
Abstract
While hydrocelectomy is the gold-standard for treating hydroceles, it poses an increased risk to patients and a greater burden to the healthcare system. Sclerotherapy is an alternative treatment for hydroceles that involves injecting a sclerosant into the hydrocele under ultrasound guidance. This literature review aimed to assess the types of sclerosants used and how sclerotherapy compares to hydrocelectomy. A literature search was conducted of MEDLINE and EMBASE using the terms “sclerotherapy” and “hydrocelectomy,” which yielded 1058 studies, of which 29 met the inclusion criteria. Only studies published after 2000 were included to ensure the most recent information was reviewed. The results showed hydrocele sclerotherapy is done using a variety of sclerosants. The most used agents are polidocanol, phenol, and STS. Of these, phenol had the highest clinical success rate of 96.5%. There was evidence for the use of atypical agents, such as tetracycline antibiotics, which yielded cure rates up to 93%, and alcohol, which was found to be especially useful for treating multiseptated hydroceles. The results comparing sclerotherapy to hydrocelectomy indicated hydrocelectomy to be a more effective method in completely curing hydroceles. However, this came at the cost of more complications. Additionally, sclerotherapy was found to be more advantageous for secondary outcomes, such as healthcare costs and burden to patients. In conclusion, this review shows that while hydrocelectomy is more effective, sclerotherapy is a valuable alternative for treating hydroceles. Due to the lack of standardization among studies, a definitive conclusion cannot be made regarding which sclerosant is best to use.
Introduction
Hydroceles are fluid-filled sacs that form around the testicle and cause enlargement of the scrotum. 1 Hydroceles can occur in males of all ages, with acquired hydroceles being more common in men over the age of 65. 2 The aetiology of hydroceles can be divided into primary and secondary. Primary hydroceles occur mostly in children and are divided into communicating and non-communicating depending on whether they communicate with the peritoneal cavity. 3 Communicating hydroceles are usually congenital and will persist for the first 1 to 2 years of life, after which they will spontaneously resolve upon closure of the processus vaginalis. 4 Non-communicating hydroceles are due to an imbalance between secretion and reabsorption of the fluid created by the tunica vaginalis and are often seen in older adolescents. 5 Secondary hydroceles occur due to trauma, malignancy, or infection. 5 In North America, epididymitis and viruses are the most frequent infectious causes of a hydrocele, however the most common cause worldwide is Wuchereria bancrofti filariasis. 6 Rarely, testicular cancer can be an aetiology of hydroceles, with about 10% of testicular tumours presenting with a hydrocele. 6
Most hydroceles are asymptomatic and do not require management. With time and increasing size, they can interfere with physical activity and sexual function causing patients to seek treatment. 7 As hydroceles progress, they can also increase the pressure around the testes which may affect the blood supply and cause spermatogenic arrest. 1 Other complications of hydroceles include pain, spontaneous rupture, or infection.7-9 Hydroceles are diagnosed by ultrasound, which shows a cystic, anechoic collection around the testis with no internal blood flow.1,10 Additionally, there may be echoes which correspond to protein or cholesterol content within the hydrocele. 10 This differs from a malignancy, which presents as a well-circumscribed hypoechoic solid lesion with internal blood flow. 11 Larger hydroceles may compress testicular vasculature and mimic testicular torsion on ultrasound. 10 If ultrasound remains inconclusive, CT or magnetic resonance imaging should be done to further evaluate the mass. 1
The gold standard of management for hydroceles is hydrocelectomy, but it comes with the risks of general anaesthesia, pain, and infection.12,13 Additionally, hydrocelectomy requires the use of healthcare resources that could be used for other surgeries. 12 This is especially true for Canada, which has limited operating-room times and long waiting lists for specialists. On average, from October 2022 to March 2023 in Ontario, non-urgent patients waited 116 days from time of referral to see a urologist and an additional 83 days for surgery. 14 The cost and complication rates of hydrocelectomy, along with the limited operating-room time in Canadian hospitals make it necessary to explore alternative treatments for hydroceles, such as sclerotherapy. The purpose of this literature review was to gain insight into the efficacy of different sclerosing agents used for hydrocele sclerotherapy. Additionally, this review aims to compare the efficacy and complications of sclerotherapy to the gold-standard treatment of hydrocelectomy.
