
Abstract
Purpose:
This study aimed to assess the experiences and challenges faced by Canadian radiologists participating in Multidisciplinary Team rounds (MDT), with a focus on demographics, meeting characteristics, preparation processes, and perceptions of workload and compensation.
Methods:
The Canadian Association of Radiologists constituted a working group which developed a 35-question survey that was distributed to 1958 radiologists and radiology trainees across Canada. The survey garnered 129 complete responses, for a response rate of 6.6%.
Results:
Respondents predominantly practiced in academic settings (65.9%) and had subspecialty training (96.1%). The majority reported that MDT rounds lasted 30 to 60 minutes and discussed 6 to 10 cases. Most radiologists (62.8%) were the sole presenters of imaging. Preparation time was often limited, with only 6.2% having dedicated time for preparation. 59.8% of respondents reported receiving additions to caseloads within the 24-hour period prior to the meetings. While 93.8% valued the opportunity for interaction with colleagues, 93.8% felt inadequately compensated for their efforts by their practices, while 92.3% felt inadequately compensated by their province.
Conclusions:
While most radiologists indicated adequate time for discussion and meaningful clinical engagement during rounds, many highlighted repeated challenges such as last-minute case additions, lack of protected preparation time, and technological barriers. Systemic barriers also play a role and include lack of provincial remuneration and workforce issues which in turn impact individual workload pressures.
Introduction
Multidisciplinary team (MDT) rounds are a cornerstone of modern healthcare, facilitating collaborative and evidence-based decision-making for complex cases across specialties. Radiologists play a pivotal role in these meetings, offering critical insights that influence management decisions based on imaging findings. In many jurisdictions, multidisciplinary discussion is mandated during cancer care management and has been shown to improve survival outcomes for lung,1-3 abdominal,4-6 and breast cancers.7,8 However, the demands of MDT participation, including case preparation, presentation, and discussion, can create a plethora of challenges for radiologists. In some jurisdictions, participation in MDT rounds is not remunerated, in spite of the significant workload associated with preparing for and presenting cases.9-11 The shift to virtual or hybrid meeting models, especially during and after the COVID-19 pandemic has both made it easier for some radiologists to participate in multidisciplinary collaborations, and increased the likelihood of technological challenges and frustrations. 12 To better understand the current nature of these challenges, the working group conducted a nationwide survey to evaluate the experiences and practices of radiologists involved in MDT rounds in Canada.
The survey targeted all practicing radiologists in Canada and was distributed through established communication channels and professional networks. It explored key themes, including demographic characteristics, workload, preparation time, case management, and the infrastructure supporting MDT rounds. Additional topics included radiologists’ perceptions of administrative burdens, external imaging integration, perceived individual value, and the overall quality of MDT discussions.
Methods
The Canadian Association of Radiologists MDT working group developed a survey based on their experiences with MDT rounds. All practicing radiologists in Canada were eligible, and consent was implied by survey completion. Per the standard Canadian Association of Radiologists (CAR) process for surveys of members related to practice patterns and quality assurance, institutional review board approval was waived.
The 35-question survey was available in English and French on SurveyMonkey (SVMK Inc.), ensuring anonymity and offering no financial incentives. The survey was distributed electronically through CAR communication channels and by personal outreach to the professional networks of the working group. It was open for response for 52 days. Targeting radiologists involved in multidisciplinary rounds, the survey reached 1958 potential respondents and garnered 129 complete responses (6.6% response rate). Notably, 304 unique complete response regarding rounds were obtained from the 129 survey respondents; the results provided in Tables 2 and 3 are based on 304 responses about individual rounds. Descriptive statistics were summarized, and data management was conducted using Excel for Windows.
