
Abstract
Introduction
Breast magnetic resonance imaging (MRI) is widely regarded as the most sensitive method for detecting breast cancer.1,2 Accurate and efficient interpretation of breast MRI primarily depends on dynamic contrast-enhanced (DCE) sequences, which are considered the cornerstone of MRI examinations. 3 However, most breast MRI protocols also incorporate T2-weighted unenhanced sequences, which can provide additional insights into lesion morphology and internal composition, aiding in their characterization.4-12
A high T2 signal in breast lesions can correspond histologically to cystic or adipose components, mucinous or myxoid stroma, edema, necrosis, or hemorrhage. 4 T2 hyperintensity in breast lesions may be linked to benign conditions like fibroadenoma, fat necrosis, and lymph nodes.6,7,9,13,14 However, there is considerable overlap between benign and malignant lesions in terms of T2 signal, with certain carcinoma subtypes, such as mucinous and metaplastic neoplasms, often displaying high T2 signal intensity.5,10
Several studies have investigated factors associated with malignancy in breast MRI-guided biopsies.15-21 However, to the best of our knowledge, only one study focused specifically on the outcome breast lesions with high T2 signal. 22 In their original work Bissell et al 22 observed a 18% malignancy rate in T2 hyperintense lesions, challenging the notion that high T2 signal is a benign imaging feature. Older age and larger lesion size were found to be an important predictor of malignancy in that analysis.
The primary objective of this investigation is to assess the malignancy rate in breast MRI-guided vacuum-assisted biopsies (MVAB) performed on lesions exhibiting high T2 signal. The secondary objective is to examine the association between various factors and the biopsy outcomes.
Materials and Methods
Patients and Inclusion Criteria
The local IRB’s research ethics committee approved this retrospective study, and the need for informed consent was waived.
We conducted a retrospective analysis of all MVAB performed at our institution between January 2016 and December 2021. The 2016 to 2021 range was chosen because it was sufficiently large and recent, and for which complete electronic medical records and imaging data were available. The cohort included only cases involving biopsies of lesions with high T2 signal. The evaluation of the T2 signal was based on the breast MRI that led to the biopsy recommendation performed in our institution. Cases with suboptimal T2 sequences that prevented lesion assessment were excluded. For patients undergoing 2 biopsies, both lesions could be included if they exhibited a high T2 signal and were distinct from each other. In patients with known breast cancer, the case was included only if the biopsied lesion was distinct from the malignancy.
Breast MRI and Biopsy Techniques
All breast MRI studies were conducted using either a 1.5 or 3 T imaging system (Siemens Healthcare) with a dedicated breast coil. The standard breast MRI protocol included a localizer, non-fat-saturated and fat-saturated axial T1-weighted sequences, an axial T2-weighted STIR sequence, and 5 post-contrast axial T1-weighted sequences. Additionally, post-processed subtraction images and maximum intensity projection (MIP) images were generated for each examination.
In our practice, when an MRI-detected lesion requires tissue sampling, we typically begin with a mammogram—unless one has been performed within the past 6 months—followed by a targeted ultrasound. If no clear correlate is identified on either modality, we proceed with MVAB.
For the MVAB, the patient was positioned prone in a dedicated breast biopsy coil using a grid device. Axial plane–unenhanced and contrast-enhanced fat-suppressed T1-weighted images were acquired. The lesions were targeted using dedicated MRI biopsy software (Hologic, Aegis Breast Imaging and Interventional Software, Bedford, MA, USA). The MRI-guided biopsy procedure was conducted using a 9-gauge MRI-compatible vacuum-assisted device (ATEC, Suros Surgical Systems, Bedford, MA, USA) with a range of 8 to 14 samples obtained per procedure in most cases. A breast biopsy clip was deployed in the biopsy cavity at the end of the MVAB (TriMark, Hologic, Bedford, MA, USA).
