,10 While the number of Canadian radiology residency positions have decreased, American residency programs are generally larger, often including more fellows, which provide an added layer of support and help reduce the call frequency.10,13 Call burden is further reduced as the transition to independent call tends to be more graduated among American programs, with PGY2 residents typically not working overnight. Many American programs have also shifted from the traditional 24-hour shifts to a night float system. Finally, the requirement for Canadian residents to pass an oral board examination for licensing may be a contributory factor in burnout. 6
Efforts have been made within the radiology community to raise awareness, promote advocacy, and take action to enhance wellness. Previous studies have supported both individual (“bottom-up”) and structural (“top-down”) strategies to combat burnout, with the Association of University Radiologists advocating for a combined “top-down” and “bottom-up” approach. 14 At the inaugural 2023 American Roentgen Society wellness summit, the “top-down, bottom-up” approach was further expanded in that physician well-being programs should not only be leadership-drive (“top-down”), but also receptive to feedback (“bottom-up”). 15 Similarly, the American College of Radiology has recommended 10 actions to correct burnout risk factors on an institutional and individual level. 16 These recommendations included ensuring adequate staffing, reducing call responsibilities, improving workflow efficiencies, restoring a sense of control, promoting lifestyle balance, reducing feelings of stress and isolation, and fostering community engagement. 16
There is a lack of studies that examine the implementation and use of interventions to mitigate burnout among radiology trainees. Notably, our study is the first in Canada to investigate self-reported burnout among radiology residents, survey solutions, and evaluate these targeted interventions at our institution.
Methods
Study Setting
This single institution cross-sectional study received ethics approval by our institutional review board. The primary training environments for the residents were at 2 tertiary care academic hospitals in a large Canadian city. At the time of survey administration, in a post-pandemic setting, there were 27 PGY 2-5 residents in 2021, 26 in 2023, 25 in 2024, and 26 in 2025.
Data Collection
