
Abstract
Waiting times for medical imaging examinations in Canada are growing as the demand for these tests exceeds current capacity. This document summarizes strategies that may be employed to increase medical imaging patient throughput in an environment of limited resources. This document also advocates for provincial measures to optimize use of resources and national policies that support sustainable radiology services to meet growing demand now and in the future.
Background
Waiting times for medical imaging examinations in Canada are growing as the demand for these tests exceeds current capacity.
This document has been created to summarize strategies that may be employed to increase medical imaging patient throughput in an environment of limited resources. Some strategies are applicable at the level of individual institutions or departments. This document also advocates for provincial measures to optimize use of resources and national policies that support sustainable radiology services to meet growing demand now and in the future.
The authors conducted a review of published literature as well as practices at our own institution, in addition to reaching out to academic and community radiologists who are board members of the Canadian Association of Radiologist. We acknowledge differences between institutions and the needs of the populations which they serve. Report turnaround time is another major component of radiology which is not discussed in this summary.
Budget and funding is province-specific and also falls beyond the scope of this summary, however many strategies discussed may lead to reduced healthcare costs, such as minimizing duplicate or low value studies. Reducing imaging wait-times reduces delay to diagnosis, in turn potentially reducing the costs associated with treating more advanced or complicated disease.
Strategies to decrease waiting times and improve the match between demand and supply can be considered in 4 approaches (Figure 1):
Increasing capacity
Increasing efficiency
Reducing demand
Prioritizing capacity
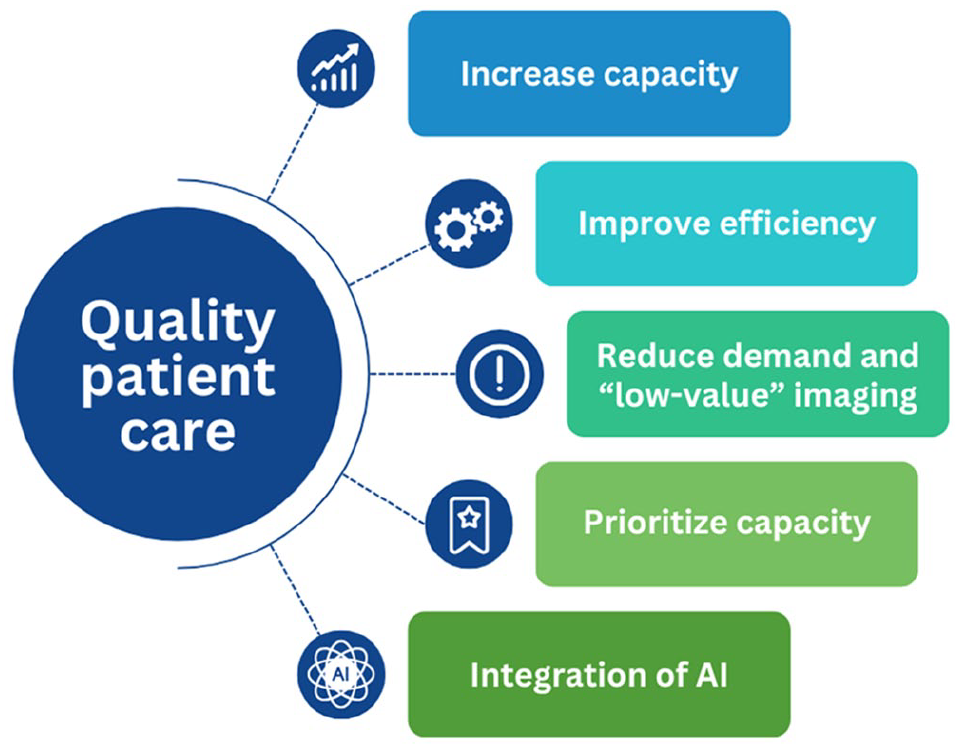
Strategies to increase throughput.
Increasing Capacity
Increasing the overall capacity of radiology departments nationwide is the long-term solution to be able to meet increasing demand. This requires increasing both workforce and infrastructure.