Results
Demographics
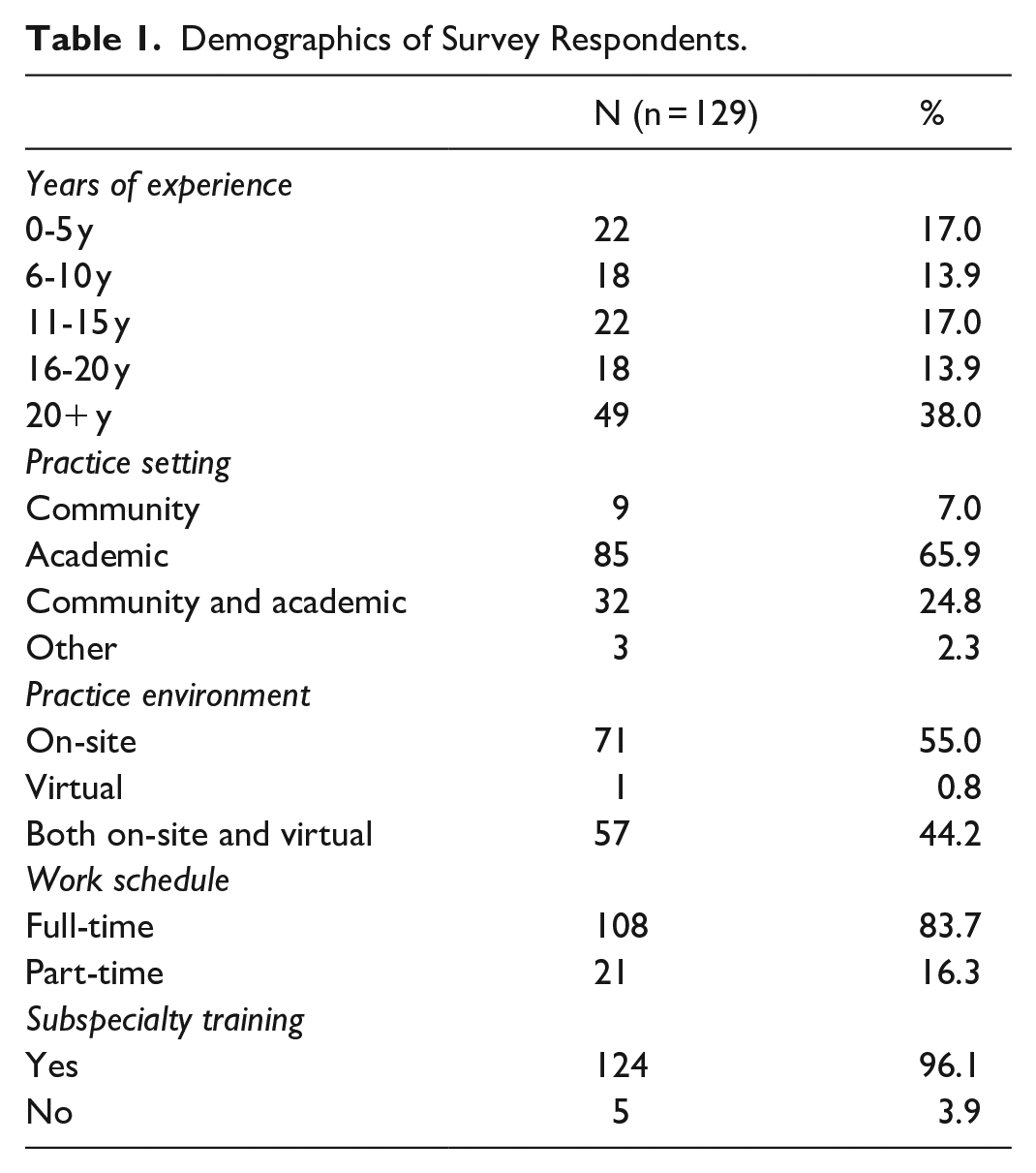
Nearly half of the respondents were from Ontario (49.6%, 64/129; Figure 1). The majority of survey respondents practiced at an academic institution (65.9%, 85/129), and had varying years of experience in practice (Table 1). Almost all respondents either practiced on-site or in a hybrid on-site/remote setting (99.2%, 128/129; Table 1). All but 5 respondents had subspecialty training (96.1%, 124/129) and most worked full-time (83.7%, 108/129; Table 1).
