
Abstract
Analytic morphomics refers to the accurate measurement of specific biological markers of human body composition in diagnostic medical imaging. The increasing prevalence of disease processes that alter body composition including obesity, cachexia, and sarcopenia has generated interest in specific targeted measurement of these metrics to possibly prevent or reduce negative health outcomes. Typical morphomic measurements include the area and density of muscle, bone, vascular calcification, visceral fat, and subcutaneous fat on a specific validated axial level in the patient’s cross-sectional diagnostic imaging. A distinct advantage of these measurements is that they can be made retrospectively and opportunistically with pre-existing datasets. We provide a narrative review of the current state of art in morphomics, but also consider some potential future directions for this exciting field. Imaging based quantitative assessment of body composition has enormous potential across the breadth and scope of modern clinical practice. From risk stratification to treatment planning, and outcome assessment, all can be enhanced with the use of analytic morphomics. Moreover, it is likely that many new opportunities for personalized medicine will emerge as the field evolves. As radiologists, embracing analytic morphomics will enable us to contribute added value in the care of every patient.
This is a visual representation of the abstract.
Introduction
Analytic morphomics refers to the accurate measurement of specific biological markers of human body composition in diagnostic medical imaging. The increasing prevalence of disease processes that alter body composition including obesity, cachexia, and sarcopenia has generated interest in specific targeted measurement of these metrics to possibly prevent or reduce negative health outcomes. 1
Morphomics has a broad potential application across numerous patient cohorts. Typical measurements include the area and density of muscle, bone, vascular calcification, visceral fat, and subcutaneous fat on a specific validated axial level in the patient’s cross-sectional diagnostic imaging (eg, at the level of the fourth lumbar vertebrae 2 ). These measurements can be taken automatically, semi-automatically or manually depending on the type of software utilized. Automatic segmentation involves software generated results without manual manipulation of the data and is currently limited in its achievable accuracy and reliability. Semi-automatic segmentation involves initial computer software segmentation with subsequent manual adjustments to ensure accuracy. Manual segmentation is the most labour intensive with the inherent limitation of increased interobserver discrepancies. The application of a density “mask” in the form of a range of Hounsfield units (HU) can be applied to a slice of the patient’s cross-sectional imaging to identify all the tissue-types of interest based on its density/attenuation (eg, fat, muscle, etc.) (Figure 1 3 ).
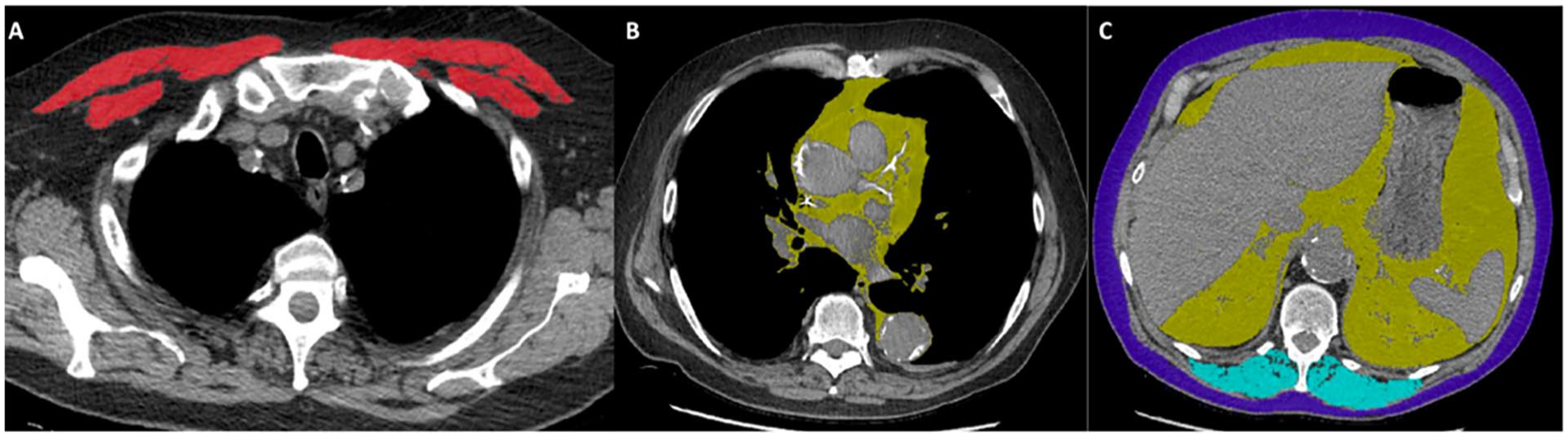
Examples of morphomic segmentation. Axial CT images of the thorax and upper abdomen demonstrating examples of morphomic software segmentation of pectoral musculature in red (A), mediastinal fat in yellow (B), visceral and subcutaneous fat in yellow and purple respectively (C), and erector spinae musculature in blue (C).