Image Review and Data Collection
All breast MRI and MVAB results from the study period were retrospectively reviewed by one of 2 fellowship-trained breast radiologists with 20 and 10 years of experience, respectively (O.G. and Y.A.). Imaging data were extracted from the Picture Archiving and Communication System (PACS). T2 hyperintensity was defined as signal intensity equal to or greater than that of normal lymph nodes on short tau inversion recovery (STIR) sequences. In cases of heterogeneous T2 signal, the predominant signal pattern was used for analysis. Ambiguous cases were resolved by consensus between the 2 radiologists. Additional imaging characteristics were extracted from the images based on the BIRADS lexicon, 23 including breast density, background parenchymal enhancement, lesion type and morphology and kinetic assessment. All MRI studies were processed using a commercially available computer-aided detection system (Hologic, Aegis Breast Imaging and Interventional Software, Bedford, MA, USA). Radiologists were blinded to pathology outcomes during the retrospective image review to minimize bias.
Demographic and pathologic data were also collected from patient electronic and medical records. Malignancy was defined as either invasive malignancy or ductal carcinoma in situ (DCIS) on pathology. High risk lesions were considered benign, unless upgraded to malignancy on surgery. For each case, the demographic, radiological, and pathological information was recorded in a spreadsheet (Microsoft Excel 2022).
Data Analysis
The correlation between various demographic and imaging characteristics and the binary pathological outcome (benign vs malignant) was evaluated using appropriate statistical tests. The pathological outcome was determined based on findings from MVAB and, when available, subsequent surgical excision. The chi-square test or Fisher’s exact test was employed for categorical variables, while Student’s t test or Mann-Whitney U test was used for continuous variables. All calculations were 2-tailed, and P < .05 was considered statistically significant. Multivariable logistic regression analysis incorporated all variables with a P-value <.05. The statistical analysis was done using SPSS version 28 (IBM, Armonk, NY, USA).