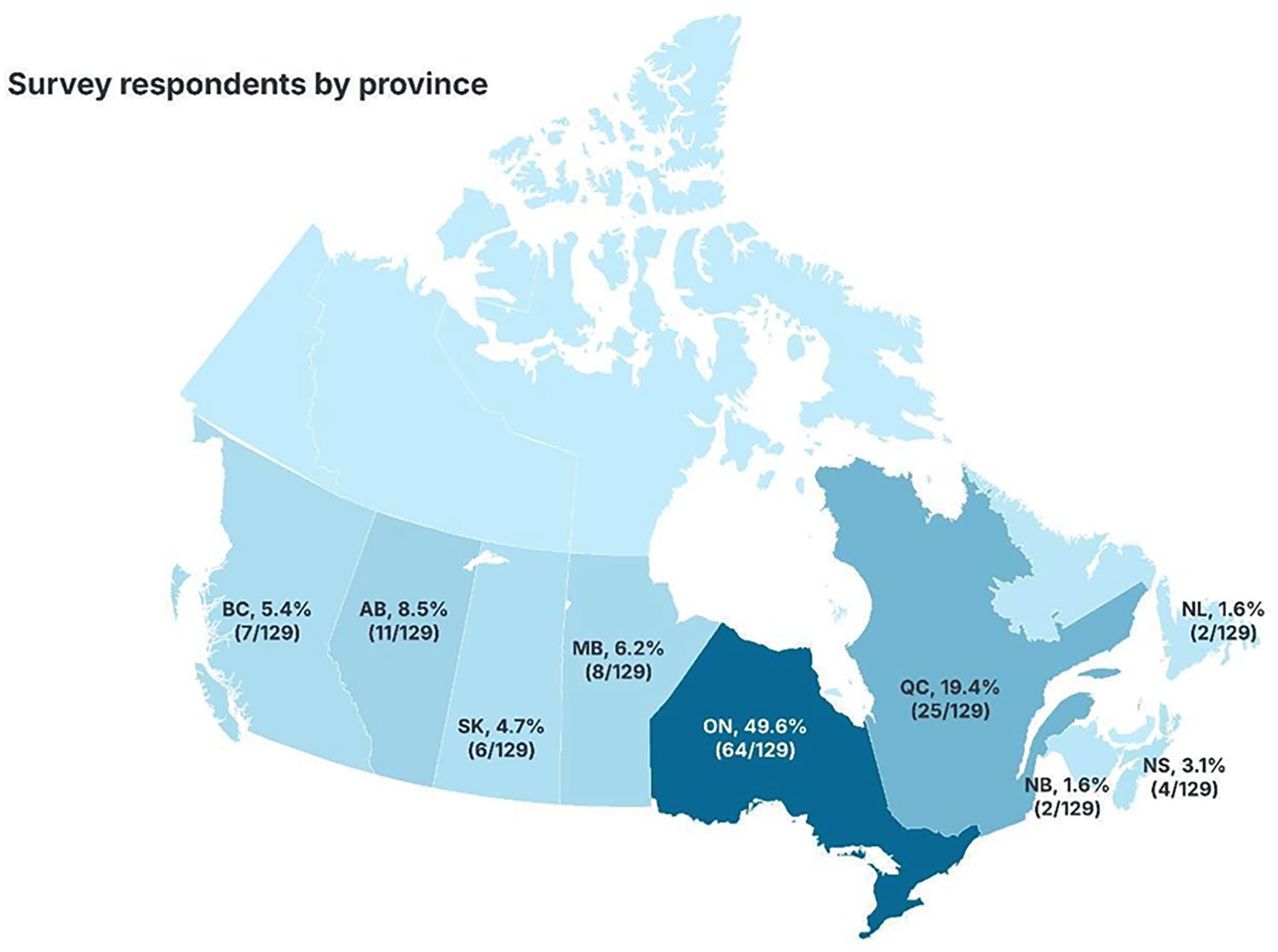
Respondent province of practice.
Demographics of Survey Respondents.
Characteristics of MDT Rounds
Content
The vast majority of the MDT rounds lasted between 30 and 60 minutes, with most discussing an average of 6 to 10 cases per round (Table 2). Most respondents indicated that more than half of their MDT rounds were oncological (83/129, 64.3%). Several respondents indicated they contribute to covering more than one type of MDT rounds at their institution, yielding 304 unique responses about individual rounds (Tables 2 and 3).
Distribution and Characteristics of MDT Meetings by Specialty.