Four anonymous voluntary surveys were distributed through Qualtrics to PGY 2-5 residents between 2021 and 2025. PGY-1 residents were excluded from the survey due to the off-service component of the first year in the Canadian radiology curriculum. Two pre-intervention surveys were distributed in 2021 and 2023, and 2 post-intervention surveys were distributed in 2024 and 2025. After each survey, 2 reminders were sent to encourage participation.
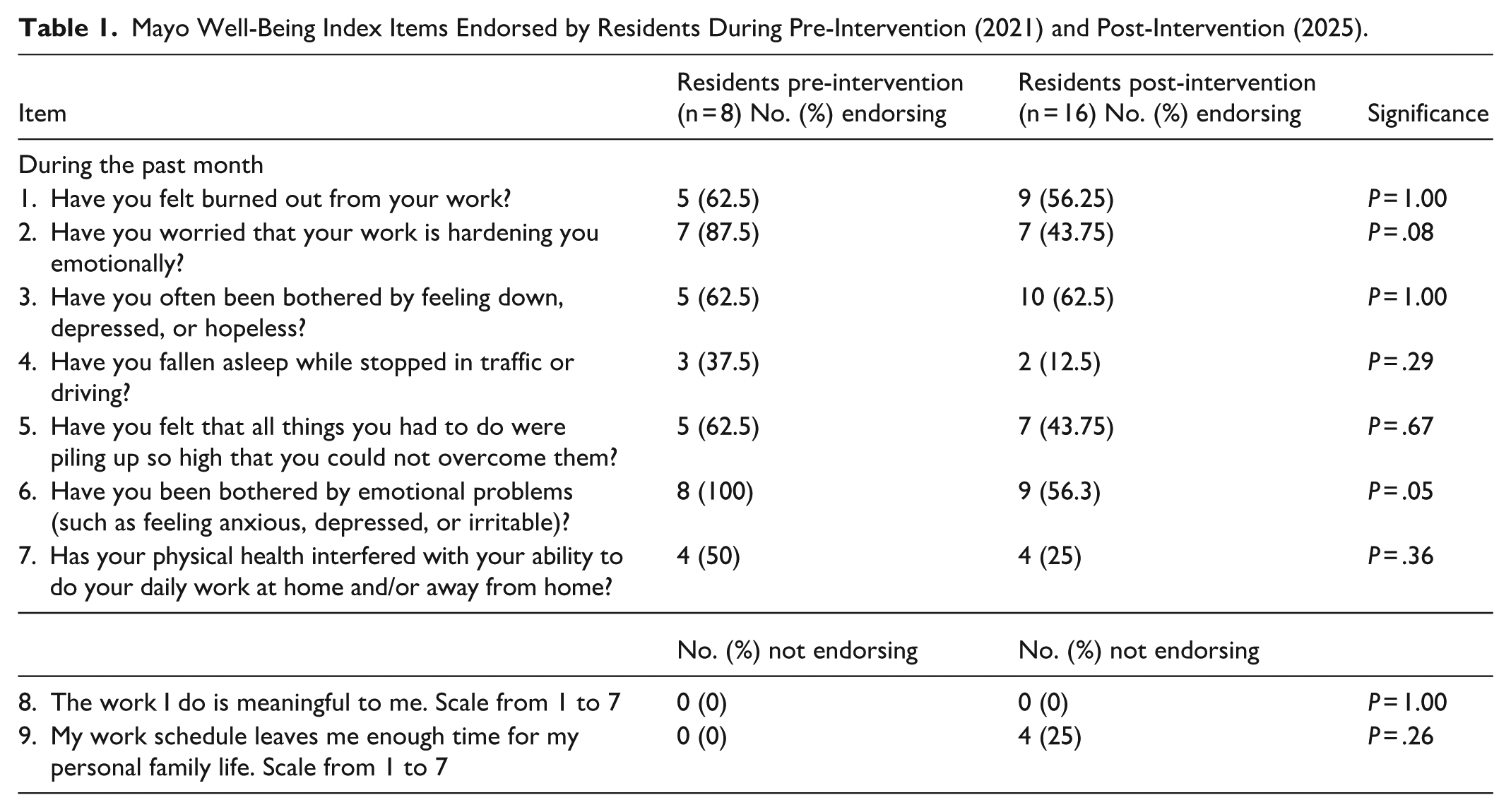
The first survey conducted in 2021 (pre-intervention) and fourth survey conducted in 2025 (post-intervention) included questions on basic demographics and burnout symptoms, using the 9-item validated Mayo Clinic Well-Being Index to screen and identify the burnout and distress rates (Table 1). Respondents answered 7 yes/no items about questions about the domains of burnout, depression, stress, fatigue, and mental and physical quality of life.17,18 The last final questions used a Likert scale to assess work life integration and meaning in work. 19 A cumulative score greater than 4 was considered positive for burnout and distress.
Mayo Well-Being Index Items Endorsed by Residents During Pre-Intervention (2021) and Post-Intervention (2025).
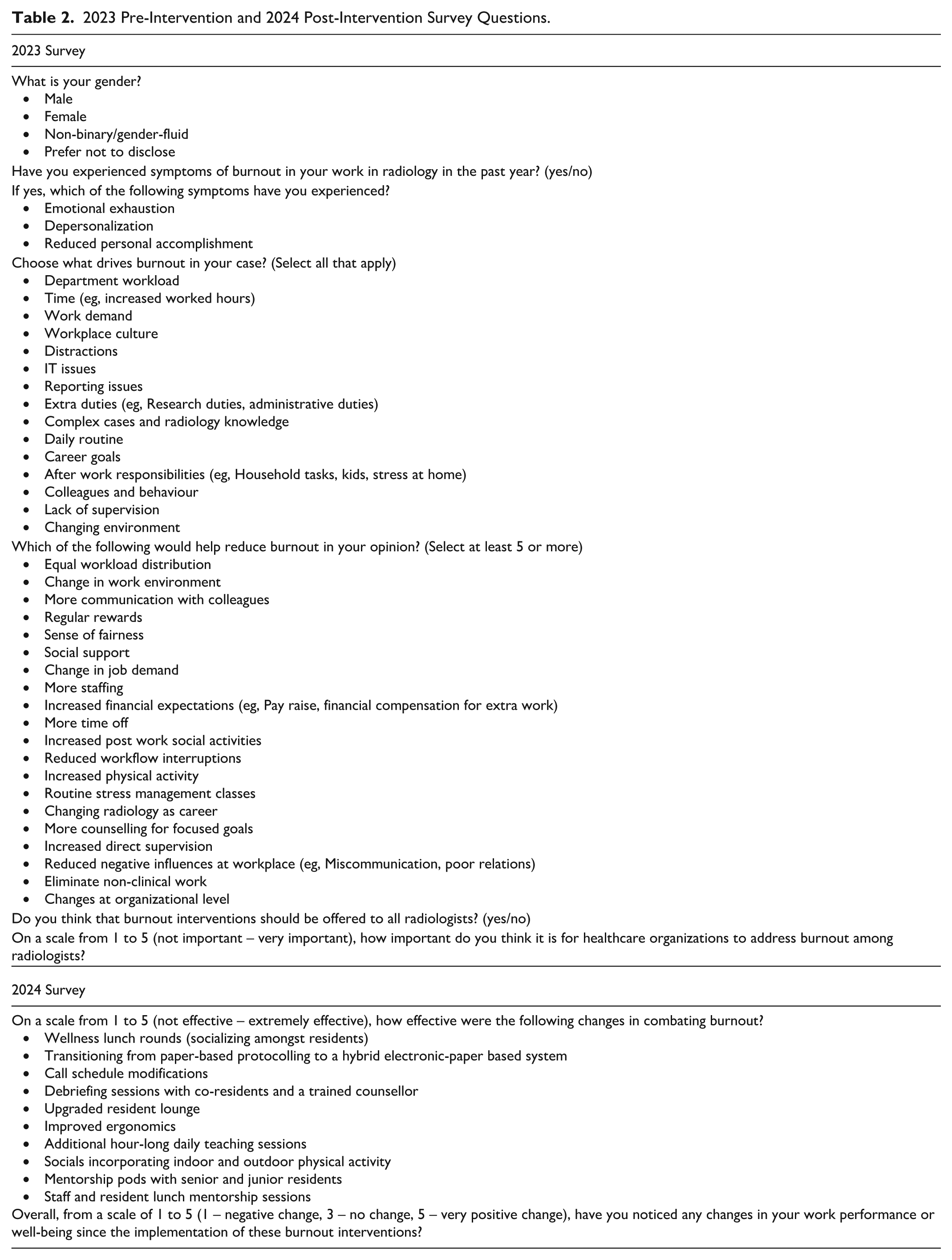
The second survey, administered in early 2023, included questions on demographics, burnout symptoms, contributing factors, and suggestions for strategies to mitigate burnout (Table 2). These variables were selected based on existing literature or were identified by the authors as potentially relevant to burnout and wellness intervention planning. Following the collection of baseline data, a series of interventions were developed and implemented during 2023 to 2024, guided by survey responses to maximize their effectiveness. The third survey distributed in 2024, used a Likert scale to assess the impact of the burnout interventions (Table 2).
2023 Pre-Intervention and 2024 Post-Intervention Survey Questions.
Wellness Initiatives
Based on the survey results, the domains of time, extra duties, work demand, perceived lack of knowledge, daily routine, and career goals were identified as areas to target interventions. Interventions were specifically aimed at improving well-being and burnout rates and were implemented between 2023 and 2024. Institutional-level initiatives were overseen by departmental leadership (Department Chair, Wellness Vice-Chair, Institutional Medical Leads, and/or Residency Program Director), while interpersonal-level interventions were headed by resident leaders (Chief Residents, Resident Wellness Representative, and/or Junior and Senior Resident Representatives). All the wellness interventions are described in detail below:
Interventions targeted at addressing work hours:
Wellness Lunch Rounds: Wellness lunch rounds involved providing residents with an unscheduled lunch break once a month to either socialize together or complete personal tasks.
Call Schedule Modifications:
Eliminating 24-hour weekend call shifts: On average, residents were previously scheduled for at least two 24-hour weekend call shifts every 4 weeks at a tertiary centre. Post-intervention, the requirement to complete 24-hour weekend call shifts was eliminated by splitting the 24-hour weekend call shifts into day and night shifts. Improving ultrasound coverage: Weekend and evening sonographers were hired at a primary and secondary care centre. Prior to this change, residents were assigned dedicated ultrasound call shifts to provide scanning coverage at this centre. This staffing implementation reduced the number of scheduled call shifts for residents.
Interventions targeted at addressing work demands:
Hybrid online and paper-based protocolling system: Paper-based protocolling was transitioned to a predominately online based protocolling system. Prior to this change, residents received a phone call for every requested scan and manually printed, protocolled, and delivered requisitions to the technologists on paper. Using online protocolling, the administrative burden and number of phone calls was significantly reduced.
Debriefing sessions: Bi-annual group debriefing sessions with resident wellness counsellors were organized. This provided residents a safe space to discuss their thoughts and concerns.
Upgrading the resident lounge: The resident lounge was upgraded with a new couch, microwave, mini fridge, microphone, and speakers.
Improved ergonomics: Ergonomic improvements were implemented in the on-call reading room, including adding a standing desk and 2 ergonomic chairs.
Social events: Social events were organized including spring and winter overnight retreats with outdoor physical activities, program-sponsored lunches at local restaurants, organized physical activities (indoor pickleball matches, disc golf and ropes courses), and seasonal gatherings (Summer and Christmas departmental parties).
