
Abstract
Keywords
Introduction
CT-guided percutaneous needle biopsy of lung lesions is a common interventional procedure performed in diagnostic radiology. This procedure is generally considered safe for most patients although complications can occur.
The most commonly reported complications include pneumothorax, parenchymal bleeding, and haemoptysis. 1 Pneumothorax is the most common of these occurring in 25.9% of cases, with the incidence of pneumothorax requiring a chest tube reported at 6.9%.2-4 Systemic air embolism is a rarer but potentially fatal complication, with a symptomatic incidence reported at 0.06%. 5
18F-FDG PET/CT imaging has recently been shown to increase the diagnostic accuracy of CT-guided lung lesion biopsy particularly for larger lesions, decreasing the rate of inconclusive results by up to 9.9%.6,7 This may decrease the number of associated complications by decreasing the need for repeat biopsy.
As well, performing a PET/CT scan prior to a CT-guided lung biopsy may also help identify potentially safer alternate biopsy sites outside of the lungs. Targeting these lesions may decrease the overall number of biopsy-associated complications even further.
The purpose of this study was to confirm the association of a pre-biopsy PET/CT scan with a higher diagnostic rate for CT-guided lung biopsy, to assess the association with post-biopsy complications, and to evaluate the potential to identify alternate safer sites to biopsy.
Methods
Inclusion/Exclusion
This retrospective observational multisite cross-sectional study was approved by our local institutional ethics review board with a waiver of patient informed consent obtained. We searched the Picture and Archiving Communication System (PACS) of 2 large Canadian tertiary care academic hospitals for consecutive patients who underwent CT-guided lung biopsy between January 1, 2020 and December 31, 2021. Only adult patients (≥18 years) were included in the search. Patients who had intervention for intra-operative lesion localization, CT-guided chest wall biopsy, or CT-guided mediastinal mass biopsy were excluded from assessment (Figure 1).
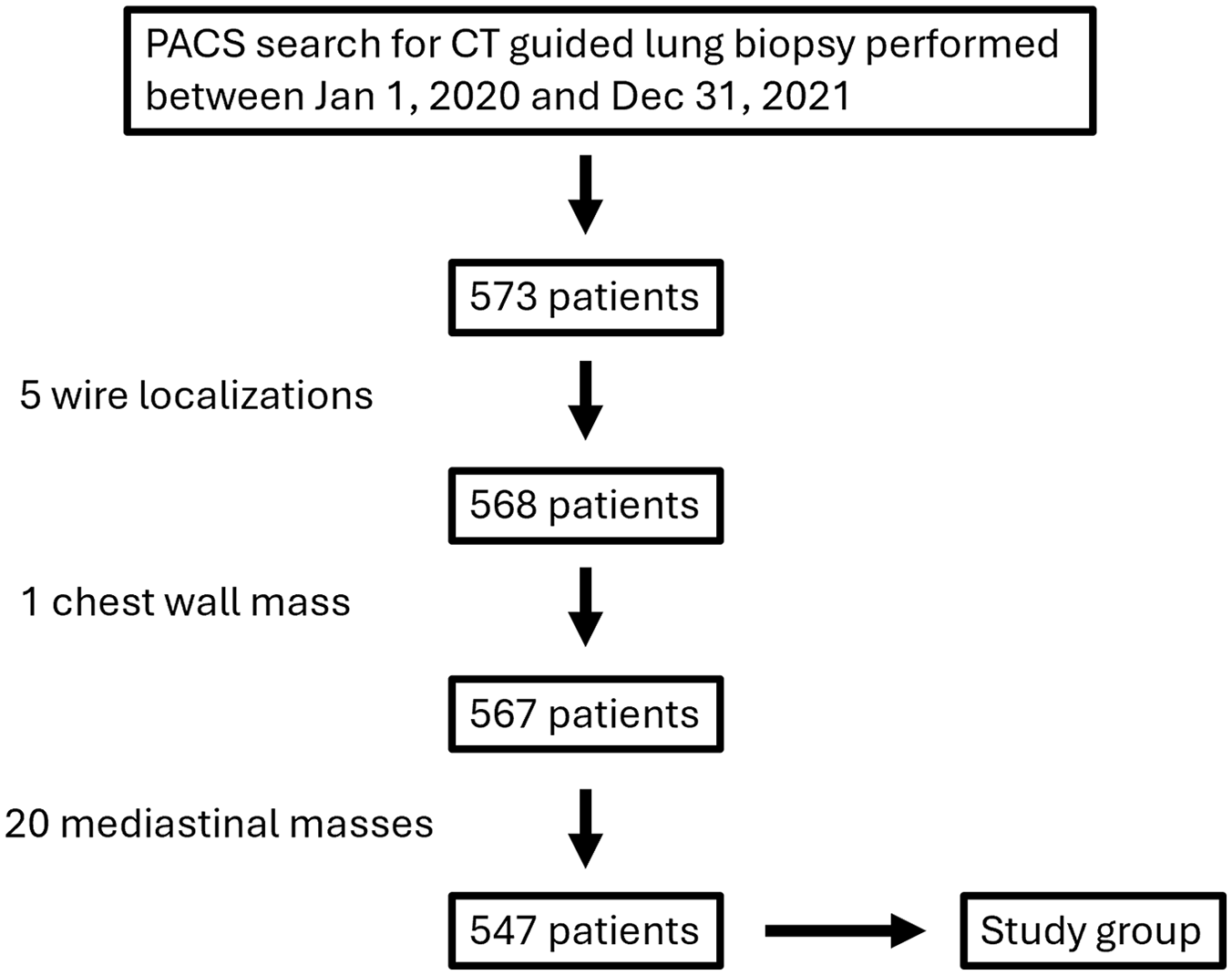
Flow chart demonstrating initial search strategy and exclusions resulting in final study population of 547 patients. Only adult patients (≥18 years old) were included.
Study Groups
The study population was subdivided into 3 study groups: those who had a PET/CT scan within 8 weeks (<57 days) prior to biopsy, those who had a PET/CT scan within 8 weeks (<57 days) after biopsy, and those who had no PET/CT scan performed within this time range. Biopsied lesions with also grouped by size (largest diameter in 3 dimensions) and categorized as lung nodules (<3 cm) or lung masses (≥3 cm).
CT-Guided Lung Biopsy Technique