An alternative method is to use a perimeter tool to identify and draw around the anatomical structure of interest, such as the psoas muscle for example. 4 A distinct advantage of these measurements is that they can be made retrospectively and opportunistically with pre-existing datasets. This information is reproducible and can applied to many patient cohorts.
Sarcopenia is a term describing the decrease in both skeletal muscle volume and function as people age and in concert with various disease processes. Sarcopenia is defined by the European Working Group on Sarcopenia in Older People (EWGSOP) as skeletal muscle mass that is 2 standard deviations below the mean in a normal reference population. 5 Sarcopenia is a major theme of current morphomics research. It is a demonstrable risk factor for negative clinical outcomes and can be reliably utilized as a marker for patient frailty. 6 Computed Tomography (CT) imaging in lieu of traditional dual energy X-ray absorptiometry (DEXA) or bioimpedance analysis is now considered the “gold standard” with regard to muscle mass assessment. 7 Cross-sectional muscle mass in the lumbar region is strongly representative of whole-body muscle mass in healthy individuals and can be reliably used as a surrogate for whole body assessment. 8
In addition to skeletal muscle, the volume and density of visceral fat has shown correlation with important clinical outcomes. Decreasing density of abdominal visceral fat and increasing volume of pericardial and intrathoracic fat are associated with increased cardiometabolic risk. 9 The morphomic analysis of visceral fat is more accurate than traditional body mass index (BMI) measurement in the assessment of cardiometabolic risk 10 (Figure 2).
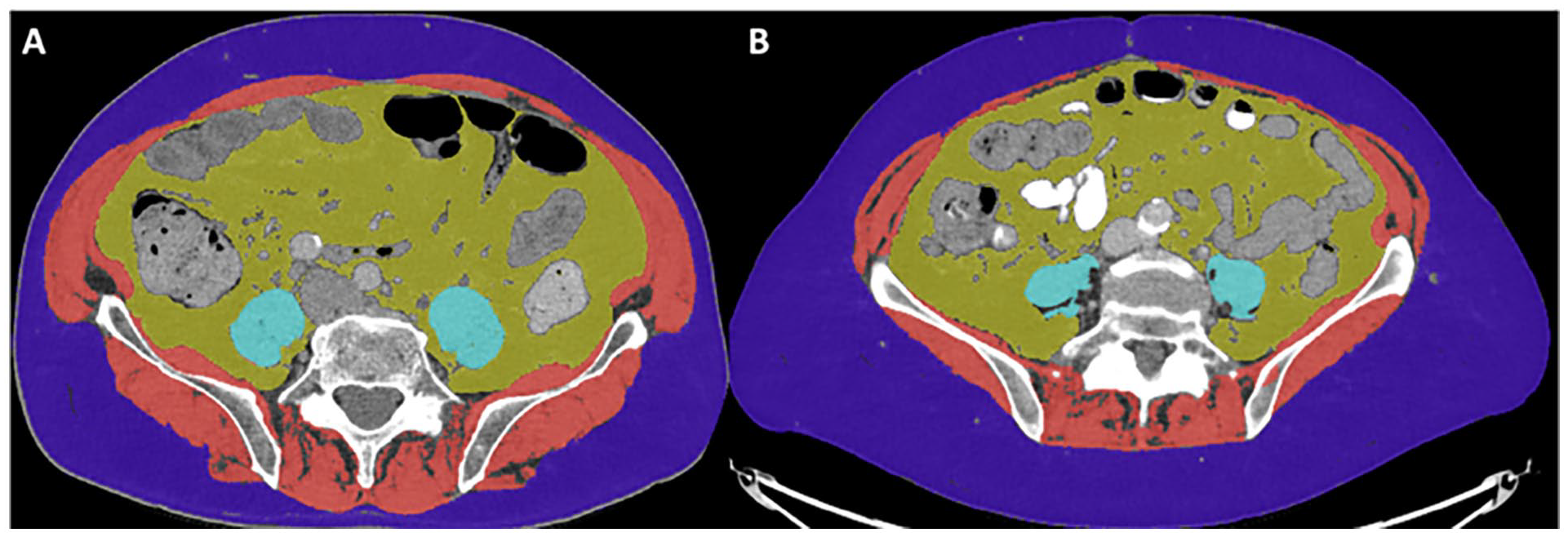
Different body composition in 2 age, sex, and BMI matched patients. Axial CT of the abdomen at the level of L4 in 2 age, sex, and BMI matched patients. Psoas muscle (light blue), abdominal wall muscle (red), pelvic muscle (red), and paraspinal muscle (red) volume and density are decreased in Patient B in comparison to Patient A. There is comparable visceral fat (yellow) between both patients. There is increased volume of subcutaneous fat (purple) in Patient B in comparison to patient A. These representative images demonstrate examples of analytic morphomic segmentation tools identifying and quantifying differences in body composition that traditional BMI measurements fail to capture.