Interventions targeted at resident perceived lack of knowledge:
Supplementary teaching sessions: Supplementary hour-long teaching sessions were incorporated into the program.
Interventions targeted at supporting resident career goals:
Mentorship groups: All residents were organized into informal mentorship groups that included both junior and senior residents.
Mentorship lunches: A pilot program was introduced to facilitate mentorship between staff and residents. As part of the initiative, staff members took residents out for lunch, providing an opportunity to discuss career development, share professional insights, and foster meaningful connections in a relaxed setting.
Academic Half Day on financial wellbeing: The department sponsored a grand rounds lecture and academic half day on financial wellbeing, which included a guest speaker.
Statistical Analysis
Analyses were formed on GraphPad Prism 10.5 (GraphPad Software Inc., California). Missing values were excluded from analysis. Categorical variables were expressed as values and/or percentages. Fisher’s exact test was performed to compare differences between the 2021 and 2025 respondents. A two-sided P value of <.05 was considered statistically significant. The Likert scale questions were analyzed independently where higher values indicated agreement for a certain statement.
Results
Across the 4 PGY levels, the survey response rates were 30% (2021), 57.7% (2023), 60% (2024), and 62% (2025). Using the Mayo Clinic Well-being Index, 50% of respondents were identified as being burned out and distressed in 2021 (Table 3). Notably, 87.5% endorsed being worried about work hardening them emotionally, and 100% endorsed being worried about emotional problems (Table 1).
Burnout and Distress Rates During Pre-Intervention (2021) and Post Intervention (2025).
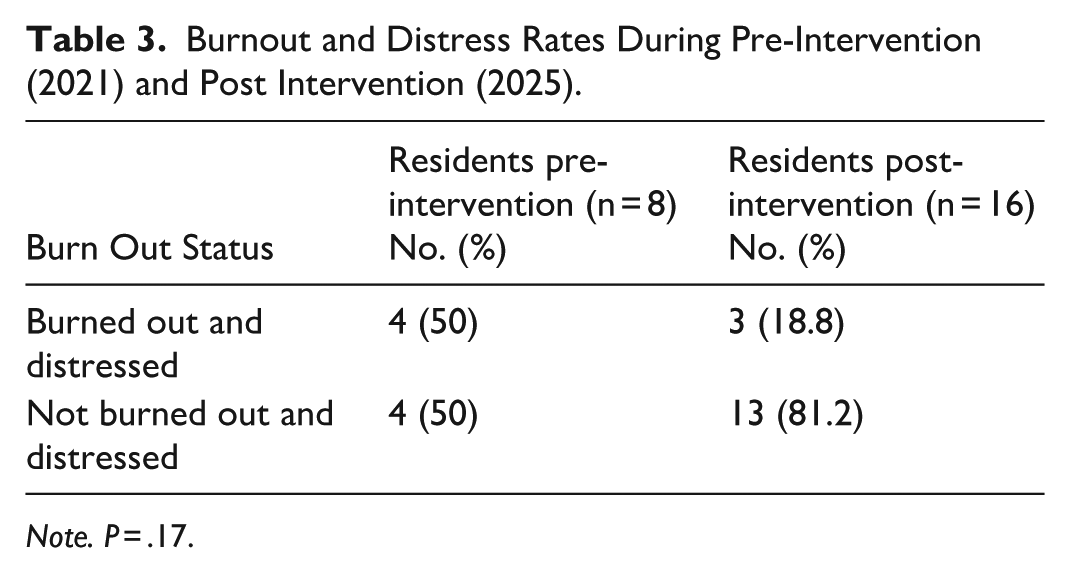
Note. P = .17.
In 2023, 80% of respondents endorsed emotional exhaustion, 40% endorsed depersonalization, and 80% endorsed a reduced sense of personal accomplishment. Key contributors to burnout included time (eg, increased work hours, time constraints), extra duties (clinical and administrative), departmental workload, distractions, and perceived lack of radiology knowledge when dealing with complex cases (Figure 1). More time off, reduced workflow interruptions, increased physical activity, elimination of non-clinical work, and increased staffing were perceived as popular potential interventions to reduce burnout (Figure 2). 87% of respondents believed that burnout interventions should be offered to all radiologists, with 73% endorsing that it is very to extremely important for healthcare organizations to address burnout.
