
Abstract
This practice guideline serves as an update to the Canadian Association of Radiologists’ 2013 Technical Standards for Bone Mineral Densitometry Reporting. It aims to align bone mineral density testing and reporting practices in Canada with current clinical best practices, including guidelines from Osteoporosis Canada and the International Society for Clinical Densitometry. Key updates include the endorsement of both FRAX and CAROC tools for evaluating fracture risk, guidance for analyzing male patients and transgender patients, and provision of clinical management guidance of relevance to BMD reporting harmonized with that of Osteoporosis Canada. The document emphasizes the importance of accurate data collection in fracture risk assessment and provides recommendations for reporting fracture risk, T-scores, and clinical management strategies. Additionally, it outlines indications for baseline BMD testing and reassessment timelines, aiming to facilitate appropriate patient management and enhance bone health outcomes. This guideline is intended to complement existing standards and support healthcare professionals in delivering optimal care for patients undergoing BMD testing in Canada.
Preamble
This practice guideline is a supplement to the Technical Standards for Bone Mineral Densitometry Reporting that was previously published in 2013. 1 Changes are outlined, where appropriate, to provide clinical guidance that is harmonized with current practice, including the Osteoporosis Canada clinical practice guidelines 2 and the International Society for Clinical Densitometry official positions for adults. 3
Introduction
The Canadian Association of Radiologists (CAR) last released technical standards on bone mineral density (BMD) reporting by central dual energy X-ray absorptiometry (DXA) in 2013. 1 The 2013 standards presented expectations for BMD testing and reporting in Canada. The CAR BMD Practice Statement Working Group undertook a revision and update of the 2013 standards, focusing on specific areas related to BMD reporting, with the intent of aligning recommendations with current medico-scientific evidence and clinical best practices, including the most recent guidelines from Osteoporosis Canada 2 and the International Society of Clinical Densitometry (ISCD). 3 Where the CAR guidance differs from that of other organizations, a rationale is provided to support the divergence.
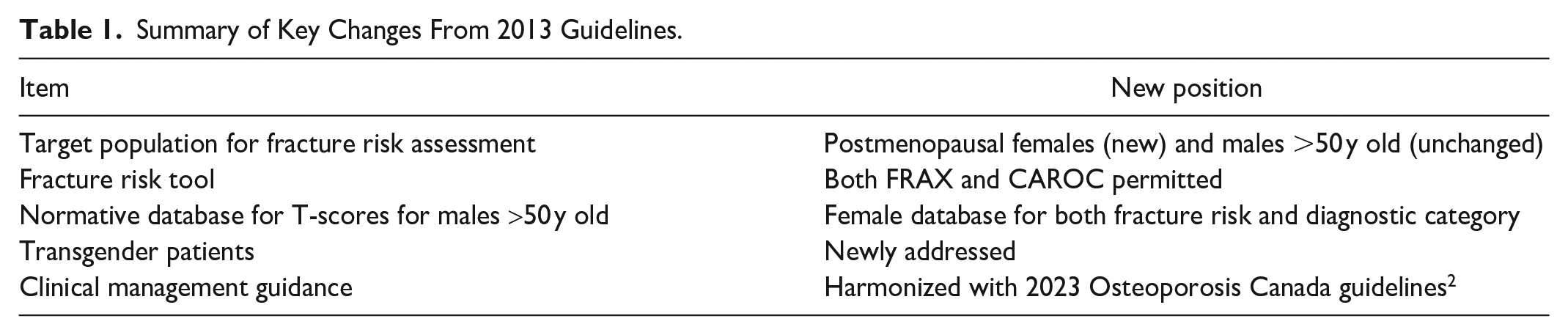
The purpose of this practice guideline is to provide current expectations for BMD testing and reporting in Canada. This practice guideline is not intended to replace the comprehensive 2013 BMD technical standard, 1 but rather to serve as an update: key changes are summarized in Table 1. The guidance presented herein was informed by a comprehensive review of the literature and based on expert consensus from the working group, as well as a harmonization of clinical approaches (ie, CAR, Osteoporosis Canada, and ISCD practice guidelines). These clinical documents are not intended as a substitute for thorough training in BMD during residency and ongoing continuing medical education (CME). The guidance provided here should apply to the vast majority of patients undergoing BMD testing in Canada. However, there will be patients with special circumstances that are beyond the scope of this document: such patients are often under the clinical care of osteoporosis specialists.