Results
During the study period, 1345 MVABs were performed at our institution. Among them, 174 biopsies from 165 women met the inclusion criteria and were included in the cohort (Figure 1).
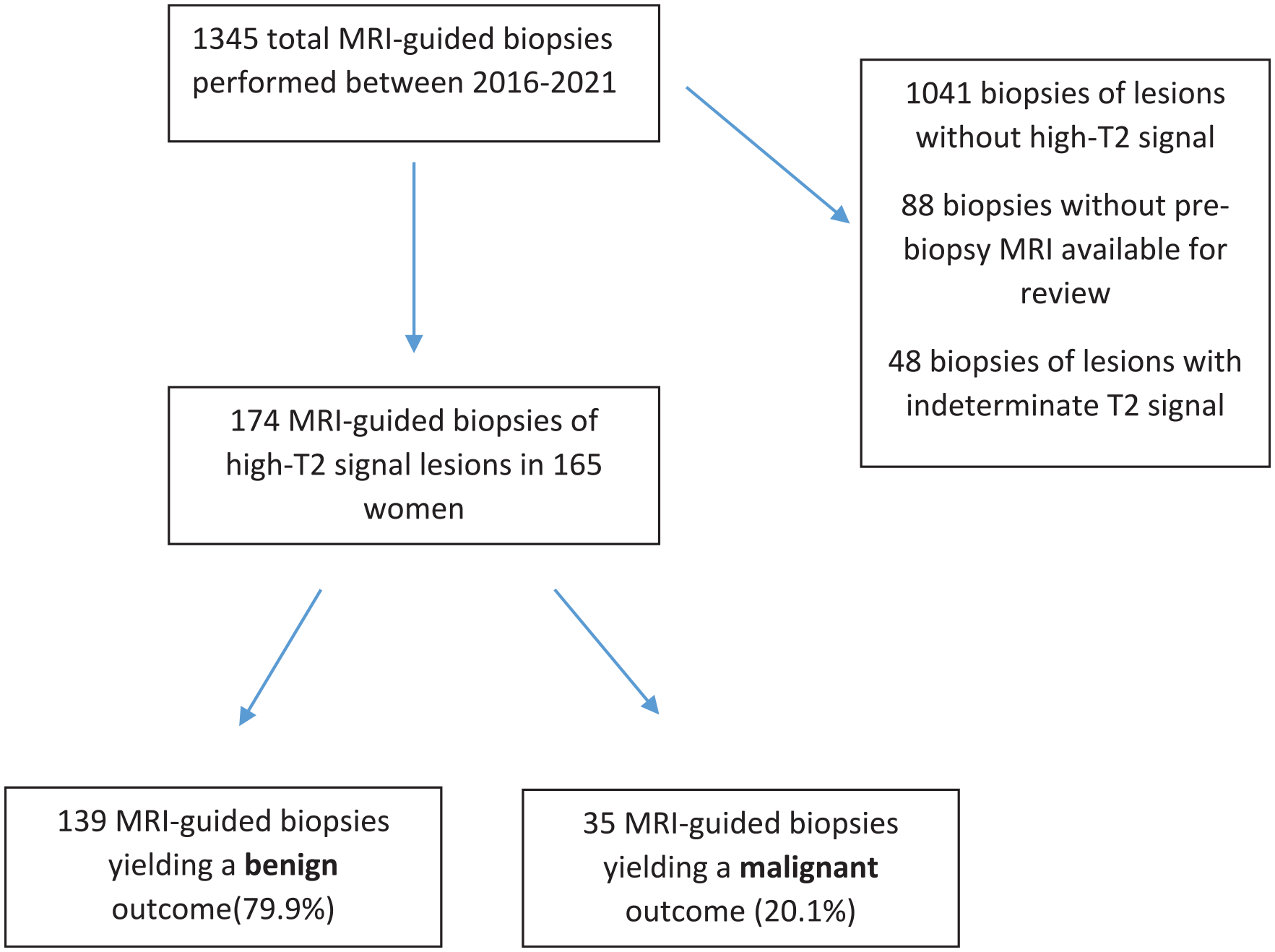
Flow chart of study cohort.
The median patient age was 56 years (range: 27-83). A family history of breast cancer was present in 44% of patients, while 16% had a personal history of the disease. The most common indication for breast MRI was disease extent evaluation (36%), followed by high-risk screening (32%). The median lesion size on MRI was 9 mm (range: 3-98 mm). The most common lesion type was non-mass enhancement (NME, 40%), most commonly in a focal distribution (50%).
MVAB yielded a benign result in 123 lesions (71%) and a malignant result in 32 patients (18%). In 19 lesions (11%), MVAB detected high-risk pathology, most commonly papilloma (13 cases), followed by ADH (3 cases), lobular neoplasia (2 cases), and radial scar (1 case). Surgical excision upgraded 3 of these high-risk lesions to malignancy, resulting in a total of 35 malignant cases (20%). The remaining lesions either yielded benign results on surgery or remained stable for at least 1 year of follow-up and were therefore classified as having a benign outcome.
The most common malignant diagnosis was DCIS (20 cases, 57%), followed by infiltrating ductal carcinoma (14 cases) and a single case of mucinous carcinoma. The majority of diagnosed DCIS cases were high-grade (53%), whereas most IDC cases were low to intermediate grade (86%). The predominant receptor subtype among IDC cases was luminal A (86%). No cases of micropapillary-type DCIS were identified
The most common benign diagnosis was fibrocystic changes (FCC), with was diagnosed in 53 patients (38%).
Figures 2 and 3 depict a case featuring a T2 hyperintense lesion that was diagnosed as mucinous carcinoma.