Strategies to increase capacity:
• Increasing the radiology workforce
• Upskilling of existing workforce
• Increasing non-medical support staff
• Increasing and updating infrastructure
• Extending hours of operation
Increasing the Radiology Workforce
Currently there are shortages throughout Canada of trained staff required to operate a radiology department including medical imaging technologists, nurses and radiologists. Recruiting more personnel will be necessary to meet demand long-term, however it is acknowledged that it may be challenging for sites to recruit employees even if funding for positions is available. The increasing demand for diagnostic and interventional radiology highlights a need for long-term workforce planning in these fields, including increasing:
- Full-time equivalent (FTE) positions for technologists, nurses and radiologists at both hospitals and community radiology practices
- College and university and post-graduate training positions for technologists and nurses
- Residency positions for training radiologists
- International recruitment for all health human resources related to radiology
- Upskilling opportunities for existing staff
Increasing international recruitment may be facilitated by streamlining pathways for recognition of international qualifications that are comparable to Canadian qualifications. This is medium-term strategy that highlights the importance of advocacy and funding for radiology workforce planning.
Strategies for increasing workforce should be considered alongside short-term plans for sustainable workforce retention 1 as part of wider workforce planning.
Upskilling
Providing upskilling opportunities for existing workforce to increase their skill mix can allow greater scheduling flexibility to help meet areas of peak demand with the existing workforce, including mobility across multiple sites for multi-site health networks. 1 For medical imaging technologists, this could mean upskilling to be able to work in multiple modalities. In some settings, ultrasound technologists have been upskilled to be able to perform certain procedures such as thyroid nodule fine needle aspiration (FNA) to improve access whilst maintaining or improving diagnostic yield.2,3 Establishing upskilling pathways and supporting the ongoing professional development of the existing workforce is fundamental to sustainably increasing the capacity to train future HHR, for example, increasing future technologist training positions.
Non-Medical Workforce
Consider leveraging non-medical workforce by delegating as many tasks as possible to non-medical support staff to increase the efficiency of technologists.1,4,5 Recruiting more non-medical personnel may be more feasible in the short term than recruiting health professionals in the context of health workforce shortages. This would allow technologists to spend more time performing scans. Positions that could be increased include administrative/clerical support roles and patient transportation personnel.
Imaging Assistants
Many centres now utilize imaging assistants who are trained to perform tasks that are usually performed by the technologist, but which do not require specialized technologist training such as:
- Preparing the patient for the study (changing clothes, storing belongings, supervise oral contrast, assist with or perform IV cannulation, direct patient to scan area, etc.)
- Transferring patients on and off the scanner
- Taking phone calls and co-ordinating patient logistics
- Patient transport from Emergency or inpatient wards to reduce delays and time when the scanner is held empty
- Room preparation and restocking supplies
- Chaperone during intimate examinations
- Assisting with documentation
Co-ordinating patient logistics can reduce the time burden on technologists for complex cases that may require multiple clinical teams or anaesthesia. Imaging assistants have the potential to enhance workflow for technologists and radiologists, particularly in the setting of skills shortages where hiring more technologists and nurses may be challenging.
Adequate staffing not only increases scanning throughput but is also beneficial for the patient experience. 4
Increasing and Improving Existing Infrastructure
Increasing infrastructure, including the number of available scanners, should be part of a long-term strategy to meet increasing demand.
Replacing old scanners with new models that have a shorter exam time and improved functionality such as faster reconstruction of multiplanar reformats also increases capacity.
Robust networks and RIS/PACS systems are integral to the management of patients’ radiology data. Maintenance and upgrades are required to accommodate a higher volume of scans and to avoid significant outages and downtime which cause delays.
Scheduling templates should be updated, particularly for MRI, to allow increased scheduling throughput when implementing ultrafast MRI protocols.
Extend Operating Hours
Increasing operating hours maximizes the capacity of existing infrastructure.4,5 Many Canadian institutions already utilize after-hours and weekend lists, however there is variability across organizations. 6 Demand for both inpatient and outpatient scanning may extend into “out-of-hours” periods: increasing capacity during these periods may improve efficiency by creating a better match between services and demand. 4
Temporarily increasing operating hours for busy periods in the calendar year and running a “scanning blitz” can also improve patient access, for example, before holiday seasons. Reviewing demand fluctuation at an institution will determine the optimal time to run a “blitz” and these should also be co-ordinated with radiologist reporting schedules in advance. Additional or enhanced remuneration for technologists and radiologists for additional work during “blitz” periods should be offered to make this a sustainable and appealing short-to-medium term strategy to reduce imaging wait times.