Summary of Key Changes From 2013 Guidelines.
In 2022, the CAR also began the process of updating its BMD Accreditation Program (BMDAP), under the auspices of the Canadian Medical Imaging Accreditation Council; the process is ongoing and will reflect the clinical guidance presented in this practice guideline. This document, in conjunction with the 2013 CAR Technical Standard, 1 will form part of the accreditation requirements.
Fracture Risk Assessment
Providing a 10-year fracture risk using a validated fracture risk tool is a key component of BMD reporting. The following sub-sections review aspects of determining and reporting fracture risk.
Target Population
The target population for current osteoporosis management guidelines is postmenopausal females and males aged 50 years or older, 2 and this is adopted here. For females this is a change from previous Canadian guidelines1,4 which used a female threshold of age 50 years. The CAR reporting guidance applies to all ages undergoing BMD testing, though there are differences in the reporting between younger and older patients. 1
Fracture Risk Tool
The CAR recommends either the Canada-specific version of FRAX 5 or the 2010 version of the CAROC (Canadian Association of Radiologists/Osteoporosis Canada) risk tool.1,6 This is a change from previous guidelines1,4 that endorsed CAROC in BMD reporting, at least in part as the Canada-specific FRAX software had not been widely available on BMD machines. 4 Current Osteoporosis Canada guidelines suggest the use of the Canada-specific FRAX tool, which is now widely available on BMD machines, as the preferred tool for fracture risk assessment, with CAROC as an alternative. 2
From an implementation perspective there are 2 main differences between the 2 tools. The first is the number of clinical risk factors used in the model, 6 for FRAX (when femoral neck T-score is available) and 2 for CAROC, as detailed in Table A1. The second is the output for 10-year fracture risk, which is expressed as a percent value on a continuous scale for FRAX for major osteoporotic fracture (MOF) and for hip fracture, versus MOF expressed in 1 of 3 ranges (<10%, 10%-20%, >20%) for CAROC.
Of the 2, only FRAX can be fully operationalized with the Osteoporosis Canada management guidelines, 2 which invoke a 15% fracture risk cut point in decision making for pharmacotherapy, as well as for timing of BMD and fracture risk reassessment. FRAX is now widely available on BMD machines, with the fracture risk generated by the software without user reference to graphs or charts. FRAX has been shown to provide better risk stratification than CAROC in fracture risk prediction. 7 FRAX is used by Fracture Liaison Services (FLS) and many clinician specialists, resulting in greater concordance vis a vis BMD reports that use FRAX. FRAX will be updated, with new validated risk variables added; Trabecular Bone Score (TBS) has already been incorporated into FRAX. There are no plans to curate CAROC. As such, the Working Group encourages facilities to consider transitioning to FRAX.
CAROC automatically places patients in the high risk (>20%) fracture risk category when there has been a fragility fracture of the hip or spine or more than 1 fracture event; in these scenarios if FRAX yields a fracture risk less than 20% it has to be overridden and a recommendation made for pharmacotherapy. 2 CAROC makes some allowance for a disproportionately low lumbar spine BMD, with a fracture risk of “at least moderate” assigned for L-spine T-score <−2.5 and otherwise low risk. Although this is not accommodated in FRAX, disproportionately low (<−2.5) lumbar spine, femoral neck, or total hip T-scores are incorporated into the Osteoporosis Canada management decision algorithm as discussed in the Reporting Fracture Risk section.
