
Abstract
Introduction
Uterine fibroids, benign tumours of the female genital tract, are estimated to be found in a quarter of women in their reproductive years. 1 While these tumours are often silent, women may experience symptoms ranging from abdominal cramps, infertility, and, most commonly, bleeding which is reported in about 25% of women with fibroids. 2 In some cases, the bleeding can be so severe that it requires blood transfusion and can have a devastating impact on women’s quality of life. According to a 2016 Canadian cohort study, 4.1% of women between the ages of 20 and 49 reported having a current diagnosis of uterine fibroid, and about half of them reported suffering from moderate to severe stymptoms. 3
Besides medical management, gynaecologists are performing hysterectomies to treat patients suffering from symptoms related to uterine fibroids. While it has long been considered the definitive treatment for fibroids, there is growing interest in developing less invasive, uterine sparring options to treat fibroids, such as myomectomy. 4 For more than 20 years, another option has been available in Canada for women; Uterine Fibroid Embolization (UFE) performed by interventional radiologists (IR).5,6 Despite having a proven track record of safety and efficacy, not every eligible patient gets offered the procedure or even knows of its existence. 7
Our research aims to illustrate the present utilization of UFE in Canada and initiate a discussion with a panel of experts regarding the challenges and potential benefits associated with this practice.
Methods
We conducted an online survey study that met the criteria for institutional review board approval exemption as per CAIR policies on survey to be conducted to members. Implicit consent was considered when participants voluntarily completed the online survey and confidentiality was guaranteed. The survey was developed by 3 independent researchers (2 interventional radiologists and one CAIR staff member). The CROSS Checklist was used to write and review this paper. 8
The survey counted 16 multiple choice questions aiming at different aspects of UFE practice in Canada: patient awareness of the procedure, symptoms leading to UFE, setting in which the procedures are performed, number of UFE done at each site, patient care pre- and post-UFE, use of MRI, embolization technique, type of analgesia, and sociodemographic data (province of practice and clinical setting) about survey respondents. Two questions pertained to internal CAIR matters and will not be discussed in this article.
The survey was developed online using the SurveyMonkey platform (www.surveymonkey.com) in both French and English languages. Invitations to participate in the survey were extended to 792 members of the Canadian Association for Interventional Radiology (CAIR) across Canada. Membership includes 195 attending physicians, along with medical students, residents, technologists, nurses, and other professionals. The invitations were distributed via email through an official CAIR communication on April 5th, 2023. The survey was accessible for a duration of 28 days, during which 2 reminder notifications were issued. Importantly, there was no minimum response requirement for an individual to be considered a respondent to the survey.
Survey responses were completely anonymous, and no identifying information was obtained. Due to the limited number of participants from several regions of Canada, it was not feasible to analyze the data by province or specific region.
Data were compiled using Microsoft Excel™, and the results of each multiple-choice question were expressed as percentages. It is important to note that for certain questions, respondents had the option to select multiple answers. This accounts for the total percentage exceeding 100% for some questions.
The findings of the survey were presented and deliberated upon at the annual CAIR meeting held in Quebec City on May 26th, 2023. A panel of experts in the field, consisting of 5 interventional radiologists representing distinct provinces in Canada, one patient representative and a gynaecologist, engaged in a discussion concerning the challenges and pitfalls associated with UFE in Canada. The key insights arising from this roundtable discussion are detailed in the subsequent section of this paper.
Results
Out of 792 distributed surveys, 87 were completed, representing an 11% response rate.