Biopsies were performed by multiple (28) different licenced diagnostic radiologists with variable experience. The distribution of experience among the radiologists was uneven with 39.3% performing fewer than 5 procedures (this group accounted for 21/547 or 3.8% of the total number of biopsies performed), 17.9% performing 5 to 10 procedures (33/547; 6.0% of total biopsies), 10.7% performing 15 to 30 procedures (66/547; 12.1% of total biopsies), 14.3% performing 30 to 40 procedures (142/547; 26.0% of total biopsies), and 17.9% performing over 40 procedures (285/547; 52.1% of total biopsies) within the study period. Of note, a total of 78.1% (427/547) of the biopsies were performed by experienced radiologists completing more than 30 procedures during the study period. Trainees (residents or fellows) were involved (variable involvement) in 35.8% of the procedures. As such, there is likely some variability in specific technique for each procedure. The following is a typical biopsy protocols within these departments.
Prior to biopsy, patients are screened for risk factors associated with an increased risk of bleeding and are managed as outlined in published consensus guidelines.8,9 Informed consent is obtained and sterile technique is utilized. Many patients receive conscious sedation with intravenous midazolam (typically 1 mg) and fentanyl (typically 50 µg) under monitoring. 1% lidocaine (5-10 mL) is administered for local anaesthesia along the planned biopsy path prior to biopsy.
A co-axial technique is typically used with a 19-gauge guiding needle, 22-gauge aspiration needle, and 20-gauge core biopsy needle (typically 1 cm throw length). Using CT fluoroscopic guidance the lesion is biopsied along the approach deemed best by the involved radiologist. Fine-needle aspirates and cores biopsies are typically obtained. Cytotechnologists are present for most cases to initially assess sampling adequacy and prepare slides. If the sampling is deemed inadequate, the needle position is typically re-adjusted prior to obtaining core biopsy samples. The number of cores obtained varies depending on the radiologist, with 2 to 4 cores typical. Pathologists are not present at the time of biopsy.
The patients receive post-procedure monitoring in the diagnostic imaging recovery room (DIRR) for a minimum of 2 hours post-biopsy (range 2-4 hours). CT chest imaging (usually limited range) is typically obtained immediately after biopsy to assess for immediate pneumothorax and/or haemorrhage. Chest radiographs are typically acquired 2 to 3 hours post-biopsy to assess for delayed pneumothorax. In the case of no pneumothorax or small, stable, asymptomatic pneumothorax, patients are typically discharged home. In the case of a large pneumothorax, temporally enlarging pneumothorax, or significant clinical symptoms a chest tube may be inserted necessitating admission to hospital.