Morphomic assessment allows us to exploit a wealth of, perhaps currently underutilized, data present in cross-sectional imaging to provide more value to patients and care providers in a wide range of clinical scenarios.
Our research group has regularly published in the field of morphomics over the past decade. Initially our work focused on gastroenterology, with in vitro accurate assessment of intracavitatory gas with further progression to study in vivo volume of intestinal gas in functional gastrointestinal disorders.11,12 Other research at that time included the assessment of subclinical changes of adipose distribution in Familial Partial Lipodystrophy type 2, visceral fat measurement to predict the severity of pancreatitis and the correlation of lung volume and density with pulmonary function tests.13 -15 In 2018 we published studies demonstrating sarcopenia as a risk factor for post-operative survival and complications after gastric and small bowel resection.16,17 We also made interesting advances in the field of orthopaedics with morphomic characterization of fracture callous formation and maturation. 18 Recently, we confirmed morphomics can be reproduced reliably and accurately using novel ultra-low dose computed tomography scans and correlated morphomics with colon cancer and interstitial lung disease outcomes.3,19,20
In this article, we aim to provide a narrative review of the current state of art in morphomics, but also consider some potential future directions for this exciting field.
Methods
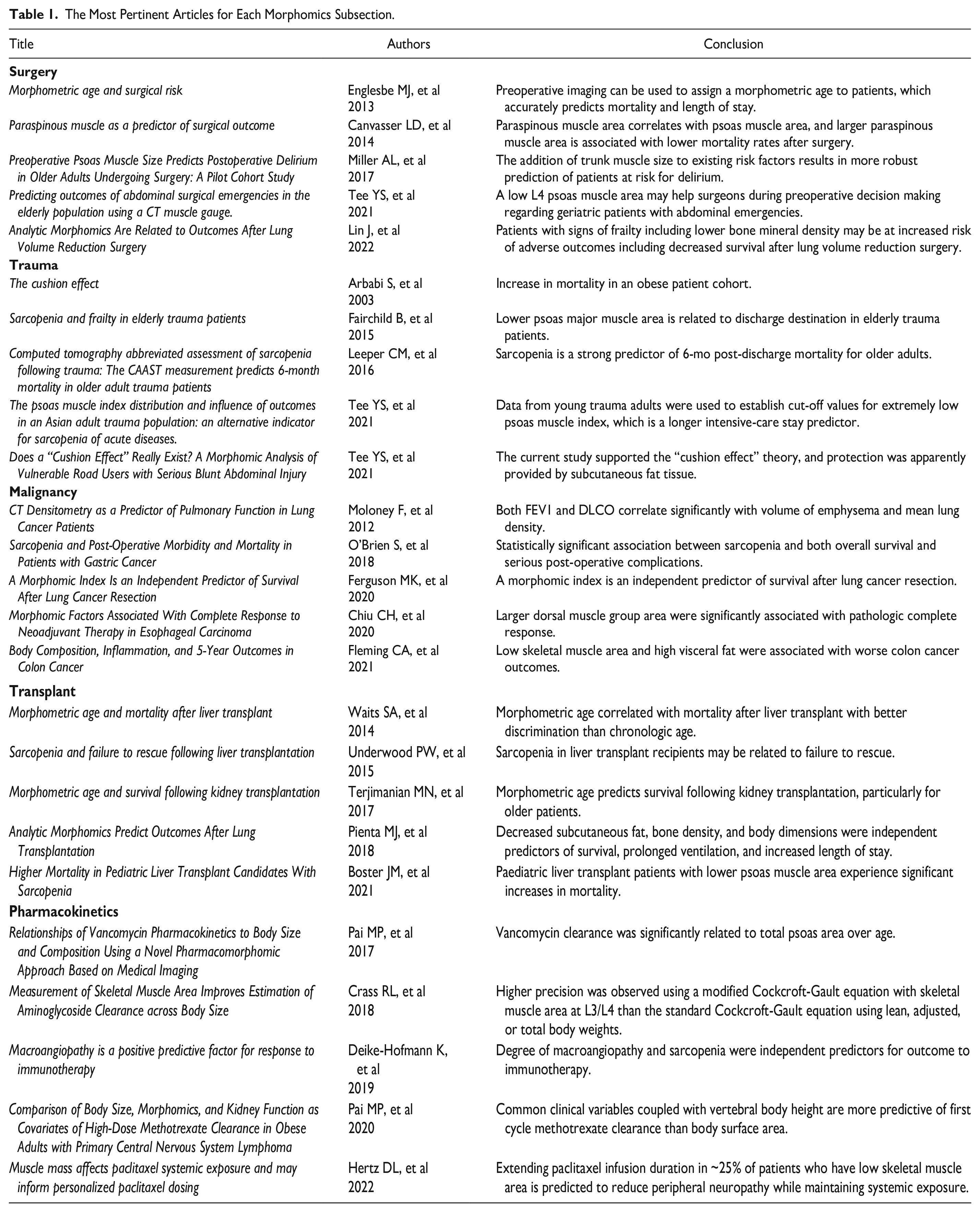
For the purpose of this narrative review, medical literature searches were conducted using PubMed, Embase, and Cochrane electronic databases. Briefly, search terms included morphomic(s), imaging biomarkers in addition to relevant MeSH terms and synonyms with the Boolean operators “or” and “and.” All English language, original, human research articles relating to the field of morphomics were identified. No timeframe limit was applied to the searches with the earliest relevant “Morphomics” related publication identified in 2010. All publication titles and available abstracts were reviewed by PWOR and JAOR independently and relevant studies were included by consensus. Additional articles were included based on our institutional expertise and knowledge of the field. This involved each author providing a list of any article they were aware of that could pertain to the goal of this review and each paper was subject to the above stated assessment and inclusion criteria. Full text articles were reviewed and a broad overview of the field of Morphomics was generated that allowed the identification of specific themes/subsections. A selection of the most relevant cited articles and their key findings are listed in Table 1.