Methods
This study used data that was publicly available without patient identifiers, and as such was exempt from review by the Institutional Review Board. A search was last conducted on June 25, 2023, of EMBASE and MEDLINE using variations of the terms: “hydrocele,” “sclerotherapy,” “hydrocelectomy,” and “interventional radiology.” Articles outlining techniques of sclerotherapy in treating hydroceles, discussing sclerosing agents, or comparing the success of sclerotherapy to hydrocelectomy were included. Only full manuscripts written in English were included. Articles written before the year 2000 were excluded from the search to ensure inclusion of the most recent information. Additionally, the references of included manuscripts were screened for other articles to include in the review. A total of 29 studies were included in this literature review. The search strategy is depicted in Figure 1 below.
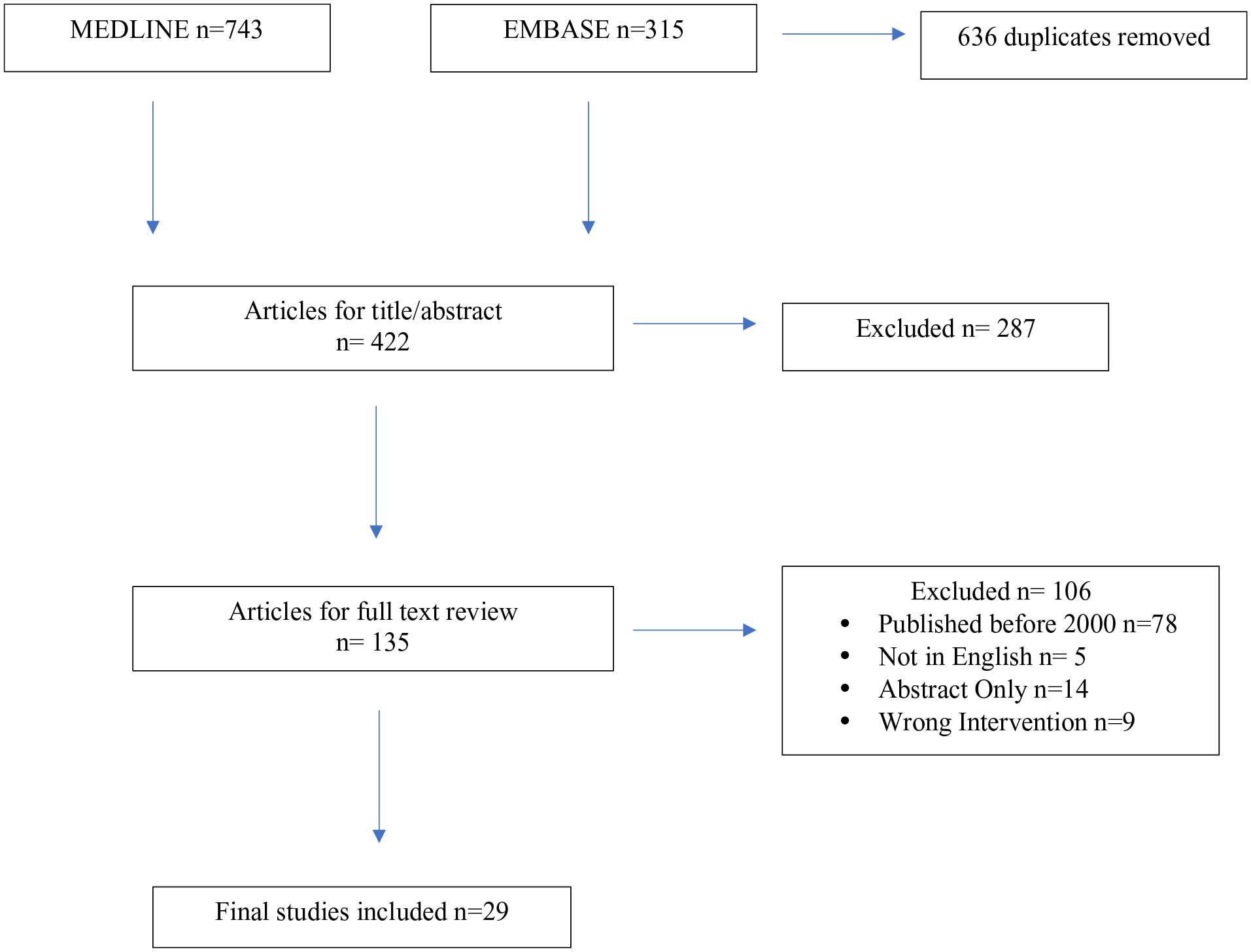
Flowchart of literature search for included studies.