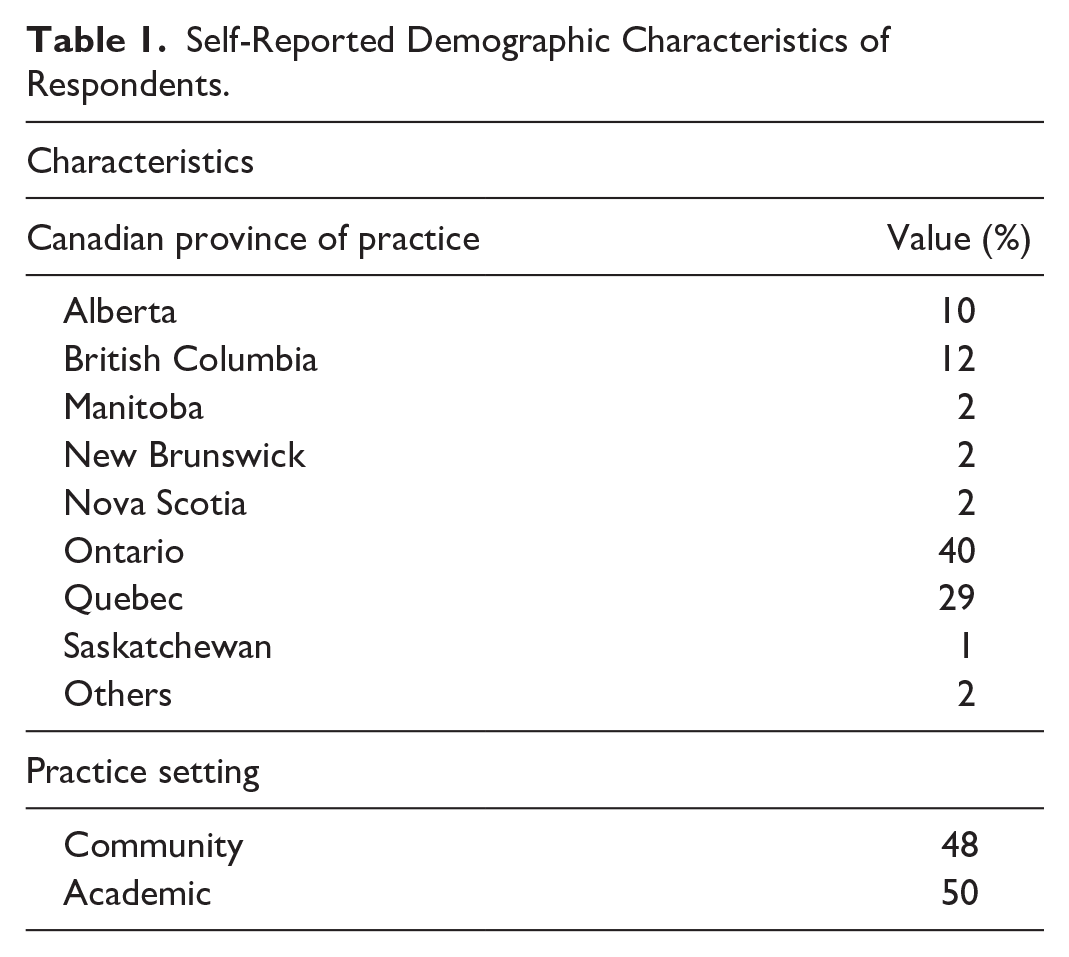
Table 1 presents the sociodemographic data of the survey respondents. The distribution aligns closely with the current membership by provinces composition of the CAIR. Respondents represented all Canadian provinces, except for Prince Edward Island, Newfoundland, and the territories. Detailed response rates for each survey question are provided in Table 2.
Self-Reported Demographic Characteristics of Respondents.
Survey Responses.