Record Review
Electronic records for all participants were reviewed to determine the presence of biopsy-related complication. CT-guided biopsy complications were classified as pneumothorax with or without chest tube placement, haemothorax, post-biopsy hospital admission, or presentation to the emergency department within 3 days of biopsy.
Electronic records for all participants were also reviewed to assess the diagnostic result of biopsy. Biopsy-associated surgical pathology and cytology reports were reviewed and the results were classified as either diagnostic or non-diagnostic. The results were further classified as malignant or non-malignant. Final pathology diagnosis was also recorded.
Alternate CT-Guided Lung Biopsy Sites
For those patients who received a PET/CT scan within 8 weeks after biopsy, the PET/CT images and reports were reviewed to determine if alternate potentially safer biopsy sites would have been identified if the PET/CT was performed prior to the biopsy. This review was completed by a single radiologist with 20 years experience reporting PET/CT and performing CT-guided lung and non-lung biopsies. To minimize bias, the investigator was blinded to complication and pathology finding at the time of this review. For CT-guided lung biopsies, potential alternate biopsy sites were recorded and divided into two categories. Category 1 sites included biopsy sites with a definitely lower risk than CT-guided lung biopsy—accessible lytic bone lesions, liver lesions, accessible lymph nodes, and other. Category 2 sites included biopsy sites with a possibly lower risk than CT-guided lung biopsy—lesions accessible to endoscopic-guided biopsy, adrenal lesions, accessible bone lesions without cortical lysis, and other. Patients who received a PET/CT scan prior to the biopsy were not included in this assessment due to the significant possibility of referral bias.
Lung Lesion Characteristics
We considered the possibility that patients with solid versus semisolid (groundglass or mixed density) opacities identified on the initial CT scans may have influenced the urgency with which to pursue PET/CT. This could potentially bias the association of pre- or post-PET/CT and the measured biopsy success rate (ie, mixed density lesions may be less likely to have a pre-biopsy PET/CT scan but be more likely to have non-diagnostic biopsy results). To ensure that these lesion features were not confounding, we reviewed the CT scans acquired during the biopsy and classified the target lesions as either solid or semisolid. To minimize bias, the investigator was blinded to the PET/CT patient group category at the time of this review. The proportion of lesion types was compared between included groups who had a PET/CT prior to biopsy versus after biopsy to assess whether this was a confounding factor.
Statistical Analysis
Acquired data was categorical and continuous. When applicable, categorical variables were statistically compared using Pearson chi square test. Continuous variables are presented as mean ± SD. Normality of continuous variable data was assessed with a Kolmogorov-Smirnov test. Normally distributed continuous variables were statistically compared using an unpaired student t-test. The Mann Whitney U test was used to assess non-normally distributed data. P-values <.05 were considered significant. All data were arranged in Excel version 16.8 (Microsoft Inc, Redmond, Wash) and were analyzed with SPSS version 20.0 (SPSS Inc, Chicago, Ill).
Results
Patient Characteristics
A total of 547 patients who underwent percutaneous CT-guided lung biopsy were included in the study. This group included 251 (46.0%) men (mean age 70.7; age range 30-92 years) and 296 (54.0%) women (mean age 69.3; age range 18-91 years).
PET/CT was performed within 8 weeks prior to CT-guided lung biopsy in 296 (54.1%) of patients, whereas 76 (13.9%) of patients had a PET/CT scan performed within 8 weeks after biopsy. PET/CT was not performed within 8 weeks before or after biopsy in 175 (32.0%) of patients.
The group who had a PET/CT scan prior to lung biopsy consisted of 273 solid and 23 semisolid lesions. The group who had no PET/CT scan within 8 weeks prior to biopsy consisted of 232 solid and 19 semisolid lesions. There was no statistically significant difference in lesion types between these 2 groups (P = .930).
For the 547 total lesions, mean size was 3.80 ± 2.34 cm (range 0.8-20.5 cm). Lesion size was not significantly different between biopsies preceded by PET/CT (3.85 ± 2.53 cm, range 0.8-20.5 cm) compared to those who did not have a PET/CT scan prior to biopsy (3.75 ± 2.24 cm, range 0.8-14.8 cm; P = .957).
