
Abstract
Introduction
Radiology reports play a crucial role in efficiently and comprehensively communicating important radiological information between radiologists and referring physicians to guide diagnosis and treatment. 1 The structure of these reports is critical for effective communication. There is currently a lack of evidence on how radiologists should structure their reports for neuroradiology studies.
There are several reporting structures in radiology, including free-text and structured reports. 2 Radiology reports summarize key imaging findings in a concise format, typically divided into sections such as study type, clinical history, technique, comparison, findings, and impression/summary. The primary differences between free-text and structured reports are found in the findings and impression sections, which are the most critical components of radiology reports.
Free-text reports are structured as short paragraphs in which radiologists synthesize and present their interpretations. This format is currently the most used structure in neuroradiology reports. 3 Free-text reports offer radiologists flexibility to describe their interpretations in a cohesive manner, which is particularly useful in the context of complex diseases affecting multiple structures. However, studies have highlighted important limitations, including a lack of reproducibility and considerable inter-reader variability.3,4 Additionally, referring physicians must carefully read through paragraphs to locate specific information of interest as there is a lack of standardization.
Standardized and structured reports were employed to improve the uniformity of report content.5-7 Standardized reporting involves using established classifications, such as the BI-RADS or PI-RADS tools, or unifying reporting language through resources like the RadLex database. 1 Structured reporting can take the form of a templated layout, where a predefined structure is used to build the report, or structured content, where information is selected from dropdown menus or predefined lists. 5 Both standardized and structured reports offer advantages over free-text reports, including improved efficiency, reliability, clarity, and the potential for data mining in research.6,8 Studies have also shown increased satisfaction among radiologists and referring physicians with the adoption of these formats.4,8 However, there are limitations—structured reporting can oversimplify details in complex cases or complicate workflows in atypical cases that do not align with the predefined structure. 2
In this study, we designed and disseminated a survey to radiologists and referring physicians in Ontario, to determine their preferences for reporting structures for various imaging studies. Feedback obtained from this survey can inform the development of report formats that better align with the needs of those who rely on them for patient management. The specific objectives of this study were to:
Explore how physicians read radiology reports and assess their satisfaction with current report structures.
Determine physicians’ preferences for report structures and identify differences between subgroups.
Methods
Ethical Considerations
This project was exempted from the quality improvement review committee review at the local institution.
Survey Development
Between February and March 2024, the survey was developed using REDCap by a medical student and several staff neuroradiologists.
The survey had 2 sections: satisfaction with current report sections and preferences regarding 7 neuroradiology reports. There was a mix of multiple-choice, select-all-that-apply, and open-ended questions. It included 6 demographic and practice-related questions, 13 questions regarding physicians’ preferences on various components of current reporting structures, and 5 questions for each of the 7 sample reports, presented in both free-text and structured formats. Sample anonymous radiology reports and survey questions were prepared by the project supervisor, a neuroradiologist, and reviewed by the radiologist-in-chief and radiology fellows for content and clarity. The final question allowed respondents to provide any additional feedback.
In the section surveying physicians on their preferences for specific neuroradiology studies, 7 studies were selected to be represented in the sample reports: MRI lumbar spine, MRI of the sella, MRI brain for dementia, MRI brain for glioma follow-up, MRI brain metastasis, CTA head and neck for brain, and CT brain Unenhanced. Respondents were asked to select the studies they commonly encountered in practice; sample reports for the neurological studies were shown only to those who indicated they commonly encountered those studies. A complete copy of the survey questionnaire can be found in Supplemental Appendix A.
Survey Distribution
The survey anonymously collected responses from March 2024 to July 2024. Requests to complete the survey were emailed to department heads in academic and community hospitals. the Greater Toronto Area to be shared among residents, clinical fellows, and attending physicians in their departments. Reminder emails were sent in May and June 2024.
Target respondents for this survey were physicians, residents, and fellows in family medicine, emergency medicine, internal medicine, geriatrics, medical oncology, radiation oncology, psychiatry, radiology, neurology, and neurosurgery. In the initial survey invitation email, radiologists were instructed to complete the survey based on their preferences when reading and interpreting radiology reports, rather than when drafting them.
Data Analysis
Demographic information of participants, frequency of reading entire reports, satisfaction with report section length and structure, and the usefulness of key images and radiologist contact information were summarized descriptively. Preferences for report structures across 7 neurological studies were analyzed for differences using Fisher’s Exact test, with comparisons made across specialties (radiologists and referring physicians), years of experience, and practice settings. Open-ended responses were analyzed by identifying common themes. Regression or correlation analyses were not conducted due to the small sample size.