Increasing Efficiency
Strategies to increase efficiency:
• Using abbreviated imaging protocols
• Standardization of protocols
• Scheduling similar studies together
• Modality substitution from high to lower demand modalities (when clinically appropriate)
• Centralized requesting and booking systems
• Centralized PACS and electronic medical records
• Minimize disruption from equipment maintenance
• Remote imaging for technologists
Strategies that improve efficiency allow more examinations to be performed with the existing number of scanners and workforce.
Abbreviating Protocols
Performing protocols with the minimum number of sequences or images required for accurate diagnosis reduces scan time as well as time required for reporting and data storage requirement. There is also less risk of movement artefact from patients having to remain still for long periods of time. 5 Use of abbreviated protocols generally has the most significant impact for MRI studies 5 but can also improve throughput in CT. Establishing standardized indications for abbreviated protocols allows them to be employed as frequently as possible (eg, screening, surveillance or to answer a specific clinical question).
Minimizing the use of oral and IV contrast reduces the total time per patient. With current CT technology, the limited benefit of oral contrast should be considered against the increased time and cost, as well as patient discomfort, in both the acute7,8 and elective setting. 9 The addition of IV contrast adds significant time to MRI studies and to a lesser extent, CT studies, and the added diagnostic value should be considered. Rationalizing the use of contrast agents also reduces the environmental footprint of medical imaging. 10
Standardization of Protocols
Having a limited number of standardized protocols to choose from allows technologists to be more efficient and familiar with each protocol, while also providing high quality imaging for the requested clinical indications. 5
Scheduling Similar Studies Together
Larger organizations may be able to facilitate “batch booking,” where similar study types or diseases are booked together in a “scheduling block.” This allows the technologist to repeat standardized protocols 4 and minimize delays associated with changing equipment set ups such as MRI coils or a contrast agent. This potentially improves efficiency and reduces error compared with technologists having to accommodate a mix of diseases, anatomic sites and imaging protocols.
Modality Substitution
For some clinical indications, it may be appropriate to substitute a different imaging modality that has a shorter wait-time (eg, from MRI to CT or US). “Opting in” to possible modality substitution could be an option on electronic requesting to allow radiologists discretion during protocolling of imaging requests, to minimize wait-times for the patient.
Centralized Requesting and Booking
Centralized intake models offer a significant opportunity for radiology waitlist smoothing as well as reduction of duplicate imaging. 11 Centralized intake models have positive benefits for surgical wait-times12,13 and there is the potential for similar or greater improvement in radiology. Health equity issues need to be taken into account to ensure patients involved have access to transportation when asked to be imaged at an area that is geographically further away.
Centralized PACS and Electronic Medical Records
Investment in centralized province-wide PACS and electronic medical record (EMR) systems has the potential to greatly improve efficiency in medical imaging as well throughout the entire patient healthcare pathway. Province-wide EMR has been adopted in Alberta and other provinces are beginning pilot programs for centralized systems. A centralized EMR can facilitate a province-wide radiology repository that allow access to studies and reports performed at other institutions, as an alternative strategy to having a province-wide PACS. Specific to medical imaging, centralized PACS or radiology image repository reduces the need for repeat studies due to referrers not being aware of or not being able to view prior examinations. There is also added value for technologists and radiologists who can reference prior studies performed at other sites. Integration with centralized EMR can allow efficient cross-referencing of patient information such as allergy histories and relevant laboratory data to make pre-procedure preparation faster and more accurate. Centralized PACS and EMR systems can better facilitate centralized requesting systems and integration of clinical decision-making tools.
Equipment Maintenance
Regular servicing of scanners is essential for maintaining performance. Optimally, scheduled downtime should occur during lowest activity periods to minimize disruption to overall operations and reduce impact on wait-times.