Diagnostic Yield
The overall diagnostic rate of CT-guided percutaneous lung biopsy was 458/547 (83.7%). A total of 382/547 (69.8%) of biopsies yielded a malignant pathology diagnosis (Table 1). The remainder included 76/547 (13.9%) diagnostic for non-malignant pathology and 89/547 (16.3%) non-diagnostic.
Pathology of CT-Guided Lung Biopsies Diagnostic for Malignancy.
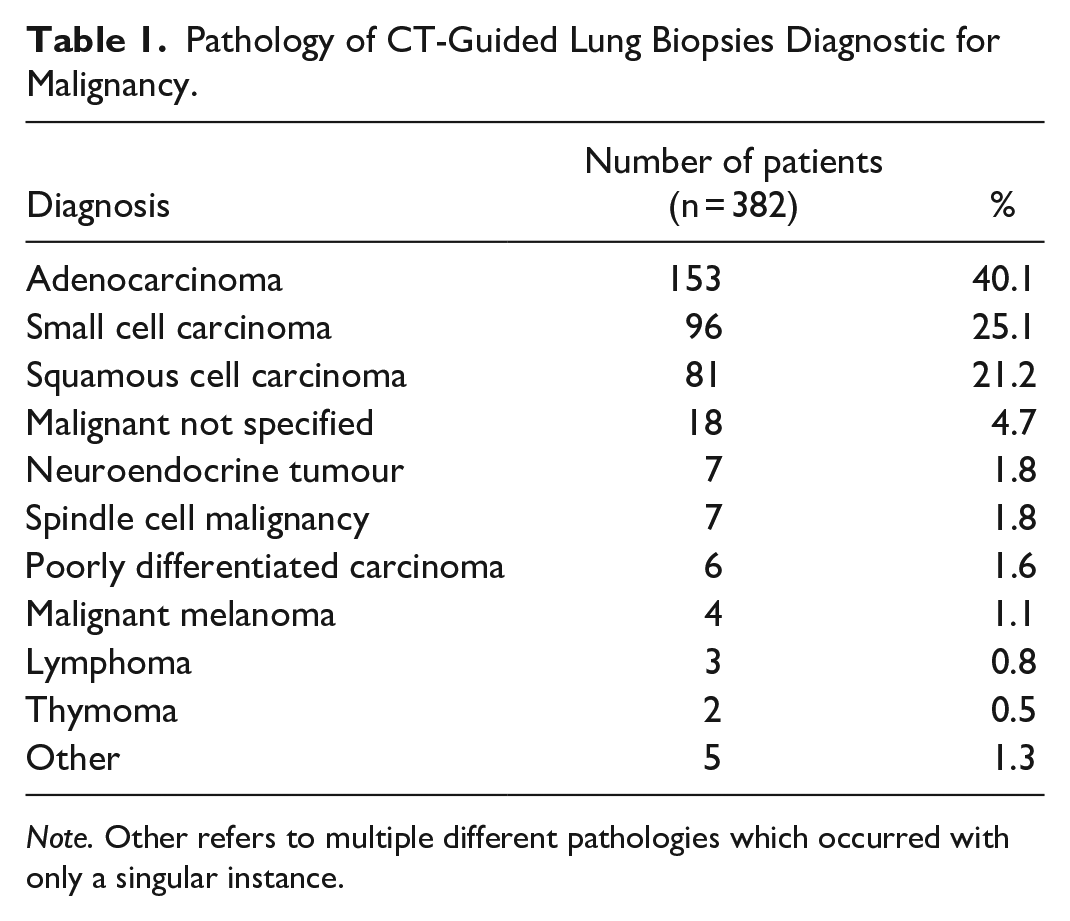
Note. Other refers to multiple different pathologies which occurred with only a singular instance.
Biopsies preceded by PET/CT had a higher rate of diagnosis (257/296, 86.8%) compared to those who did not have a PET/CT scan prior to biopsy (201/251, 80.1%; P < .05).
When categorized by size, this difference was even greater for lung masses (≥3 cm). Among the 284 lung masses, the overall diagnostic rate was 244/284 (85.9%). The diagnostic rate was significantly higher among lung masses which received PET/CT prior to biopsy (139/153, 90.8%) compared to lung masses which did not receive PET/CT prior to biopsy (105/131, 80.2%; P < .05). This suggests that performing PET/CT prior to CT-guided biopsy of lung masses (≥3 cm) increases the diagnostic yield by 10.6%.