Results
Sclerotherapy Procedure
The literature review results showed a similar technique for sclerotherapy across all included studies with variations in the type of sclerosing agent. The procedure starts with placing the patient in a supine position and sterilizing the affected area with an anti-septic solution, such as iodine or chlorhexidine. 15 The puncture site is identified using transillumination and confirmed with ultrasound to avoid damaging the testis.15,16 The skin is anaesthetized using a local anaesthetic, such as a 1% lidocaine solution.15,17 Then under ultrasound guidance, the hydrocele is aspirated using a needle and syringe, followed by scrotal manipulation to ensure entirety of the fluid is drained prior to injection of the sclerosing agent.15,17 After this, a sclerosing agent is injected, which remains in the hydrocele and functions as an irritant that destroys the epithelial lining of the hydrocele, thus preventing additional fluid accumulation. 18 The sclerosing agent is not aspirated after injection to allow for maximal contact with the epithelial wall and the initiation of an inflammatory reaction. The technique used at our institution is shown below in Figure 2.
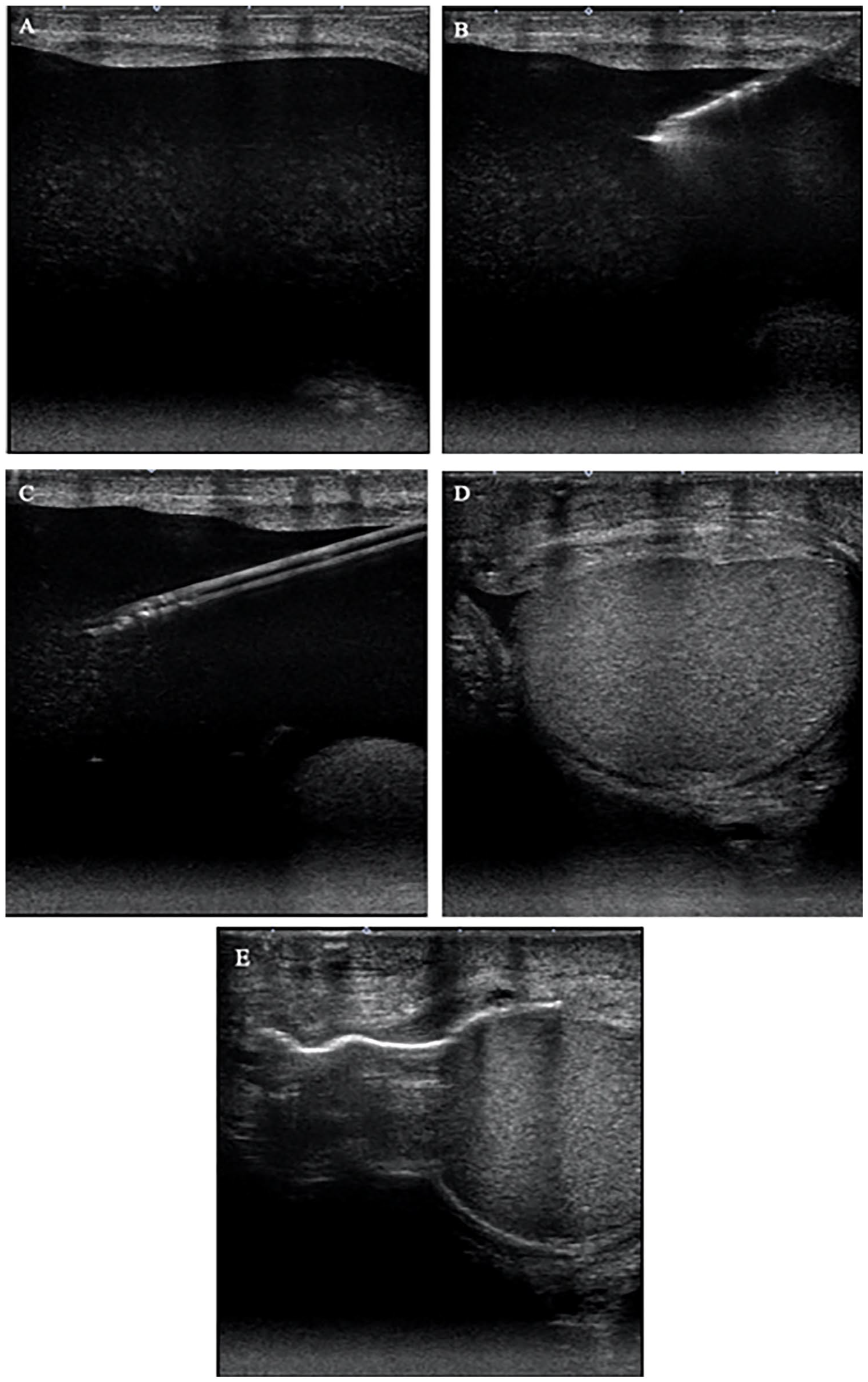
Technique of hydrocele sclerotherapy. (A) Identification of the anechoic collection around the testes. Presence of low-level echoes within collection indicate cholesterol or protein content. (B and C) Advancement of needle and cannula into hydrocele to aspirate fluid followed by injection of sclerosing agent. (D and E) Drained hydrocele with air now present within the hydrocele indicating successful injection of the sclerosant.
