
Abstract
This is a visual representation of the abstract.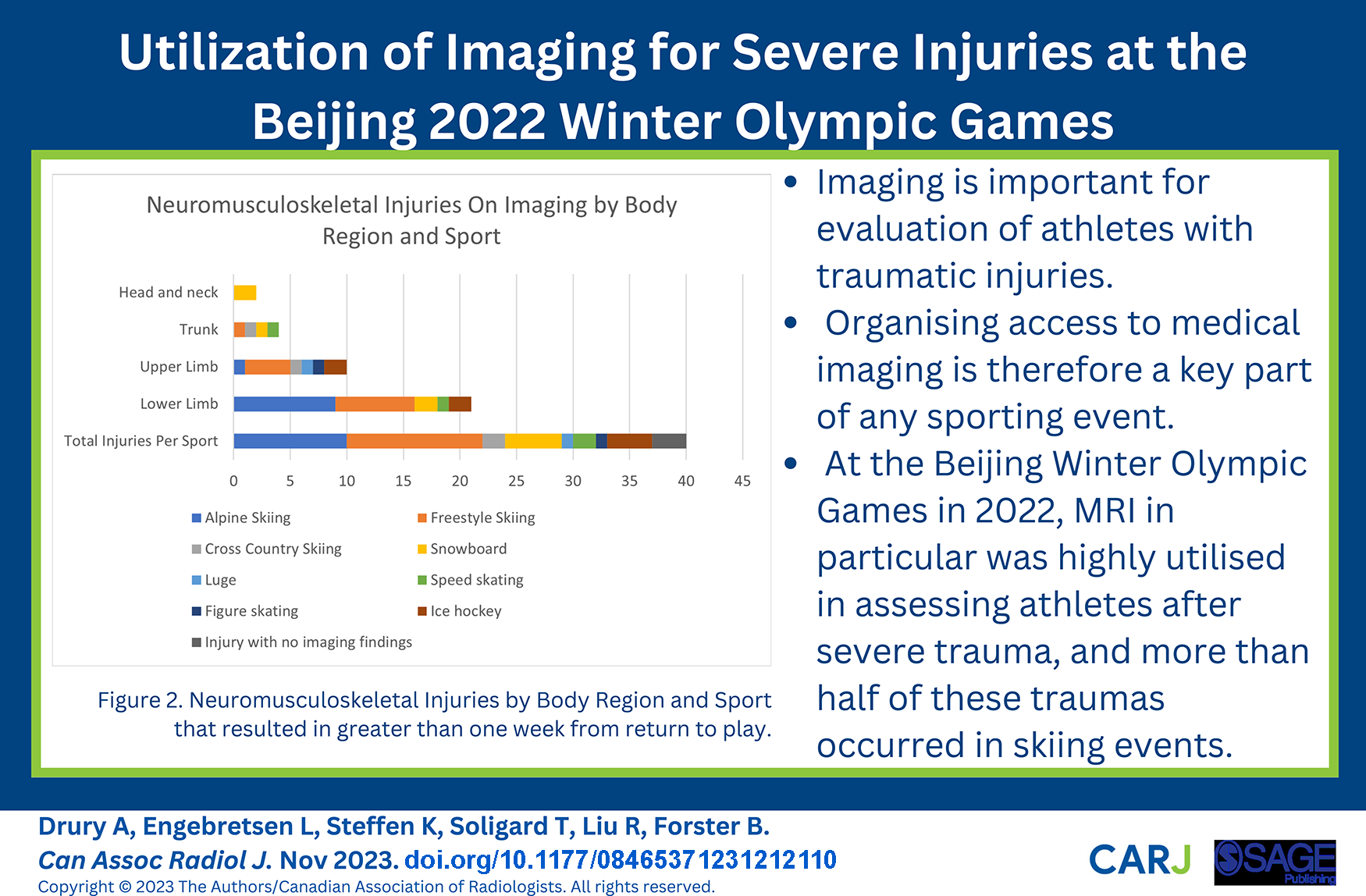
Introduction
The Beijing 2022 Winter Olympic Games welcomed 2871 athletes from 91 countries, competing in 109 events from February 4 to 20, 2022. Providing fast, effective medical care to this large cohort of high-performance athletes relied in part on diagnostic imaging to help evaluate injuries throughout the Games. Previous studies have focused on the Summer Games, 1 or described the role of imaging in specific injuries, categorized by body part or type of tissue.2-4 The Winter Games involve fewer athletes and events, but frequently involve dangerous conditions, such as high speeds in alpine terrain and on icy conditions, and metal edges and blades on skis, snowboards, and skates.