Determining the Input Clinical Risk Factors
The fracture risk assessment is highly dependent on the accuracy of the input clinical variables entered in the model (Table A1). BMD centres should make every reasonable effort to accurately collect these data. Potential sources include:
Glucocorticoid Dose Used in Fracture Risk Assessment
Recent systemic glucocorticoid use is a major factor in fracture risk assessment. The dose for increasing the fracture risk category in CAROC has been ≥7.5 mg/day (prednisone equivalent) for at least 90 days cumulative in the past year.1,4 FRAX 5 uses a threshold of 5.0 mg/day for fracture risk assessment, and Osteoporosis Canada 2 now uses a threshold of 5.0 mg/day for clinical management of bone health and fracture prevention, both with the same timing threshold of 90 days in the past year. As the foundations of CAROC have not changed, the working group suggests BMD sites using CAROC continue to use the ≥7.5 mg/day threshold.
Reporting Fracture Risk
Components of first-time and follow-up BMD reports have been previously outlined. 1 Current key considerations for inclusion in the fracture risk or management section of the BMD report are expanded on here.
Fragility Fractures
Fragility fractures, the clinical manifestation of osteoporosis, are intimately tied to BMD assessment. Fragility fractures are an important input in the fracture risk assessment with both FRAX and CAROC, while the 10-year fracture risk issued in the BMD report guides patient management. 2 It follows that physicians reporting BMD should be very well versed in fragility fractures. Radiologists also assess and report fragility fractures across multiple imaging modalities. A full discussion is beyond the scope of this document, but several relevant points are provided to facilitate risk assessment in BMD reporting. At essence is whether a given fracture indicates increased risk of future fractures, warranting inclusion in the fracture risk tool. Despite attempts to codify this there can be some subjectivity, and whether a given fracture qualifies as a fragility fracture may occasionally require clinical judgment. A comment explaining the rationale for including or excluding a fracture in the risk assessment should be provided in the BMD report when there is uncertainty.
Low energy fractures of the hip, spine, proximal humerus, and distal radius are generally considered fragility fractures, whereas fractures of facial bones, hands, feet, and ankles are not. Fractures of other bones have lower association with increased fracture risk but may be considered when the force would not normally be expected to lead to a broken bone. 1 Fatigue stress fractures (repetitive overuse stress applied to normal bone) and pathological fractures (eg, through metastases) are not included as they do not indicate increased risk of future fractures that should be treated under osteoporosis paradigms. The risk of a subsequent fracture is greatest within 2 years of a fracture, and FRAX and CAROC may underestimate the fracture risk in this scenario. 2
Vertebral fractures can be particularly challenging in fracture risk assessment. They are one of the most common fragility fractures 9 and they indicate a high risk of future fracture warranting pharmacotherapy for osteoporosis regardless of BMD. 2 However, many do not undergo imaging at the time of the event as only about one third of patients present clinically with back pain. 10 They may be detected on subsequent imaging performed for other reasons, yet only about one half are reported by radiologists when found incidentally. 10 Conversely, minor abnormalities which are not true fractures might be reported, using terms such as “mild wedging,” resulting in referrals for BMD and inappropriate inclusion in fracture risk assessments. The presence of a vertebral fracture has been most commonly assessed using the Genant semiquantitative method (GSQ). 11 More recently the modified algorithm-based qualitative (mABQ) approach, wherein a vertebral fracture is diagnosed based on evidence of endplate fracture or cortical buckling/breaks, has been shown to more accurately identify vertebral deformities associated with future vertebral fractures. 12 While mABQ is not predicated on a quantitative assessment, it is still recommended that the degree of height reduction be reported by radiologists as there are clinical implications of fracture grading. For example, severity of fracture (>40%), recency (within 2 years), and number (>1) of vertebral fractures may factor into a decision to initiate anabolic therapy. 2
Indications for Baseline BMD
Evidenced-based recommendations for a baseline BMD test were provided in the Osteoporosis Canada clinical practice guideline, 2 using a targeted approach incorporating age and risk factors. These are strongly endorsed by the CAR and are reproduced in Table B1.
There are some important qualifiers: Provincial health insurance plan restrictions or other local requirements may override these recommendations. The scope of the Osteoporosis Canada guidelines was postmenopausal females and males aged 50 years and older, with a focus on people with primary osteoporosis. There will be additional indications for BMD in patients with more complex medical conditions, including younger patients. The Osteoporosis Canada algorithm did not explicitly recommend a baseline BMD for management of bone health and fracture prevention in patients with previous hip or spine fracture, or ≥2 fracture events, as these patients are at established high fracture risk and pharmacotherapy was recommended. However, depending on the individual situation a baseline BMD might still be warranted to facilitate monitoring.