Remote Imaging
Remote scanning is an evolving technology that may allow patients to undergo complex studies such as MRI in areas which have a shortage of skilled technologists. 14 This technology allows a CT or MRI technologist to operate one or more machines remotely. There is onsite support from a technologist-assistant to get patients changed, help them on and off the imaging couch, position the patient and place any necessary intravenous lines. There is additionally the potential for remote ultrasound imaging to improve access in remote areas. Telerobotic ultrasound allows a technologist or radiologist to manipulate the ultrasound probe remotely, with a patient assistant on site. 15 Tele-ultrasound is another remote imaging strategy in which a local healthcare provider with basic ultrasound training, such as a nurse or technician, performs the ultrasound with or without real time expert guidance. There is the potential for applications in general 16 and obstetrical ultrasound. 17
Remote imaging may address skill shortages in smaller and remote centres within Canada to improve equity of access to healthcare. Remote scanning may also provide more flexible working options for technologists which may allow greater workforce participation and reduce some aspects of workplace commuting in urban centres.
Reducing Demand
Strategies to reduce demand:
• Automated flagging of duplicate orders
• Automated flagging of similar orders that may be combined
• Integrated clinical decision support tools
• Collaborative planning with referrers around future demand
Reducing Demand in the Short-Term
The reasons for increasing demand for medical imaging are multi-factorial and are part of the evolving practice of medicine.
Changing the ordering practices of clinicians is generally a long-term strategy. In the short- to intermediate-term, some low-value investigations that could be reduced include:
- Duplicate orders for the same test, which may be requested by different physicians seeing the patient at different visits
- Interrogating other hospital databases for duplicate orders for the same test in different geographic locations
- Orders for more than one modality answering the same clinical question (eg, requesting both a CT and an ultrasound to assess the same organ)
- Combining bookings for the same modality where appropriate. For example, an order for a renal tract US from one physician could be combined with a separate order for a pelvic US from a different physician in the same ultrasound appointment rather being scheduled as different appointments on 2 different days
Reducing Low-Value Radiology
There are numerous guidelines addressing the issue of evidence-based appropriate imaging, including the best type of imaging and timing depending on the clinical context. The Canadian Association of Radiologists (CAR) has evidence-based practice guidelines for a wide variety of clinical scenarios. 18 Appropriate imaging is a complex area which involves ethical decisions around how to use resources balanced with the potential risk or benefit to patients. Variation exists between guidelines, commonly due to regional differences.
In general, radiology positively contributes to patient diagnosis and ongoing care. 19 Ideally, the appropriate use of imaging would:
- Minimize time to accurate diagnosis
- Minimize cost to patients and the healthcare system
- Avoid harm associated with incorrect diagnosis or incidental findings that require subsequent investigation
- Minimize harm to the patient from the imaging test (eg, exposure to ionizing radiation or contrast agents)
Low-value imaging adds little to no value to patient management; despite this, it is a growing source of healthcare costs in Canada. 11
Even when evidence-based guidelines are available, there are many reasons why clinicians may request tests outside recommendations, for example:
- Not aware of guidelines
- Guidelines too difficult to look up in a time-pressured clinical scenario
- Recommended test is not locally available or wait-time is too long 20
- Expectations of patients to have an imaging test, even when one is not recommended 20
- Patient may have concurrent medical conditions which require imaging outside of standard guidelines
Although changing practice around use of imaging is complex, striving toward the most appropriate use of imaging not only improves use of resources but is also beneficial for the patient.
Radiology departments can address the burden of low-value imaging requests by:
- Working cohesively with requesting departments 19
- Establishing standardized imaging pathways in conjunction with relevant clinical departments to reduce low-value imaging
- Integrating clinical decision support tools into electronic requesting platforms, 11 including requesting platforms for family physicians and nurse practitioners
Collaborative Planning With Referrers
Having a collaborative working relationship with referrers provides an opportunity to jointly decide how best to allocate radiology resources to meet different clinical needs. Open channels of communication allow departments to understand each other’s constraints and how they may both optimize their limited resources to accommodate one another. For example, in our institution, an audit of CTs performed in the emergency department for pancreatitis allowed for discussion of current imaging guidelines. The discussion highlighted that pressure for imaging was commonly driven by admitting clinical teams and prompted the radiology department to engage with these additional medical and surgical teams through educational rounds. Regular scheduled interdepartmental meetings or rounds may provide a platform for ongoing feedback. In our institution, a regular interdepartmental meeting provided the opportunity to discuss planned changes to Emergency Department staffing. Our department adjusted the start time of early reporting radiologists and increased the number of radiologists working at different times in the early morning, daytime and evening, in anticipation of the planned change which now allows faster turnaround time of radiology reports at times of high emergency department activity.