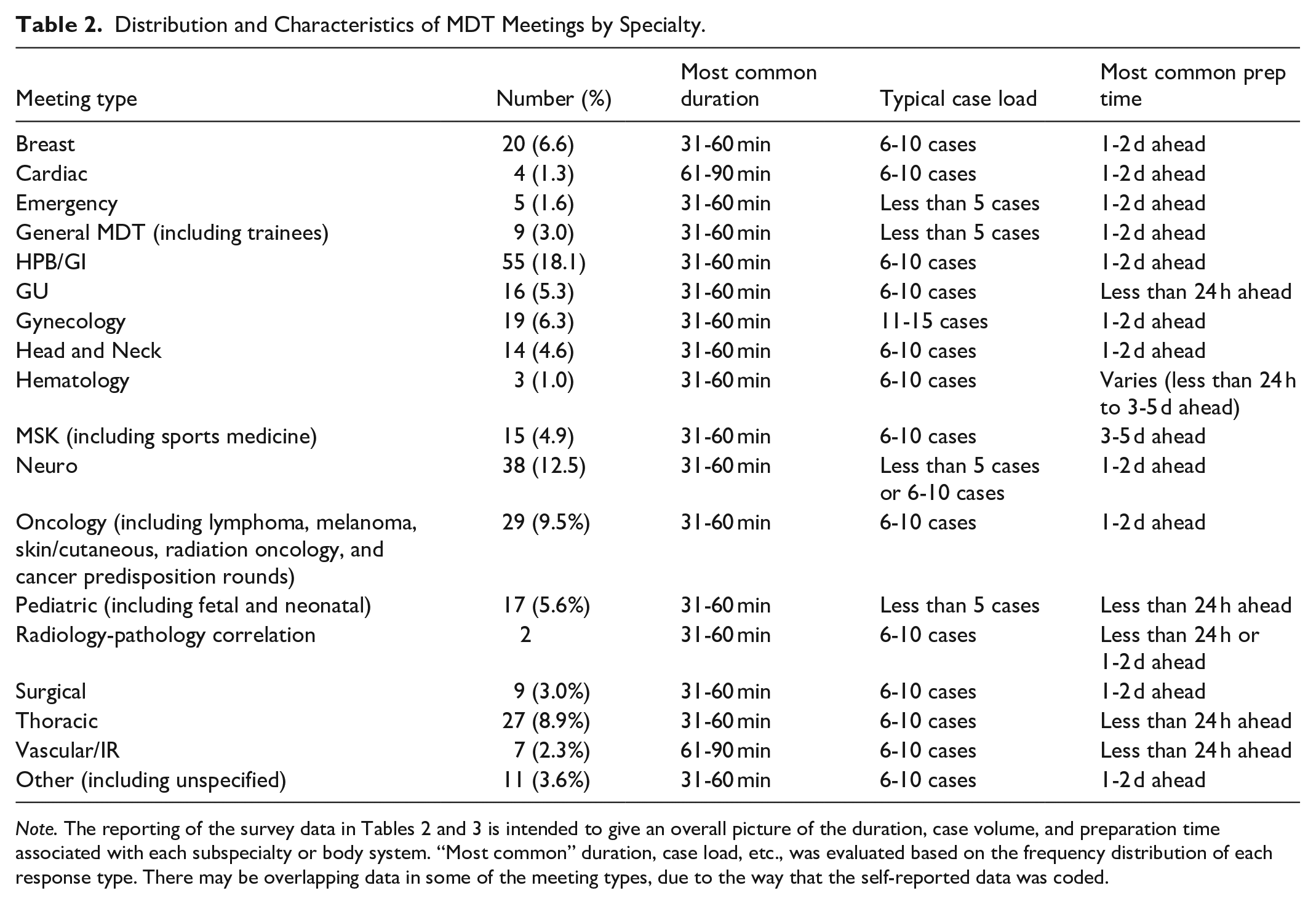
Note. The reporting of the survey data in Tables 2 and 3 is intended to give an overall picture of the duration, case volume, and preparation time associated with each subspecialty or body system. “Most common” duration, case load, etc., was evaluated based on the frequency distribution of each response type. There may be overlapping data in some of the meeting types, due to the way that the self-reported data was coded.
Overall Meeting Duration, Case Load, and Preparation Time.

Coverage and Preparation
The vast majority of respondents, a combined 62.8%, reported that they were the sole radiologist presenting the imaging the majority of the time (10.0% covering 51%-75%; 52.7% covering 76%-100%). In instances where the responding radiologist was not presenting the imaging, the majority of rounds were covered by radiology fellows or other sub-specialty trained radiologists from the same group or team.
Few respondents had protected time within their clinical or academic schedule to prepare for rounds (6.2%, 8/129), with most radiologists making time during their clinical schedule (44.7%, 58/129) or using their time outside of clinical hours to prepare (78.3%, 101/129). Free text comments revealed that some sub-specialty rounds have protected time, however, this is the exception.