Severe injuries have been categorized by the International Olympic Committee (IOC) as greater than 7 days of time lost from sport. 5 By describing the incidence of severe injuries from these Games, the patterns of modality use, and the distribution of these modalities across venues/sports, we hope to facilitate a more comprehensive understanding of trauma care at the Winter Olympics. By examining the role of imaging in diagnosis and management of severe injuries, and the modalities relied upon by different sports across the venues, the organization of trauma care at future competitive winter sports events at any level can hopefully be optimized. Based on radiology care utilized in prior Olympic Games, 1 we hypothesize that cross-sectional imaging would play a critical role in evaluating severe injuries at the Beijing 2022 Winter Games.
Methods
Data Collection
As part of standardized protocols, all National Olympic Committee (NOC) medical teams reported the daily occurrence of injuries, and athlete data was collected in concordance with the “Information Notice on the Processing of Personal Data of Patients for the Games of the Beijing 2022 Olympic and Paralympic Winter Games.” Our study and intent to publish the data were approved by the International Olympic Committee, and signed consent to use data for research was obtained from all athletes as part of the overarching agreement between athletes and the IOC. Our study and intent to publish has also been approved by our institutional Office of Research Ethics (at the local large Canadian university), and the Norwegian National Research Ethics Committee. From the NOC physician reports, we extracted all injury reports that involved imaging, and then sub-selected for reports that described severe injuries, which were defined by greater than 7 day time-loss from training or competition. 5 Data security was rigorously maintained, with data tracked using the athlete identification number, and other identifiers, including country of athlete origin, removed.
Diagnostic imaging operated at all sites from February 4 to February 20, 2022, throughout the duration of the games. Modalities performed at the Games included radiography (DR), computed tomography (CT), magnetic resonance (MR) imaging, and ultrasound (US). The Beijing Olympic Village (BVL) Polyclinic had one DR on site, while CT and MRI were performed at the nearby Beijing Anzhen Hospital (<15 minutes driving time). The Yanqing Olympic Village (YVL) Polyclinic included one DR, one mobile CT, and an MRI unit; the nearest hospital was <30 minutes driving time. The Zhangjiakou Olympic Village (ZVL) Polyclinic included one DR and one CT, while MRI was performed at the Chongli hospitals (<15 minutes driving time). Two additional dental CT machines were provided at the ice hockey facilities, National Stadium and Wuesong, though these were excluded from this study as injuries did not result in significant time lost from sport. Ultrasound was provided at all Polyclinics, with musculoskeletal ultrasound performed by the orthopedic surgeons as part of the physical exam, and no images were recorded for use in this study. Ultrasounds were offered by some individual teams, and performed privately by team physicians in athlete residences, and thus were also excluded from this study.
For each athlete accreditation number, we collected data on date of injury, sport, venue, reported time-loss, and modality. Injuries in all sports and events were included; this consisted of 7 different sports, across 15 disciplines, in 109 events. These disciplines are Alpine Skiing, Freestyle skiing, Cross-country skiing, Biathlon, Bobsleigh, Curling, Figure Skating, Ice hockey, Luge, Nordic Combined, Short track speed skating, Speed skating, Skeleton, Ski jumping, and Snowboarding. Injury events were then excluded that did not meet criteria for severe injury (7 days of time-loss), as well as injury events that were purely superficial, such as skin lacerations. DICOM files from the remaining DR, CT, and MR study, including images and the original reports, were collected retrospectively based on the athlete accreditation numbers on the NOC injury reports. Data was then collected from each original imaging report, including body region and area of injury and the tissue and pathology types, per prior IOC recommendations for recording and reporting of epidemiological data on injury and illness in sport. 5
Data Organization and Analysis
If an athlete was seen at multiple medical facilities for the same injury, there were in some cases multiple NOC reports. These were reconciled by date of injury and accreditation number, and it was assumed that a single athlete on a single day had experienced a single injury. If a different report was issued for an athlete on a subsequent day, this was treated as a separate injury. If one injury event resulted in multiple injuries, for example, bilateral knee ligament tears, this was recorded as one injury for the purpose of overall incidence, in keeping with IOC recommendations 5 and thus as a single incidence of MRI use.
DICOM images were not reassessed for concordance with the final report issued by the original reporting radiologist, as quality assurance was not a component of the study.