Results
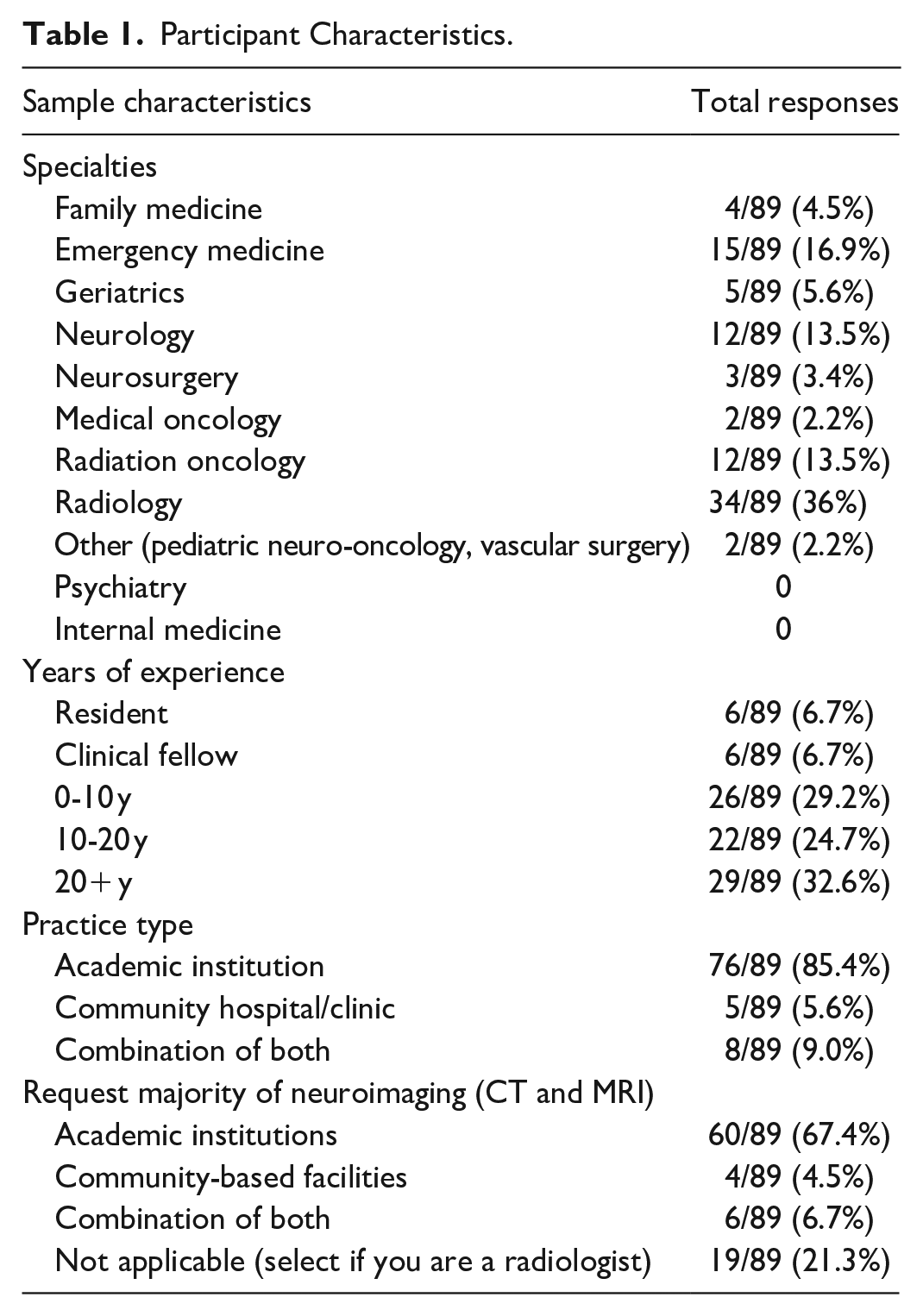
A total of 89 responses were collected in the survey. Two responses were excluded from the analysis due to representing only one respondent per specialty, resulting in a total of 87 responses analyzed. Table 1 outlines the demographic information of the respondents. No responses were received from internal medicine or psychiatry. Most respondents were radiologists (34/87, 41.5%) with over 20 years of staff experience (29/87, 33.3%), working at academic institutions (76/87, 87.4%).
Participant Characteristics.
Satisfaction on Reporting Structures
The first part of the survey consisted of questions on how physicians read radiology reports and their preferences for various components of a radiology report. When asked about the frequency of reading the entire radiology report, the most common response was “most of the time” (32/87, 36.8%; Supplemental Figure 1). However, a substantial proportion of physicians (29/87, 33.3%) indicated that they read the body of the report “only if the impressions section describes an abnormality” or that they rarely read beyond the impressions section.
A Fisher’s exact test revealed a statistically significant difference between specialties (P = .035). Neurologists showed high positive residuals (3.677) for selecting “Always” reading the full report, while radiologists had high positive residuals (2.302) for selecting “Rarely, as I only read the impression.” No significant differences were found among other demographic subgroups (years of experience or practice settings).
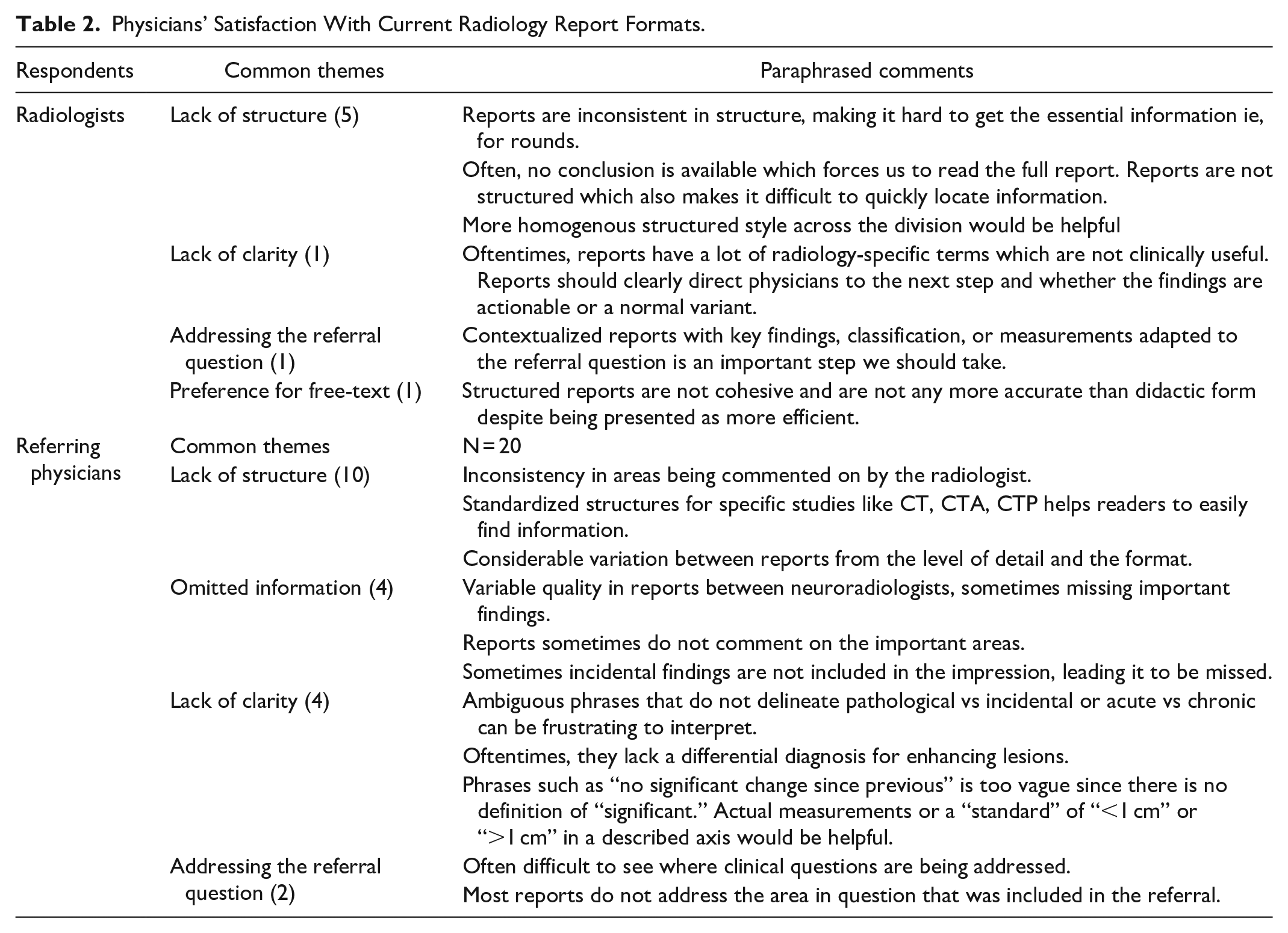
Clinicians were surveyed on their current satisfaction with neuroradiology reports they typically receive in practice. Most referring specialties indicated that they were either “neutral” (14/53, 26.4%) or “satisfied” (28/53, 52.8%). Radiologists similarly responded that they were “neutral” (10/34, 29.4%) or “satisfied” (19/34, 55.9%). When asked to elaborate on the reasons for dissatisfaction, both radiologists and referring physicians most cited variable quality among radiologists’ reports, difficulty locating the clinical information in question, failure of some reports to address critical findings, and lack of clarity in phrasing (Table 2).