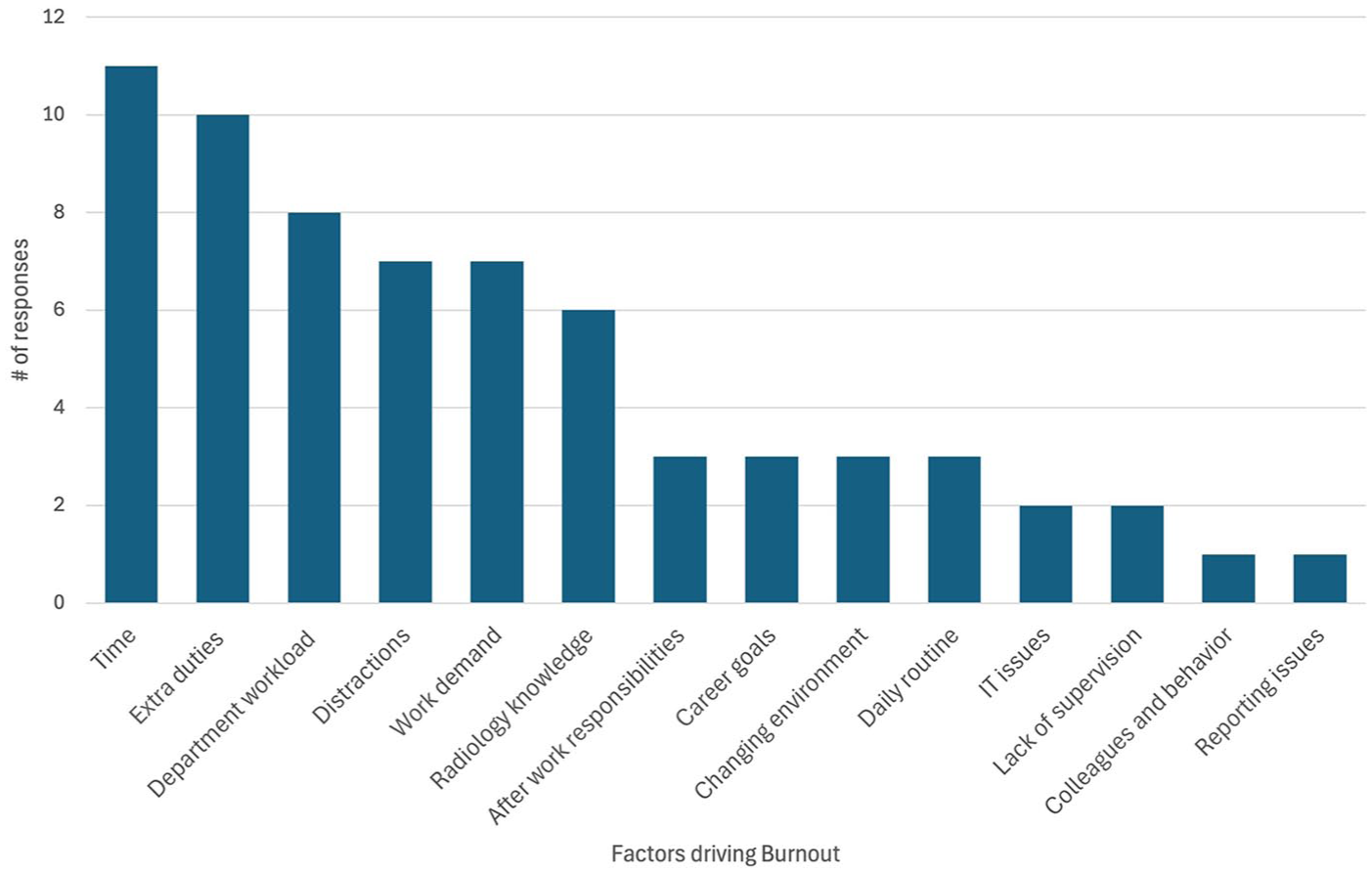
Factors contributing to resident burnout.