In many rounds, cases were received either 3 to 5 days (38.8%, 50/129) or 1 to 2 days (41.1%, 53/129) before rounds. Only 2.3% get more than a week’s notice. However, in some instances (10.1%, 13/129), the cases were made available less than 24 hours prior to the MDT rounds.
Additionally, some institutions implemented cut-off times for adding extra cases: 22.4% (29/129) required a 24-hour notice, 13.2% (17/129) required 48 hours, 10.9% (14/129) required 72 hours, while 34.1% (44/129) had no cut-off time. However, the comments reveal that there is widespread non-compliance with cut-off policies.
Cases
Many respondents reported frequent add-on or urgent cases during rounds. Specifically, 40.3% indicated these occurred 0% to 25% of the time, while 29.5% noted a frequency of 26% to 50%. A smaller percentage experienced add-ons 51% to 75% (13.2%, 17/129) or 76% to 100% (17.05%, 22/129). A small majority of respondents (51.2%, 66/129) indicated that cases performed at another facility require a formal second read or dedicated consult. Free-text comments on the survey indicated that there is significant variability in local practices and expectations governing second reads; some institutions provide formal reviews/consults for all second opinions, while others focus solely on unreviewed studies due to backlog issues.
A total of 69.8% (90/192) and 16.3% (21/129) reported receiving requests to remove or substitute cases within 24 hours from rounds in 0% to 25% to 26% to 50% of the time respectively. These requests were primarily for last-minute additions of substitute cases, with reductions in overall case volumes being rare.
Respondents reported widespread issues related to the clarity of the radiological discussion questions and the sufficiency of clinical information required to prepare for rounds. The majority of respondents (42.6%, 55/129) indicated that the discussion and clinical questions were clear, while 24.8% (32/129) thought they were clear 51% to 75% of the time. Many radiologists expressed that presentations often lack specific target questions, making it challenging to prepare. In fact, over half (54.2%) were unsure which radiological study the discussion pertained to, leading to a need for comprehensive reviews of all relevant imaging, including screening, diagnostic, and staging tests.
Most respondents (55.0%, 71/129) felt they received sufficient clinical information to prepare for rounds. However, several noted the time spent searching electronic records for accurate details, highlighting inconsistencies in information availability across clinical teams. Most respondents (91.4%, 118/129) reported that repeat imaging due to quality or timing issues was needed in fewer than 50% of cases, indicating that such issues rarely necessitate repeat imaging in the majority of cases reviewed.
Infrastructure
The data shows that most radiologists review some external cases (from other facilities, hospital systems, cities, or provinces), but the proportion varies significantly. The largest segment of respondents (36.4%) reviews a relatively small proportion (0%-25%) of external cases, and a substantial group (31.0%) reviews between 26% and 50% of external cases. About a quarter of respondents (22.5%) reviews a majority (51%-75%) of external cases.
Just over half (51.2%) of facilities require a formal second read or dedicated consult for external cases, indicating a significant additional workload. The majority (68.2%) import external studies directly into their PACS system. A smaller portion (12.4%) use external repositories, while 17.1% use other unspecified methods.
Support staff handle the bulk of retrieving duties (83.7%), which can optimize the radiologist’s workflow. A small percentage of radiologists (15.5%) handle their own importing; very few cases are handled by technologists (3.1%) or fellows (1.6%).
Only 23.3% report that external repository access is as good as their local PACS, and half (50.4%) of respondents indicated inferior performance of the external systems. About a quarter (26.4%) marked this as not applicable, likely corresponding to those who import directly to PACS.
Administration and Time
Most MDT rounds are scheduled during clinical hours (68.2%, 88/129), with the second most common time being before clinical hours (44.2%, 57/129), and a relatively even split between lunch hours (36.4%, 47/129) and after-hours (33.3%, 43/129) scheduling. Comments reveal that some institutions use early morning slots in an effort to minimize disruption to clinical work, since there is a perception that rounds occurring later in the day have more of a disruptive impact.
Most respondents (82.9%, 107/129) reported that their rounds were virtual or hybrid, with only 9.3% (12/129) reporting that their rounds take place in person. More than one quarter of respondents (27.1%) would prefer in-person rounds, but individual commenters acknowledged that the logistics of multi-site teams and scheduling conflicts make hybrid or virtual platforms the more effective option.