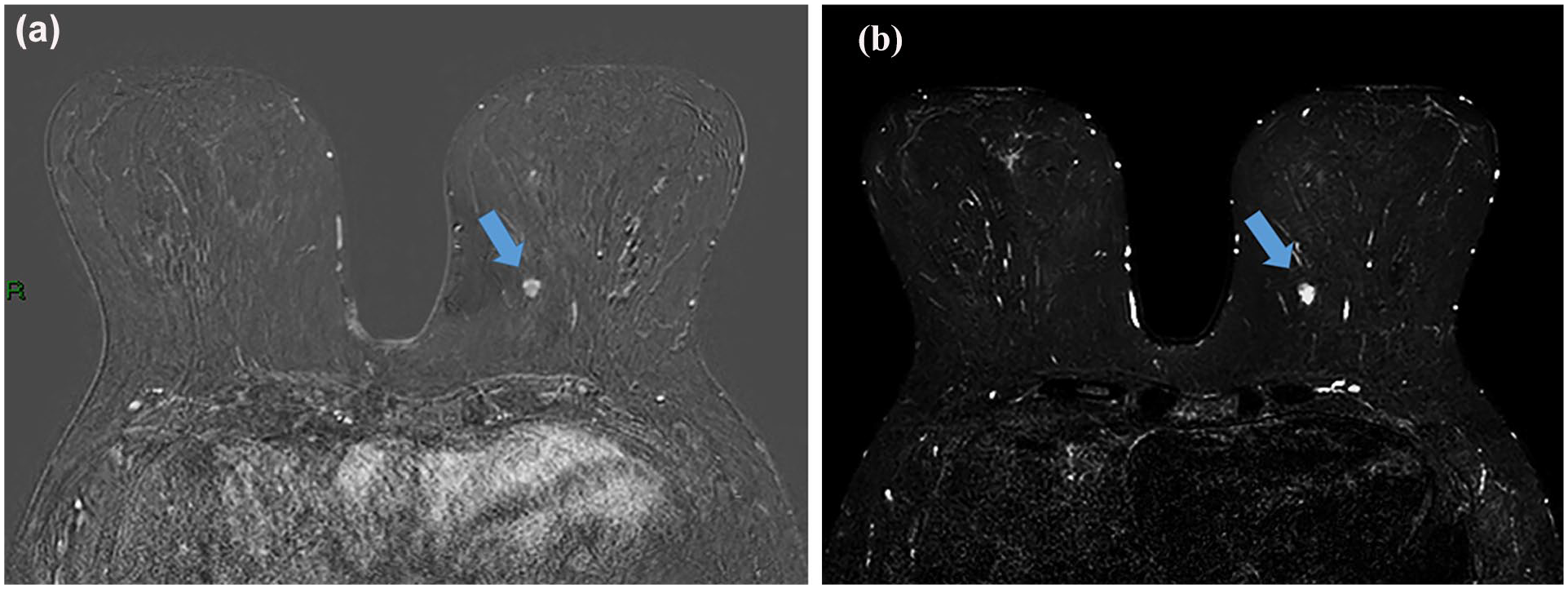
Breast MRI subtraction (A) and STIR (B) sequences of a 64-year-old patient with a family history of breast cancer. Breast MRI shows an irregular enhancing mass in the left lower inner quadrant with high T2 signal (arrows). No corresponding finding on mammogram and ultrasound.