The Most Pertinent Articles for Each Morphomics Subsection.
Clinical Applications of Morphomics
Surgery
Peri-operative risk assessment is a routine element of surgical care that incorporates validated scoring systems to objectively assess a patient’s physical reserve and ability to survive and recover from surgical intervention. 21 For example, the Estimation of Physiologic Ability and Surgical Stress (E-PASS) scoring system is a validated tool for predicting postoperative morbidity and mortality following elective gastrointestinal surgery. 22 Morphomics offers a potentially objective, and reproducible metric in this regard. Identifying the extent of age and disease related sarcopenia, vascular calcification, bone density, etc. may allow for a more accurate identification of an individual patient’s physiological reserve and help identify those who will better tolerate the challenges of post-operative healing and recovery. Morphomics has been shown to correlate with post-operative length of stay and 1-year mortality more consistently than chronological age. 23 This type of opportunistic assessment on already acquired pre-operative imaging will help identify low-risk older patients and high-risk younger patients, thereby informing the decision-making process on optimal patient selection.
The financial cost of surgical intervention is a practical consideration, and the efficient utilization of resources will ultimately result in a larger number of patients receiving high quality care. Negative peri-operative events are more prevalent in older, more co-morbid patients and increase the financial cost of these patient’s care. 24 Analytic morphomics has highlighted a significant relationship between sarcopenia (the lowest tertile of lean muscle area) and the cost of surgical care. 25 A specific targeted pre-operative intervention in this patient cohort to improve lean muscle bulk may help reduce peri-operative adverse events and subsequent financial cost. Aerobic and resistance exercises have been effective in increasing muscle bulk in elderly patients. 26
In addition to physical post-operative complications, post-operative delirium results in functional decline, and increased mortality. Psoas muscle area as a surrogate for overall frailty and patient age correlates with the development of delirium, with “low” psoas muscle area being defined as the lowest tertile of the gender standardized study population. 27 This further strengthens the novel use of morphomics as a pre-operative risk stratification tool.