The majority (59.7%, 77/129) reported having adequate time for discussion during MDT 76% to 100% of the time, and about a fifth (18.6%, 24/129) had adequate time 51% to 75% of the time.
Remuneration and Perceptions
Of the 129 respondents, over 83% (108/129) felt that their MDT-specific workload was increasing over time. A smaller minority (1.5%) and (14.7%) respectively felt it had diminished or stayed the same compared to their past experience participating in MDT rounds. We did not delve further to investigate why, in some instances, the workload was perceived as being static.
In terms of incentives to continue commitment to MDT rounds, the vast majority of respondents valued the opportunity to interact with their clinical colleagues (93.8%) and also maximized the ability to get feedback on cases (64.3%) whilst being opportunistic about potential research and other collaborations (64.3%; Figure 2). Approximately half of the respondents felt MDTs provided validation from colleagues, as well as contributions to continuing medical education (CME) credits for the Royal College of Physicians and Surgeons of Canada Maintenance of Certification (MOC) program (55.8% and 51.1% respectively). A similar number of individuals felt it was an obligatory responsibility of their job description (48.8%). A much smaller group of individuals cited revenue to their practice (18.6%) and other reasons (3.8%) as reasons for their participation.
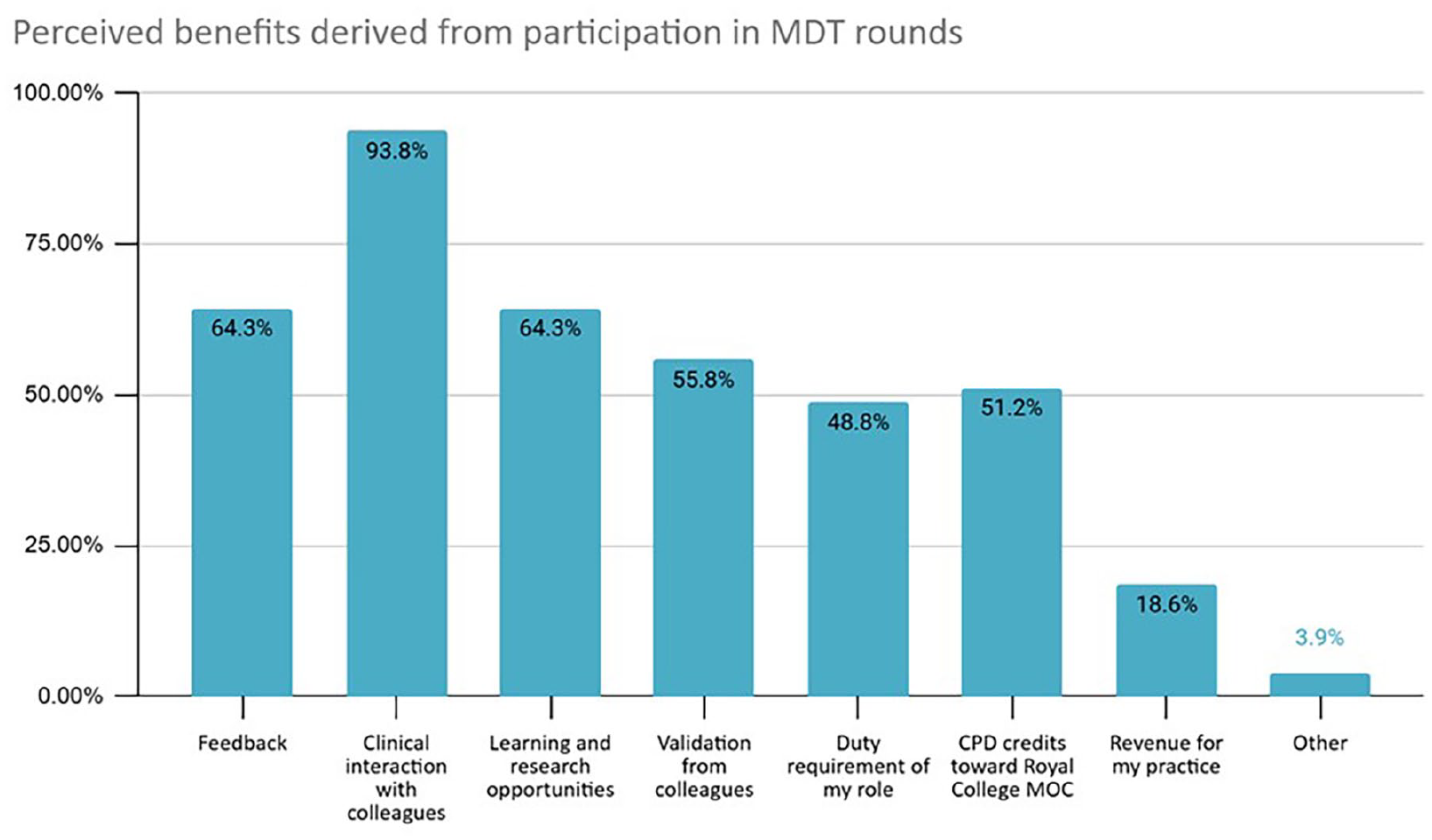
Perceived benefits derived from participation in MDT rounds.