Type of Sclerosants
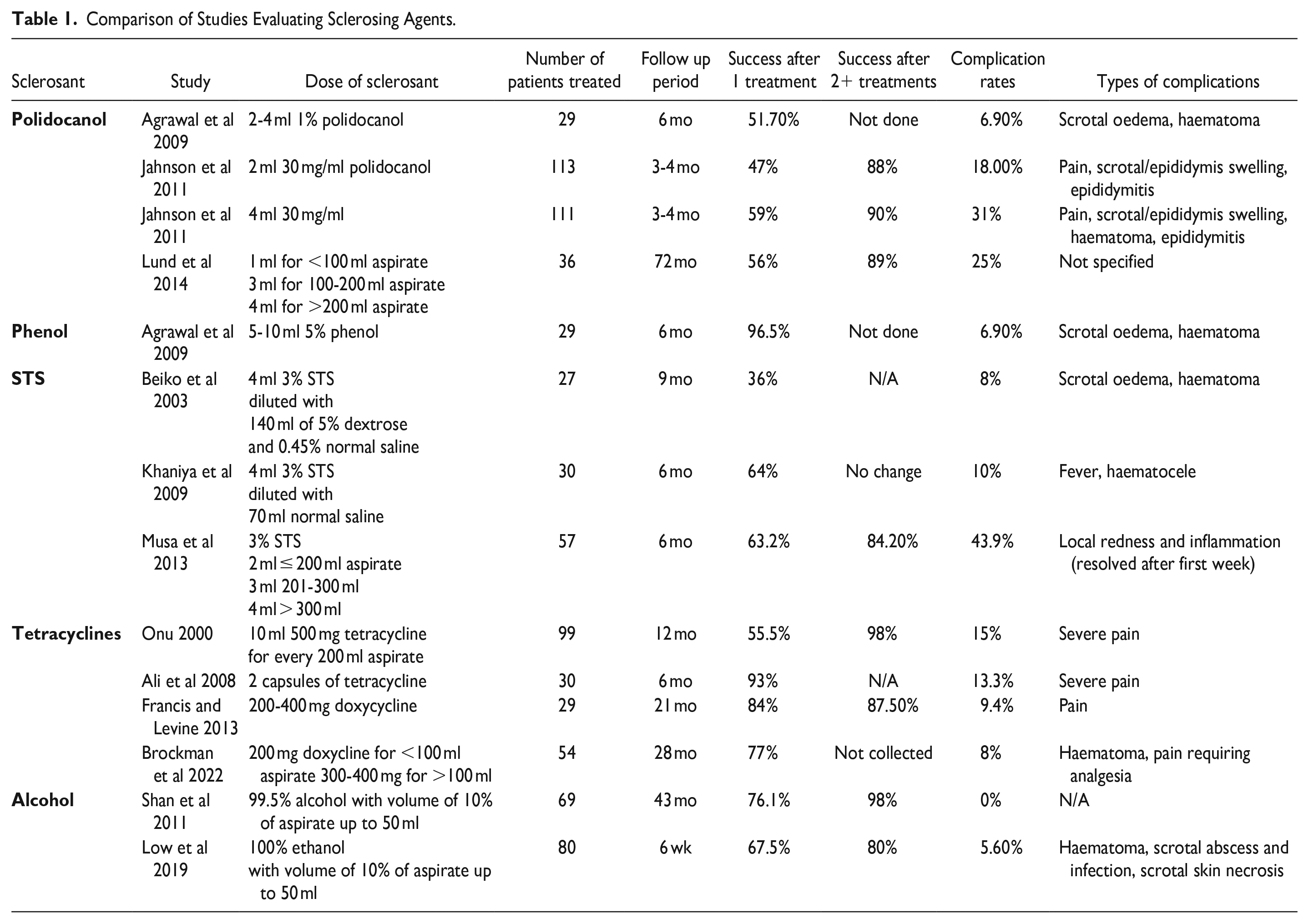
A variety of sclerosants have been used for sclerotherapy with a lack of consensus on which is most effective for treating hydroceles. The literature demonstrates the use of several sclerosants including: phenol, polidocanol, sodium tetradecyl sulfate (STS), tetracycline, doxycycline, and alcohol, each with varying levels of efficacy. 19 A summary of success and complications rates for each is depicted in Table 1.