The opportunistic nature of these morphomic assessments means some patients may not have abdominal imaging performed. Thoracic paraspinous muscle area correlates with psoas muscle area and is also associated with post operative mortality. 28 This allows patients with only thoracic imaging performed to avail of the benefits of morphomic pre-operative risk stratification.
Various peri-operative outcomes in different disciplines have been investigated with analytic morphomics. Subcutaneous and visceral fat distribution predicts complications of small bowel resection in Crohn’s disease better than traditional BMI assessment and correlates with general superficial post operative surgical site infections. 1 Decreased psoas muscle area is an independent risk factor for numerous post-operative complications, including; emergency operations involving elderly patients, mortality in elective abdominal aortic aneurysm repair, and mortality in perforated peptic ulcer patients.29 -31 Patients who have undergone lung volume reduction surgery for emphysema experience more negative outcomes when they demonstrate increased frailty and decreased bone mineral density on morphomic assessment. 32
There is a growing body of work in peri-operative morphomics that has the potential to generate more accurate risk stratification techniques, improve targeted pre-operative optimization programs and produce relevant post-operative recovery metrics.
Trauma
The mechanism of injury, patient age, sustaining a head injury, haemodynamic instability and injury severity score are all well recognized prognostic factors to be considered in trauma patient assessment. 33 Significant traumatic injury places demand on a patient’s physiological reserve and older frail patients have a limited capacity in this regard. Psoas muscle morphomics have been used in trauma patients as an objective surrogate for frailty and baseline fitness. Decreased psoas muscle area in trauma patients has been significantly correlated with increased likelihood of intensive care unit (ICU) admission, increased length of stay in ICU, loss of independence on discharge, and increased post discharge mortality.34 -36 Opportunistically applying analytic morphomics to trauma cross sectional imaging and highlighting patients with relevant risk factors will allow aggressive nutritional support, higher levels of physical therapy and increased safety assessment to prevent recurrent trauma.
Road traffic accidents confer high morbidity and mortality rates. 37 Widespread improvement of motor vehicle safety standards has improved safety overall, however the body composition of the patient involved in the road traffic accident is highly variable and the subject of ongoing research. Injury patterns for obese patients are different than that of normal weight patients, with one proposed hypothesis being that increased adipose tissue has a protective effect that is, the “cushion effect.” 38 Morphomic assessment of >300 trauma patients demonstrated that subcutaneous fat volume at the L4 vertebral level has been correlated with decreased serious intra-abdominal injuries, thus supporting the proposed “cushion effect.” 39 Additionally, obese patients are more at risk of extremity injuries, thoracolumbar spinal injuries, and pulmonary contusions. 40 In the thorax, morphomics of spine alignment, chest depth, and bone density in combination with statistical models have been shown to better estimate the severity of injury in adult frontal road traffic accidents over statistical models alone. 41
Road traffic accidents causing whiplash injury are one of the most common injuries in today’s society, which results in a huge economic burden being placed on the legal and medical systems. There is ongoing debate whether whiplash can be attributed to an objective pathological/anatomical process or if it is more based on cultural and psychological factors. 42 Magnetic resonance imaging (MRI) based morphomics of cervical muscle area and density has been utilized in assessment of whiplash injury to establish objective risk factors. However, systematic review of whiplash related morphomics has found current data to be heterogenous and inconsistent, with a more standardized approach recommended in future research. 43
Easily retrievable morphomic information has the potential to add value and guide initial diagnosis, emergency management, further investigations and long-term management of trauma patients.
Malignancy
Body composition is intimately related to risk of and the sequalae of malignancy. Increased BMI is associated with an overall increased risk of malignancy. 44 Subsequent malignancy related cachexia is a known consequence of the energy consuming process that is tumour growth. 45 Morphomics allows differentiation between the individual elements that contribute to overall body composition such as subcutaneous fat, visceral fat, muscle volume, muscle density, and bone density etc.