The majority of individuals felt that rounds were not adequately compensated (monetary or time) either in their practice (93.8%) or in their province (92.2%). In 46.5% of cases, there was no compensation at all. In the remaining instances, compensation was via a fee code (23.2%), via the individual practice plan (18.6%) or some other unstipulated means (24%; Figure 3).
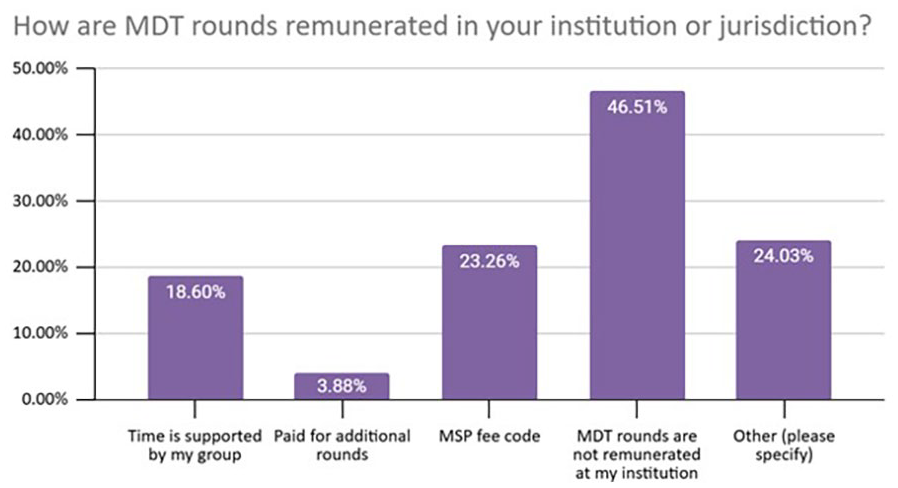
Remuneration methods.
Discussion
Our findings illustrate that the scope of pathologies discussed in MDT rounds across Canada extends well beyond oncology, reflecting the broad clinical relevance of these meetings. This trend has also been observed in the published literature, much of which is also survey-based and reflects perspectives from other national contexts.10,13,14,15,16-19 Variability in case volume and pace suggests that the structure of MDT rounds is influenced by both clinical urgency and the nature of the cases presented. Prior studies have highlighted that the burden of MDT participation often falls disproportionately on radiologists compared to other specialists, particularly in oncological settings.20,21 Radiologists play a critical role by providing expert imaging interpretation that directly informs management decisions.22-25
While most MDT rounds are covered by subspecialty-trained radiologists, trainees may also be involved. Some academic centers offering valuable learning opportunities under staff supervision, especially for radiology fellows. While beneficial for training,26,27 this can increase the time commitment required from supervising radiologists.
Radiologists expressed several frustrations related to preparation and workflow. The timing of case list distribution often forces radiologists to prepare during evenings or weekends, sometimes while on call. This practice not only disrupts work-life balance but also reflects a disconnect between institutional policies and actual practice. Moreover, the time commitment required for MDT participation is substantial. Kane et al report that radiologists spend approximately 20% of their time on MDT-related activities, underscoring the significant workload involved. 28 Many of our survey respondents reported a lack of protected time for preparation, further exacerbating the challenge of delivering high-quality reporting and analysis under time constraints.