Physicians’ Satisfaction With Current Radiology Report Formats.
Regarding the perceived length of various sections in radiology reports, the techniques, findings, and impression/summary section were each considered appropriate in length by the majority of referring physicians and radiologists (Supplemental Figure 2). The overall consensus for both groups was that the sections are appropriate in length. However, radiologists were more likely to indicate that each section is “too long” compared to the referring clinicians.
Most referring physicians (36/53, 67.9%) and radiologists (25/34, 73.5%) responded that capitalized section headers are useful when reading reports. Regarding the necessity of including a final impression/summary section, the vast majority of referring physicians (51/53, 96.2%) and radiologists (26/34, 76.5%) indicated that it is essential.
When asked about the preferred structure of the impression/summary section, about half of the referring clinicians (27/53, 50.9%) and radiologists (20/34, 58.8%) preferred bullet points for each finding. Some referring clinicians (19/53, 35.8%) and radiologists (9/34, 26.5%) expressed no preference for structure, while a smaller group of referring clinicians (4/53, 7.5%) and radiologists (3/34, 8.8%) preferred a short, consolidated paragraph.
The inclusion of key annotated images highlighting relevant imaging findings was found to be useful by most referring clinicians (40/53, 75.4%) and radiologists (25/34, 73.5%). Opinions on the inclusion of the reporting radiologist’s contact information at the end of the report were revealed more referring clinicians (38/53, 71.7%) indicating it being necessary than radiologists (18/34, 52.9%).
Preferred Reporting Structure for Different Neurological Studies
To further explore preferences for reporting structures, physicians were presented with sample reports for 7 neurological studies both structured and free-text formats. These reports corresponded to studies that respondents frequently encountered in their practice. The 3 most encountered studies were CT Brain Unenhanced (52/87, 59.8%), MRI Lumbar Spine (48/87, 55.2%), and CTA Head and Neck for stroke (44/87, 50.6%; Supplemental Figure 3).
Figures 1 and 2 summarizes physicians’ preferences for report structures across different neurological studies. Structured reports were preferred over narrative reports for all studies. No significant differences were observed based on respondents’ specialties or specific neurological studies (Supplemental Appendix B). Notably, a substantial proportion of referring physicians (24/29, 82.8%) and radiologists (12/14, 85.7%) preferred structured reports for CTA Head and Neck for stroke. In contrast, there were relatively mixed preferences of report types on MRI of the sella among referring physicians (4/8, 50%) and MRI for glioma follow-up among radiologists (6/12, 50%).
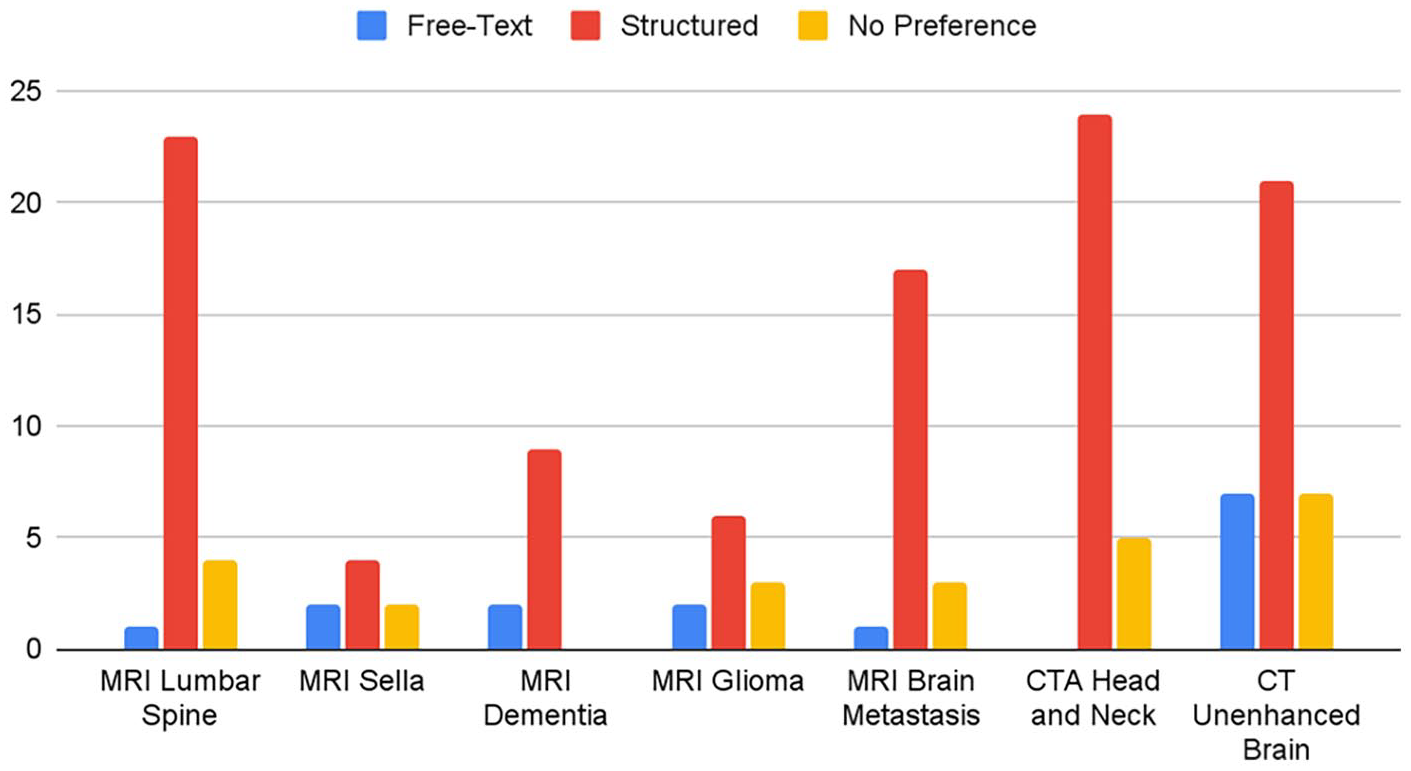
Referring physicians’ preferred report structure for neuroimaging studies.