Obesity and the resulting increased baseline inflammation are proposed as a pro-oncogenic and pro-metastatic environment. In particular, high visceral fat has been shown to be markedly proinflammatory. 46 With prospective analysis of a 28 patient colorectal cancer patient cohort, sarcopenia (defined as area less than the 10th percentile of an age and sex matched population) and increased visceral fat were shown to confer an increased risk of post-operative morbidity and mortality. 20
In lung cancer patients, frailty and sarcopenia are independent risk factors for post-operative outcomes. 47 Forced expiratory volume in 1 second (FEV1) and diffusing capacity of carbon dioxide (DLCO) are traditionally used in the preoperative assessment of patients in an attempt to assess surgical risk. Morphomic assessment of lung volume and lung density correlates with the long standing traditional metrics of FEV1 and DLCO, respectively, and may have utility in pre-operative risk assessment. 15 Despite some heterogeneity in results comparing sarcopenia with surgical outcomes (likely due to ethnic variation), in a retrospective analysis of 944 patients, morphomic assessment of dorsal muscle group area, visceral fat, and trabecular bone density have been shown to be independent risk factors for survival after non-small cell lung cancer resection. 48
Analytic morphomics has been applied to various gastrointestinal malignancy related research studies. The addition of neoadjuvant chemoradiotherapy prior to oesophagectomy for oesophageal malignancy has increased survival. 49 In these patients, increased dorsal muscle group area, suggesting a lack of frailty, is associated with an increased likelihood of complete response and gives rise to the possibility of utilizing morphomics for risk stratification and treatment decisions in addition to traditional metrics. 50 Gastric malignancy carries a high mortality with gastrectomy being the curative treatment of choice. Sarcopenia in these patients has been associated with decreased overall survival and post-operative complications. 16
In pancreatic cancer in older patients, clinical geriatric assessment in combination with morphomics is predictive of outcome after surgical resection, further demonstrating the synergistic value of morphomics. 51
Overall, morphomics has demonstrated value in all stages of cancer patient care but being of particular utility for treatment related risk stratification.
Transplant
Age is often a heavily relied upon metric to decide if patients are suitable candidates for transplant surgery. However, operative risk varies widely in patients of the same chronological age. 52 Assessing individual morphomics on already acquired pre-operative CT imaging allows the combination of objective morphomics and intuitive age-related risk to quantify a “morphometric age.” In a retrospective study of 348 liver transplant patients in comparison with a 3313 patient control group, morphometric age has been shown to correlate with mortality in liver transplant patients, that is, a patient with a lower morphometric age than their age-matched peers has a decreased post-operative mortality. 53
Multiple morphomic parameters have been assessed in transplant patients. Increased visceral fat as a percentage of overall body composition correlates with increased post-liver transplant mortality. 54 Increased subcutaneous fat thickness has been shown to predict the development of new onset post-transplant diabetes in liver transplant patients. 55 “Failure to rescue” or the development of complications resulting in death post-transplant is increased in patients with morphomics confirmed psoas muscle sarcopenia (lowest tertile of muscle area). 56 In addition to the psoas muscle groups which are only available on abdominal imaging, the dorsal paraspinal muscle groups can be measured in thoracic imaging and have also shown statistical correlation with survival post liver transplant. 57 Decreased bone mineral density as a marker of patient physical decline has also been shown to be a marker of increased post liver transplant mortality. 58
Increased pre- and post-operative mortality has also been demonstrated in the paediatric liver transplant patient with morphomics defined sarcopenia. 59 Routine height and weight assessment of these paediatric chronic liver disease patients are confounded by organomegaly and stunted height with morphomic assessment of psoas muscle area helping to circumvent this limitation in assessment. 60 More accurate risk assessment will assist in identifying those patients in greatest need of a transplant and thereby, may potentially reduce organ waiting list mortality.
In lung cancer, the selection process of patients who receive a lung transplant is of vital importance with effects on waitlist and post-operative mortality. Psoas muscle area is significantly associated with less time in intensive care after lung transplant surgery. 61 Decreased post-lung transplant mortality and decreased length of hospital stay is associated with increased subcutaneous fat volume and bone density. 62 Again, analytic morphomics can play a role in transplant patient risk stratification and selection.