Collaborative planning around new services such as new screening programs, new cancer therapies and new surgical programs, allows joint advocacy and planning. This should include both radiology and pathology, to allow for appropriate level of support and staffing for anticipated increases in demand, and to ensure successful implementation.
Prioritizing Capacity
Strategies to prioritize capacity:
• Align workforce scheduling with demand
• Separating inpatient and outpatient workflows
• Paperless referral management systems for optimized scheduling
• Fit-for-purpose triage systems
Aligning Scheduling With Demand
Reviewing demand levels and redistributing technologist rosters accordingly maximizes the efficiency of the technologist workforce. 4 In some scenarios, this could mean adding additional technologists to busy periods, however the added cost would be balanced by improved efficiency, quality, safety and patient satisfaction. 4 This would include consideration of extending after-hours and weekend operations for outpatient services at sites not already doing so. 5
Separating Inpatient and Outpatient Studies
Inpatient and outpatient workflows have distinctly different requirements and combining the 2 can be disruptive. 5 Where possible, designating inpatients and outpatients to different scanners can improve the efficiency of both workflows, as well as providing a better experience for patients in both settings. Some provinces already operate dedicated outpatient-only imaging services which provide highly efficient services for ambulatory outpatients.
Paperless Referral Management and Scheduling
Fully digital, paperless referral systems allow for more efficient handling and triage of referrals, including “flagging” of duplicate requests, minimizing lost paper requests, managing allergies and co-ordination with other appointments or investigations. In 2014, fully paperless requesting occurred in a minority of Canadian academic institutions, 6 a proportion which has likely now significantly increased. Conversion from paper-based to digital requesting was a key strategy in clearing excessive colonoscopy waitlists in an Australian hospital by improving booking efficiency. 21 With electronic medical records now the norm, integration of systems to alert technologists and bookings staff of any contraindications to diagnostic or interventional radiology procedures allows efficient preparation of the patient both prior to and upon arrival. 4 Electronic scheduling systems should also facilitate automated outpatient appointment reminders and confirmation, freeing clerical staff to manage non-routine issues. Booking templates should be flexible to accommodate different durations of scans so that short examinations are not booked for an excessive time slot. Ideally, patients should have access to the booking templates to allow self-booking where possible, similar to other industries such as the airline industry.
Optimizing Triage
There is variation between the triage systems used between Canadian institutions for booking of imaging requests. A universal triage system may better guide clinicians with diverse experiences and levels of expertise. 6 In addition, having a common triaging system can allow more direct comparison of wait-times across different geographic areas and across provinces to allow for better distribution of healthcare funding to areas with increased demand.
Whichever current triage categories are used by an institution, they should meet the needs of the institution and its referrers. Incorporating specific time periods (eg, “within 10 days”) may be more helpful than just descriptors such as “urgent” or “semi-urgent.” In general, most Canadian academic institutions do not meet all of their wait-time targets. 6 If actual wait-times significantly differ from the expected triage categories, revising triage categories may prevent a “priority creep” from referrers requesting a more urgent timeframe than they actually require. In addition, having publicly available wait-times posted in different institutions allows for increased transparency and may encourage patients to schedule their imaging exams in areas that have shorter wait-times, when feasible. 22 A clear system allows appropriate requesting by referrers and exam prioritization and protocolling.