Comparison of Studies Evaluating Sclerosing Agents.
Polidocanol
Polidocanol is an alcohol ethoxylate with the empiric formula of C30H62O10 that was originally used as a local anaesthetic until it was identified to be an effective sclerosing agent. 20 It functions by inducing a local inflammatory reaction that causes endothelial cell lysis. 20 Previous studies have indicated its success rate to be between 45% and 85%. 21 In this search, the success rates for polidocanol ranged between 47% and 56% after one treatment and 88% and 90% after 2 or more treatments.15,21,23 When polidocanol was compared to a placebo injection of sodium chloride into hydroceles and recurrence at 5 weeks was measured, it was found that only 44% of patients in the polidocanol group had recurrence versus 78% of patients in the placebo group. 21 This study indicates the advantage of using a sclerosant agent in treating hydroceles compared to simply aspirating the hydrocele. Additionally, there have been case reports showcasing the efficacy of polidocanol after failure of treatment with other agents including gentamicin and dexamethasone. 22 A 32-year-old male patient with a hydrocele attempted several treatments with 5 mg of dexamethasone and 40 000 units of gentamicin, however there was recurrence of the hydrocele within 2 weeks each time. 22 The patient then tried 3 mg of polidocanol which successfully eliminated the hydrocele with no recurrence upon follow-up at 1 year. 22
In the literature, higher doses of polidocanol have higher rates of success, but come at the cost of increased complication rates. A study done comparing 2 ml of 30 mg/ml polidocanol versus 4 ml showed there to be a better success rate in those treated with the 4 ml dose. 23 A curative outcome after the first treatment was seen in 59% of the patients in the 4 ml group compared to 47% in the 2 ml group. 23 However, 31% of patients in the 4 ml group had complications compared to 18% in the 4 ml group. Additionally, all patients with high intensity complications were in the 4 ml group. 23
The complication rates after sclerotherapy with polidocanol ranged from 6.9% to 31% across studies and consisted mainly of pain, haematoma, oedema, and scrotal infection.15,21,23 There was one reported case of severe pain requiring 6 hours of bed-rest post-procedure, after which pain resolved without the use of analgesia. 22 To minimize pain, there was a suggestion to use polidocanol mixed with lidocaine prior to injection. 22
Phenol
Phenol has been used as a sclerosant since the 1920s. 19 Phenol also functions as a caustic agent that damages the endothelial cells of the tunica vaginalis and induces fibrosis, which prevents re-accumulation of the fluid. 19 Previous studies have shown phenol to have similar success rates as hydrocelectomy. 24 Agrawal et al 15 found phenol to have curative outcomes of 96.5% with a single treatment, which was comparable to the 100% curative outcome rate seen in the surgery group with no statistically significant difference between the 2 groups. 15 When comparing phenol to polidocanol, they found the curative outcome rate of polidocanol was only 51.7%. 15 They did not find any differences in terms of pain or complications between the phenol and polidocanol groups. 15 Both groups had a complication rate of 6.9%, which consisted of scrotal oedema and haematoma. Therefore, it was concluded that phenol is a more effective sclerosant than polidocanol with similar levels of risk to the patient. This study also concluded 5% phenol to be the concentration of choice, as their success rate was higher than the previous studies that only used 2.5% to 3% phenol. 15
Sodium Tetradecyl Sulfate
STS is another sclerosant that is commonly used. It functions similarly to phenol by causing endothelial cell damage and inducing an inflammatory response that causes fibrosis. The curative outcome rates of STS ranged from 36% to 63% after one treatment.13,25,26 Across the identified studies, researchers used a solution of 3% STS that was diluted with normal saline or a combination of a dextrose and normal saline solution. The complication rates of STS ranged from 8% to 10%.13,25,26 However, one study reported erythema at the site of injection in 43.9% of patients after the procedure, which resolved within 1 week of the procedure. 26 Overall, the results indicate that STS is a relatively effective sclerosant, though not as effective as other available agents.