Morphomics has also been used to establish a “morphometric age” in renal transplant patients and is an independent risk factor for mortality. 63 These measurements can help identify patients who are at increased risk of post renal transplant diabetes. 64
Patient selection to receive an organ transplant is clearly of paramount importance in the context of utilizing scarce resources in the most effective manner. Additional reliable information to aid in this process is welcome.
Pharmacokinetics
Traditionally, dosing of some medications has been based on patients’ body weight as it is a simple and reproducible metric to obtain. The combination of height and weight to establish a BMI score is not an accurate assessment of whole body composition. 65 Other metrics such as ideal body weight and adjusted body weight are mathematical transformations of height and weight and do not incorporate known factors that contribute to body composition (eg, age and ethnicity). 66 Body composition effects medication distribution and clearance. 67 Medication dose, safety, and efficacy may be optimized with individual morphomic assessment of already obtained diagnostic cross-sectional imaging.
Aminoglycosides are a group of commonly prescribed antibiotic medications with a weight-based dosing recommendation. The volume of drug distribution and drug clearance is based on body weight and renal function respectively. In the current context of increasing population obesity, this dosing paradigm has come under scrutiny. Morphomic skeletal muscle assessment will allow individual analysis of patient body composition and may help inform dosing decisions. 68
Paclitaxel is a commonly prescribed chemotherapeutic agent that is dosed, based on body surface area and the general dosing principle is based on providing the maximum dose tolerable by the patient whilst minimizing potential side-effects. Peripheral neuropathy is a common dose limiting toxicity. 69 Obese patients have been shown to receive less effect from body surface area chemotherapy dosing, suggesting individualized morphometric body composition analysis may improve patient outcomes. 70 Hertz et al demonstrated that adjusting paclitaxel infusion timing in patients with decreased psoas muscle area (defined as <7080 mm2 of skeletal muscle mass at the T11 vertebral level) can allow patients to experience less peripheral neuropathy while maintaining adequate systemic exposure. 71
Immunotherapy augments the body’s immune system in the treatment of malignancy. Morphomics has been used to identify surrogate markers for the patient’s immune system that is, total vascular plaque index (abdominal aorta) and psoas muscle density. These radiological biomarkers (ie, macroangiopathy and sarcopenia) are independent risk factors when considering immunotherapy outcome. 72
High dose methotrexate is required to treat primary central nervous system lymphoma. Interestingly, the pharmacokinetics of methotrexate do not appear to differ in obese and non-obese patients. Vertebral body height (a metric reliably correlated with kidney size) and kidney function estimation variables have been shown to predict clearance of methotrexate and can inform dosing regimens. 73
The prospect of individual patient dosing based on accurate body composition assessment is of great interest and may lead to improved efficacy and tolerability of medication-based treatment.
Miscellaneous
The various broad applications of analytic morphomics demonstrates its dynamic and promising utility for patient care.
In orthopaedics, morphomic analysis of tibial fracture callous density and callous volume on low dose CTs has allowed objective and reproducible results with regard to individual patient healing and structural integrity of the developing callous. 18 This further advances the concept of increased individualization in patient care.
For respiratory physicians, idiopathic inflammatory myopathies can result in the development of interstitial lung disease where early detection of disease progression allows early intervention and possibly improved clinical course. An increase in skeletal muscle area with reduction in density suggesting overall reduction in muscle quality has been shown in a retrospective cohort morphomic assessment of 31 patients and may be reliable in initial assessment and management. 3
Acute pancreatitis is a common emergency department presentation with various aetiologies. Increased intrabdominal visceral fat has been shown to predict increased severity of acute pancreatitis and the subsequent development of systemic complications. 13
In gastroenterology, accurate assessment of in vitro intracavitary gas volume has been demonstrated with CT morphomics with subsequent development of specific HU reference ranges. 11 Subsequent research expanded on this study and the volume of intestinal gas has been assessed in vivo in functional and organic gastrointestinal disorders. No significant difference in gas volume between functional and organic gastrointestinal disorders was identified. 12 These 2 studies highlight the transition of morphomics from laboratory-based investigations to clinical applications.