Artificial Intelligence (AI)
There is a growing number of potential applications of AI along a patient’s medical imaging pathway that can reduce the time taken for tasks or reduce the number of personnel required in resource-limited environments. Assigning protocols to studies is usually a duty of the radiologist which can take away time from diagnostic interpretation. 23 There is the potential for this to be partly or fully performed by AI and natural language processing models have shown potential for protocolling brain 24 and musculoskeletal MRIs. 25 AI also has the potential to identify patients who will develop severe or critical outcomes based on information in electronic medical records. 26 This information could be used triage imaging studies to prioritize certain patients for urgent imaging. 23 Use of deep learning reconstruction techniques such as Siemen’s Deep Resolve and GE’s AIR™ Recon DL has been found to reduce exam time without compromising image quality and diagnostic confidence.27,28 Use of AI-based worklist reprioritization applications may reduce report turnaround times for studies with critical findings such as CT pulmonary angiogram.29,30 Cost may be a limiting factor for centres to invest in AI applications, which may include the cost of upgrading infrastructure or systems to facilitate an AI application. The concern of ongoing validation of AI solutions in the Canadian health care environment may also be a limiting factor for adoption of AI in imaging. For centres that can facilitate the use of AI, applications can potentially assist with (Figure 2):
- Scheduling of diagnostic and interventional imaging, including patient reminders
- Radiology department staff scheduling
- Automated or semi-automated protocolling of imaging requests
- Triaging of studies to be performed
- Identifying duplicate orders
- Reducing image acquisition time (CT and MRI)
- Image reconstruction and post-processing
- Prioritizing studies for timely reporting
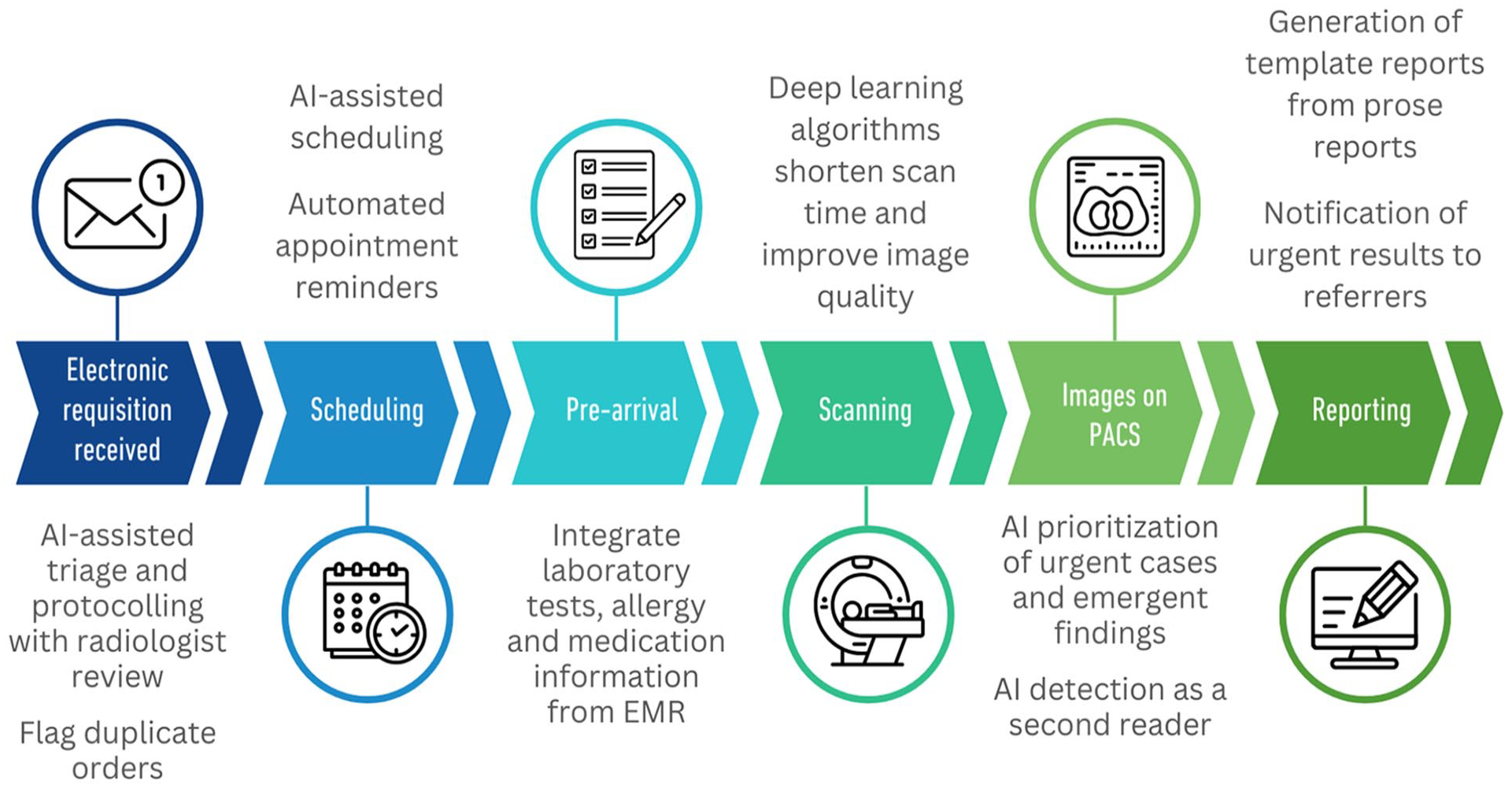
Potential roles of AI in the radiology patient journey.