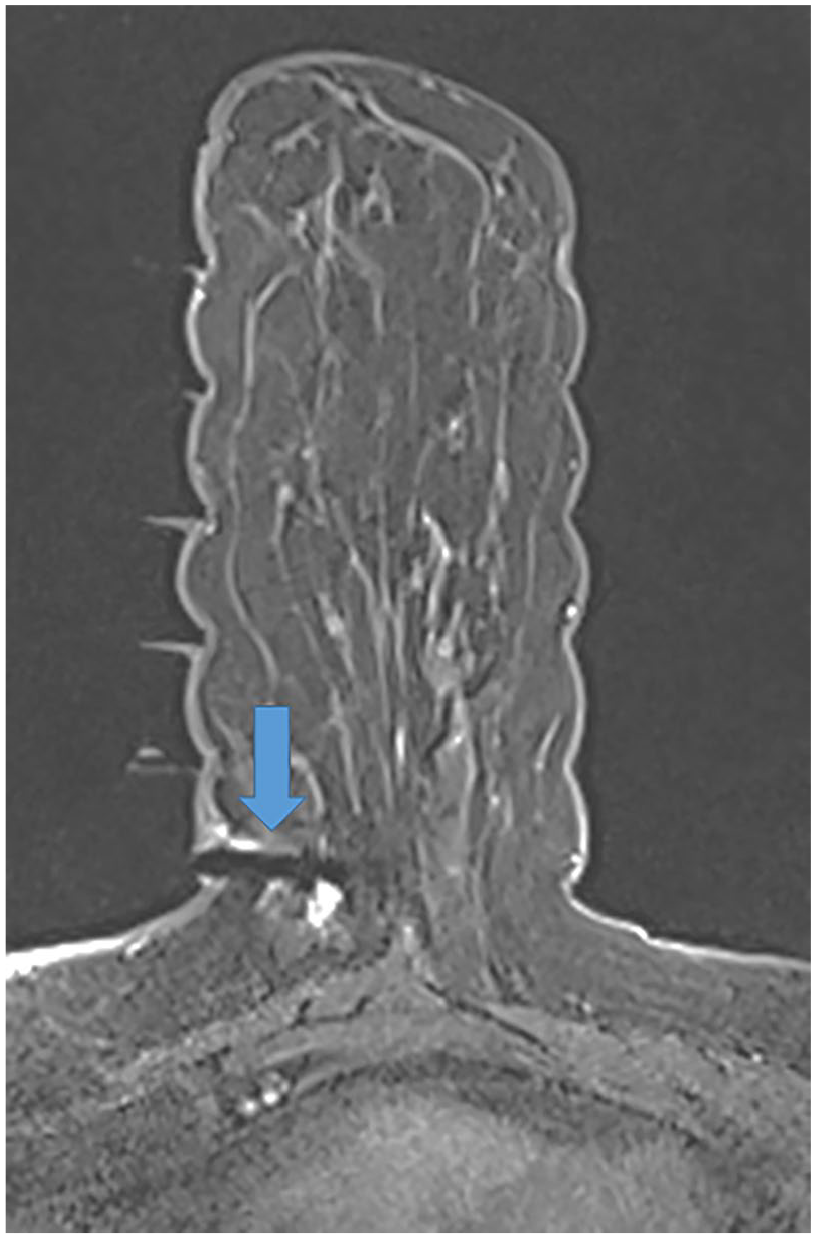
Image of left MRI-guided breast biopsy of the mass showing the needle with its tip near the lesion (arrow). Pathology revealed mucinous carcinoma.
On univariate analysis, older age (Mean 61 vs 54 years, P = .03), washout kinetics (29% vs 13%, P = .03), and MRI indication for extent of disease evaluation (53% vs 32%, P = .02) were the strongest predictors of malignancy. In Multivariable analysis, older age and washout kinetics remained significant (P = .04 and .01, respectively). MRI indication was not significant (P = .06), though the result was close to the predefined cutoff and may indicate a possible association (Table 1).
Association Between Different Parameters and Final Pathology.