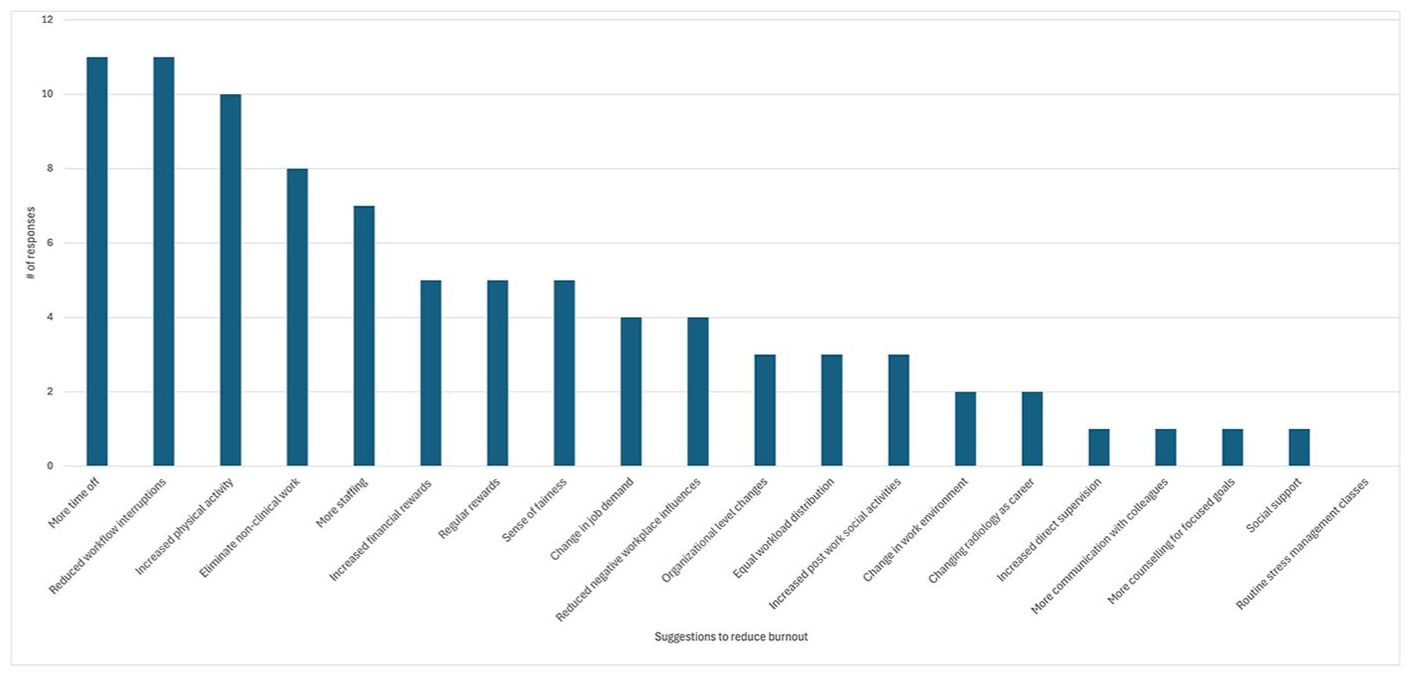
Suggestions for wellness interventions.
Over the course of the study period, residents responded positively to the interventions, with the post-intervention group having a lower range of scores from −1 to 6, compared to the pre-intervention range of 0 to 7 (Figure 3). Interventions involving work hours, such as wellness lunch rounds and call schedule modifications, were self-reported to be the most effective in mitigating burnout (Table 4). Comparatively, interventions focused on mentorship and debriefing were less favourably received, with residents rating them as only “slightly effective” in combating burnout. Modifications to work demands, such as improving the work environment through ergonomics and upgrading the resident lounge were considered “moderately effective.” 18.8% residents identified as being burned out and distressed using the Mayo Well-Being Index; however, when compared to the pre-intervention rate of 50%, this was not statistically significant (P = .167). Further, when comparing the individual items within the Mayo Wellbeing Index, there were no statistically significant differences between the pre-intervention and post-intervention respondents, despite the proportion of residents being worried about emotional problems decreasing from 100% to 56.3% (Table 1).
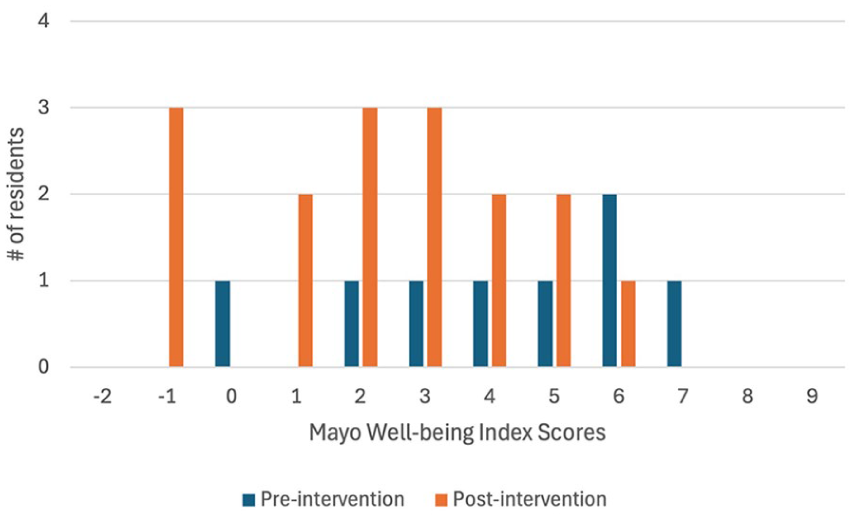
Distribution of Mayo Well-being Index Scores of residents during pre-intervention (2021) and post-intervention (2025).