Tetracyclines
Tetracycline antibiotics are unconventional sclerosant agents that have been shown to be successful in treating hydroceles. They are especially useful in developing countries where conventional agents may not be readily available. 27 These antibiotics work to damage the endothelial layer of the hydrocele and then cause the subsequent deposition of fibrin by fibroblasts to prevent re-accumulation. 16 Both tetracycline and doxycycline have been used for sclerotherapy. Ali et al 27 and Onu 28 reported curative outcomes of 93.3% and 55.5%, respectively when using tetracycline.27,28 After multiple treatments, Onu 28 reported a similar final success rate of 98%. In the studies done by Ali et al 27 and Onu, 28 13.3% and 15% of patients, respectively reported severe pain requiring analgesia. There were no incidences of complications such as haematoma or scrotal infection reported, however Onu 28 reported scrotal inflammation in 23% of patients.
Doxycycline was found to have higher initial success rates after one treatment with one study reporting a curative outcome rate of 84% and another reporting a similar rate of 77% after one injection.16,29 Patients also reported minimal pain, with only 4% of patients requiring analgesia. 29 However, 4% of cases resulted in symptomatic haematoma formation. 29 Additionally, treatment was identified to be more likely to fail in patients over the age of 63 with comorbidities, such as: hypertension, diabetes, or those on anticoagulation therapy. 29
Alcohol
Alcohol is another unconventional sclerosant that has shown to be useful for treating hydroceles. The curative outcome rates for alcohol across 2 studies was found to be 76.1% and 67.5% after one injection.17,24 Alcohol is especially useful in treating multiseptated hydroceles. One case report used a combination of 6 mg tissue-type plasminogen activator (TPA) and 30 cc of dehydrated ethanol to treat a complicated hydrocele that persisted despite 3 hydrocelectomies. 30 Their results showed no recurrence of the hydrocele upon follow-up 7 months after sclerotherapy. 30 This combination is beneficial for multiseptated hydroceles because the TPA breaks down septations in the hydrocele, thus allowing the alcohol to reach the epithelium of the hydrocele and induce necrosis. 30
The use of alcohol does come with a risk of complications. Low et al 17 demonstrated a 5.6% complication rate after sclerotherapy with alcohol. Most of the complications were haematoma formation or infection, however there was one incidence of scrotal skin necrosis secondary to leakage of the sclerosant into the wall of the scrotum, and one incidence of scrotal abscess formation, thus indicating an association with more severe complications.
Sclerotherapy Versus Hydrocelectomy
Hydrocelectomy is the gold standard for treating hydroceles, however there has been a push towards using less invasive methods. 12 A recent meta-analysis looked at 5 randomized control trials comparing hydrocelectomy with sclerotherapy. Their results showed no significant differences between the 2 procedures in terms of curative outcomes, though there was a significant increase in the recurrence of hydroceles in the sclerotherapy groups. 12 Recurrence occurred in 48 of 97 participants in the sclerotherapy group, but only 4 of 92 participants in the surgery group. 12 The meta-analysis concluded that hydrocelectomy is superior to sclerotherapy for treating hydroceles, however sclerotherapy is useful for people unable to undergo surgery. 12 It should be noted that this study did not account for differences in the volumes of the hydroceles.
Similar conclusions were made by Beiko et al 13 when comparing sclerotherapy using 3% STS with hydrocelectomy. Their results showed sclerotherapy completely eradicated the hydrocele in 36% of patients. 13 This compared to a curative outcome rate of 84% in the hydrocelectomy group, suggesting hydrocelectomy is more effective in treating hydroceles. 13 There was speculation on whether increasing the concentration of the sclerosant would help with the success rates of the procedure. Khaniya et al 25 increased the concentration of STS when comparing hydrocelectomy to sclerotherapy to assess if it would yield a better curative outcome. In their study, recurrence occurred in 34.6% of patients in the sclerotherapy group versus 0% in the hydrocelectomy group, indicating that hydrocelectomy remained a more successful management option. 25 Shan et al 31 compared phenol to hydrocelectomy. Their study showed the same curative outcome rate of 97.5% for both procedures, however the patients in the sclerotherapy group underwent up to 5 sclerotherapy sessions compared to a single operation for the hydrocelectomy group. 31 Only 19 of the 40 hydroceles were cured after a single injection of phenol. 31 Korkes et al 32 showed similar clinical success rates between hydrocelectomy and sclerotherapy using alcohol as a sclerosant, with rates of 94.8% and 92.8%, respectively. However, 50% of patients in the sclerotherapy required a second procedure. 32 These results suggest hydrocelectomy is more effective for definitive management of hydroceles.