Conclusion
Medical imaging wait-times are an increasing issue throughout Canadian academic and community radiology centres, with the potential to compromise patient outcomes. Medical imaging is an increasing contributor in patient care pathways. Individual centres should implement strategies to optimize use of their existing infrastructure and workforce in the short-term. These efforts should ideally be led collaboratively by radiology physician leaders, administrative teams and referring clinicians. In parallel, broader co-ordination with provincial health authorities and the Ministry of Health is essential to align local initiatives with system-wide policies, funding models and regulatory frameworks to ensure sustainable impact (Figure 3).
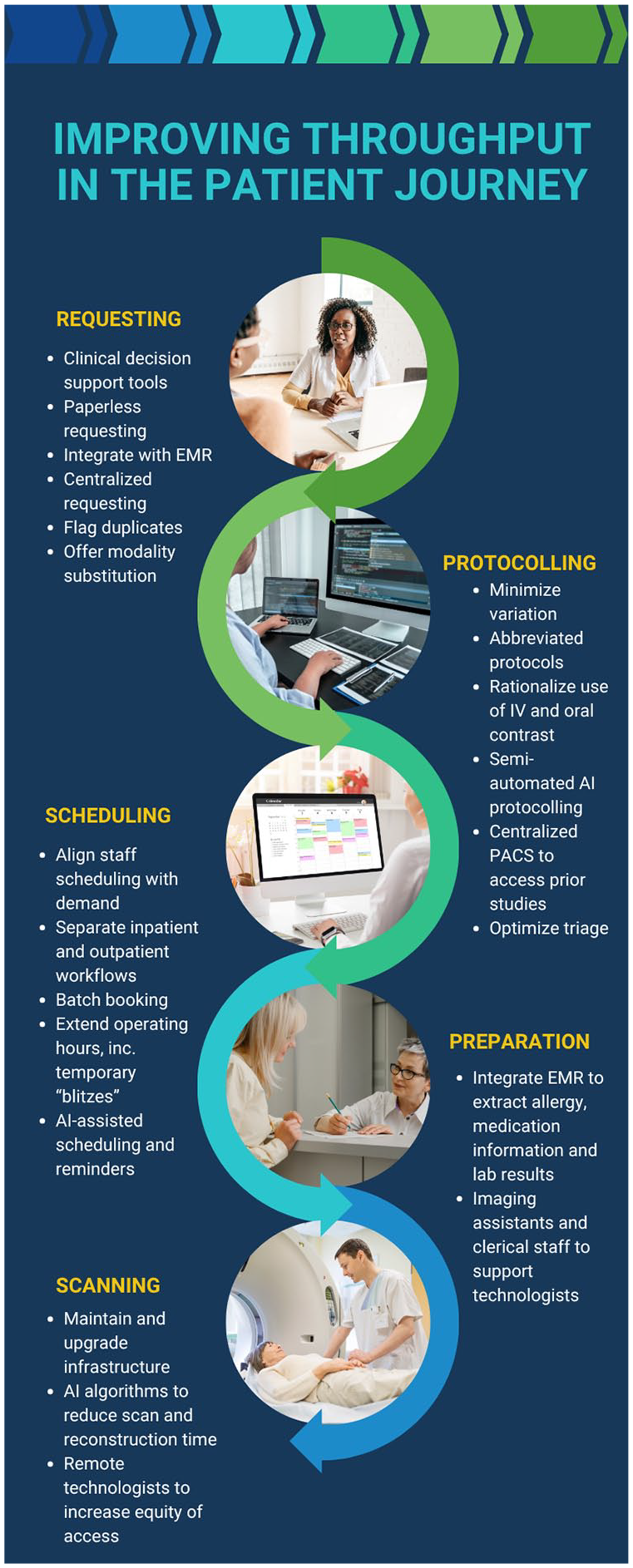
Summary of strategies.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.