Recommending When to Reassess BMD and Fracture Risk
BMD reports should contain a recommendation on when the next BMD should be performed.1,3 Recommendations applicable to most patients were provided in the Osteoporosis Canada clinical practice guideline 2 and are endorsed by the CAR. These are reproduced in Table B2 for centres using FRAX. For centres using CAROC the recommendations in Table B2 are a best fit to the FRAX-based timelines. As in the consideration for baseline BMD, there are important qualifiers. Provincial health insurance plan restrictions or other local requirements may override these recommendations. There may be individual medical scenarios which warrant more frequent monitoring than provided in this general guidance.
BMD reporting physicians can provide the specific follow-up time for the individual patient, either in number of years or as a stated calendar year, or a more generalized approach can be taken, for example with the report including the relevant (FRAX-based or CAROC-based) table as part of the template. A statement should be included that earlier follow up is indicated if the patient develops secondary causes of osteoporosis, new fracture, or other risk factors for rapid bone loss. 2
Recommending Management
BMD reports should contain recommendations for pharmacologic, and potentially (depending on local practice) non-pharmacologic, interventions 3 in accordance with the Osteoporosis Canada guidelines 2 to help ensure the results of the study appropriately carry through to patient management. Pharmacotherapy initiation is particularly dependent on the results of the BMD and fracture risk assessment. Recommendations in the BMD report may be of varying detail and specificity depending on local practice. In order of ascending level of directed guidance, approaches include:
a reference to the Osteoporosis Canada guidelines
a template table reproducing the guideline recommendations (see below)
a specific recommendation for the individual patient,
all based on and referencing the Osteoporosis Canada guidelines. 2
Table B3 summarizes the pharmacotherapy recommendations based on FRAX. 2 An equivalent table cannot be generated based on CAROC due to the 15% risk used in management decisions.
Reporting Diagnostic Category
BMD reports should provide the diagnostic category (normal, low bone mass, osteoporosis) as previously recommended, 1 in keeping with current best reporting practices. 3 To avoid pharmacological intervention based solely on a densitometric diagnosis of osteoporosis, it should be clear from the report that management decisions are based on the fracture risk and T-score, not the diagnostic category, as discussed in the preceding section.
Male Patients
In the 2013 CAR Technical Standards, 1 for males aged 50 years or older the T-score used to establish the diagnostic category was based on the male normative database. As the T-score used in fracture risk is always derived from the female normative database, this meant that males were analyzed twice, once as a male and once as a female. It is now recommended that the T-score used in establishing both the diagnostic category and the fracture risk is based on the female normative database, 3 so males are only processed once, as females, to determine the T-score. Note that this refers only to derivation of the T-score: the sex-specific fracture risk then must be established, by entering as a male when using FRAX, or by using the male fracture risk chart or graph when using CAROC. Table B4 summarizes the normative databases to be used in BMD assessment. 3
Transgender Patients
As BMD assessments are dependent on the sex of the patient, an approach to addressing transgender patients is needed. An informative review of key considerations and challenges in addressing transgender patients in a BMD department has been provided. 13 In many circumstances it is not possible for the BMD staff to determine whether a transgender patient is more appropriately analyzed and reported as a female or male. The referring specialist might indicate on the requisition which sex to use in the assessment, while some centres might have a policy for analysis and reporting of transgender patients. However, in the absence of such direction, the following approach is suggested.13,14 For a patient identified as transgender, their data is analyzed by the BMD technologist, and reported by the BMD physician, using both male and female data. The referring clinician is best positioned to then make management decisions based on the data. It is emphasized that this is a suggestion in the absence of expert guidelines, and that local policy may override this. Identifying a patient as transgender can be challenging in the BMD department; referring physicians are strongly encouraged to provide this information.