Resident Response to Wellness Interventions.
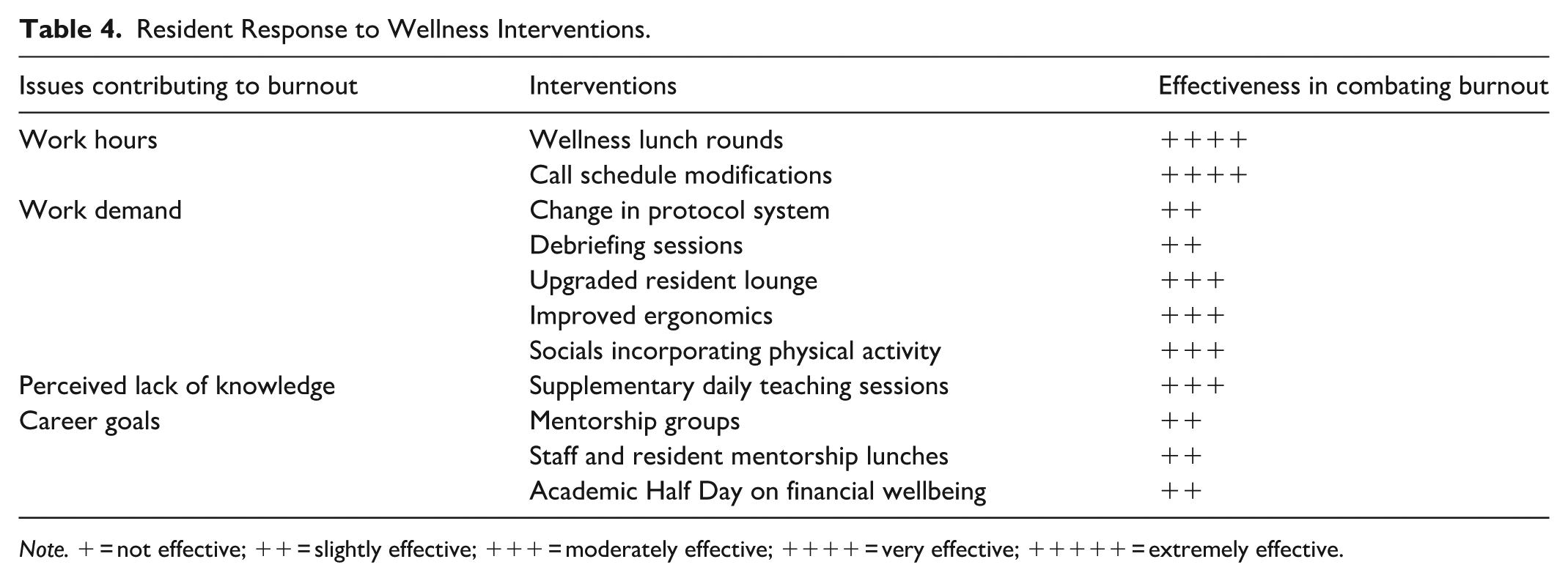
Note. + = not effective; ++ = slightly effective; +++ = moderately effective; ++++ = very effective; +++++ = extremely effective.