In rare conditions such as, familial partial lipodystrophy type 2 which is characterized by lipohypertrophy, lipoatrophy, insulin resistance and early cardiovascular disease, quantitative whole body MRI assessment can help demonstrate the subclinical changes in fat distribution and guide best medical therapy. 14
With regard to imaging technique, the reduction in radiation dose delivered to the patient while maintaining diagnostic integrity is of increased interest in the context of ever-increasing numbers of diagnostic imaging studies being performed. Body composition, specifically volume of adipose tissue, has been shown to be a strong predictor of radiation dose to the patient. 74 Technological advances have allowed the integration of iterative reconstruction as a method of achieving ultra-low dose CT scans. O’Mahony et al demonstrate comparable and reliable morphomic metrics can be obtained from novel ultra-low dose CT scans. 19
Upper limb lymphoedema is a debilitating condition secondary to abnormal lymphatic drainage. There is no gold standard measurement of arm circumference to assess current disease severity and changes following therapy. Horbal et al demonstrated analytic morphomics is comparably accurate to a manual tape measure and raises the possibility of morphomics becoming the gold standard measurement tool in this patient cohort due to its precise and repeatable nature. 75
Abdominal aortic calcification is a known risk factor of cardiovascular morbidity and mortality with challenges in its accurate assessment including subjectivity and cost. 76 Morphomics is a potential novel measurement tool than can be utilized in non-contrast and contrast enhanced studies to reliably measure abdominal aortic calcification, thus contributing to patient risk assessment. Increased morphomic abdominal aortic calcification has been correlated with increased Framingham risk scores, again supporting its use as a cardiovascular risk stratification tool. 77
Limitations of this study include the heterogeneity of the publications included, that is, the studies have different sample sizes, research methods, and research aims. Additionally, a large proportion of the data described in this study is retrospective in nature. There is inherent heterogeneity in manual segmentation and morphological indices measured at a single vertebral level. These limitations are to be expected in the context of a relatively novel medical field with homogenous prospective data now required.
Conclusion and Future Directions
Morphomics has transitioned from a novel academic pursuit to a growing evidence base of clinically relevant information with potential for translational impact on patient care. Potential future utility lies in incorporating validated morphomic metrics into every radiology report, thereby providing useful information for physicians deciding on various elements of patient care. Patient care will become more individualized with objective metrics that are intuitive in understanding.
Morphomics may allow greater understanding of normal physiological and pathological processes with a potential for the growing field of artificial intelligence to be integrated, with a view to automatic output of relevant morphomic parameters. A recent article has demonstrated this point whereby a combination of deep convolutional neuronal networks and threshold-based segmentations from spectral detector contrast enhanced abdominal CT enabled accurate analysis of body composition. 78
A key component in the successful translation of analytic morphomics to the clinic is the establishment of a range of normal morphomic values for the reference population of interest. For example, a research group at the University of Michigan in the United States has developed a database of approximately 6000 adult patients, primarily imaged due to trauma, as a proposed baseline reference of normal morphomic parameters. This database is titled the Reference Analytic Morphomic Population or “RAMP” and has aspirations of also becoming a reference point for specific diseases processes in the future. 79 A paediatric (PRAMP) database of approximately 2500 patients has allowed the development of baseline normal reference growth parameters in children in the form of psoas muscle area, trabecular bone density, and visceral fat. 80 These proposed reference parameters for “normal” baseline morphomics are subject to the previously mentioned limitations of analytic morphomics and require ongoing critical evaluation with regard to accuracy and clinical utility.
The realization that simple quantitative parameters extracted from routine imaging studies could impact patient care, catalyzed the development of the morphomics field. As shown herein, imaging based quantitative assessment of body composition has enormous potential across the breadth and scope of modern clinical practice. From risk stratification to treatment planning, and outcome assessment, all can be enhanced with the use of analytic morphomics. Moreover, it is likely that many new opportunities for personalized medicine will emerge as the field evolves. As radiologists, embracing analytic morphomics will enable us to contribute added value in the care of every patient.
Footnotes
Abbreviations
BMI Body mass index
CT Computed tomography
DEXA Dual energy X-ray absorptiometry
DLCO Diffusing capacity of carbon dioxide
FEV1 Forced expiratory volume in 1 second
HU Hounsfield unit
ICU Intensive care unit
MRI magnetic resonance imaging
Author Contributions
Conceptualization, P.W.O’R. and J.A.O’R.; methodology, P.W.O’R. and J.A.O’R.; writing—original draft preparation, P.W.O’R.; writing—review and editing, J.A.O’R., M.M.M., and D.J.R.; supervision, M.M.M. and D.J.R. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.