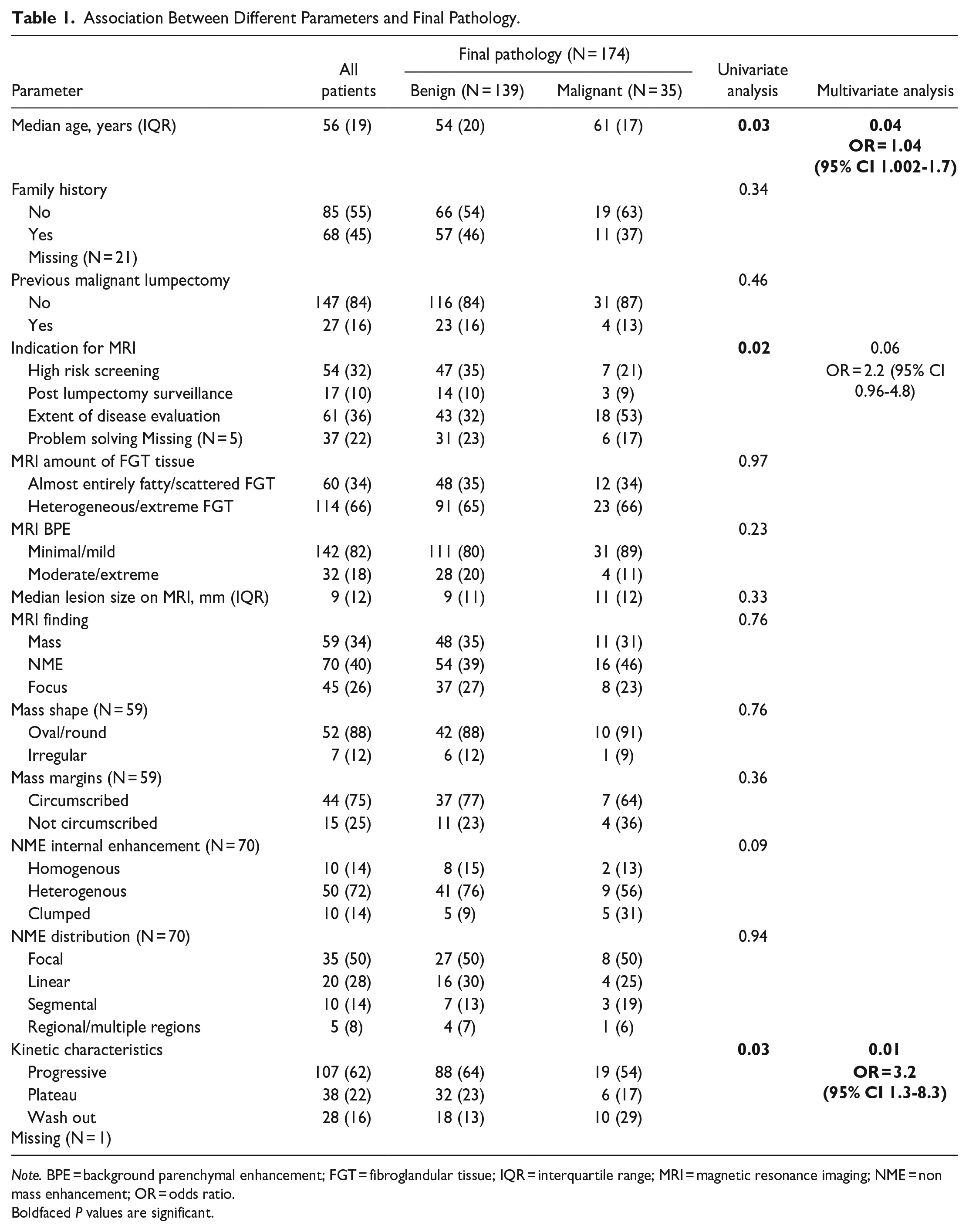
Note. BPE = background parenchymal enhancement; FGT = fibroglandular tissue; IQR = interquartile range; MRI = magnetic resonance imaging; NME = non mass enhancement; OR = odds ratio.
Boldfaced P values are significant.
Discussion
This study sought to examine the outcomes of MVAB performed on breast lesions exhibiting high T2 signal intensity. To our knowledge, it is the largest investigation on this topic. While T2 hyperintensity is generally associated with benignity in the breast, there is surprisingly little literature to substantiate this expectation.
We observed an 20% malignancy rate in lesions with high T2 signal, which is consistent with a previous study by Bissell et al, 22 who reported an 18% malignancy proportion in a cohort of 100 T2 hyperintense lesions. A recent meta-analysis on the performance of MVAB, involving 10 592 biopsied lesions, found a pooled malignancy rate of 29.6% (95% CI 23.6%-36.5%). 24 The 20% rate is lower than this expected range, lending support to the idea that high T2 signal may indicate benignity. However, a 20% malignancy rate is noteworthy and suggests that high T2 signal should not be considered a definitive marker for excluding malignancy.