In contrast to the literature, there has been a case report that documented the failure of 3 separate hydrocelectomies in treating a hydrocele in a 4-year-old male. 18 After the third attempt, sclerotherapy with STS was trialed as a method of treatment and the hydrocele was successfully treated. 18 This case report is important in outlining the use of both methods in complicated cases where the hydrocele is refractory to treatment. It is also important for highlighting the safe use of sclerotherapy in children.
Complications
One of the advantages of sclerotherapy is it allows patients to avoid the typical risks that come with a surgical procedure, such as undergoing general anaesthesia. In the meta-analysis done by Shakiba et al, 12 they did not find significant differences in the complication rate between hydrocelectomy and sclerotherapy. This is contrary to previously published studies that demonstrated increased risk of infection, scrotal oedema, and haematoma that comes with hydrocelectomy. 33 A retrospective analysis of all hydrocelectomies done at public hospitals in Helsinki, demonstrated that complications occurred in 1 in 9 patients that underwent hydrocelectomy, with 25% of hydrocelectomy patients having an unexpected emergency room visit within 90 days of surgery. 33 In this study, 16.1% of patients had moderate or severe complications after the surgery and 32.4% of these patients required reoperation. 33 These results exhibit the significant risk of post-operative complications for patients undergoing hydrocelectomy.
Across the literature, studies show a greater number of complications for post-hydrocelectomy patients when compared to sclerotherapy. In one study, 46% of hydrocelectomy patients experienced minor complications as opposed to 0% in the sclerotherapy group. 32 In another study, 73.5% of patients in the surgery group complained of post-operative pain lasting up to 30 days after the procedure, compared to the sclerotherapy group which had no complaints of post-procedural pain. 31 One study showed there was a statistically significant increase in the number of patients with fever after hydrocelectomy, with a greater number of pyoceles and surgical site infections in this group. 25 Overall, the literature demonstrates greater incidences of complications after hydrocelectomy.
In the past, sclerotherapy has been thought to cause infertility in men. 31 However, the literature shows the effect on spermatogenesis is the same between sclerotherapy and hydrocelectomy, with an equivalent decrease in spermatozoid concentration per millilitre. 31 Additionally, studies on semen analysis after sclerotherapy showed only a temporary change in the motility and morphology of sperm, with both characteristics returning to baseline within 12 months. 24 These results indicate a lack of evidence to support the argument that sclerotherapy is associated with a greater risk of infertility as compared to hydrocelectomy.
Secondary Outcomes
Shakiba et al 12 found that the recovery time after sclerotherapy was shorter than after hydrocelectomy, allowing for patients to return to daily activities quicker. Thus, this option is often seen as more advantageous for patients. Overall, the patient satisfaction between the 2 procedures was found to be similar. Khaniya et al 25 demonstrated a patient satisfaction rate of 61.9% and 95% for sclerotherapy and hydrocelectomy, respectively. Despite the seemingly large discrepancy, the difference was not found to be statistically significant. Beiko et al 13 also found rates of patient satisfaction for sclerotherapy and hydrocelectomy to be 75% and 87.5%, respectively. Additionally, several studies have demonstrated the decreased cost of sclerotherapy compared to hydrocelectomy, with one study showing sclerotherapy costs 9 times less than surgery. 13 Other studies showed sclerotherapy to have a mean cost of 463 United States Dollars (USD) compared to 2558 USD for hydrocelectomy. 32
Discussion
The literature shows several sclerosants can be used to treat hydroceles. The most frequently used agents are polidocanol, phenol, and STS. Of the 3, phenol had the highest clinical success rate of 96.5% after a single treatment, which is the most comparable to the efficacy of hydrocelectomy. However, phenol is not universally available, and there have also been concerns of the toxicity of phenol related to systemic absorption. In one case report, a patient developed jaundice secondary to chemically induced hepatitis following systemic absorption of phenol during sclerotherapy for hemorrhoids. 34 While the literature for hydrocele sclerotherapy does not show any cases of systemic absorption when using phenol, its toxicity should still be taken into consideration and a careful technique should be used when injecting.