Data trends are presented by organization into summary tables (see below) highlighting both the modalities used, and the injuries incurred for each sport. By recording the imaging pathway experienced by each athlete, from initial medical care, to initial imaging, to any transfer to another Olympic medical facility or dedicated referral hospital for further care, we hope to better understand how this distribution of resources and transfer requirements affected severely injured athletes. Summarizing the severe injuries in each sport was subsequently done to provide evidence of the types of trauma incurred by each athlete, and which injuries are more common in each sport. Formal statistical analysis was not performed due to the small sample size.
Results
In total, 2871 athletes from 91 National Olympic Committees participated in the Beijing Winter Olympic Games and are thus included in our study parameters. Over the course of the games, 171 radiographs, CTs, and MRIs were performed on these athletes across the Beijing, Yanqing, and Zhangjiakou sites, as well as at the dedicated referral hospitals, for all injuries. This distribution is highlighted in Table 1.
Overall Number of Athlete Imaging Examinations Performed by Olympic Site and Modality.
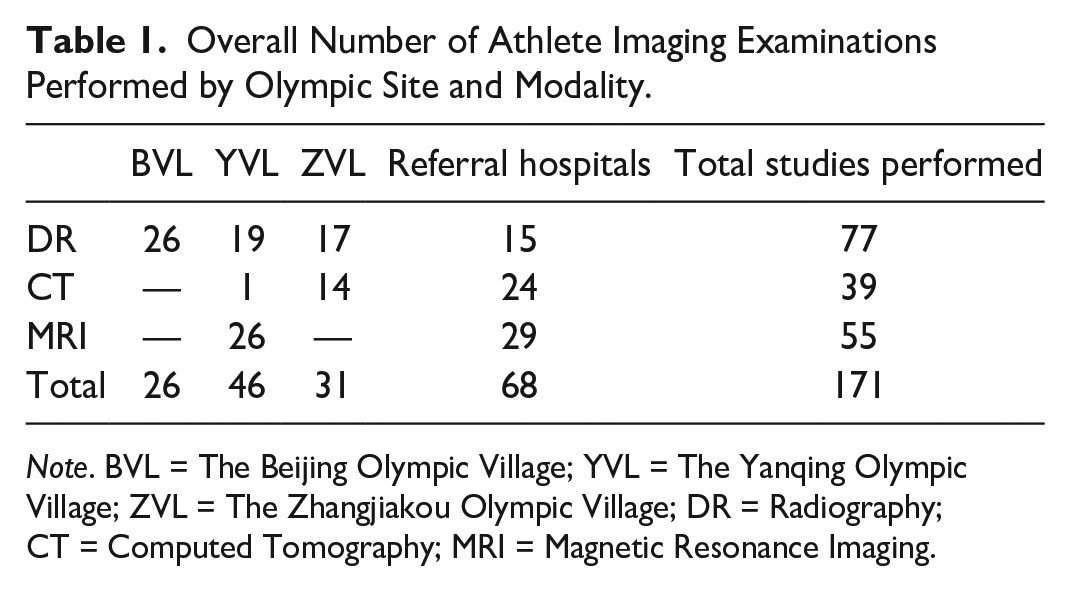
Note. BVL = The Beijing Olympic Village; YVL = The Yanqing Olympic Village; ZVL = The Zhangjiakou Olympic Village; DR = Radiography; CT = Computed Tomography; MRI = Magnetic Resonance Imaging.
As evidenced from this table, 68 of the total 171 (40%) of studies were completed at referral hospitals. The way each athlete accessed imaging across these sites is displayed in Table 2, which illustrates where each athlete was initially seen, initially imaged, and if they required any transport to another Olympic medical facility (eg, seen at an Athlete Medical Station and transferred to Polyclinic) or to the dedicated referral hospitals (Table 2).
Athletes With Severe Injuries by Venue, Site of Transfer, and Imaging Modality Performed.