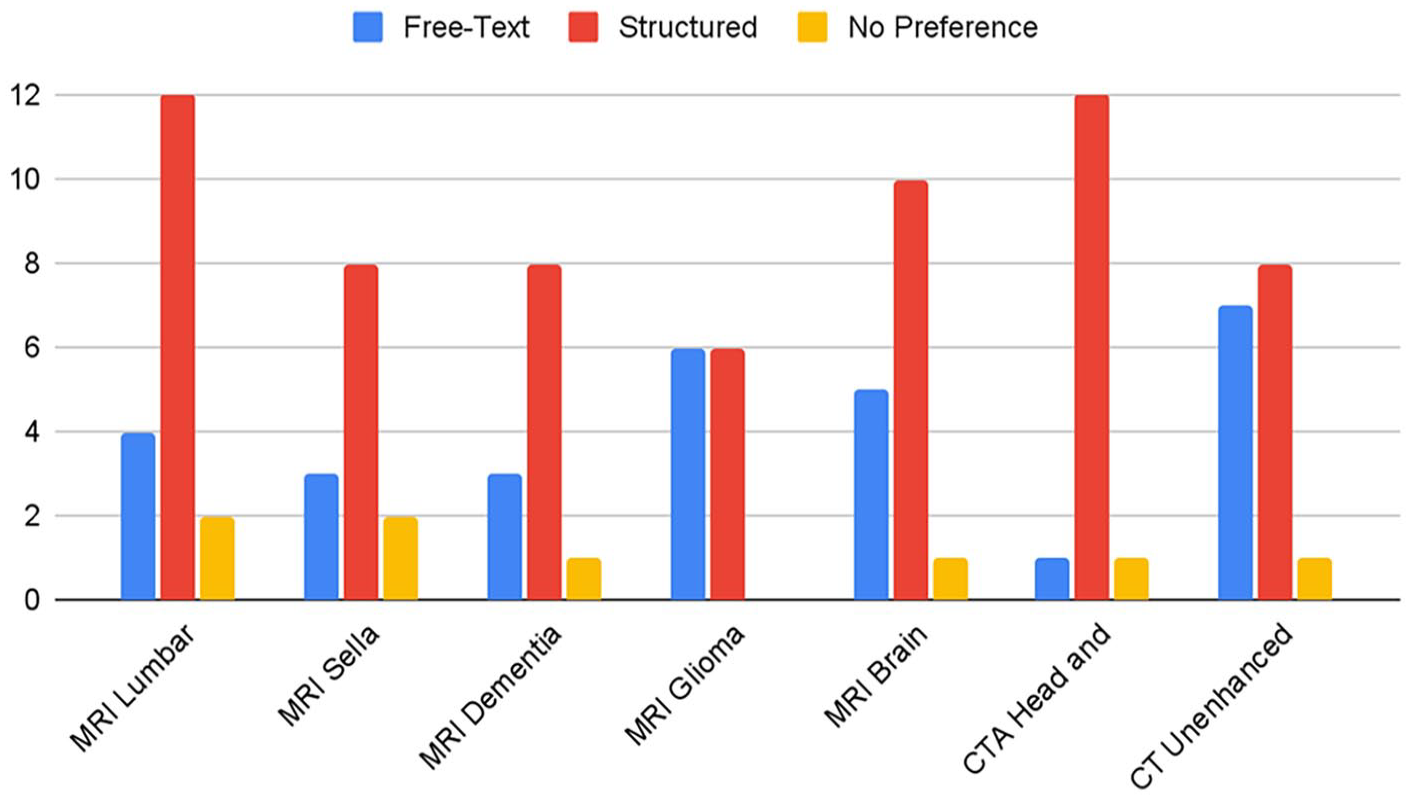
Radiologists’ preferred report structure for various neuroimaging studies.
Respondents were asked to select all applicable reasons for their preferences for each neurological study. For respondents that preferred structured reports, “ease in finding information” was overall the most frequently selected reason for both radiologists and referring physicians (Figures 3 and 4). Notably, the most commonly selected reason for preferring structured reports for MRI brain metastasis among radiologists was that it “saves time.” The most selected reason for preference for structured reports for MRI brain for dementia was comprehensiveness. For respondents who preferred free-text reports, “fewer unnecessary sections” was the most frequently selected reason for their preference across all studies for both radiologists and referring physicians, with the second reason being it saving time (Figures 5 and 6).