For lung nodules (<3 cm) the overall diagnostic rate was 214/263 (81.4%). There was no significant difference between those that had a pre-biopsy PET/CT compared with those that did not for this group (P = .601).
Complications
The overall rate of post-biopsy pneumothorax was 237/547 (43.3%) with a total of 62/547 (11.3%) requiring a chest tube. There was no significant difference in the rate of pneumothorax, requirement of a chest tube, or hospital admission rate between those that had a PET/CT scan prior to biopsy and those that had no PET/CT scan prior to biopsy (Table 2).
CT-Guided Lung Biopsy Complications.
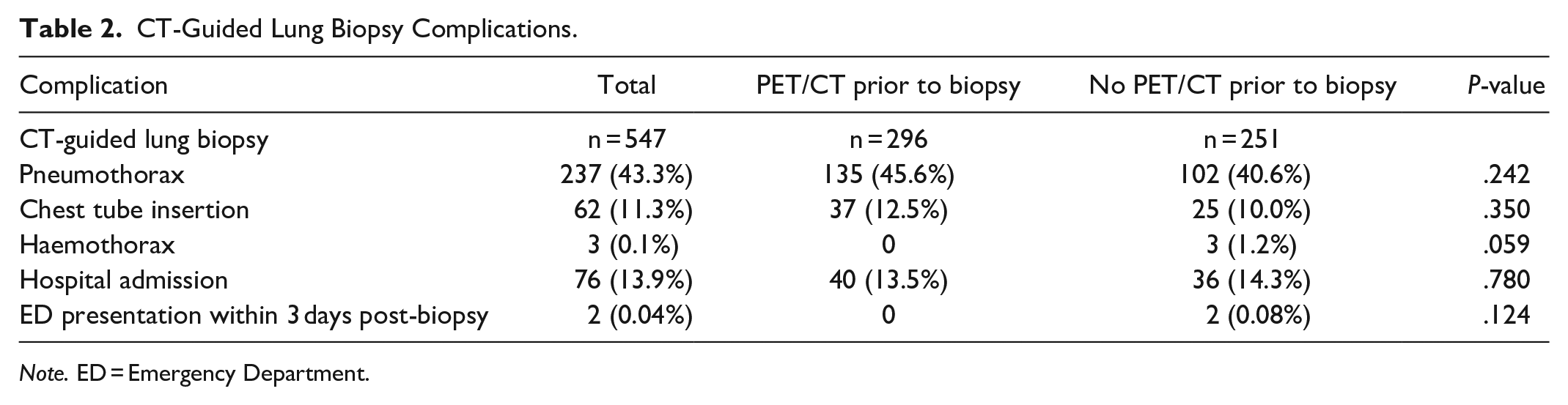
Note. ED = Emergency Department.
Lung nodules were associated with a significantly higher rate of pneumothorax (129/263, 49.0%) compared with lung masses (108/284, 38.0%; P < .05). However, there was no significant difference in the rate of chest tube insertion, haemothorax, hospital admission, nor re-presentation to the emergency department within 3 days of biopsy between these groups.
Age was not significantly different between patients who had CT-guided lung biopsies complicated by pneumothorax (70.1 ± 10.0) and those without pneumothorax (69.9 ± 14.4, P = .82).
Alternate Biopsy Sites
For the 76 patients who had a PET/CT scan performed within 8 weeks after lung biopsy, 32 patients (32/76; 42.1%) were identified to have other safer sites of disease amenable to biopsy, many with multiple sites. 22/76 (28.9%) had lesions categorized as definitely lower risk to biopsy than CT-guided percutaneous lung biopsy (category 1). 25/76 (32.9%) had lesions categorized as probably lower risk to biopsy than CT-guided percutaneous lung biopsy (category 2). Some patients had both category 1 and category 2 lesions (Table 3).
Alternate Accessible Biopsy Sites Identified on PET/CT Which Are Definitely Safer (Category 1) or Possibly Safer (Category 2) Compared to CT-Guided Percutaneous Lung Biopsy.