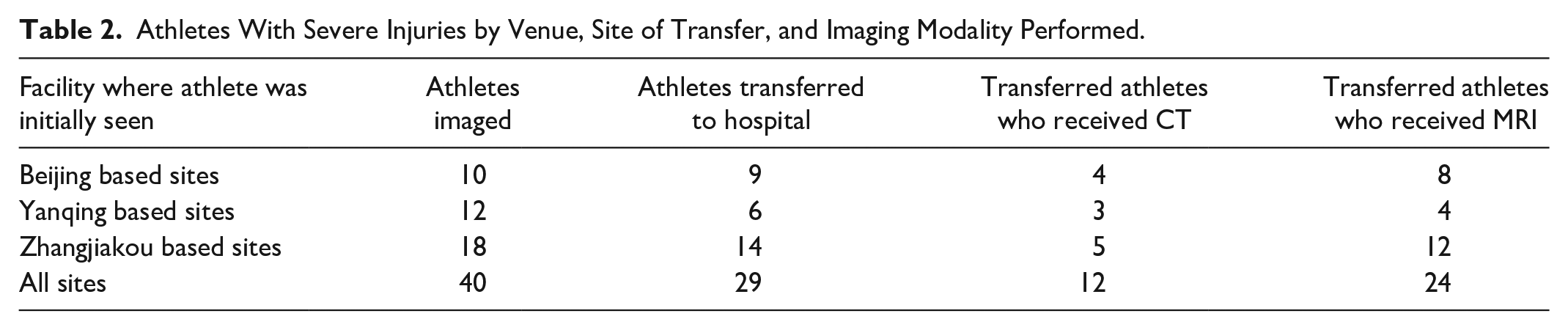
Overall, 40 athletes were imaged for severe trauma which was deemed to result in greater than 7 days off sport. These were all included in Table 2, as the goal was to demonstrate how athletes accessed imaging resources. At the Beijing venues (which did not have CT or MRI facilities in the referral Polyclinic), of the 8 athletes imaged, 7 were transferred to hospital, and they all received an MRI. Two athletes also underwent CT. From Zhangjiakou, which had access to CT but not MRI, 14 out of 18 athletes initially imaged were transferred to hospital, and 12 of these patients received MRI. The Yanqing venues had the fewest number of athletes transferred to hospital. These were the only venues that had access to dedicated MRI in their referral Polyclinic. Of the 12 athletes imaged, 6 were transferred. Although the small sample size limits the statistical significance of the data, the site without CT or MRI transferred 88% of patients, the site with CT but not MRI transferred 78% of patients, and the site with both cross-sectional imaging modalities transferred 50% of patients.
With this understanding of distribution of resources across venues, we subsequently analyzed the injuries incurred in each sport. No severe traumas resulting in more than 7 days loss of play originated from Curling, Biathlon, Nordic Combined, or Skeleton and these disciplines are therefore not shown as subcategories in all tables. The multiple disciplines within the sport of speed skating have been combined due to incomplete record keeping in terms of which specific type of speed skating the athlete was participating