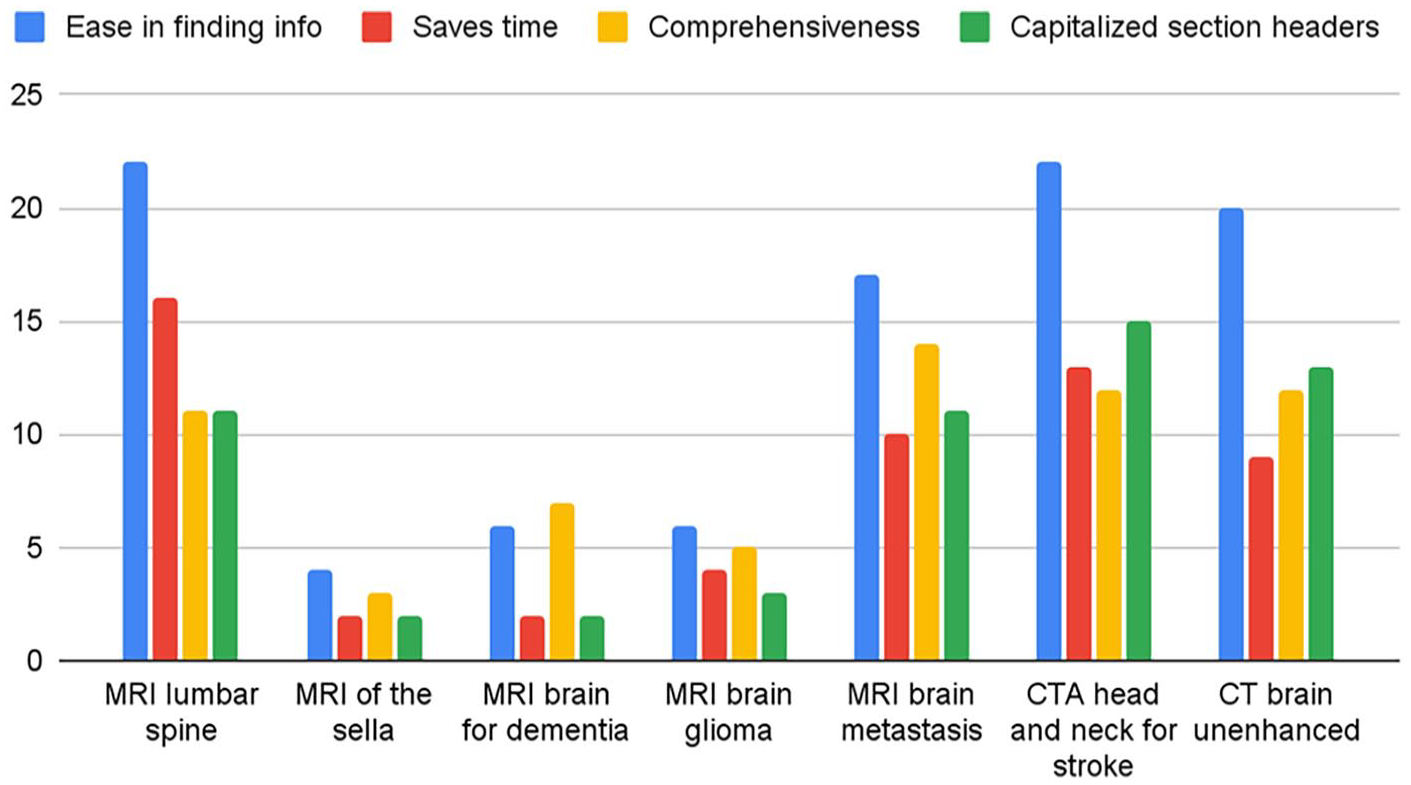
Referring physicians’ reasons for preference for structured reports.
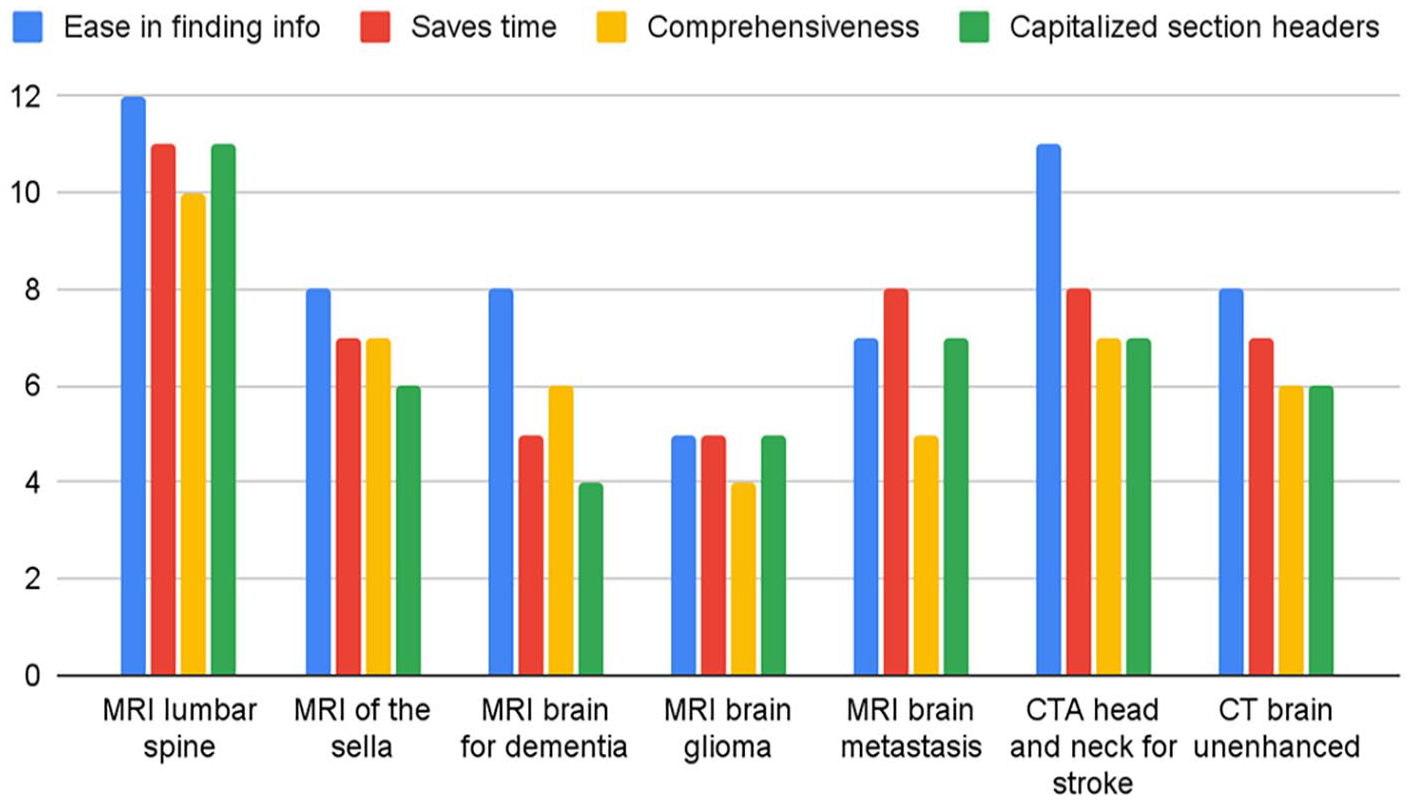
Radiologists’ reasons for preference for structured reports.