Communication challenges were a recurring theme in our findings. More than half of respondents reported unclear clinical questions, and many were uncertain about which imaging studies were relevant. Although most felt they received adequate clinical information overall, the time spent searching for key details highlights inefficiencies in information sharing. Other surveys have similarly found that radiologists are not always provided with sufficient clinical information prior to MDT rounds, and that the non-attendance of referring clinicians can further hinder effective discussion. 15 In line with our findings, a recent Canadian study by Elias et al examining MDT communication between radiologists and referring physicians identified the lack of a clearly defined clinical question as a key area for improvement. They emphasized the value of establishing guidelines on the type and amount of clinical information needed to support radiologists in preparing for MDT rounds. 17 These findings underscore the need for better integration of clinical systems and more consistent, structured communication practices.
Second opinion requests vary in intent and frequency from institution to institution. In many instances a formal second opinion is being requested by a sub-specialty trained radiologist prior to an MDT rounds discussion. The purpose is two-fold: first, to document a formal report in the clinical record and second, to obtain a review by a radiologist more versed with the nuance needed to inform decision making. The availability of a report from a primary read varies and in some cases the study in question may be unread (due to departmental backlogs). In either circumstance, this adds to the overall workload and expectation of the reviewing radiologist. Although renumeration is not the only acknowledgment of time and effort spent it is universally modest for second opinion reads and may therefore be viewed as a less desirable commodity.
The frequent demand for second opinions and urgent case reviews underscores the critical role radiologists play in clinical decision-making but raises questions about the efficiency of pre-meeting planning and case triage by clinical colleagues. Administrative challenges further strain radiologists’ capacity and highlight the need for streamlined processes and clearer expectations. By addressing the frustrations linked to abrupt changes and unclear expectations, departments can foster a more supportive work environment, ultimately benefiting both radiologists and the clinical teams they support.
Reviewing external imaging studies from outside the radiologists’ primary hospital or work environment is a routine part of MDT participation,28,15,29 though our survey found that it typically accounts for less than half of the cases. However, these cases often require additional effort due to limited access to prior imaging or clinical context, and reliance on support staff to address technological barriers can hinder efficiency. Although repeat imaging due to quality or timing issues is uncommon, there remains room for improvement in standardizing imaging protocols and enhancing inter-facility communication.
Despite survey data suggesting that adequate time is scheduled for MDT rounds, free-text comments reveal that meetings often run over time, and cases may be deferred or re-reviewed by different radiologists. High case volumes and insufficient preparation by presenting clinicians can compromise the quality of discussions. Some respondents noted that discussions occasionally become overly academic, detracting from their clinical utility. These findings suggest that while time allocation may appear sufficient on paper, its actual use and structure warrant closer examination.
Finally, perceptions of workload and compensation reveal a significant disconnect between the acknowledged value of MDT rounds and the reimbursement for radiologists. Radiologist participation in MDTs is associated with substantial unreimbursed time and costs.10,17,29,30 Nearly half of our respondents work in environments without a provincial fee code to support this work, despite clinical guidelines emphasizing the importance of multidisciplinary consensus in managing complex cases. This disparity highlights the need for advocacy and systemic changes to align expectations with appropriate recognition and support.
Conclusion
This survey provides an overview of the experiences and challenges faced by Canadian radiologists participating in MDT rounds. While MDTs are essential for collaborative patient care, radiologists reported difficulties such as inadequate preparation time, last-minute case additions, unclear clinical questions, and barriers to external imaging integration. Despite these challenges, most respondents valued the clinical importance of MDT participation and acknowledged adequate time for discussion in most cases. Our survey emphasizes the integral role that radiologists play in the triage and management of patients most notably in the setting of oncological pathology and complex disease processes. It is one service commitment which consistently emphasizes our patient facing role.
The results underscore the need for systemic improvements, including better adherence to case submission deadlines, enhanced integration of external imaging systems, and the provision of protected time for preparation. Addressing these issues will help optimize radiologists’ contributions to MDTs and improve overall efficiency.
A follow-up position statement paper could delve deeper into these findings and offer specific recommendations to support radiologists and enhance the effectiveness of MDT rounds.
Footnotes
Acknowledgements
The authors gratefully acknowledge the members of the Canadian Association of Radiologists MDT Working Group: Drs. Cameron Hague, Elsie Nguyen, Emil Lee, Carolyn Flegg, and Adnan Sheikh for their contributions to the development of the survey questions and for their thoughtful participation in discussions that informed the analysis and interpretation of the results.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.