in, particularly following the removal of athlete identifiers from the data set. Within each discipline, sub-disciplines for each athlete were unfortunately not always recorded, and following the anonymization of data, could not be cross-referenced, and each discipline is thus reported as a single category.
As demonstrated by Figure 1, Skiing athletes accounted for the majority of imaging studies for evaluation of severe trauma, particularly in MRI, where these athletes accounted for 17 out of the 28 MRIs performed. Alpine and Freestyle Skiing had comparable use of MRI, but Freestyle had double the number of plain films performed. Perhaps surprisingly, given both sports have Freestyle events with jumps and racing, Snowboard had relatively low use of imaging compared to Skiing, and was comparable to Ice Hockey with both utilizing 4 MRIs.
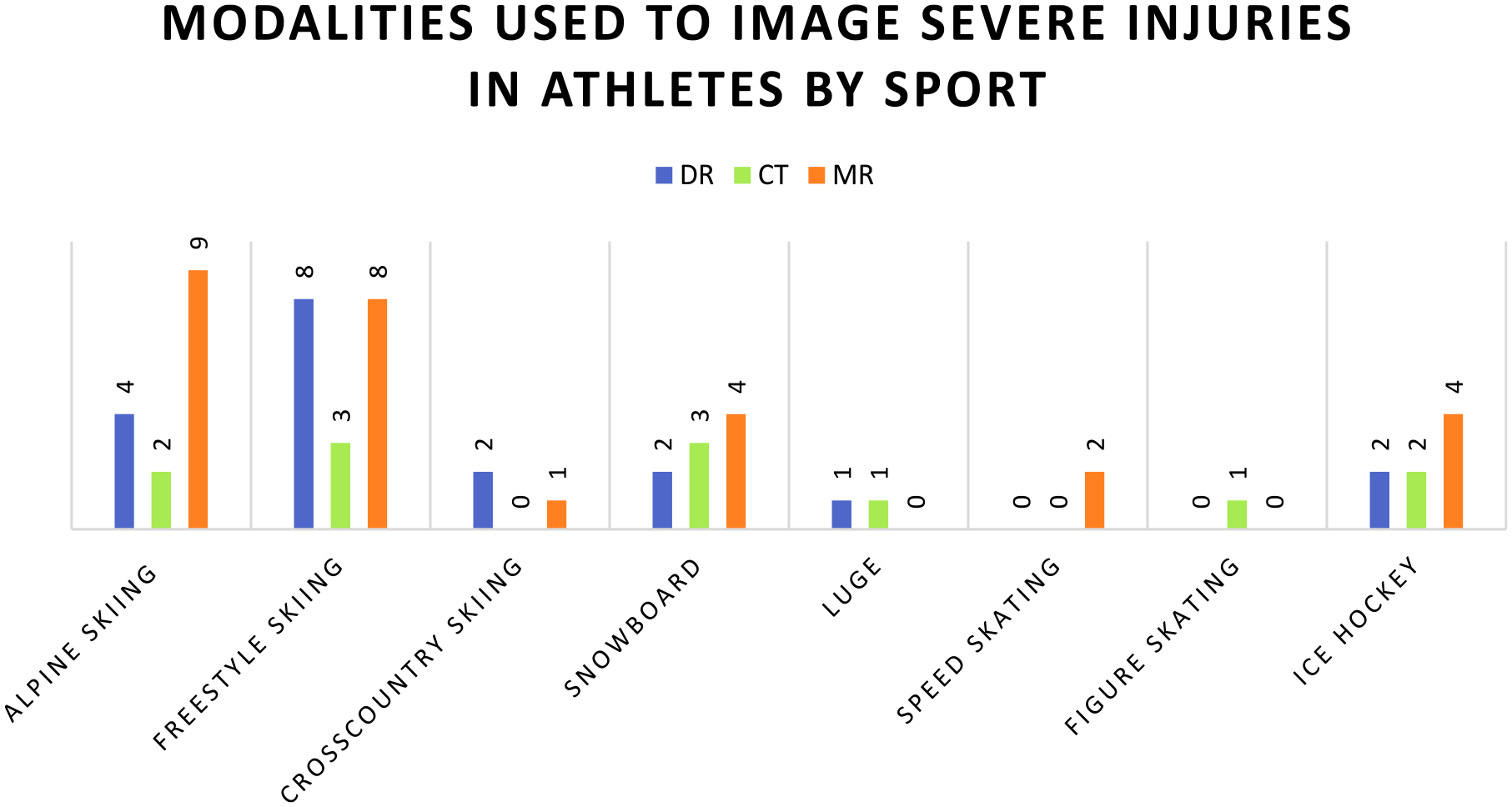
Athletes with severe injuries by sport and imaging modality. Some athletes required more than one modality for a single injury.
To present the results, we have subsequently categorized the types of injuries experienced based on the body region and tissue type injured (Figure 2). While there were 59 imaging studies performed to assess for severe traumatic injuries, 3 patients had no cause of injury on imaging. Two of these patients underwent radiograph and CT solely to rule out head and spine injuries, and one was a plain radiograph for elbow injury.
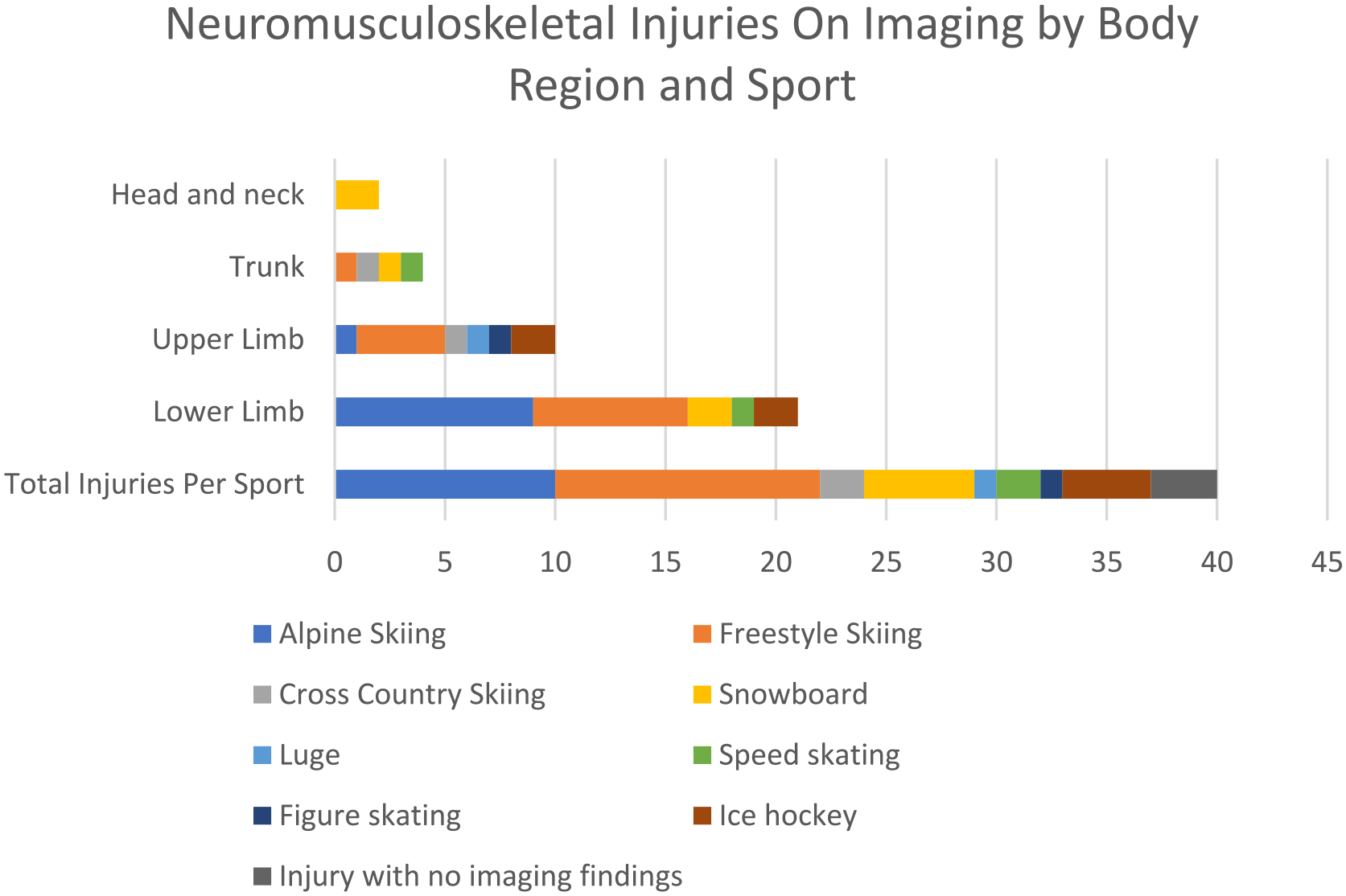
Neuromusculoskeletal injuries by body region and sport that resulted in greater than 1 week from return to play.