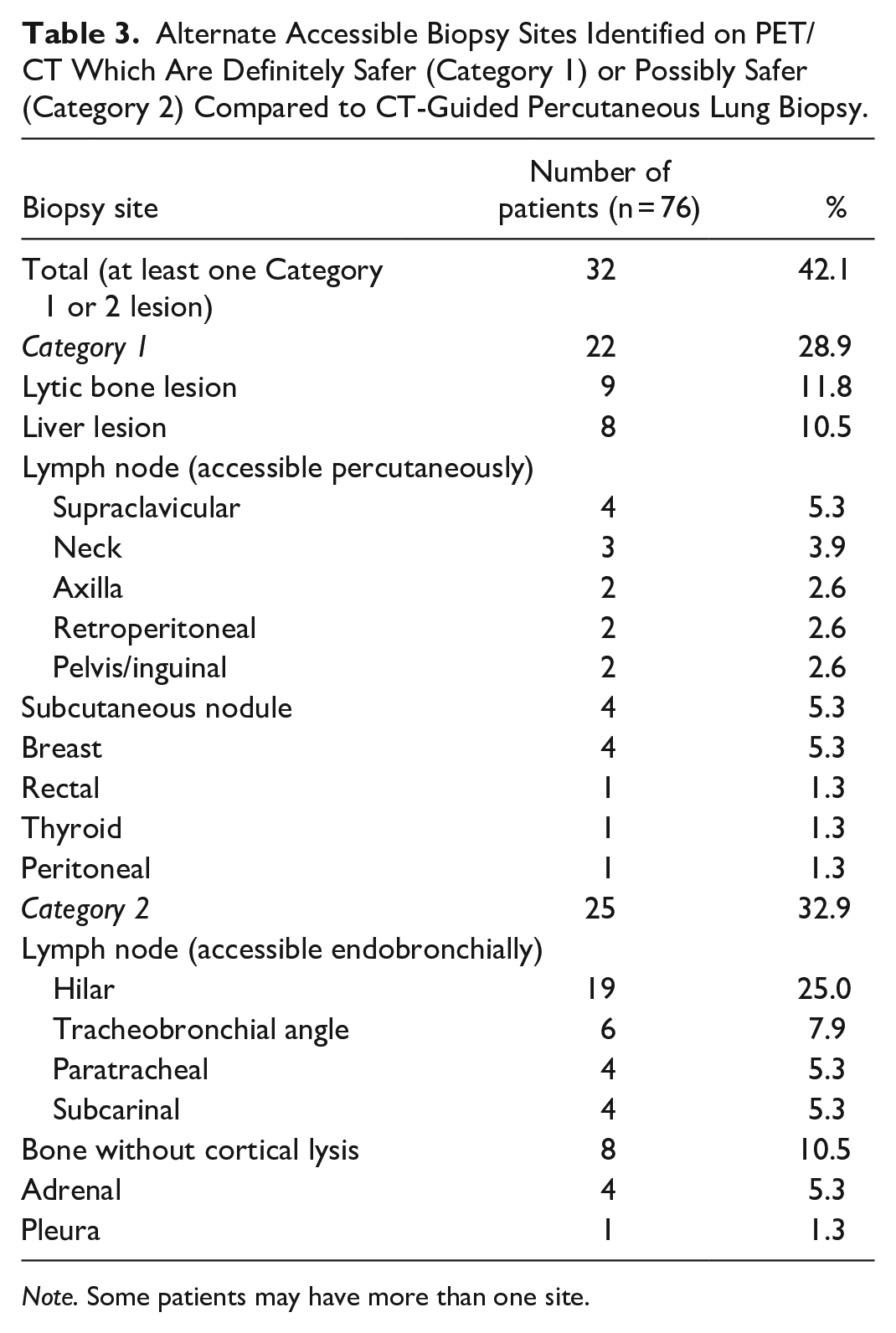
Note. Some patients may have more than one site.
Discussion
This retrospective observational study demonstrated 2 mechanisms by which a prior PET/CT may have a positive clinical impact on CT-guided percutaneous lung biopsies. First, PET/CT prior to biopsy significantly increases the rate of diagnostic success, decreasing the requirement for repeat biopsy, particularly for lung masses (≥3 cm diameter). Second, PET/CT can identify sites outside of the lungs which have an improved biopsy safety profile.