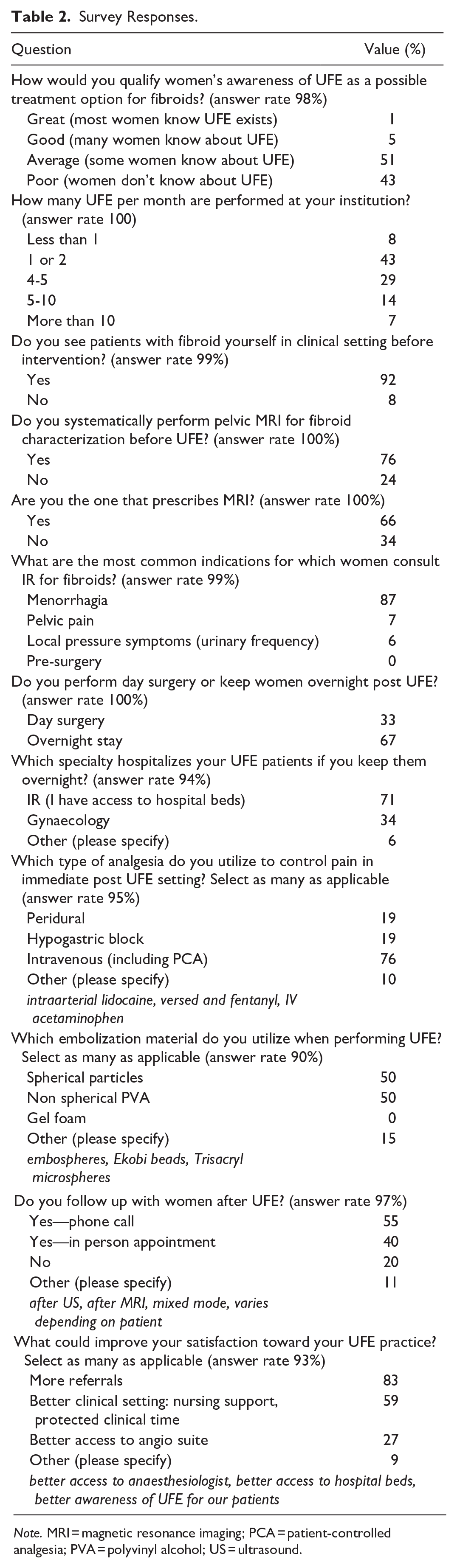
Note. MRI = magnetic resonance imaging; PCA = patient-controlled analgesia; PVA = polyvinyl alcohol; US = ultrasound.
Most, 94% (81/86), respondents assessed women’s awareness of UFE as treatment option for fibroids as either average or poor (Table 2). When inquired about the frequency of UFE performed at their institutions, 43% (37/87) indicated treating fewer than 2 patients per month. In current UFE practice in Canada, 92% (79/86) of patients are seen in clinic by IR before the procedure. Additionally, 76% of IRs requested a pelvic MRI before the procedure (Table 2). The primary indication for UFE was menorrhagia, accounting for 87% (75/86) of cases. Post-UFE, 67% (58/87) of patients were kept overnight. Of these, 71% (58/82) were hospitalized in interventional radiology units, 34% (28/82) in gynaecology, and 6% in other specialties, including internal medicine. Depending on the hospital setting, patients were sometimes admitted under more than one medical specialty which accounts for the cumulative total exceeding 100%.
For pain management post UFE, intravenous analgesia was used in 76% (63/83) of UFE cases. Epidural was used in 19% (16/83) of cases and hypogastric blocks were used in another 19% (16/83) of cases. Multimodal analgesia protocols account for the total exceeding 100%.
Regarding embolic agents, IR utilized spherical particles (50%) and non-spherical polyvinyl alcohol (PVA) (50%) during UFE procedures. Gel foam was mentioned anecdotally by a minority of respondents in the comment section of the survey. Notably, several respondents indicated the use of both spherical and non-spherical particles. This is reflected in the cumulative response rate exceeding 100% highlighting the concurrent use of these embolic agents in certain cases. Fifty-nine percent (48/81) of respondents indicated that enhancements in the clinical setting, such as nursing support, better access to the angio suite, or protected clinical time, would constitute a major improvement in their practice.
Discussion
At the 2023 annual CAIR scientific meeting, an expert panel discussed the survey results. A patient representative from a non-profit organization summarized the challenges in accessing treatment, noting a general lack of awareness about UFE: “Yes we do have to be advocates for ourselves, but it’s also very tiring when we’re dealing day to day with a battle [with fibroids] and we have to go to the doctor for 5 or 6 times, sometimes years on end before having a treatment that works.”
In their 2015 guidelines, 9 the Society of Obstetricians and Gynaecologists of Canada SOGC recommend that UFE be proposed to properly selected patients with symptomatic uterine fibroids who wish to preserve their uterus (recommendation class II-3A, ranking of the Canadian task force on preventive health care). 10 UFE is also recommended (III-B) for women with acute uterine bleeding associated with uterine fibroids. 10
However, the patient representative observed that referring physicians sometimes do not present UFE as a treatment option, a sentiment echoed by 94% of survey respondents who felt women had a poor or average awareness of UFE.