Body regions and tissue types in Figure 2 have been defined based on the International Olympic Committee Census Statement for recording and reporting of epidemiological data. 5 There were no reported intraabdominal or intrathoracic soft tissue injuries. Injured tissue categories (per IOC) included Muscle/Tendon, Nervous Bone, Cartilage/Synovium/Bursa, Ligament/Joint Capsule, and Superficial Tissues/Skin. Imaging that was positive for nervous system injury was all related to spine trauma, where there was an injury to the vertebral bone or intervertebral disc.
As potentially expected, based on the high number of imaging studies performed on Alpine and Freestyle Skiing athletes seen in Figure 1, athletes in these sports had the majority of injuries (22 out of 37). Of these, the lower limb was most involved (16/22 injuries). Cross country skiing had the fewest severe traumas, with only 2 injuries compared to 10 in Alpine Skiing and 12 in Freestyle. Perhaps surprisingly, there were only 5 severe traumatic injuries in Snowboard. The fewest injuries were in Figure Skating and Luge.
Injury examples include ligamentous tears, as seen in Figure 3, fractures, as seen in Figure 4, as well as meniscal tears, tendon injuries, bony contusions, and osteochondral injuries. While MRI accounted for nearly half the imaging studies (47%) on these severely injured athletes, some individuals only required X-ray and CT, such as in cases of extremity fracture as seen in Figure 4, where the diagnosis was made on plain film, with CT subsequently performed for operative planning including 3D reformats.

Lower limb injury in a skier requiring MRI evaluation. Sagittal PD FSE image, arrow points to the ACL tear.