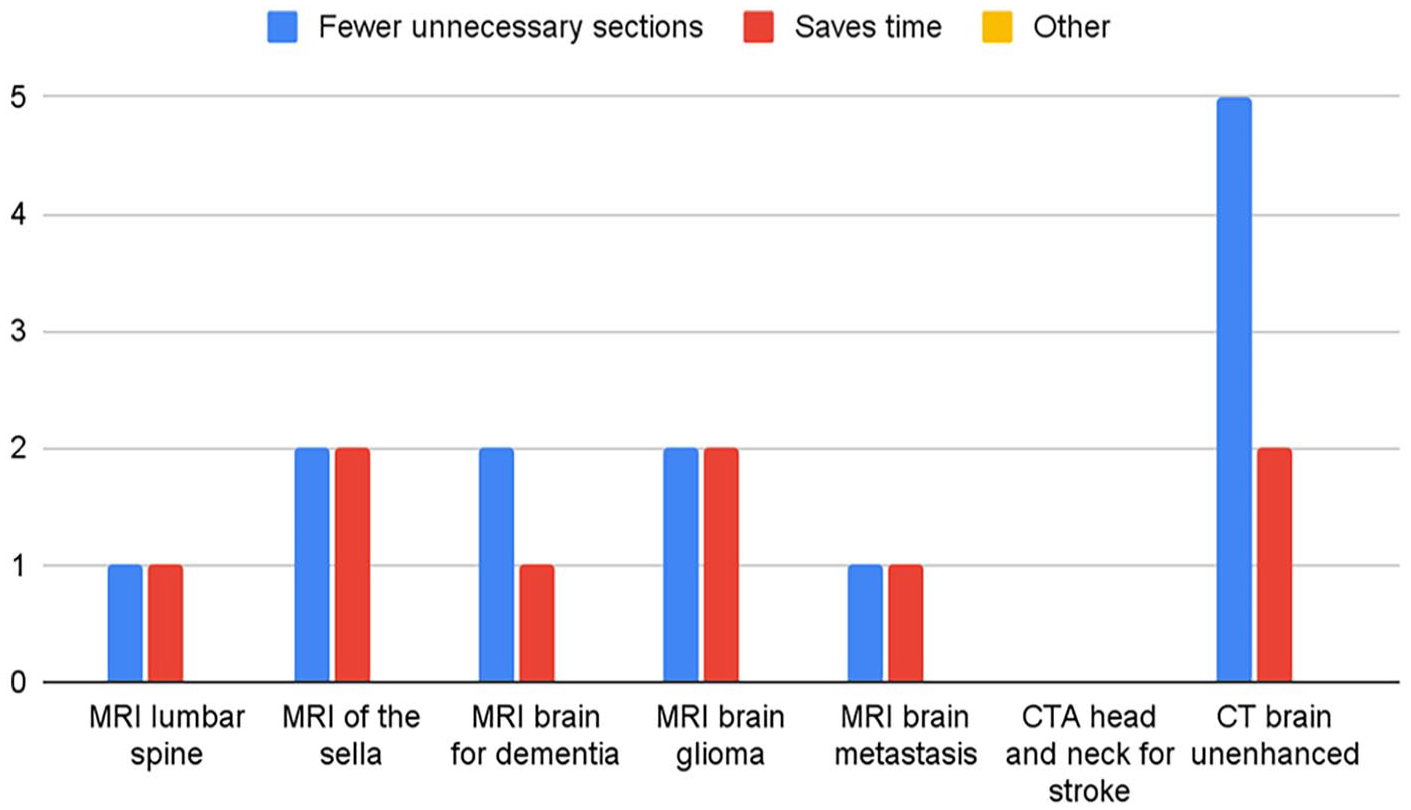
Referring physicians’ reasons for preference for free-text reports.