For patients aged less than 50 years this issue applies only to the sex used to determine the Z-score, as T-scores are not used clinically, and a fracture risk is not provided. For patients aged 50 years and older this applies only to entering the sex in the fracture risk assessment; the female normative database is used to establish the T-score for both males and females (Table B4) as well as transgender patients, and the Z-score is not used clinically. Assessing interval change is not affected at any age as this is a measured parameter expressed in g/cm2 and is not sex-dependent.
Advanced Applications
Several advanced applications are available on DXA machines which can aid in the management of osteoporosis patients. While a detailed review is beyond the scope of this document, an introduction is provided here. BMD technologists and physicians performing and reporting these tests should undergo appropriate education and training. Key points on implementation have been issued. 3
Trabecular Bone Score (TBS)
TBS is a DXA software program that extracts gray-level textural information from the standard PA spine BMD acquisition. 15 It is associated with bone microarchitecture and provides fracture risk information that is independent of BMD and clinical factors. It has been incorporated into FRAX, providing a revised fracture risk, with greatest impact in patients whose facture risk is otherwise close to therapeutic intervention thresholds. For BMD centres using FRAX on the BMD machine, the TBS result is automatically incorporated in the provided fracture risk. If centres perform TBS but use CAROC, the TBS value should be included in the fracture risk section of the BMD report for use with FRAX by the referring clinician.
Vertebral Fracture Assessment (VFA)
Given the high fracture risk associated with vertebral fractures, many of which have not been documented on imaging, dedicated vertebral imaging has been recommended to identify vertebral fractures in certain scenarios where management may be altered. 2 This is often performed using radiographs but can be performed on a DXA machine wherein lateral imaging of the spine is performed using a dedicated Vertebral Fracture Assessment (VFA) technique. This allows point-of-care assessment without the need to return for radiographic imaging. Indications for considering lateral spine imaging (either radiographs or VFA) based on BMD parameters and fracture risk, as well as based on clinical factors, are reproduced in Table B5 from the Osteoporosis Canada guidelines. 2 It might be challenging to fully implement these in the real time workflow in a busy BMD department, and sites may wish to develop their own indications accomodating local workflow.
Full Femur Imaging (FFI)
Atypical femoral fractures (AFF) are uncommon stress fractures occurring in the femoral diaphysis between the lesser trochanter and the supracondylar flare.16,17 AFFs are associated with, though not exclusively, the use of antiresorptive medications for osteoporosis, so patients undergoing BMD may be at risk. Complete AFFs are often preceded by incomplete AFFs which can be detected on imaging, allowing interventions to prevent progression. Bilateral full-length femur imaging (FFI) can be performed on DXA machines to identify incomplete AFFs. BMD departments can establish which patients will undergo FFI. For example, ISCD suggests considering FFI in patients who are receiving bisphosphonate or denosumab therapy, or who have discontinued it within the last year, with a cumulative exposure of 3 or more years, especially those on glucocorticoid therapy. 3
Conclusion
The goal of this practice guideline is to complement and update the information from the 2013 CAR Technical Standards for Bone Mineral Densitometry Reporting. 1 To inform this update, the Working Group reviewed the current literature and relevant guidelines. Recommendations were put forward based on these sources of evidence, as well as expert consensus (especially for areas in which there was a paucity of published literature). The Working Group anticipates that this guidance document will help BMD physicians and technologists in their practice, ensuring best practice BMD and fracture risk reporting, enabling appropriate patient management and maintenance of good bone health.