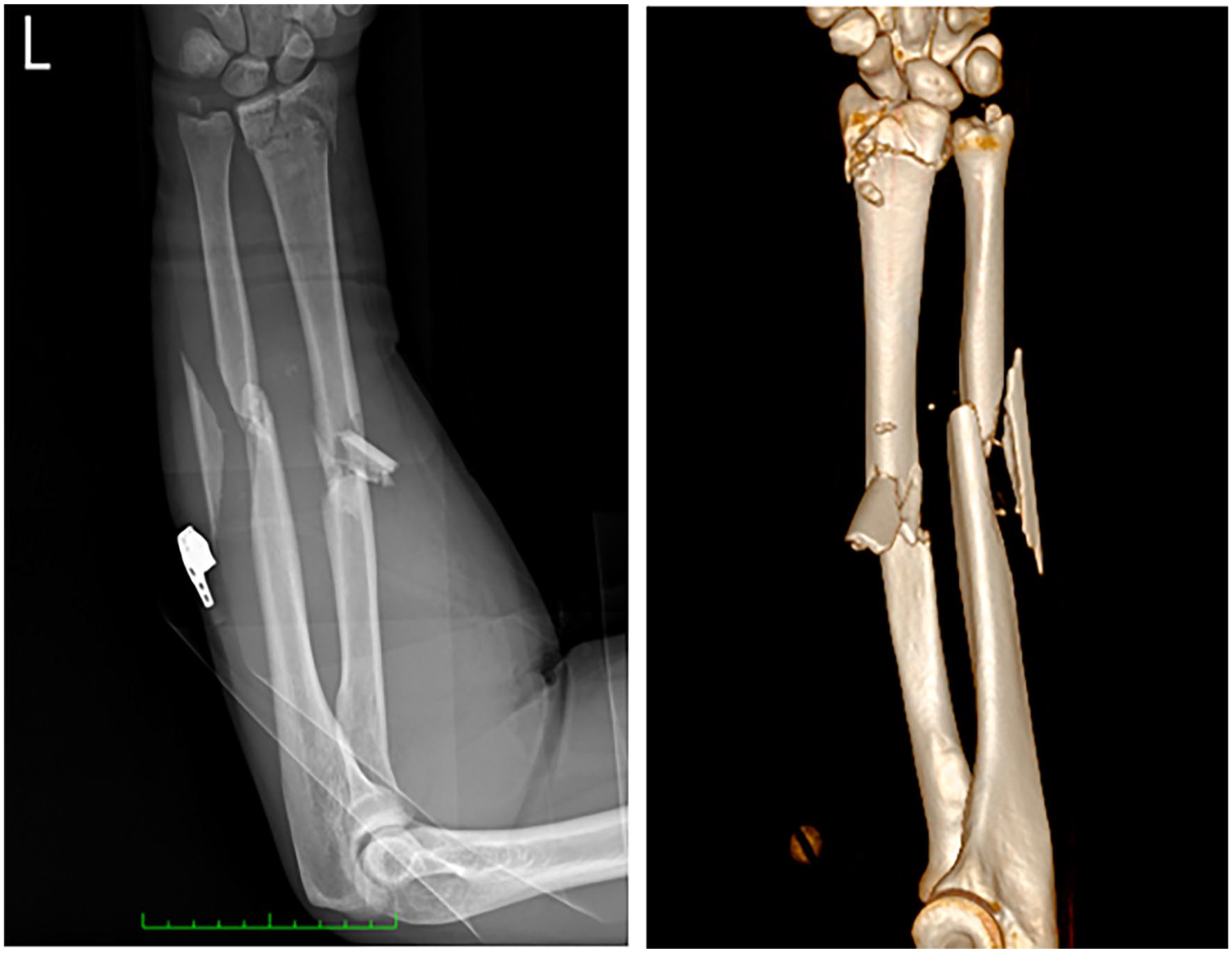
Forearm trauma. Radiograph and 3D reconstruction from CT demonstrate comminuted intra-articular fracture of the distal radius, ulnar styloid fracture, and comminuted, displaced, and angulated fractures of the radius and ulna mid-diaphyses.
Discussion
By demonstrating the use of imaging across all major venues of these Winter Olympics, we hope to inform future organization of medical imaging resources at professional and amateur sports venues. Optimizing the organization of medical resources so that they are accessible by severely injured athletes is a key clinical and policy implication of this study. For example, the demonstrated reliance on MRI, combined with the high number of severe injuries associated with skiing, paints a clear picture of why this modality should be easy to access for athletes in this sport.
If a limited number of MRIs are available for a winter sporting event, placing these machines in easy reach of the sports with the highest frequency of severe injuries that required diagnosis on MRI would be optimal. In our study, Alpine and Freestyle Skiing had comparable use of MRI, but Freestyle had double the number of plain films performed. The Alpine ski venue at Yanqing had an MRI on site, whereas the Big Air Shougang and Zhangjiakou Zone, with the Genting Snow Park, where Freestyle Skiing occurred did not have MRI on site. This may suggest that plain film use was increased when athletes had less immediate access to MRI. In a young population such as Olympic athletes, maximizing accessibility of radiation-free modalities is an important point of consideration.