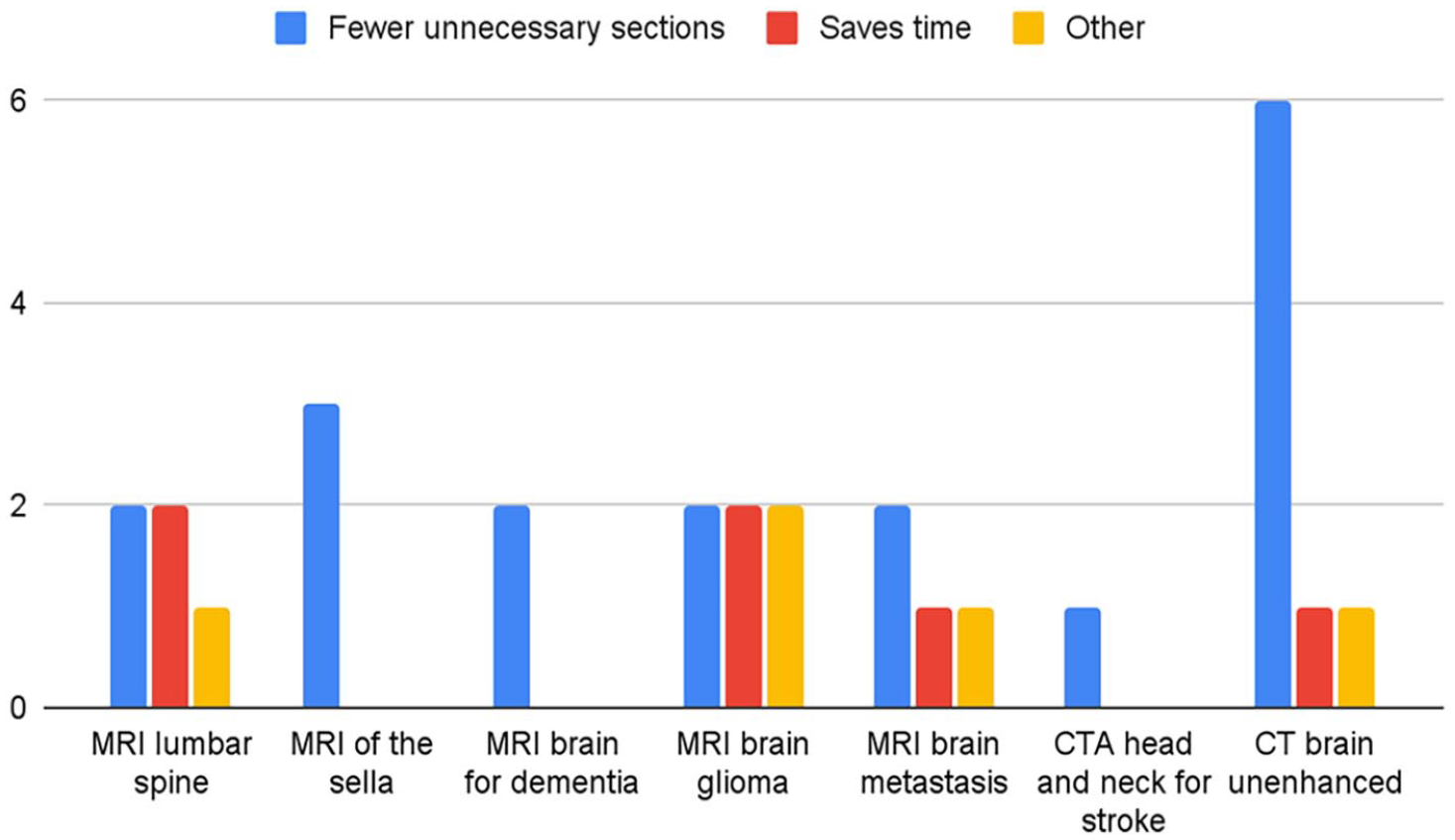
Radiologists’ reasons for preference for free-text reports.
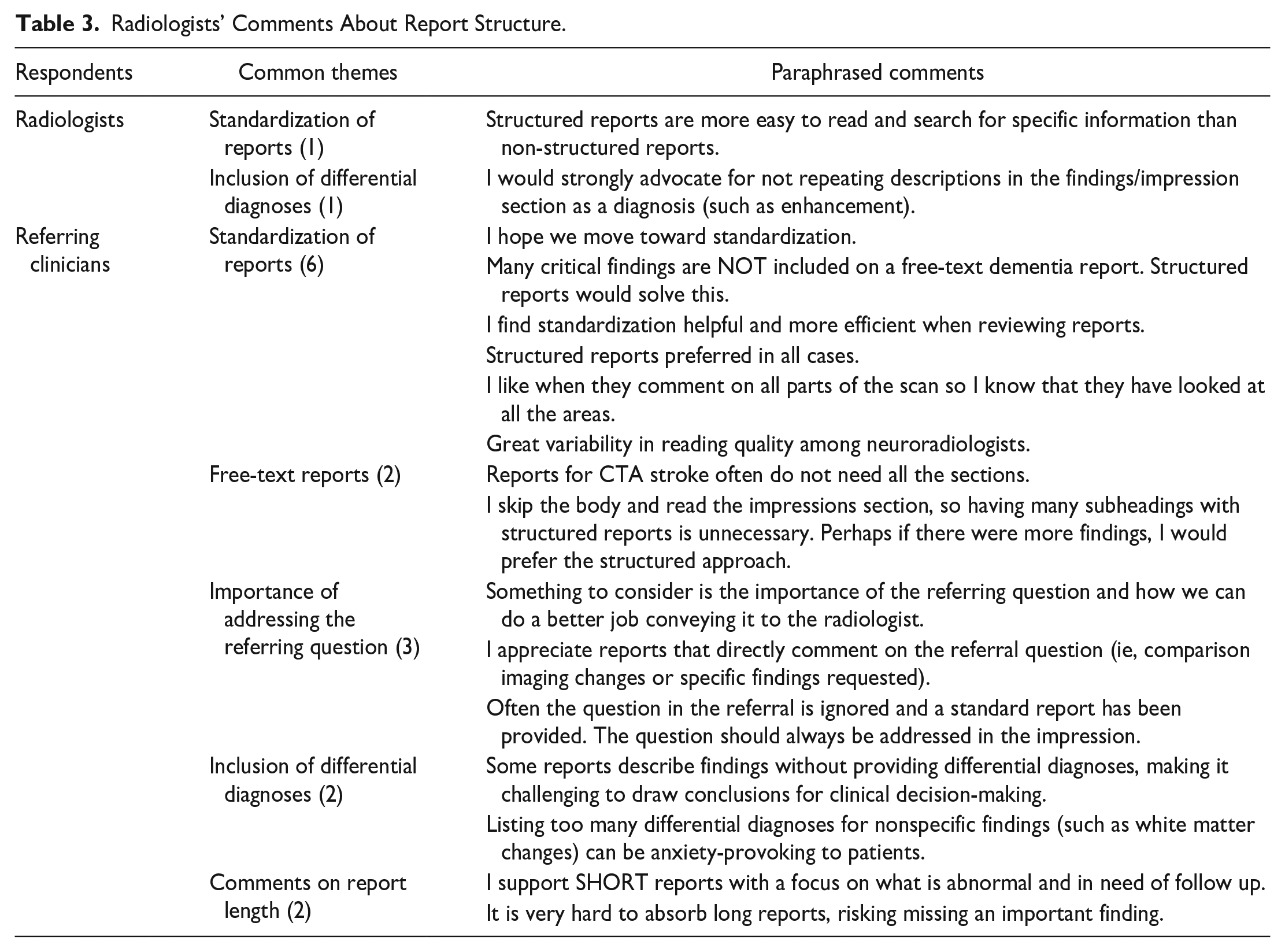
At the end of the survey, respondents had the opportunity to provide additional comments regarding radiology report structures (Table 3). Several referring physicians and radiologists expressed support for shifting toward using structured reports with an emphasis on standardization of contents to improve comprehensiveness and facilitate ease of finding information. Some highlighted concerns about the heterogeneity in radiology report structure and length, noting that lengthy reports may increase the risk of physicians overlooking critical findings. Additionally, respondents emphasized the importance of reports addressing the referral question to enhance clinical correlation.