Footnotes
Appendix A: FRAX and CAROC Risk Factors
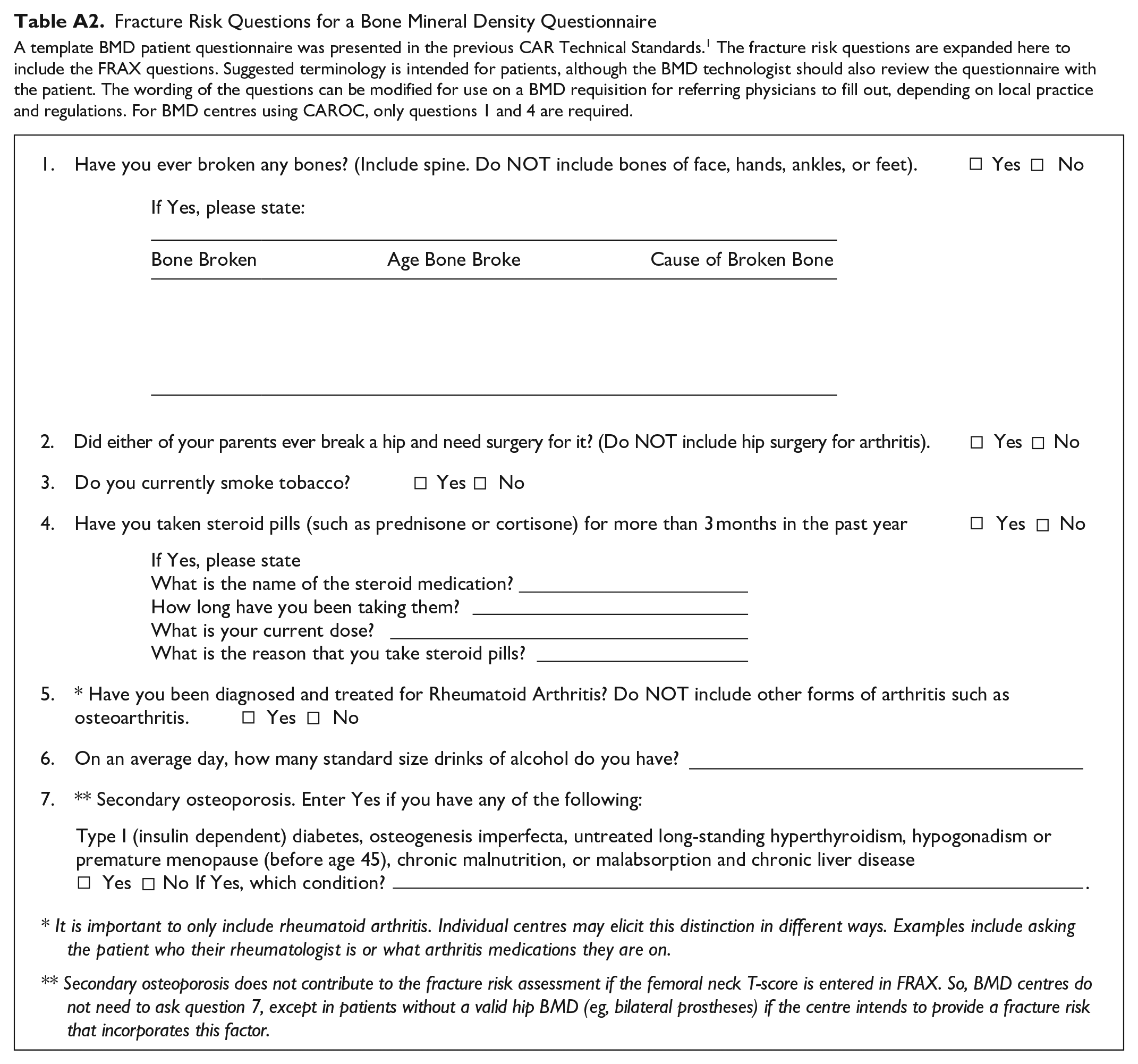
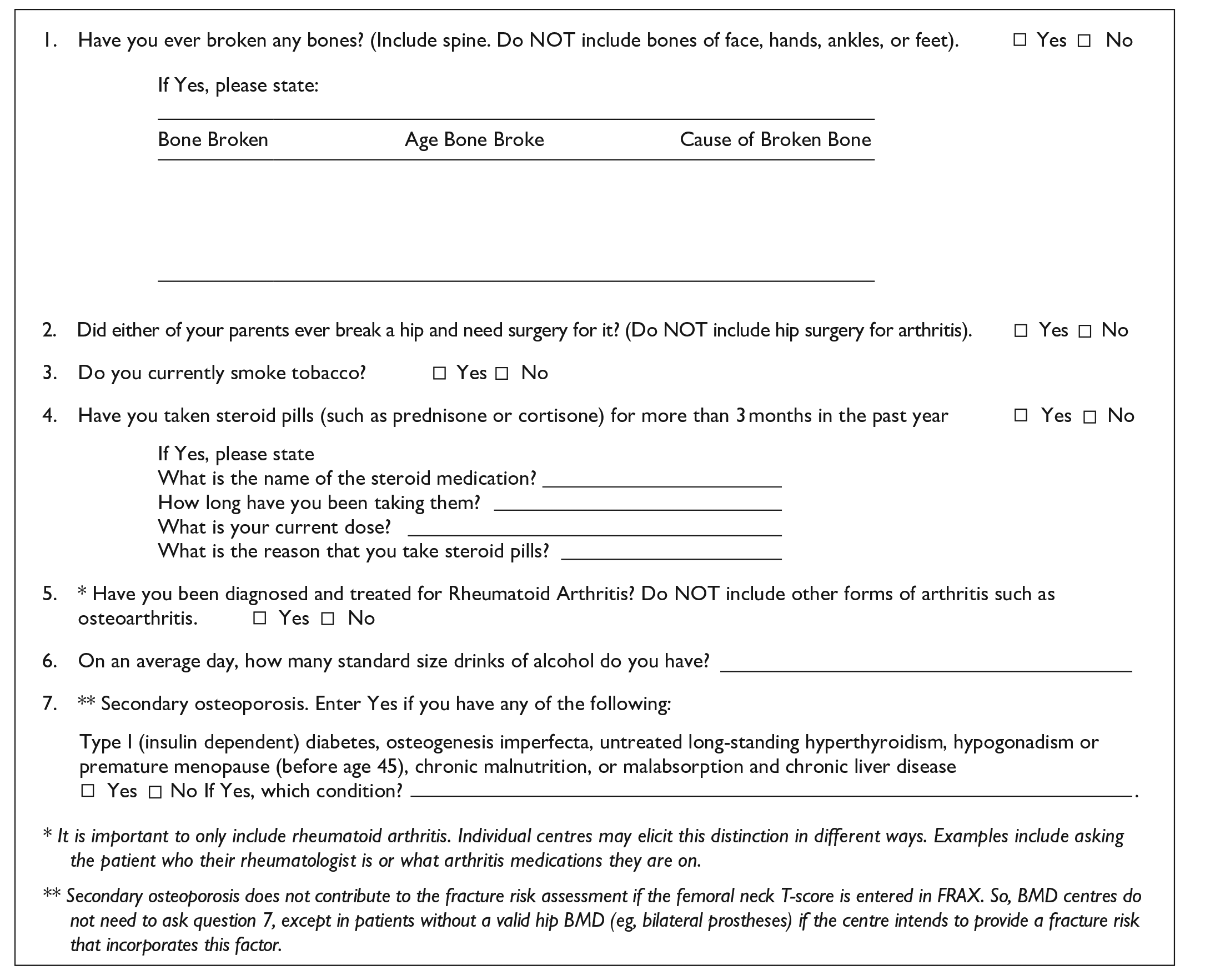
Fracture Risk Questions for a Bone Mineral Density Questionnaire
A template BMD patient questionnaire was presented in the previous CAR Technical Standards. 1 The fracture risk questions are expanded here to include the FRAX questions. Suggested terminology is intended for patients, although the BMD technologist should also review the questionnaire with the patient. The wording of the questions can be modified for use on a BMD requisition for referring physicians to fill out, depending on local practice and regulations. For BMD centres using CAROC, only questions 1 and 4 are required.
|
Appendix B
Acknowledgements
The Chair and members of the Working Group wish to thank Dr. Arvin Hariri (McMaster University, Hamilton, Ontario) for sharing his expert advice during the development of these guidelines. The Working Group would also like to thank the CAR members and representatives from Osteoporosis Canada and the Canadian Society of Endocrinology and Metabolism who took the time to review the document and to provide their feedback on earlier drafts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.