This perception is neither new nor unique to Canada. In 2010, Zurawin et al had noted a strong desire in American patients to have improved access to different therapy options for fibroid treatment, including UFE. 11 In 2017, a survey conducted by the Society of Interventional Radiology in the United States showed that 62% of women aged 18 years old and above had never heard of UFE. 12 A 2023 survey conducted on a social media group for American obstetricians\gynaecologists identified 4 possible explanations for the relative lack of popularity of UFE 13 : (1) the current American College of Obstetricians and Gynecologist guidelines which recommends UFE in a limited number of patients; (2) the FEMME trial, which suggests women who underwent myomectomies had a better fibroid related quality of life after 2 years compared to those who had UFE 2 ; (3) some concerns about fertility; (4) a potential knowledge gap about UFE amongst gynaecologists.
However, the 4-year follow-up FEMME showed no statistical difference in quality of life between myomectomy and UFE. 14 As for fertility, a 2020 review showed a post UFE fertility rate of 38.3% in women less than 45 years old expressing a desire to maintain fertility or become pregnant with many pregnancies proceeding uneventfully. 15 In comparison, fertility status post myomectomy is estimated between 53.6% and 55.9%. 16 More research needs to be conducted on the impact of UFE on pregnancy. Also, other options such as percutaneous ablation of fibroids by either thermal ablation of focused ultrasound may be preferable in certain situations. 16
In our survey, 87% (75/86) of respondents identified menorrhagia as the most common symptom leading to UFE. Severe menorrhagia can be debilitating. One of our panel members noted that many patients are unable to work and need blood transfusions while waiting for fibroid treatment. This is an area where UFE has demonstrated its clinical efficacy; clinical studies have indicated that menorrhagia showed the most notable improvement following the procedure, with 89% of women experiencing improvement in menstrual bleeding post-UFE. 17
During our panel discussion, the patient advocate suggested that multidisciplinary clinics could address a lot of frustration stemming from getting treatment in a timely fashion. In the literature, these clinics have been noted as being beneficial not only to patients, but also physicians as they can promote research and better our understanding of the short- and long-term implications of UFE and myomectomy.18,19
Panellists pointed out several challenges hindering the establishment of multidisciplinary clinics including securing IR time and staffing these clinics with nurses and technologists—issues that survey respondents also identified as problematic. Collaboration between medical specialties was also deemed crucial for optimizing UFE access.
Our survey revealed that IR is involved in post-UFE care in 80% of cases with 71% of IR hospitalizing patients under their service post-UFE. This involvement indicates a shift in IR from a consultant role to a more clinical specialty. This is also reflected in the amount of clinical exposure planned for the IR residency pathway.
Collaboration with diagnostic radiologists also plays a vital role with most IRs in Canada ordering pre-procedural MRI. This aligns with Keung et al who recommends MRI for evaluating uterine anatomy and excluding non-leiomyomata aetiologies of pelvic pain and abnormal uterine bleeding. 20 Sarcomatous uterine lesion are rare, especially for women under 50 years, with incidence of 0.08% to 0.13%. Although uncommon, embolization of uterine sarcoma could delay cancer treatment and have catastrophic consequences. 21 Hindman et al published a consensus in Radiology proposing an algorithm to evaluate for suspicious lesion. 22 While the description of sarcomas characteristics on T1, T2, DWI, and ADC is beyond the scope of this article, we encourage radiologists to familiarize with these findings. 22 Furthermore, strict reporting according to the International Federation of Gynaecology and Obstetrics (FIGO) classification is key.23,24 MRI also allows to characterize indicators of UFE success or complication; (1) large bulky uterine fibroids (showing less reduction in size and have higher recurrence rates); (2) FIGO 0-1 and 2 fibroids which may undergo sloughing or expulsion or develop superimposed infection; (3) adenomyosis which can be associated with different response to UFE; (4) fibroid enhancement (as non-enhancing fibroid will not respond to UFE). 25 Of note, there appears to be no contraindication to perform UFE for adenomyosis, but questions remain regarding recurrence rates for patient who received embolization treatment. Also, more research is being done to improve markers of UFE outcomes. 26 The ongoing QUESTA trial comparing UFE versus hysterectomy in adenomyosis treatment should provide insight to women with adenomyosis. 27