In situations where phenol cannot be used, alternatives like tetracycline antibiotics have been suggested. 27 Tetracyclines were found to have a similar curative outcome rate of up to 93% in one study after one treatment, and 98% in another after 2 treatments.27,28 Between these 2 studies done by Ali et al 27 and Onu, 28 there was a large discrepancy between the first-time curative outcome rate, with Onu 28 reporting a primary rate that was 38% lower than what was reported by Ali et al. 27 This could possibly be attributed to differences in the amount of tetracycline used, however an explicit dose was not documented by Ali et al. 27 Despite this, both studies provide evidence for the use of tetracyclines as a sclerosant. It should be noted that one of the complications of using tetracyclines as a sclerosant is severe pain, which was supported by the data found in this literature review.27,28 Tetracyclines also are absolutely contraindicated in situations where there is a patent processus vaginalis due to the risk of peritonitis. 28
There is also evidence for unconventional agents like alcohol, which is particularly useful in combination with thrombolytics for treating multiseptated hydroceles.30,31 While the evidence shows alcohol is an effective sclerosant, it comes with unique complications that can make it a risky option. Alcohol was the only sclerosant in the literature to cause scrotal skin necrosis secondary to leakage. If alcohol is used, it is important that it is injected carefully to avoid contact with the scrotal wall.
When comparing hydrocelectomy and sclerotherapy for treating hydroceles, the literature shows sclerotherapy has higher recurrence rates, with a reported risk ratio of 9.43 between the 2. 12 Multiple studies across the literature highlight the need for several treatments of sclerotherapy to have similar curative outcomes as hydrocelectomy.12,13,25,31 Attempts at using different sclerosants or increased concentrations of the sclerosant still did not equate to the efficacy of hydrocelectomy. 25 This can likely be attributed to the procedure of the hydrocelectomy removing the entirety of the hydrocele sac as opposed to sclerotherapy which functions by causing fibrosis to prevent fluid re-accumulation. One limitation of these studies is that there was no comparison of the volumes of hydroceles being treated and thus it cannot be assessed whether the size of the hydrocele influenced the recurrence rates in the sclerotherapy and hydrocelectomy groups.
While the higher curative outcome rate of hydrocelectomy suggests it is a more effective option for treating hydroceles, it also has a higher rate of complications and longer recovery times, thus creating a greater burden for patients.12,25 There are more reports of pain and infection after hydrocelectomy compared to sclerotherapy. While these complications can also occur after sclerotherapy, it is less commonly reported in the literature. Additionally, hydrocelectomy poses the risks that come with general anaesthesia and thus may not be a suitable option for individuals with multiple comorbidities or elderly individuals. 12
In terms of secondary outcomes, the literature shows sclerotherapy to be more advantageous than hydrocelectomy. The cost for hydrocelectomy was significantly larger than sclerotherapy due to the greater number of healthcare resources required. 12 Patients were also able to be discharged home the same day with shorter recovery times post-procedure. Additionally, there were similar rates of patient satisfaction between hydrocelectomy and sclerotherapy. 12 Therefore, indicating sclerotherapy to be a useful technique especially in countries where healthcare resources may be limited or when attempting to minimize the impact on patients.
One of the limitations of this literature review is that most of the included studies had smaller sample sizes making it difficult to assess whether the results are generalizable to the entire population. Another limitation of this review was the different follow up periods in each study with some being as short as 3 months, thus allowing for the possibility of recurrence rates of hydroceles that were not accounted for.
Conclusions
In conclusion, this literature review aimed to address which sclerosants are commonly used for hydrocele sclerotherapy and how sclerotherapy compares to hydrocelectomy. The literature shows sclerotherapy is commonly used in the treatment of hydroceles. Arriving at a consensus on which sclerosant should be used is difficult due to the lack of standardization among how a study defines a clinically significant outcome. Future studies should compare sclerosants using a more standardized study design.
Furthermore, this review has revealed that overall hydrocelectomy is more effective in treating hydroceles compared to sclerotherapy. However, sclerotherapy is advantageous for patients unsuitable for surgery. It also carries a lower risk of post-procedural complications, has shorter procedural recovery times, and offers a lower cost-burden on the healthcare system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.