In this study, performing a PET/CT scan prior to biopsy of a lung mass increased the rate of successful diagnostic sampling by 10.6% compared to not performing PET/CT prior to biopsy. This finding is similar to literature published by other centres. Stefanidis et al recently published data demonstrating a 9.9% increase in the diagnostic success rate by performing PET/CT prior to CT-guided lung biopsy. 6 Cerci et al also demonstrated similar findings with a 8.1% reduction in the non-diagnostic rate for PET/CT guided lung biopsy procedures compared to CT guidance alone. 7 By targeting lesions or regions of a larger mass with the greatest metabolic activity, it appears that PET/CT prior to CT-guided lung biopsy significantly improves the biopsy success rate (Figure 2).
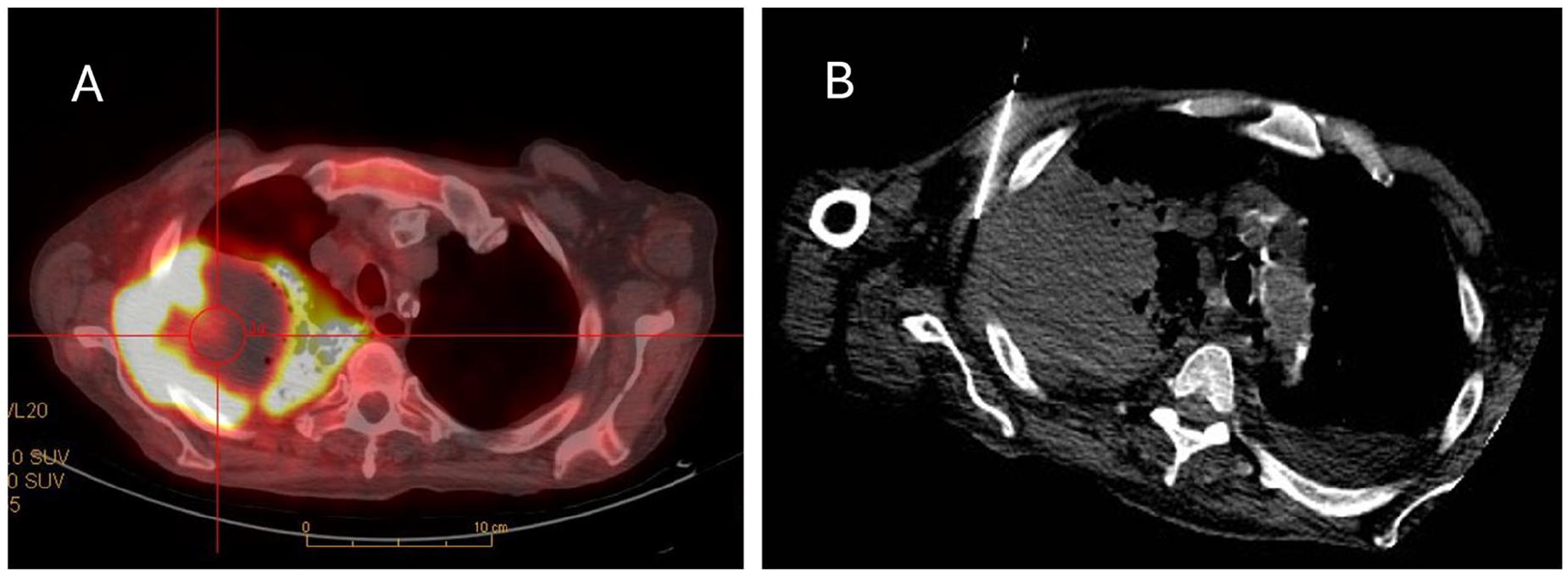
(A) Transverse image from a fused 18F-FDG PET/CT scan demonstrating a large lung mass with peripheral viable FDG-avid tumour and central non-FDG avid necrosis. The subsequent CT-guided lung biopsy (B) targeted the lateral FDG-avid margin of the mass and was diagnostic.