Access to imaging resources is particularly relevant in the setting of winter sports, where adverse weather conditions such as icy roads and snowstorms can make transfer to other facilities difficult, despite relatively close facilities. Data can also be extrapolated outside of athletic competition setting; if a town has a ski hill, it can be anticipated that many transfers will be required of skiers to the closest MRI machine. Ensuring the local hospital has MRI capability could improve access to care.
Given the high speed, high impact nature of winter sports, head and spine imaging was necessary on several occasions to rule out craniospinal injury requiring surgical intervention, in the absence of any other body parts involved. While these injuries ultimately did not have imaging findings, they were a necessary part of patient care and thus included in the study. Comparison with summer Olympic data is difficult due to lack of information on negative CT studies performed during trauma cases. In this case, the involved sports were skiing and snowboarding, which the data already emphasizes as relatively high-injury sports that require urgent access to trauma imaging. Snowboarding resulted in fewer injuries than skiing but was the only discipline to result in positive imaging findings of the head and neck in severe trauma, with one cervical spine injury and one facial injury. The only other sport where an athlete had a suspected cervical spine injury, excluded with normal imaging, was Freestyle Skiing.
The relatively few severe traumatic injuries in Snowboard compared to Freestyle or Alpine Skiing were somewhat surprising, and we wondered if this could be accounted for by the number of athletes involved. A total of 310 athletes competed in Alpine Skiing, and 272 in Freestyle Skiing, while 233 competed in Snowboard. While the number of injuries is small, limiting statistical comparison, this does not appear to account for the ratio of injuries, with 10 in Alpine and 12 in Freestyle Skiing, and 5 in Snowboard.
By describing the reliance on imaging in the winter sport setting, we can compare with available information on summer sport imaging use, to better understand the relative risk associated with winter sports versus summer sports. In the Rio de Janeiro 2016 Summer Olympic Games, for example, 221 injuries were recorded that resulted in greater than 7 days of time lost from sport, 6 in 11 274 participating athletes. This equates to a ratio of 0.0196 severe injuries per athlete. In the Tokyo 2020 Games, there were 11 315 athletes with 205 severe injuries, for a ratio of 0.018 severe injuries per athlete. 7 In the current study from Beijing, there were 40 severe injuries that underwent imaging, in 2871 athletes, with the resultant ratio being 0.0139 severe injuries per athlete. A comparable number of severe injuries is therefore seen, with 0.01 to 0.02 injuries per athlete at both Summer and Winter Olympic games. While Alpine and Freestyle Skiing are responsible for a high percent of Winter Olympics severe injuries, Summer severe injuries are disproportionately associated with bicycle moto cross (BMX) racing, highlighting the comparative risks of these fast sports on uneven terrain. 7
Our study does have limitations. While detailed information was recorded on where each athlete accessed medical imaging care, there was limited recorded data on why the patient was transferred to hospital in each case. Evaluation of the data on the role of imaging played patient transfer is therefore limited by a lack of information about the distribution of other services; for example, it is unclear whether the patients at Yanqing would need to be transferred regardless of imaging, due to the organization of orthopedic surgery. More complete prospective compilation of data on other trauma-related services with these severely injured patients may be of use in the future.
Data was also limited by the variable recording of sport subdiscipline details. Anecdotally, ski and snowboard cross had a high number of perceived injuries, but without subdiscipline information attached to all records, this is difficult to ascertain.
As described in the Data Collection above, ultrasound was excluded from this study. Therefore, any severe injuries diagnosed solely based on ultrasound would have been missed. If these studies were intended for inclusion in future projects, it would require reliable record of imaging findings from all the team physicians from every country, which may not be feasible.
Conclusion
Medical imaging is a critical part of caring for severe traumatic injuries with high stakes implications for athletes facing long return to play times. Understanding the frequency and type of imaging used in evaluating these injuries is necessary for predicting where and when athletes will need medical imaging, and thus being able to organize imaging at sporting events of any level. At the Beijing Winter Olympic Games in 2022, radiography, CT, and MRI each played important roles in the evaluation of severe trauma for these athletes, with MRI being particularly integral, comprising half of studies on severely injured athletes and nearly 80% of ski and snowboard imaging studies. Perhaps equally important were the critical injury imaging results that showed no injury; using CT to rule out acute intracranial injury was necessary for several patients. Appreciating which sports had high imaging usage, what injuries these modalities were used to diagnose, and how athletes accessed these resources can help with operations management for future sporting events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LE serves as Head of Medical Sciences in the International Olympic Committee. TS serves as scientific manager in the Medical and Scientific Department of the International Olympic Committee. BBF serves as a member of the International Olympic Committee Medical and Scientific Games Group.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.