Radiologists’ Comments About Report Structure.
Discussion
This study underscores the need for improved information organization and standardization in radiology reports. Although most respondents described they were satisfied with current neuroradiology they receive, further questions revealed some dissatisfaction regarding heterogeneity of reports across radiologists and institutions and length of reports. Structured reports were consistently favoured over free-text reports for all neurological studies across specialties, with “ease in finding information” cited as the most common reason for their preference. However, a subset of physicians expressed a preference for free-text reports, particularly for CT Brain Unenhanced (among referring physicians) and MRI glioma (among radiologists), due to their streamlined format with fewer unnecessary sections compared to structured reports. Referring clinicians and radiologists shared overall similar preferences of structured reports across different neuroimaging studies; there were no significant differences between the preferences of different specialties and neuroimaging studies according to the Fisher’s exact test.
Improving Comprehensiveness in Radiology Reports
Several physicians commented on the importance of including clinical interpretation and differential diagnoses, which are sometimes omitted in radiology reports. Clinicians emphasized the value of radiologists providing clinical interpretation beyond nonspecific descriptions of imaging findings, such as “hyperintense” or “stable mass,” as these are more practically useful. This concern is particularly significant, as studies have identified substantial variability in the language used to convey diagnostic certainties in radiology reports. 9 Institutions that have implemented structured reporting have reported significantly improved linguistic standardization compared to free-text reports. 10
Comprehensiveness must be balanced with the length of reports, however. As demonstrated in the survey, physicians do not always read the full body of the report and often only read the impression/findings section. Some comments at the end of the survey supported this trend, where long paragraphs can hinder comprehension and in missed findings.
Preferences Between Free-Text and Structured Reports
In our study, both radiologists and referring physicians preferred structured reports over free-text reports. These findings align with other studies that have implemented structured reporting, where both clinical referrers and radiologists showed a preference for structured formats. 11
However, a risk associated with structured reports is the potential fragmentation of information and misinterpretation, particularly when clinical findings are categorized by anatomic regions or pathological processes. Structured reports can be challenging for radiologists to organize and for referring physicians to interpret, especially in complex cases involving imaging findings across multiple anatomical regions. Clinicians often pose specific clinical questions to be addressed in radiology reports. In such cases, it requires additional effort from radiologists to edit structured report templates to emphasize the relevant information. Therefore, there remains a need for free-text reports to provide flexibility.
Efficiency in Radiology Reports
There were some minor differences in physicians’ preferences for report structure across the 7 neurological studies. While structured reports were preferred for most studies, there was a relatively higher preference for structured formats in studies requiring a thorough review of findings for disease diagnosis or exclusion, such as MRI Brain for Glioma follow-up and CT Brain Unenhanced. Structured reports were overwhelmingly preferred for CTA Head and Neck for Stroke, a time-sensitive study where physicians prioritize structure over narrative context to quickly locate critical findings.
Limitations
Our study has several important limitations. Capturing the nuances in physicians’ preferences within a short survey, with a limited set of sample reports, presents inherent challenges. In the sample reports, we attempted to capture the most common reports in each study, where there are seemingly normal scans with some incidental findings that are not usually clinically significant. However, case complexity can influence physicians’ preferences for report structure as the readability and cohesiveness can be reduced with multiple findings. This will be a valuable topic to study in the future. We worked with a small sample size and an uneven distribution of responses across specialties, ranging from 2 to 34 responses. Radiologists were the most represented group (34 responses), while medical oncology and neurosurgery had only a few responses (2 and 3, respectively). Additionally, most of our participants worked in academic centres, which may not fully represent the preferences of physicians across different types of institutions.
Preferences for report structures may be influenced by historical institutional practices, where physicians tend to prefer the type they are most exposed to. The preferences of their radiology colleagues, particularly among residents and fellows, may also play a role, as they are often familiar with and comfortable adopting their supervising physician’s preferred format.
Conclusion
This study highlights physicians’ strong preference for structured radiology reports due to their ease of information retrieval and comprehensiveness. However, some physicians preferred free-text reports for their flexibility and conciseness. These findings underscore the need for standardization to enhance report organization and communication while maintaining flexibility for complex cases. Addressing limitations such as variability in institutional practices and ensuring inclusion of clinical interpretation will be critical for optimizing reporting structures in neuroradiology.
Supplemental Material
sj-docx-1-caj-10.1177_08465371251328260 – Supplemental material for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey
Supplemental material, sj-docx-1-caj-10.1177_08465371251328260 for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey by Jimin Lee and Paula Alcaide-Leon in Canadian Association of Radiologists Journal
Supplemental Material
sj-docx-2-caj-10.1177_08465371251328260 – Supplemental material for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey
Supplemental material, sj-docx-2-caj-10.1177_08465371251328260 for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey by Jimin Lee and Paula Alcaide-Leon in Canadian Association of Radiologists Journal
Supplemental Material
sj-docx-3-caj-10.1177_08465371251328260 – Supplemental material for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey
Supplemental material, sj-docx-3-caj-10.1177_08465371251328260 for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey by Jimin Lee and Paula Alcaide-Leon in Canadian Association of Radiologists Journal
Supplemental Material
sj-pdf-4-caj-10.1177_08465371251328260 – Supplemental material for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey
Supplemental material, sj-pdf-4-caj-10.1177_08465371251328260 for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey by Jimin Lee and Paula Alcaide-Leon in Canadian Association of Radiologists Journal
Supplemental Material
sj-pdf-5-caj-10.1177_08465371251328260 – Supplemental material for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey
Supplemental material, sj-pdf-5-caj-10.1177_08465371251328260 for Characterizing the Preferred Reporting Methods in Neuroradiology: A Multispecialty Survey by Jimin Lee and Paula Alcaide-Leon in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.