Discussion
To the best of our knowledge, this is the first Canadian study to survey strategies to reduce burnout, implement targeted interventions, and evaluate their effectiveness among radiology trainees. Given the high burnout rates among radiology trainees, there is a growing need for effective tools and interventions aimed at promoting physician wellbeing. Our residency aimed to improve wellness and reduce burnout by implementing wellness interventions at both interpersonal and institutional levels. The major factors contributing to burnout, such as time constraints, work demands, and knowledge gaps were noted by our cohort, similar to prior studies.6,7,10
The Mayo Well-Being Index was implemented in the pre-intervention period of 2021 and post-intervention period of 2025 to identify residents with burnout and distress and stratify their well-being. The Mayo Well-Being Index has been validated as an accurate measure of distress and burnout for physicians and trainees.17,18 Its national benchmark data, ease of scoring and administration, breadth of dimensions covered, and ability to identify residents at risk of committing medical errors are its advantages.17-19 The brevity of Mayo Well-Being Index as well as our subsequent custom surveys were designed to be cognizant of survey fatigue. This approach contributed to a response rates of 30% (2021), 57.7% (2023), 60% (2024), and 62% (2025) which were notably higher than prior Canadian studies (18.7%, 40%).5,6
Reported interventions have included individual wellness days, resident wellness retreats, and meditation and mindfulness sessions.20-22 Despite these efforts, prior research on wellness interventions for both radiologists and non-radiologists have demonstrated mixed results. For instance, Ip et al’s team implemented departmental initiatives (eg, additional week of vacation, a reading room assistant program, presentations on nutrition and sleep, etc.) to enhance team-building, work culture, work-life balance, and personal well-being. However, these initiatives did not lead to any change in radiologists’ self-reported burnout. 23 Moreover, Clemons et al investigated the effect of daily reflection, but found no significant impact on reported burnout or overall happiness among oncologists. 24 Comparatively, Pitman et al implemented a 3-year wellness curriculum, which resulted in lower burnout rates among radiology residents, with improvement specifically in emotional exhaustion and depersonalization. 22 In our study, conducted with a Canadian post-pandemic perspective, overall burnout and distress rates decreased from 50% to 18.8% between the pre-intervention and post-intervention respondents; however, this was not statistically significant. Further, there were no statistically significant differences in the individual items of Mayo Well-Being Index. This is possibly due to the inherently small sample size, (n = 8 in the 2021 survey, n = 16 in the 2025 survey) which limited the ability to conduct robust data analysis. In addition, with the surveys that spanned 4 years, some of the 2021 respondents may have graduated and some of the 2025 respondents may be new. However, the post-intervention group had a lower range of scores from −1 to 6, compared to the pre-intervention range of 0 to 7, with lower scores indicating better quality of life, less distress, and burnout. When examining the Likert score responses to interventions, interventions targeting work hours were perceived as more effective in mitigating burnout than interventions focused on mentorship and debriefing. Interventions such as wellness lunch rounds and resident retreats, originally intended to address other aspects of well-being, may have also fostered camaraderie and bonding among residents. These experiences likely provided a more natural and organic method of mentorship and debriefing, which may otherwise occur infrequently in the hospital setting. Splitting the 24-hour weekend call shifts and having weekend sonographer coverage were well-received by residents. Future initiatives could include implementing contingency plans for shift coverage, improving the work environment to ensure trainees receive adequate rest, and trialling sessions on fostering professional fulfilment. Additionally, program leadership and administration that prioritizes wellness initiatives and integrates wellness into the institutional culture can have a positive impact on the well-being of radiology trainees and overall department.2,15,23,25
This study has a few limitations. Firstly, it was conducted within a large Canadian program consisting of 6 to 8 residents per year. As a result, the diversity of implemented interventions and their efficacy may not be generalizable to other practice settings (eg, smaller programs with 2-3 residents per year). Implementation of wellness initiatives was not standardized possibly limiting generalizability. For example, it is challenging to ensure the quality of the supplementary teaching sessions are delivered uniformly, as these are provided on a volunteer basis by staff radiologists. In addition, not all the suggested wellness interventions could be fully implemented due to financial (ie, increased financial rewards) or logistical constraints (ie, organizational level changes). Future research could explore attendance rates for these initiatives, demographic differences (eg, residents with families), and the long-term effects of interventions on wellness and burnout.
Conclusion
Burnout is a multifaceted issue with profound implications on both healthcare professionals and the quality of patient care. Addressing burnout among radiology residents requires a comprehensive approach which considers the prevalence, contributing factors, and effectiveness of burnout interventions. Our study identified key factors contributing to burnout, including time, extra duties, and perceived radiology knowledge. Using a combined “top-down” and “bottom-up” approach, we implemented targeted interventions. Although, there were no overall significant differences in burnout and distress rates with the pre and post-intervention respondents, interventions addressing work hours were subjectively the most well received and effective in combating burnout.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was granted by the Department of Radiology at the University of British Columbia.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Chang is a recipient of a speaker honorarium at Bayer. Dr. Hague is a recipient of consultant fees for VIDA diagnostics and speaker honorarium and advisor fees for Boehringer Ingelheim. Dr. Yuen is the recipient of the Gordan E. Trueman Award for presenting this research. Drs. Chang, Joshi, Young-Spiers, and Yuen are members of the University of British Columbia Radiology Wellness Committee.