The heterogeneity noted in our survey regarding embolization materials is reflective of the equipoise regarding the different approaches. One RCT comparing non-spherical polyvinyl alcohol and tris-acryl gelatin microspheres, showed similar pain scores. 28 However, non-spherical PVA was associated with a more significant inflammatory response and more transient global uterine ischaemia. 28 At this point, no material currently in use has proven itself to be distinctly superior.29,30
Equipoise also persists regarding optimal pain management in UFE. Our survey indicated a more prevalent use of intravenous anaesthesia among most respondents; however, the scientific literature presents a less definitive picture. In 2019, Saibudeen et al concluded in a meta-analysis that no superior pain management protocol for UFE had been definitively established. 31 Furthermore, the heterogeneity of the UFE protocols reviewed, which included various combinations of opioids, non-steroidal anti-inflammatory drugs, acetaminophen, nerve blocks, and intra-arterial injections, made it challenging to draw concrete conclusions from existing research. 31
Since then, a small retrospective study involving 79 women suggested that epidural anaesthesia provided superior pain control compared to hypogastric nerve block in post-UFE patients. 32 This study also noted that peak pain intensity typically occurred 12 hours post-intervention. 32 Given that the duration of pain relief from intra-arterial lidocaine ranges between 2 and 4 hours and that from hypogastric nerve block lasts approximately 8 to 10 hours, these methods may fall short for managing pain effectively.33,34
Despite its potential advantages, our survey revealed that epidural anaesthesia is infrequently used in Canada. Further investigation is warranted to understand the underlying reasons, but limited access to anaesthesiologists is likely a significant factor. More research on optimizing anaesthesia in UFE could be conducted regarding the incorporation of triamcinolone into the hypogastric nerve block. This addition has been reported to extend pain relief for up to 33 hours post-UFE, offering a promising avenue for enhancing patient comfort and recovery. 35
The study aimed to assess current UFE practices in Canada by surveying all members of CAIR association which includes IR as well as medical students, technologists, nurses, and industry partners. The survey contained clinical questions describing daily IR work, making it challenging for non-IRs to provide meaningful responses. This may explain our low response rate as it was sent to all CAIR members, not exclusively to 195 CAIR members who are IRs. Additionally, the exact number of IRs in Canada is unknown to both the Canadian Association of Radiology and CAIR. Some IRs performing UFE may not be CAIR members, thus were not included in our study. This recruitment approach introduced reporting bias, and the insights presented in this article may not fully represent the diversity of practices across Canada. Also, the questionnaire could have been developed using a more robust methodology, using a stepwise development approach (systematic review of critical issues, focus group validation of the questions, and test-retest fidelity on a limited number of participants).
Future research should strive to collect data from a broader and more diverse demographic. A first step was taken during the CAIR panel discussion, where the involvement of both a patient representative and a gynaecologist expanded the discourse to address certain blind spots for IRs. Collaborating with gynaecologists and women’s advocacy groups for follow up study could offer valuable insights into the patient experience and gynaecological expertise, potentially leading to less IR-centric conclusions.
Conclusion
Interventional radiologists across Canada perceive women in Canada still have limited awareness of UFE.
Interventional radiologists are now involved in every step of the patient’s trajectory. The majority of women undergoing UFE are seen both before and after the procedure by interventional radiologists, with a significant proportion of these physicians hospitalizing patients under their care.
There appears to be no consensus in embolic agents and pain management protocols. Women would benefit from the more widespread use of epidural analgesia for pain management after undergoing UFE.
Footnotes
Acknowledgements
The authors acknowledge the support of CAIR in drafting, distributing, and transmitting the initial data of this questionnaire. Without their contribution, such a study would not have been possible. The authors would also like to thank the experts who contributed to the panel: Dre Alessandra Cassano-Bailey, Dr Nevin De Korompay, Dr Darren Ferguson, Dr Amol Mujoomdar, Dr Jean-Pierre Pelage, Mme Néhémie Pierre-Louis, and Dr Marie-Hélène Racicot. Thanks also to CAIR’s director Luciana Nechita.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.