This study demonstrated a post-biopsy pneumothorax rate of 43.3%. While there were no reported deaths or re-presentations to the emergency department within 3 days of biopsy, a total of 62/547 (11.3%) of patients developed a symptomatic pneumothorax requiring a chest tube. A total of 76 patients (13.9%) required admission to hospital after biopsy to manage symptoms and/or chest tubes. This complication rate is somewhat higher than that previously reported in a systematic review and meta-analysis from Huo et al which demonstrated an overall pooled pneumothorax rate of 25.9% and chest tube insertion rate of 6.9% after CT-guided percutaneous biopsy. 3 The higher complication rate in our study may relate to a more complex than average patient group typically associated with tertiary care centres. Pneumothorax rates of up to 61% have been reported with patient risk factors including increased age and increased severity of underlying lung disease. 10 An impact of biopsy technique cannot be excluded although this is considered unlikely given the number of different radiologists involved in performing the biopsies in our study. Of note, there has recently been an increase in demand for core biopsies in order to characterize tumour biomarkers of importance to modern therapies. 11 This may result in a higher pneumothorax rate compared to previous data related to fine-needle aspiration only. While not represented in our series of patients, severe complications including air embolism and death can rarely occur after CT-guided lung biopsy.5,12
Given this complication profile, it is prudent to ensure there are no alternate potentially safer sites to biopsy outside of the lung prior to considering a CT-guided percutaneous lung biopsy. In this study, we evaluated 76 patients who had a PET/CT scan performed within 8 weeks after CT-guided lung biopsy. 42.1% of this population demonstrated a FDG-avid lesion at an alternate site which is potentially safer to biopsy. 28.9% had activity at a site considered definitely safer to biopsy. This data is not surprising considering PET/CT is well established as having higher diagnostic accuracy than CT alone for the detection of lymph node metastases and metastatic disease outside of the lungs.13,14 In addition to potentially improving safety, biopsy of one of these alternate sites may also provide additional clinically important information regarding metastatic disease and tumour stage.
Importantly, our study focuses specifically on evaluating patients who have had a CT-guided lung biopsy performed clinically in the presence or absence of pre-biopsy PET/CT. This evaluation demonstrates the impact of PET/CT on this specific population. Considering these 2 mechanisms (increased diagnostic rate and identification of alternate safer biopsy sites) we estimate that performing PET/CT prior to CT-guided percutaneous biopsy may decrease the overall lung biopsy rate by 28.9% to 52.7%. The lower end of this range includes only the rate of those with alternate sites identified which are definitely safer to biopsy (28.9%). The higher end of this range sums the rate of patients with definitely safer sites to biopsy, those with possibly safer sites to biopsy, and the rate of patients that require repeat biopsy due to non-diagnostic sampling (42.1% + 10.6%). When multiplied by an overall post-procedure hospitalization rate of 13.9%, performing PET/CT prior to CT-guided lung biopsy potentially decreases the need for post-biopsy hospitalization in 4.0% to 7.3% of this patient group.
There are several limitations to consider in our study. Retrospective evaluation of a clinical population potentially introduces biases. We considered that patients with semisolid (ground glass or mixed density) lung lesions may be more likely to have a non-diagnostic biopsy and less likely to have a pre-biopsy PET/CT scan but determined this potential bias was not significant. We did not control for several factors including the specific indication for the biopsy, the specific radiologist performing the procedure, the specific pathologist evaluating the biopsy, the lesion size, and the clinical characteristics of the patients. The similarity of our values to other recent publications with respect to the positive impact of pre-biopsy PET/CT on the diagnostic rate of CT-guided lung biopsy reduces the concern for these potential biases. Our study was also limited in scope, specifically assessing the impact of pre-biopsy PET/CT on diagnostic rate and safety. We did not evaluate other potentially important questions such as cost-effectiveness and long-term clinical outcomes. Finally, we assumed lesions identified on the PET/CT scans outside of the lung represent the same disease as the lung nodule/mass. This may not be correct in all cases but patients with 2 or more different synchronous tumour types likely represent a small percentage of the overall study population.
Conclusion
This study demonstrates 2 important mechanisms by which a PET/CT performed prior to CT-guided lung biopsy may decrease the overall biopsy rate and thereby decrease the rate of associated post-biopsy complication and hospitalization. First, for lung masses (≥3 cm diameter) PET/CT helps to target the site of highest diagnostic yield, increasing the diagnostic rate by 10.6%, thereby decreasing the need for repeat biopsy. Second, PET/CT can identify alternate safer sites to biopsy outside of the lung in 28.9% to 42.1% of patients (any size lesion). Given the complication rate associated with CT-guided percutaneous lung biopsy including pneumothorax (43.3%), hospitalization (13.1%), and need for a chest tube (11.3%), this study suggests PET/CT should be performed prior to CT-guided lung biopsy in most cases, particularly for masses ≥3 cm in diameter.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.