Older age emerged as an important predictor of malignancy in our cohort. A similar association was detected in the recent work by Bissell et al. 22 However, previous studies examining the relationship between age and MVAB outcomes—without specifically focusing on T2 hyperintense lesions—did not identify a significant association.17,18 This discrepancy may be explained by the higher prevalence of fibrocystic changes (FCC), which are often T2 hyperintense, in younger patients. In our cohort, 38% of benign lesions contained an FCC component. Consequently, the higher malignancy rate observed with increasing age may, in part, reflect the lower occurrence of benign FCC-related lesions in older individuals. Although second-look ultrasound can often detect FCC, radiologists are often not sufficiently confident to avoid MVAB, as malignancy may still be present adjacent to areas of FCC.
Washout kinetics also emerged as a key factor associated with malignancy in our study, consistent with previous research highlighting kinetic features as significant predictors of malignant lesions.15,17,18,25 This association could apply regardless of T2 signal. Additionally, we observed that malignancy rates varied based on MRI indication, with a higher proportion detected in patients undergoing MRI for the evaluation of disease extent. This association was reported in several previous works18,24-26 and is expected, given that MRI is highly sensitive in detecting multifocal, multicentric, and contralateral disease that may be occult on other imaging modalities.27,28
Apart from kinetic characteristics, no other MRI features, including background enhancement, lesion size, or lesion type such as mass, non-mass enhancement, or focus, were identified as significant predictors of malignancy. An interesting observation is that half of T2 hyperintense cases with clumped NME had a malignant outcome. However, this association did not reach statistical significance due to the small sample size of 10 cases. Clumped NME is known to have a high positive predictive value (PPV) for malignancy.29,30 In their recent work Bissell et al have shown a similar trend in lesions with high T2 lesions. 22 Further large-scale studies are needed to better evaluate the role of clumped and other enhancement patterns in this subgroup.
In their recent large meta-analysis on MVAB’s, Özcan et al 24 reported a lower proportion of ductal carcinoma in situ compared to invasive cancer, with DCIS accounting for 40% (95% CI 33.5%-46.7%). In contrast, DCIS was the most common malignant diagnosis in our cohort, representing 57%—a higher-than-expected proportion. This tendency for in situ cancer rather than invasive cancer in T2 hyperintense lesions is a notable finding that has not been extensively studied. One possible explanation is that ductal dilatation associated with intraductal cancer cells may produce high T2 signal. Furthermore, both in our practice and in others, it is routine to perform a mammogram and second-look ultrasound for MRI-detected lesions, followed by mammotomy or ultrasound-guided biopsy when feasible. Consequently, common invasive malignancies that exhibit T2 hyperintensity—such as mucinous and papillary carcinomas—are typically identified during the second-look ultrasound, thereby decreasing the likelihood of requiring MVAB.
Our study has several limitations. First, its retrospective design resulted in some missing data and may have introduced selection bias. Second, our study did not include T2-hyperintense lesions biopsies using ultrasound or mammogram guidance, which is another potential source of selection bias. Third, the study was conducted at a single centre with specific expertise and resources, which may not be generalizable to other institutions. Furthermore, the small sample size in certain subgroups, such as those with clumped NME, limits the statistical power of the analysis. Additionally, this work did not incorporate artificial intelligence tools, which could add further benefit in differentiating benign from malignant entities. Moreover, alternative approaches for evaluating T2 signal—such as comparing it to normal background parenchyma or cerebrospinal fluid—could have been used and may have influenced the results. Finally, even with the use of an objective reference point like lymph nodes, the evaluation of T2 hyperintensity remains inherently subjective, especially for lesions with heterogenous signal, which could affect the findings.
In conclusion, MRI-guided vacuum-assisted biopsy of T2 hyperintense lesions reveals a considerable malignancy rate, with DCIS being the most common diagnosis. Malignancy is more frequently observed in older patients, lesions with washout kinetics, and cases where MRI is performed for disease extent evaluation. These findings may have practical clinical implications, and further studies are encouraged to explore this topic and validate our results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.